Inflammatory and Oxidative Stress Markers—Mirror Tools in Rheumatoid Arthritis

 ,
,  ,
,  ,
,  ,
, 
 ,
, 
Abstract
:1. Introduction
2. Experimental Section
2.1. Ethical Issue
2.2. Sample Collection
2.3. Oxidative Stress Markers Analysis Steps
2.4. Lipid Peroxidation Analysis
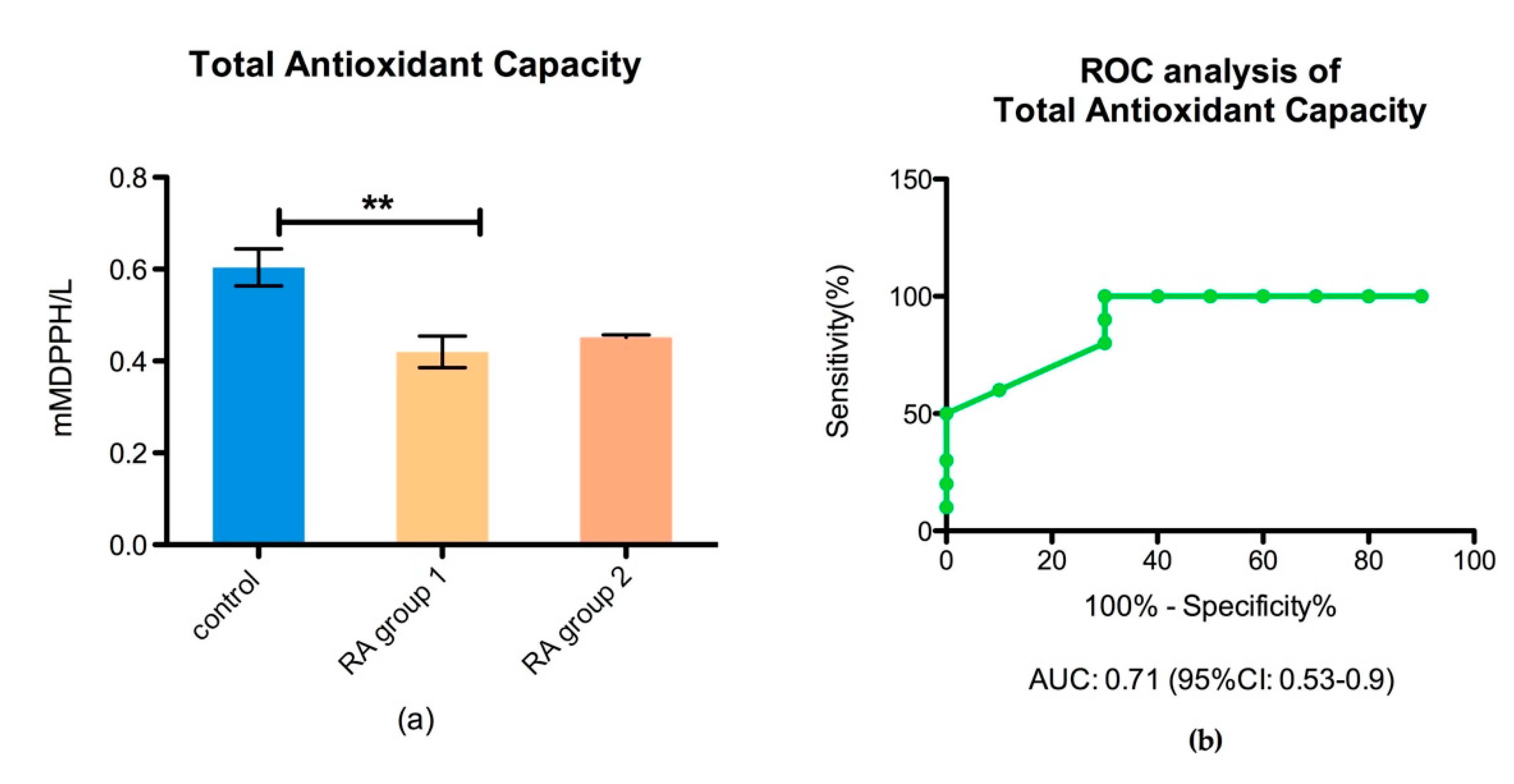
2.5. Total Antioxidant Capacity (TAC) Analysis
2.6. Complete Blood Counting (CBC)
2.7. Statistical Analysis
3. Results
3.1. The Immune Status Biomarkers
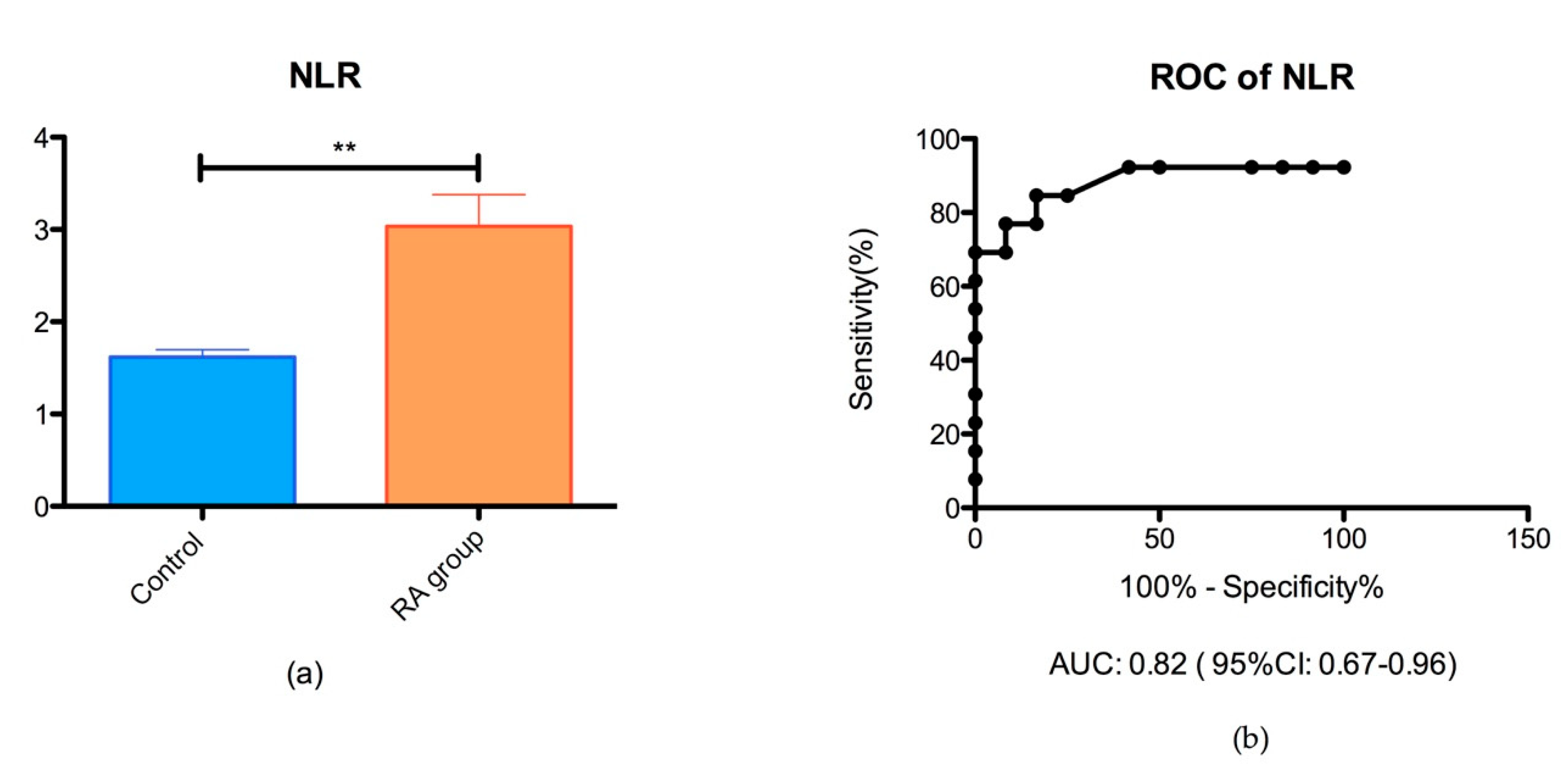
3.1.1. Neutrophil/Lymphocyte Ratio (NLR)
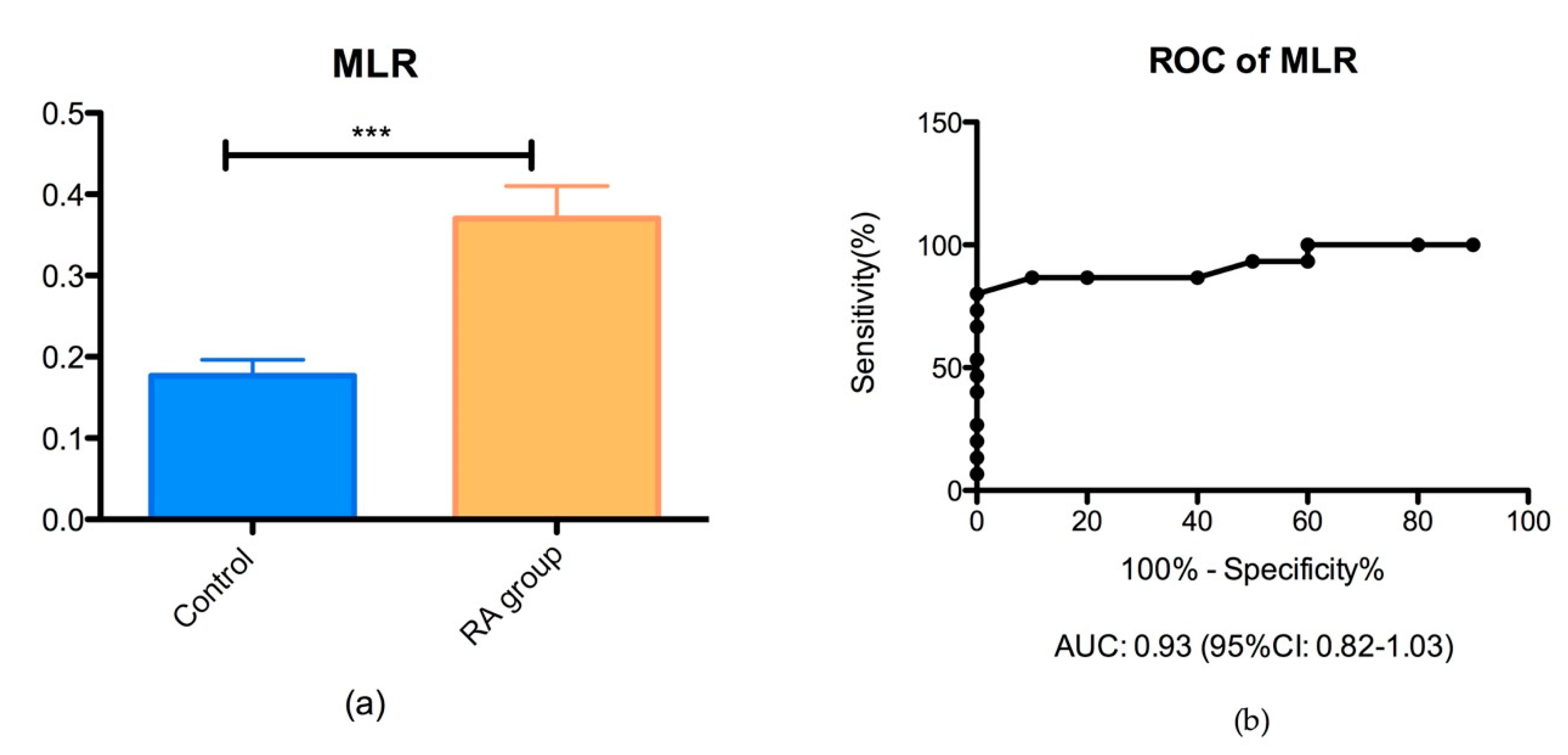
3.1.2. Monocyte/Lymphocyte Ratio (MLR)
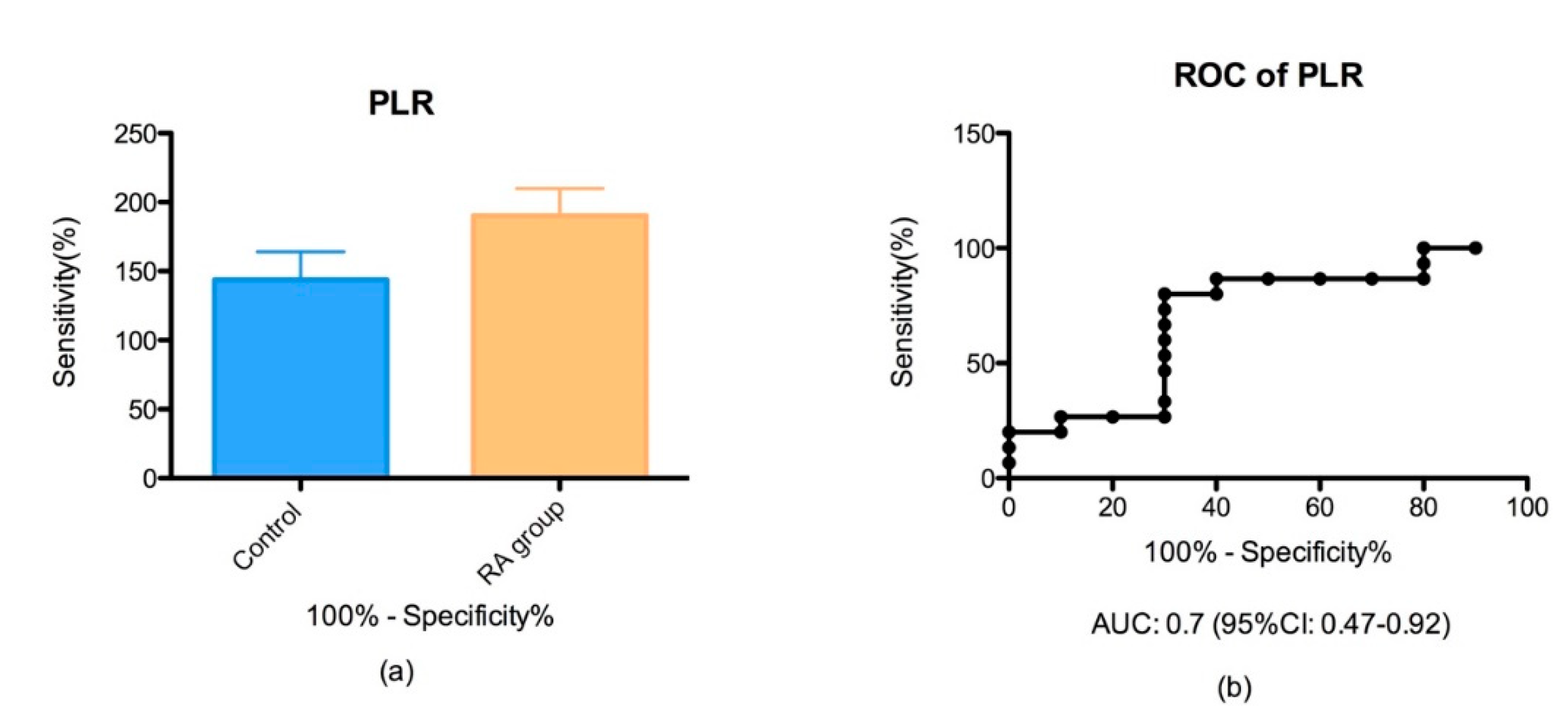
3.1.3. Platelet/Lymphocyte Ratio (PltLR)
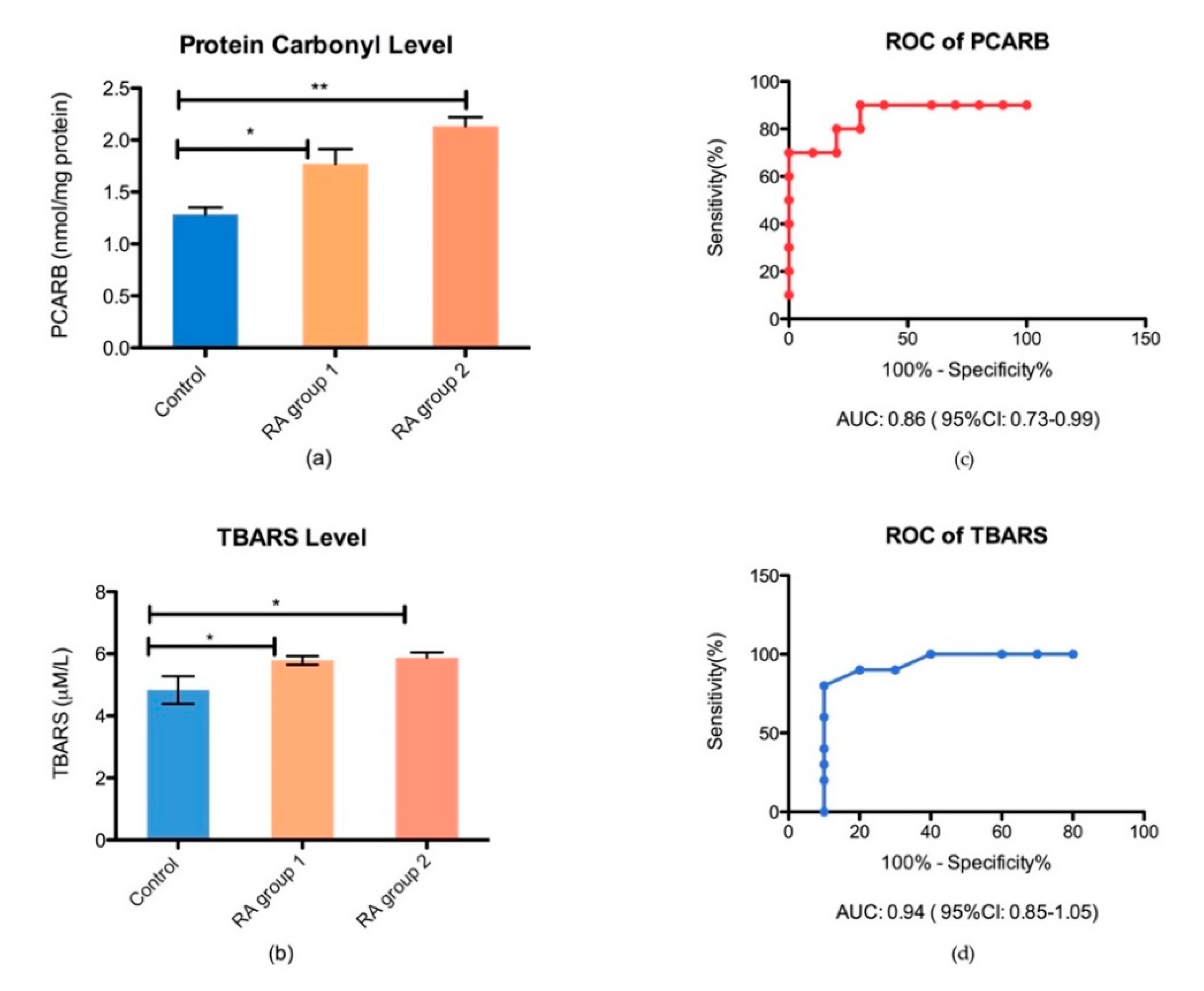
3.2. Oxidative Stress Products in Plasma
3.3. Antioxidant Defense
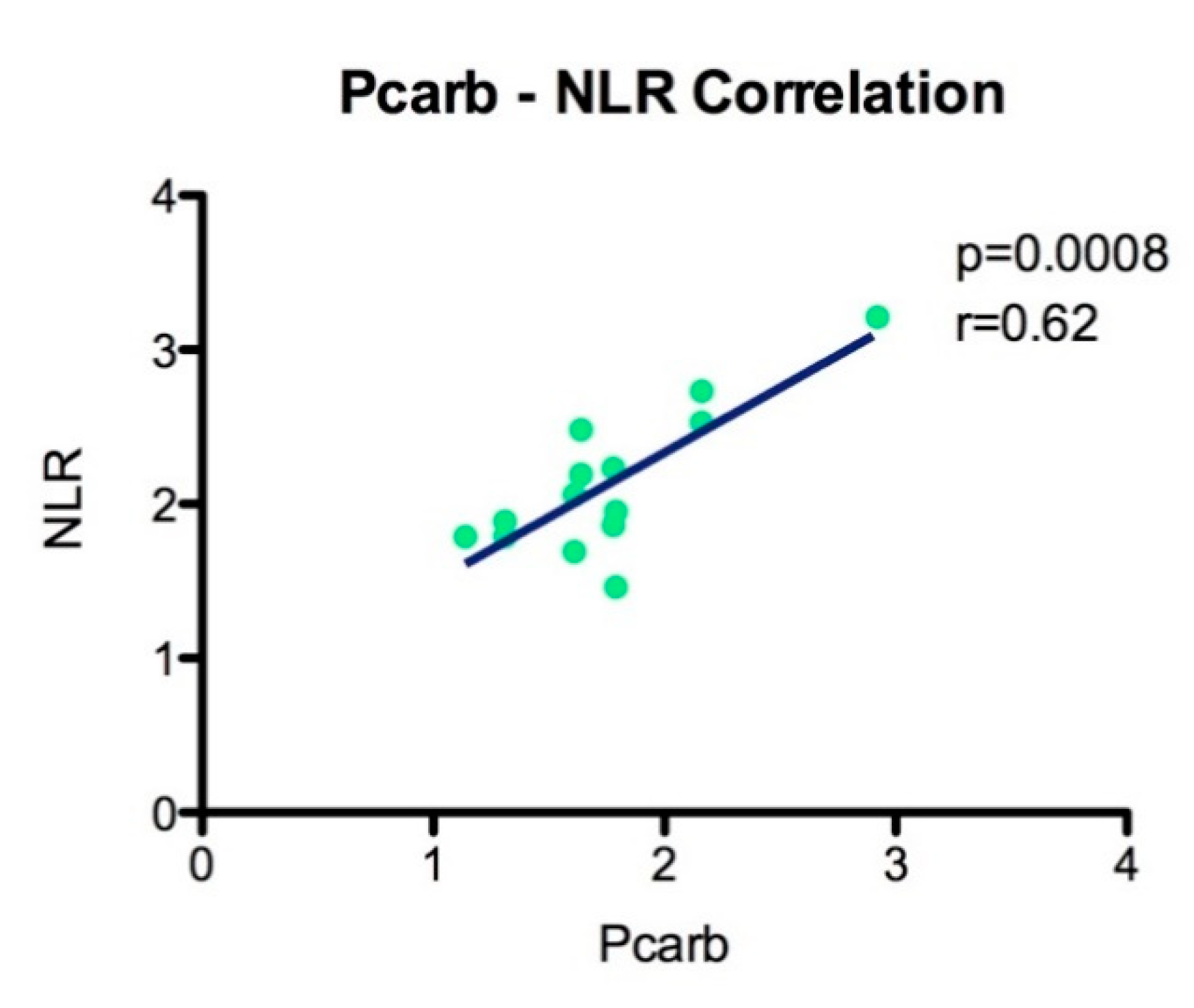
3.4. Correlation of Oxidative Stress with Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Scrivo, R.; Perricone, C.; Altobelli, A.; Castellani, C.; Tinti, L.; Conti, F.; Valesini, G. Dietary Habits Bursting into the Complex Pathogenesis of Autoimmune Diseases: The Emerging Role of Salt from Experimental and Clinical Studies. Nutrition 2019, 11, 1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fousert, E.; Toes, R.; Desai, J. Neutrophil Extracellular Traps (NETs) Take the Central Stage in Driving Autoimmune Responses. Cells 2020, 9, 915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rasmo, D.; Ferretta, A.; Russo, S.; Ruggieri, M.; Lasorella, P.; Paolicelli, D.; Trojano, M.; Signorile, A. PBMC of Multiple Sclerosis Patients Show Deregulation of OPA1 Processing Associated with Increased ROS and PHB2 Protein Levels. Biomedicines 2020, 8, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mun, S.; Lee, J.; Park, A.; Kim, H.-J.; Lee, Y.-J.; Son, H.; Shin, M.; Lim, M.-K.; Kang, H.-G. Proteomics Approach for the Discovery of Rheumatoid Arthritis Biomarkers Using Mass Spectrometry. Int. J. Mol. Sci. 2019, 20, 4368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, N.P.; Park, S.; Anh, N.H.; Min, J.E.; Yoon, S.J.; Kim, H.M.; Nghi, T.D.; Lim, D.K.; Park, J.H.; Lim, J.; et al. Efficacy of Integrating a Novel 16-Gene Biomarker Panel and Intelligence Classifiers for Differential Diagnosis of Rheumatoid Arthritis and Osteoarthritis. J. Clin. Med. 2019, 8, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Docea, A.O.; Gofita, E.; Goumenou, M.; Calina, D.; Rogoveanu, O.; Varut, M.; Olaru, C.; Kerasioti, E.; Fountoucidou, P.; Taitzoglou, I.; et al. Six months exposure to a real life mixture of 13 chemicals’ below individual NOAELs induced non monotonic sex-dependent biochemical and redox status changes in rats. Food Chem. Toxicol. 2018, 115, 470–481. [Google Scholar] [CrossRef]
- Wahba, A.; Ibrahim, M.; Mesbah, N.; Saleh, S.; Abo-Elmatty, D.; Mehanna, E. Serum LINC00305 expression and its genetic variant rs2850711 are associated with clinical and laboratory features of rheumatoid arthritis. Br. J. Biomed. Sci. 2020, 1–6. [Google Scholar] [CrossRef]
- Tanhapour, M.; Shahmohamadnejad, S.; Vaisi-Raygani, A.; Kiani, A.; Shakiba, Y.; Rahimi, Z.; Bahrehmand, F.; Shakiba, E.; Vaisi-Raygani, A.-A.; Alibakhshi, R.; et al. Association between activity and genotypes of paraoxonase1 L55M (rs854560) increases the disease activity of rheumatoid arthritis through oxidative stress. Mol. Boil. Rep. 2018, 46, 741–749. [Google Scholar] [CrossRef]
- Shahmohamadnejad, S.; Vaisi-Raygani, A.; Shakiba, Y.; Kiani, A.; Rahimi, Z.; Bahrehmand, F.; Shakiba, E.; Pourmotabbed, T.; Shahmohamdnejad, S. Association between butyrylcholinesterase activity and phenotypes, paraoxonase192 rs662 gene polymorphism and their enzymatic activity with severity of rheumatoid arthritis: Correlation with systemic inflammatory markers and oxidative stress, preliminary report. Clin. Biochem. 2015, 48, 63–69. [Google Scholar] [CrossRef]
- Rogoveanu, O.C.; Calina, D.; Cucu, M.G.; Burada, F.; Docea, A.O.; Sosoi, S.; Stefan, E.; Ioana, M.; Burada, E. Association of cytokine gene polymorphisms with osteoarthritis susceptibility. Exp. Ther. Med. 2018, 16, 2659–2664. [Google Scholar] [CrossRef]
- Trăistaru, M.R.; Kamal, D.; Traşcă, D.M.; Foarfă, M.C.; Gruia, C.L.; Rogoveanu, O.C. Rheumatoid nodules and quality of life in rheumatoid arthritis females—Complex assessment. Rom. J. Morphol. Embryol. 2016, 57, 215–225. [Google Scholar] [PubMed]
- Florentin-Ananu, V.; Chisalau, B.; Parvanescu, C.; Barbulescu, A.; Rogoveanu, O.; Firulescu, S.; Rosu, A.; Ciurea, P. High Frequency Ultrasonography of the Hand in Rheumatoid Arthritis, Psoriatic Arthritis, Gout and Osteoarthritis Patients. Curr. Heal. Sci. J. 2016, 42, 35–39. [Google Scholar]
- Mateen, S.; Moin, S.; Khan, A.Q.; Zafar, A.; Fatima, N. Increased Reactive Oxygen Species Formation and Oxidative Stress in Rheumatoid Arthritis. PLoS ONE 2016, 11, e0152925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phull, A.R.; Nasir, B.; Haq, I.-U.; Ashraf, Z. Oxidative stress, consequences and ROS mediated cellular signaling in rheumatoid arthritis. Chem. Interact. 2018, 281, 121–136. [Google Scholar] [CrossRef]
- Goronzy, J.J.; Shao, L.; Weyand, C.M. Immune Aging and Rheumatoid Arthritis. Rheum. Dis. Clin. North Am. 2010, 36, 297–310. [Google Scholar] [CrossRef] [Green Version]
- Lindstrom, T.M.; Robinson, W.H. Rheumatoid arthritis: A role for immunosenescence? J. Am. Geriatr. Soc. 2010, 58, 1565–1575. [Google Scholar] [CrossRef] [Green Version]
- Chalan, P.; Berg, A.V.D.; Kroesen, B.-J.; Brouwer, L.; Boots, A. Rheumatoid Arthritis, Immunosenescence and the Hallmarks of Aging. Curr. Aging Sci. 2015, 8, 131–146. [Google Scholar] [CrossRef] [Green Version]
- Da Fonseca, L.J.S.; Nunes-Souza, V.; Goulart, M.O.F.; Rabelo, L.A. Oxidative Stress in Rheumatoid Arthritis: What the Future Might Hold regarding Novel Biomarkers and Add-On Therapies. Oxidative Med. Cell. Longev. 2019, 2019, 7536805. [Google Scholar] [CrossRef] [Green Version]
- Smallwood, M.J.; Nissim, A.; Knight, A.R.; Whiteman, M.; Haigh, R.; Winyard, P. Oxidative stress in autoimmune rheumatic diseases. Free Radic. Boil. Med. 2018, 125, 3–14. [Google Scholar] [CrossRef]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative Stress. Annu. Rev. Biochem. 2017, 86, 715–748. [Google Scholar] [CrossRef]
- García-González, A.; Gaxiola-Robles, R.; Zenteno-Savin, T. Oxidative stress in patients with rheumatoid arthritis. Rev. Invest. Clin. 2015, 67, 46–53. [Google Scholar] [PubMed]
- Quiñonez-Flores, C.M.; González-Chávez, S.A.; Nájera, D.D.R.; Pacheco-Tena, C. Oxidative Stress Relevance in the Pathogenesis of the Rheumatoid Arthritis: A Systematic Review. Biomed. Res. Int. 2016, 2016, 6097417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaghef-Mehrabany, E.; Rad, A.H.; Alipour, B.; Sharif, S.-K.; Vaghef-Mehrabany, L.; Alipour-Ajiry, S. Effects of Probiotic Supplementation on Oxidative Stress Indices in Women with Rheumatoid Arthritis: A Randomized Double-Blind Clinical Trial. J. Am. Coll. Nutr. 2015, 35, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Batooei, M.; Roudsari, A.T.; Basiri, Z.; Yasrebifar, F.; Shahdoust, M.; Eshraghi, A.; Mehrpooya, M.; Ataei, S. Evaluating the Effect of Oral N-acetylcysteine as an Adjuvant Treatment on Clinical Outcomes of Patients with Rheumatoid Arthritis: A Randomized, Double Blind Clinical Trial. Rev. Recent Clin. Trials 2018, 13, 132–138. [Google Scholar] [CrossRef]
- Kang, E.H.; Ha, Y.-J.; Lee, Y.J. Autoantibody Biomarkers in Rheumatic Diseases. Int. J. Mol. Sci. 2020, 21, 1382. [Google Scholar] [CrossRef] [Green Version]
- Abd-Elazeem, M.I.; Mohamed, R.A. Neutrophil-lymphocyte and platelet-lymphocyte ratios in rheumatoid arthritis patients: Relation to disease activity. Egypt. Rheumatol. 2018, 40, 227–231. [Google Scholar] [CrossRef]
- Boulos, D.; Proudman, S.M.; Metcalf, R.G.; McWilliams, L.; Hall, C.; Wicks, I.P. The neutrophil-lymphocyte ratio in early rheumatoid arthritis and its ability to predict subsequent failure of triple therapy. Semin. Arthritis Rheum. 2019, 49, 373–376. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Langille, E. Optimized Oxidative Stress Protocols for Low-microliter Volumes of Mammalian Plasma. Bio-Protocol 2019, 9, 3221. [Google Scholar] [CrossRef]
- Jansen, E.H.J.M.; Beekhof, P.K.; Cremers, J.W.J.M.; Viezeliene, D.; Muzakova, V.; Skalicky, J. Short-Term Stability of Biomarkers of Oxidative Stress and Antioxidant Status in Human Serum. ISRN Biomarkers 2013, 2013, 316528. [Google Scholar] [CrossRef]
- Padureanu, R.; Albu, C.V.; Mititelu, R.R.; Bacanoiu, M.V.; Docea, A.O.; Calina, D.; Pădureanu, V.; Olaru, G.; Sandu, R.E.; Malin, R.D.; et al. Oxidative Stress and Inflammation Interdependence in Multiple Sclerosis. J. Clin. Med. 2019, 8, 1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patsoukis, N.; Papapostolou, I.; Zervoudakis, G.; Georgiou, C.; Matsokis, N.A.; Panagopoulos, N.T. Thiol redox state and oxidative stress in midbrain and striatum of weaver mutant mice, a genetic model of nigrostriatal dopamine deficiency. Neurosci. Lett. 2005, 376, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Colombo, G.; Clerici, M.; Garavaglia, M.E.; Giustarini, D.; Rossi, R.; Milzani, A.D.G.; Dalle-Donne, I. A step-by-step protocol for assaying protein carbonylation in biological samples. J. Chromatogr. B 2016, 1019, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Spanidis, Y.; Goutzourelas, N.; Stagos, D.; Mpesios, A.; Priftis, A.; Bar-Or, D.; Spandidos, D.; Tsatsakis, A.M.; Leon, G.; Kouretas, D. Variations in oxidative stress markers in elite basketball players at the beginning and end of a season. Exp. Ther. Med. 2015, 11, 147–153. [Google Scholar] [CrossRef]
- Liu, J.; Yeo, H.C.; Doniger, S.J.; Ames, B.N. Assay of Aldehydes from Lipid Peroxidation: Gas Chromatography–Mass Spectrometry Compared to Thiobarbituric Acid. Anal. Biochem. 1997, 245, 161–166. [Google Scholar] [CrossRef]
- Keles, M.; Taysi, S.; Sen, N.; Aksoy, Y.; Akçay, F. Effect of corticosteroid therapy on serum and CSF malondialdehyde and antioxidant proteins in multiple sclerosis. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2001, 28, 141–143. [Google Scholar] [CrossRef] [Green Version]
- Janaszewska, A.; Bartosz, G. Assay of total antioxidant capacity: Comparison of four methods as applied to human blood plasma. Scand. J. Clin. Lab. Investig. 2002, 62, 231–236. [Google Scholar] [CrossRef]
- Demirci, S.; Demirci, S.; Kutluhan, S.; Koyuncuoglu, H.R.; Yurekli, V.A. The Clinical Significance of the Neutrophil-to-Lymphocyte Ratio in Multiple Sclerosis. Int. J. Neurosci. 2015, 126, 1–24. [Google Scholar] [CrossRef]
- Koffeman, E.C.; Genovese, M.; Amox, D.; Keogh, E.; Santana, E.; Matteson, E.L.; Kavanaugh, A.; Molitor, J.A.; Schiff, M.H.; Posever, J.O.; et al. Epitope-specific immunotherapy of rheumatoid arthritis: Clinical responsiveness occurs with immune deviation and relies on the expression of a cluster of molecules associated with T cell tolerance in a double-blind, placebo-controlled, pilot phase II trial. Arthritis Rheum. 2009, 60, 3207–3216. [Google Scholar] [CrossRef]
- Chen, M.-H.; Chou, C.-T.; Hou, M.-C.; Tsai, C.-Y.; Huang, Y. Low but Long-lasting Risk of Reversal of Seroconversion in Patients with Rheumatoid Arthritis Receiving Immunosuppressive Therapy. Clin. Gastroenterol. Hepatol. 2020, 1542. [Google Scholar] [CrossRef]
- Avci, B.Ş.; Avci, A.; Dönmez, Y.; Kaya, A.; Gülen, M.; Özer, A.I.; Bulut, A.; Koç, M.; Nazik, H.; Satar, S. The Effectiveness of Neutrophil-Lymphocyte Ratio in Predicting in-Hospital Mortality in Non-ST-Elevation Myocardial Infarction. Emerg. Med. Int. 2020, 2020, 8718304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, K.; Zhu, W.; Liu, W.; Ma, D.; Li, H.; Yu, W.; Wang, L.; Cao, Y.; Jiang, Y. Diagnostic value of the blood monocyte-lymphocyte ratio in knee osteoarthritis. J. Int. Med Res. 2019, 47, 4413–4421. [Google Scholar] [CrossRef] [PubMed]
- Taşoğlu, I.; Çiçek, Ö.F.; Lafcı, G.; Kadirogulları, E.; Sert, D.E.; Demir, A.; Cavus, U.; Colak, N.; Songür, M.; Hodo, B.; et al. Usefulness of Neutrophil/Lymphocyte Ratio as a Predictor of Amputation after Embolectomy for Acute Limb Ischemia. Ann. Vasc. Surg. 2014, 28, 606–613. [Google Scholar] [CrossRef]
- Taşoğlu, Ö.; Bölük, H.; Onat, Ş.Ş.; Özgirgin, N.; Taşoğlu, I. Is blood neutrophil-lymphocyte ratio an independent predictor of knee osteoarthritis severity? Clin. Rheumatol. 2016, 35, 1579–1583. [Google Scholar] [CrossRef]
- Panni, R.Z.; Lopez-Aguiar, A.G.; Liu, J.; Poultsides, G.A.; Rocha, F.G.; Hawkins, W.G.; Strasberg, S.M.; Trikalinos, N.A.; Maithel, S.; Fields, R.C.; et al. Association of preoperative monocyte-to-lymphocyte and neutrophil-to-lymphocyte ratio with recurrence-free and overall survival after resection of pancreatic neuroendocrine tumors (US-NETSG). J. Surg. Oncol. 2019, 120, 632–638. [Google Scholar] [CrossRef]
- Li, K.J.; Xia, X.F.; Su, M.; Zhang, H.; Chen, W.H.; Zou, C.L. Predictive value of lymphocyte-to-monocyte ratio (LMR) and neutrophil-to-lymphocyte ratio (NLR) in patients with esophageal cancer undergoing concurrent chemoradiotherapy. BMC Cancer 2019, 19, 1004. [Google Scholar] [CrossRef]
- Xu, N.; Tang, X.-F.; Yao, Y.; Zhao, X.-; Chen, J.-; Gao, Z.-; Yang, Y.-; Gao, R.-L.; Xu, B.; Yuan, J.-Q. Predictive value of neutrophil to lymphocyte ratio in long-term outcomes of left main and/or three-vessel disease in patients with acute myocardial infarction. Catheter. Cardiovasc. Interv. 2018, 91, 551–557. [Google Scholar] [CrossRef] [Green Version]
- Chandrashekara, S.; Ahmad, M.M.; Renuka, P.; Anupama, K.R.; Renuka, K. Characterization of neutrophil-to-lymphocyte ratio as a measure of inflammation in rheumatoid arthritis. Int. J. Rheum. Dis. 2017, 20, 1457–1467. [Google Scholar] [CrossRef]
- Uslu, A.U.; Kucuk, A.; Sahin, A.; Ugan, Y.; Yilmaz, R.; Gungor, T.; Bağçacı, S.; Kucuksen, S. Two new inflammatory markers associated with Disease Activity Score-28 in patients with rheumatoid arthritis: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Int. J. Rheum. Dis. 2015, 18, 731–735. [Google Scholar] [CrossRef]
- Fu, H.; Qin, B.; Hu, Z.; Ma, N.; Yang, M.; Wei, T.; Tang, Q.; Huang, Y.; Huang, F.; Liang, Y.; et al. Neutrophil- and platelet-to-lymphocyte ratios are correlated with disease activity in rheumatoid arthritis. Clin. Lab. 2015, 61, 269–273. [Google Scholar] [CrossRef]
- Sargın, G.; Senturk, T.; Yavasoglu, I.; Kose, R. Relationship between neutrophil-lymphocyte, platelet-lymphocyte ratio and disease activity in rheumatoid arthritis treated with rituximab. Int. J. Rheum. Dis. 2018, 21, 2122–2127. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Chen, D.-Y.; Xu, X.-Z.; Liu, Y.-Y.; Yin, T.-T.; Li, N. Platelet/Lymphocyte, Lymphocyte/Monocyte, and Neutrophil/Lymphocyte Ratios as Biomarkers in Patients with Rheumatoid Arthritis and Rheumatoid Arthritis-Associated Interstitial Lung Disease. Med Sci. Monit. 2019, 25, 6474–6481. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.-F.; Cao, L.; Zeng, Y.-H.; Zhang, Z.-X.; Chen, D.; Zhang, Q.; Zhu, Y.-S. Platelet to lymphocyte ratio and neutrophil to lymphocyte ratio in patients with rheumatoid arthritis. Open Med. 2015, 10, 249–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tschopp, J.; Schroder, K. NLRP3 inflammasome activation: The convergence of multiple signalling pathways on ROS production? Nat. Rev. Immunol. 2010, 10, 210–215. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | RA Group | Control Group |
|---|---|---|
| Age mean | 59.69 ± 8.53 | 56.4 ± 6.73 |
| Sex ratio (F:M) | 11:4 | 7:3 |
| DAS28 | 2.95 ± 0.7 | - |
| Patient global VAS (mm) | 37.69 ± 13.63 | - |
| ESR (mm/h) | 30.6 (5–125) 1 | 8.4 (7–8) |
| CRP (mg/dl) | 6.71 (1.4–66.9) 1 | 2.5 (0–2.5) |
| HAQ | 0.48 (0.1–0.9) | - |
| Characteristics (Mean ± SEM) | RA Subgroup 1 | RA Subgroup 2 |
|---|---|---|
| DAS28 | 3.09 ± 0.2 | 2.49 ± 0.7 |
| Global VAS (mm) | 41.0 ± 0.3 1 | 26.67 ± 1.8 |
| ESR (mm/h) | 36.8 (5–125) | 15.8 (6–27) |
| CRP (mg/dl) | 6.75 (0.4–66.9) | 6.7 (3–9) |
| HAQ | 0.55 (0.1–1.1) | 0.25 (0.1–0.3) |
| NLR | 3.02 ± 0.42 | 3.47 ± 0.12 |
| MLR | 0.38 ± 0.2 | 0.34 ± 0,15 |
| PltLR | 206.94 ± 86.03 | 134.5 ± 33.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mititelu, R.R.; Pădureanu, R.; Băcănoiu, M.; Pădureanu, V.; Docea, A.O.; Calina, D.; Barbulescu, A.L.; Buga, A.M. Inflammatory and Oxidative Stress Markers—Mirror Tools in Rheumatoid Arthritis. Biomedicines 2020, 8, 125. https://doi.org/10.3390/biomedicines8050125
Mititelu RR, Pădureanu R, Băcănoiu M, Pădureanu V, Docea AO, Calina D, Barbulescu AL, Buga AM. Inflammatory and Oxidative Stress Markers—Mirror Tools in Rheumatoid Arthritis. Biomedicines. 2020; 8(5):125. https://doi.org/10.3390/biomedicines8050125
Chicago/Turabian StyleMititelu, Radu Răzvan, Rodica Pădureanu, Manuela Băcănoiu, Vlad Pădureanu, Anca Oana Docea, Daniela Calina, Andreea Lili Barbulescu, and Ana Maria Buga. 2020. "Inflammatory and Oxidative Stress Markers—Mirror Tools in Rheumatoid Arthritis" Biomedicines 8, no. 5: 125. https://doi.org/10.3390/biomedicines8050125