
Development of a Novel Endometrial Signature Based on Endometrial microRNA for Determining the Optimal Timing for Embryo Transfer

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Endometrial Samples
2.2. Ethical Approval
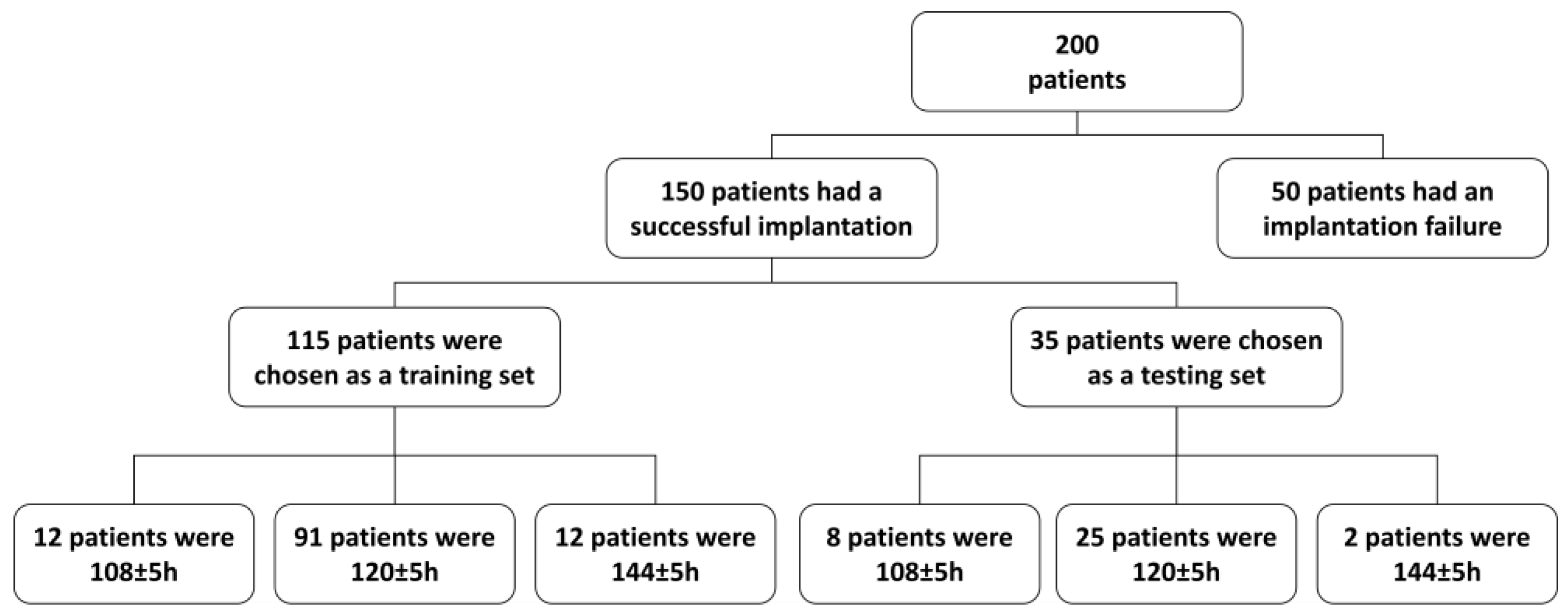
2.3. Study Design
2.4. RNA Extraction and miRNA Enrichment
2.5. cDNA Synthesis
2.6. miRNA Expression Analysis
2.7. Data Processing and Analysis
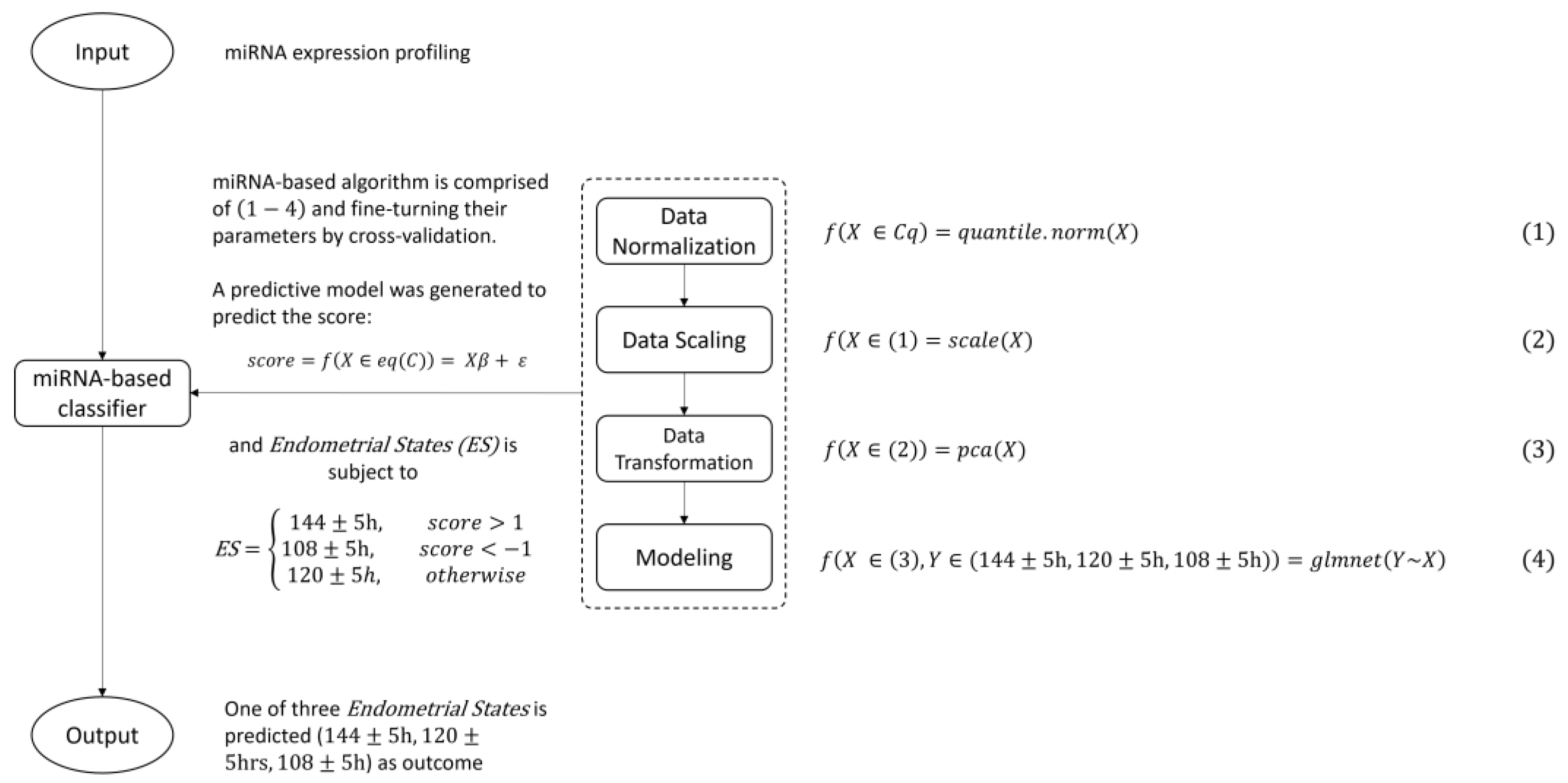
2.8. Model Building
3. Results
3.1. Evaluation of miRNA-Based Classifier’s Performance
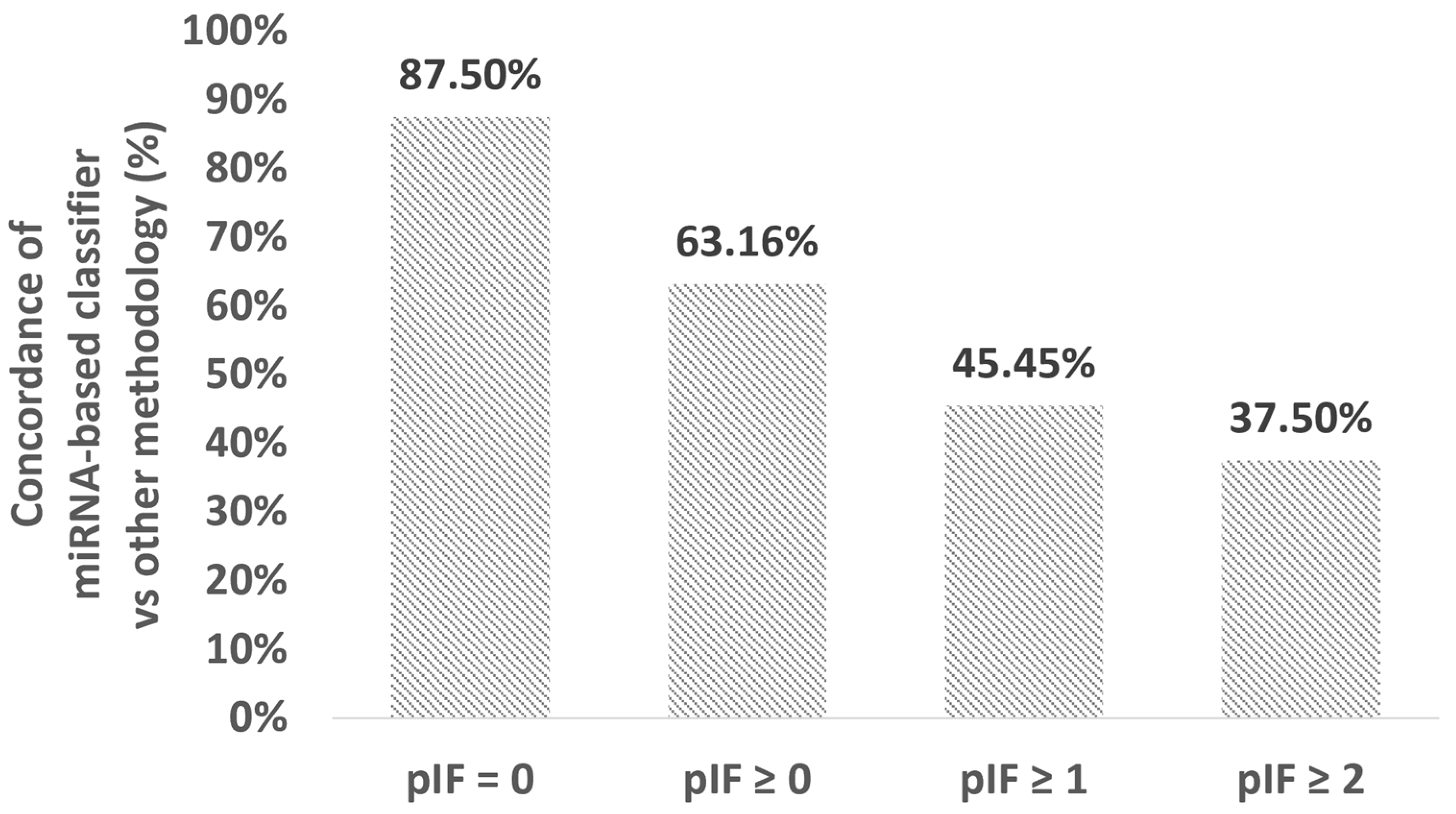
3.2. Analysis of Inconsistent Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ombelet, W.; Cooke, I.; Dyer, S.; Serour, G.; Devroey, P. Infertility and the provision of infertility medical services in developing countries. Hum. Reprod. Update 2008, 14, 605–621. [Google Scholar] [CrossRef]
- Timeva, T.; Shterev, A.; Kyurkchiev, S. Recurrent implantation failure: The role of the endometrium. J. Reprod. Infertil. 2014, 15, 173–183. [Google Scholar]
- Su, R.W.; Fazleabas, A.T. Implantation and Establishment of Pregnancy in Human and Nonhuman Primates. In Regulation of Implantation and Establishment of Pregnancy in Mammals; Advances in Anatomy, Embryology and Cell Biology; Springer: Cham, Switzerland, 2015; Volume 216, pp. 189–213. [Google Scholar] [CrossRef]
- Lessey, B.A. Assessment of endometrial receptivity. Fertil. Steril. 2011, 96, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Sebastian-Leon, P.; Garrido, N.; Remohi, J.; Pellicer, A.; Diaz-Gimeno, P. Asynchronous and pathological windows of implantation: Two causes of recurrent implantation failure. Hum. Reprod. 2018, 33, 626–635. [Google Scholar] [CrossRef]
- Mahajan, N.; Kaur, S.; Alonso, M.R. Window of Implantation is Significantly Displaced in Patients with Adenomyosis with Previous Implantation Failure as Determined by Endometrial Receptivity Assay. J. Hum. Reprod. Sci. 2018, 11, 353–358. [Google Scholar] [CrossRef]
- Acosta, A.A.; Elberger, L.; Borghi, M.; Calamera, J.C.; Chemes, H.; Doncel, G.F.; Kliman, H.; Lema, B.; Lustig, L.; Papier, S. Endometrial dating and determination of the window of implantation in healthy fertile women. Fertil. Steril. 2000, 73, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.L. Three-dimensional ultrasound assessment of endometrial receptivity: A review. Reprod. Biol. Endocrinol. 2006, 4, 56. [Google Scholar] [CrossRef]
- Child, T.J.; Gulekli, B.; Sylvestre, C.; Tan, S.L. Ultrasonographic assessment of endometrial receptivity at embryo transfer in an in vitro maturation of oocyte program. Fertil. Steril. 2003, 79, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Kupesic, S.; Bekavac, I.; Bjelos, D.; Kurjak, A. Assessment of endometrial receptivity by transvaginal color Doppler and three-dimensional power Doppler ultrasonography in patients undergoing in vitro fertilization procedures. J. Ultrasound Med. 2001, 20, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Lilic, V.; Tubic-Pavlovic, A.; Radovic-Janosevic, D.; Petric, A.; Stefanovic, M.; Zivadinovic, R. Assessment of endometrial receptivity by color Doppler and ultrasound imaging. Med. Pregl. 2007, 60, 237–240. [Google Scholar] [CrossRef]
- Check, J.H.; Lurie, D.; Dietterich, C.; Callan, C.; Baker, A. Adverse effect of a homogeneous hyperechogenic endometrial sonographic pattern, despite adequate endometrial thickness on pregnancy rates following in-vitro fertilization. Hum. Reprod. 1993, 8, 1293–1296. [Google Scholar] [CrossRef]
- Coulam, C.B.; Bustillo, M.; Soenksen, D.M.; Britten, S. Ultrasonographic predictors of implantation after assisted reproduction. Fertil. Steril. 1994, 62, 1004–1010. [Google Scholar] [CrossRef]
- Schild, R.L.; Indefrei, D.; Eschweiler, S.; Van der Ven, H.; Fimmers, R.; Hansmann, M. Three-dimensional endometrial volume calculation and pregnancy rate in an in-vitro fertilization programme. Hum. Reprod. 1999, 14, 1255–1258. [Google Scholar] [CrossRef] [PubMed]
- Ueno, J.; Oehninger, S.; Brzyski, R.G.; Acosta, A.A.; Philput, C.B.; Muasher, S.J. Ultrasonographic appearance of the endometrium in natural and stimulated in-vitro fertilization cycles and its correlation with outcome. Hum. Reprod. 1991, 6, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Lindhard, A.; Ravn, V.; Bentin-Ley, U.; Horn, T.; Bangsboell, S.; Rex, S.; Toft, B.; Soerensen, S. Ultrasound characteristics and histological dating of the endometrium in a natural cycle in infertile women compared with fertile controls. Fertil. Steril. 2006, 86, 1344–1355. [Google Scholar] [CrossRef] [PubMed]
- Brosens, J.J.; Salker, M.S.; Teklenburg, G.; Nautiyal, J.; Salter, S.; Lucas, E.S.; Steel, J.H.; Christian, M.; Chan, Y.W.; Boomsma, C.M.; et al. Uterine selection of human embryos at implantation. Sci. Rep. 2014, 4, 3894. [Google Scholar] [CrossRef]
- Diaz-Gimeno, P.; Horcajadas, J.A.; Martinez-Conejero, J.A.; Esteban, F.J.; Alama, P.; Pellicer, A.; Simon, C. A genomic diagnostic tool for human endometrial receptivity based on the transcriptomic signature. Fertil. Steril. 2011, 95, 50–60.e15. [Google Scholar] [CrossRef] [PubMed]
- Kao, L.C.; Tulac, S.; Lobo, S.; Imani, B.; Yang, J.P.; Germeyer, A.; Osteen, K.; Taylor, R.N.; Lessey, B.A.; Giudice, L.C. Global gene profiling in human endometrium during the window of implantation. Endocrinology 2002, 143, 2119–2138. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.H.; Chang, W.A.; Tsai, E.M.; Tsai, M.J.; Kuo, P.L. Investigating Novel Genes Potentially Involved in Endometrial Adenocarcinoma using Next-Generation Sequencing and Bioinformatic Approaches. Int. J. Med. Sci. 2019, 16, 1338–1348. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, P.; Frommolt, P. Challenges in the Setup of Large-scale Next-Generation Sequencing Analysis Workflows. Comput. Struct. Biotechnol. J. 2017, 15, 471–477. [Google Scholar] [CrossRef]
- Di Resta, C.; Ferrari, M. Next Generation Sequencing: From Research Area to Clinical Practice. EJIFCC 2018, 29, 215–220. [Google Scholar]
- Simoneau, J.; Dumontier, S.; Gosselin, R.; Scott, M.S. Current RNA-seq methodology reporting limits reproducibility. Brief. Bioinform. 2021, 22, 140–145. [Google Scholar] [CrossRef]
- Mandelboum, S.; Manber, Z.; Elroy-Stein, O.; Elkon, R. Recurrent functional misinterpretation of RNA-seq data caused by sample-specific gene length bias. PLoS Biol. 2019, 17, e3000481. [Google Scholar] [CrossRef]
- Liang, J.; Wang, S.; Wang, Z. Role of microRNAs in embryo implantation. Reprod. Biol. Endocrinol. 2017, 15, 90. [Google Scholar] [CrossRef]
- Garrido-Gomez, T.; Ruiz-Alonso, M.; Blesa, D.; Diaz-Gimeno, P.; Vilella, F.; Simon, C. Profiling the gene signature of endometrial receptivity: Clinical results. Fertil. Steril. 2013, 99, 1078–1085. [Google Scholar] [CrossRef]
- Gregory, P.A.; Bert, A.G.; Paterson, E.L.; Barry, S.C.; Tsykin, A.; Farshid, G.; Vadas, M.A.; Khew-Goodall, Y.; Goodall, G.J. The miR-200 family and miR-205 regulate epithelial to mesenchymal transition by targeting ZEB1 and SIP1. Nat. Cell Biol. 2008, 10, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Korpal, M.; Lee, E.S.; Hu, G.; Kang, Y. The miR-200 family inhibits epithelial-mesenchymal transition and cancer cell migration by direct targeting of E-cadherin transcriptional repressors ZEB1 and ZEB2. J. Biol. Chem. 2008, 283, 14910–14914. [Google Scholar] [CrossRef] [PubMed]
- Lam, E.W.; Shah, K.; Brosens, J.J. The diversity of sex steroid action: The role of micro-RNAs and FOXO transcription factors in cycling endometrium and cancer. J. Endocrinol. 2012, 212, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Lees, M.; Matthews, L.C.; Kimber, S.J.; Forbes, K.; Aplin, J.D. MiR-145 suppresses embryo-epithelial juxtacrine communication at implantation by modulating maternal IGF1R. J. Cell Sci. 2015, 128, 804–814. [Google Scholar] [CrossRef]
- Altmae, S.; Martinez-Conejero, J.A.; Esteban, F.J.; Ruiz-Alonso, M.; Stavreus-Evers, A.; Horcajadas, J.A.; Salumets, A. MicroRNAs miR-30b, miR-30d, and miR-494 regulate human endometrial receptivity. Reprod. Sci. 2013, 20, 308–317. [Google Scholar] [CrossRef]
- Revel, A.; Achache, H.; Stevens, J.; Smith, Y.; Reich, R. MicroRNAs are associated with human embryo implantation defects. Hum. Reprod. 2011, 26, 2830–2840. [Google Scholar] [CrossRef]
- Shi, C.; Shen, H.; Fan, L.J.; Guan, J.; Zheng, X.B.; Chen, X.; Liang, R.; Zhang, X.W.; Cui, Q.H.; Sun, K.K.; et al. Endometrial MicroRNA Signature during the Window of Implantation Changed in Patients with Repeated Implantation Failure. Chin. Med. J. 2017, 130, 566–573. [Google Scholar] [CrossRef]
- Chen, C.H.; Lu, F.; Yang, W.J.; Yang, P.E.; Chen, W.M.; Kang, S.T.; Huang, Y.S.; Kao, Y.C.; Feng, C.T.; Chang, P.C.; et al. A novel platform for discovery of differentially expressed microRNAs in patients with repeated implantation failure. Fertil. Steril. 2021, 116, 181–188. [Google Scholar] [CrossRef]
- Kang, S.T.; Hsieh, Y.S.; Feng, C.T.; Chen, Y.T.; Yang, P.E.; Chen, W.M. miPrimer: An empirical-based qPCR primer design method for small noncoding microRNA. RNA 2018, 24, 304–312. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Chen, W.M.; Hsieh, Y.S.; Fan, Y.C.; Yang, P.E.; Kang, S.T.; Liao, C.T. A Novel Multi-Gene Detection Platform for the Analysis of miRNA Expression. Sci. Rep. 2018, 8, 10684. [Google Scholar] [CrossRef] [PubMed]
- Bolstad, B.M.; Irizarry, R.A.; Astrand, M.; Speed, T.P. A comparison of normalization methods for high density oligonucleotide array data based on variance and bias. Bioinformatics 2003, 19, 185–193. [Google Scholar] [CrossRef]
- Mestdagh, P.; Hartmann, N.; Baeriswyl, L.; Andreasen, D.; Bernard, N.; Chen, C.; Cheo, D.; D’Andrade, P.; DeMayo, M.; Dennis, L.; et al. Evaluation of quantitative miRNA expression platforms in the microRNA quality control (miRQC) study. Nat. Methods 2014, 11, 809–815. [Google Scholar] [CrossRef]
- Pechenizkiy, M.; Tsymbal, A.; Puuronen, S. PCA-Based Feature Transformation for Classification: Issues in Medical Diagnostics. In Proceedings of the 17th IEEE Symposium on Computer-Based Medical Systems, Bethesda, MD, USA, 25 June 2004; pp. 535–540. [Google Scholar] [CrossRef]
- Zou, H.; Hastie, T. Regularization and variable selection via the Elastic Net. J. R. Stat. Soc. Ser. B 2005, 67, 20. [Google Scholar]
- Huang, H.Y.; Lin, Y.C.; Li, J.; Huang, K.Y.; Shrestha, S.; Hong, H.C.; Tang, Y.; Chen, Y.G.; Jin, C.N.; Yu, Y.; et al. miRTarBase 2020: Updates to the experimentally validated microRNA-target interaction database. Nucleic Acids Res. 2020, 48, D148–D154. [Google Scholar] [CrossRef] [PubMed]
- Kaya, I.E.; Pehlivanli, A.C.; Sekizkardes, E.G.; Ibrikci, T. PCA based clustering for brain tumor segmentation of T1w MRI images. Comput. Methods Programs Biomed. 2017, 140, 19–28. [Google Scholar] [CrossRef]
- Carbon, S.; Ireland, A.; Mungall, C.J.; Shu, S.; Marshall, B.; Lewis, S.; Ami, G.O.H.; Web Presence Working, G. AmiGO: Online access to ontology and annotation data. Bioinformatics 2009, 25, 288–289. [Google Scholar] [CrossRef] [PubMed]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Herington, J.L.; Guo, Y.; Reese, J.; Paria, B.C. Gene profiling the window of implantation: Microarray analyses from human and rodent models. J. Reprod. Health Med. 2016, 2, S19–S25. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.; Tan, S.; Buckett, W.; Dahan, M.H. Intra-patient variability in the endometrial receptivity assay (ERA) test. J. Assist. Reprod. Genet. 2018, 35, 929–930. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, Y.; Naji, O.; Saso, S.; Pexsters, A.; Stalder, C.; Sur, S.; Raine-Fenning, N.; Timmerman, D.; Brosens, J.J.; Bourne, T. Ultrasound assessment of the peri-implantation uterus: A review. Ultrasound Obstet. Gynecol. 2012, 39, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Copois, V.; Bibeau, F.; Bascoul-Mollevi, C.; Salvetat, N.; Chalbos, P.; Bareil, C.; Candeil, L.; Fraslon, C.; Conseiller, E.; Granci, V.; et al. Impact of RNA degradation on gene expression profiles: Assessment of different methods to reliably determine RNA quality. J. Biotechnol. 2007, 127, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Fleige, S.; Pfaffl, M.W. RNA integrity and the effect on the real-time qRT-PCR performance. Mol. Asp. Med. 2006, 27, 126–139. [Google Scholar] [CrossRef]
- Peiro-Chova, L.; Pena-Chilet, M.; Lopez-Guerrero, J.A.; Garcia-Gimenez, J.L.; Alonso-Yuste, E.; Burgues, O.; Lluch, A.; Ferrer-Lozano, J.; Ribas, G. High stability of microRNAs in tissue samples of compromised quality. Virchows Arch. 2013, 463, 765–774. [Google Scholar] [CrossRef]
- Opitz, L.; Salinas-Riester, G.; Grade, M.; Jung, K.; Jo, P.; Emons, G.; Ghadimi, B.M.; Beissbarth, T.; Gaedcke, J. Impact of RNA degradation on gene expression profiling. BMC Med. Genom. 2010, 3, 36. [Google Scholar] [CrossRef]
- Tan, J.; Kan, A.; Hitkari, J.; Taylor, B.; Tallon, N.; Warraich, G.; Yuzpe, A.; Nakhuda, G. The role of the endometrial receptivity array (ERA) in patients who have failed euploid embryo transfers. J. Assist. Reprod. Genet. 2018, 35, 683–692. [Google Scholar] [CrossRef]
- Bashiri, A.; Halper, K.I.; Orvieto, R. Recurrent Implantation Failure-update overview on etiology, diagnosis, treatment and future directions. Reprod. Biol. Endocrinol. 2018, 16, 121. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training Set (N = 115) | Testing Set (N = 35) | ||||
|---|---|---|---|---|---|---|
| 108 ± 5 h | 120 ± 5 h | 144 ± 5 h | 108 ± 5 h | 120 ± 5 h | 144 ± 5 h | |
| (N = 12) | (N = 91) | (N = 12) | (N = 8) | (N = 25) | (N = 2) | |
| Age (years) | ||||||
| Mean (SD) | 36.1 (±2.8) | 36.5 (±4.2) | 39.8 (±4.6) | 35 (±3) | 38.6 (±4.4) | 42.5 (±6.1) |
| Range | 32–40 | 23–47 | 31–46 | 31–39 | 30–47 | 32–50 |
| No. of previous implantation failure (#1) | ||||||
| Mean (SD) | 1.3 (±1.5) | 0.3 (±0.8) | 0.2 (±0.4) | 1.3 (±2) | 1 (±1.3) | 1 (±0.9) |
| Range | 0–5 | 0–4 | 0–1 | 0–5 | 0–5 | 0–3 |
| Body mass index (BMI) | ||||||
| Mean (SD) | 20.7 (±1.4) | 22.3 (±3.4) | 22.9 (±3.2) | 22.7 (±1.8) | 22.8 (±2.9) | 22.2 (±2.9) |
| Range | 18.6–23.1 | 16.9–32 | 17.7–28.9 | 20.5–26.2 | 18–29.3 | 17.9–28.4 |
| P4 Level (ng/mL) before exogenous progesterone administration | ||||||
| Mean (SD) | 0.3 (±0.3) | 0.3 (±0.1) | 0.3 (±0.1) | 0.5 (±0.7) | 0.3 (±0.2) | 0.5 (±0) |
| Range | 0.15–1.1 | 0.1–0.7 | 0.05–0.5 | 0.15–2.2 | 0.15–0.74 | 0.05–0.5 |
| Endometrial thickness (mm) | ||||||
| Mean (SD) | 10 (±2.6) | 10.7 (±2.4) | 10.1 (±2.4) | 10.1 (±2.3) | 10.4 (±2.5) | 9.6 (±1.9) |
| Range | 6.05–15.1 | 5.8–20.9 | 7–15 | 7.7–14.2 | 7.2–19.2 | 7.9–14.9 |
| A normal uterine cavity by office hysteroscopy | Yes | Yes | Yes | Yes | Yes | Yes |
| Actual Class (Training Set) | |||||||||
| 108 ± 5 h | 120 ± 5 h | 144 ± 5h | SEN | SPE | PPV | NPV | ACC | ||
| Predicted Class | 108 ± 5 h | 9 | 1 | 0 | 75.00% | 99.03% | 90.00% | 97.14% | - |
| 120 ± 5 h | 3 | 89 | 2 | 97.80% | 79.17% | 94.68% | 90.48% | - | |
| 144 ± 5 h | 0 | 1 | 10 | 83.33% | 99.03% | 90.91% | 98.08% | - | |
| 85.38% | 92.41% | 91.86% | 95.23% | 93.91% | |||||
| Actual Class (Testing Set) | |||||||||
| 108 ± 5 h | 120 ± 5 h | 144 ± 5 h | SEN | SPE | PPV | NPV | ACC | ||
| Predicted Class | 108 ± 5 h | 7 | 1 | 0 | 87.50% | 96.30% | 87.50% | 96.30% | - |
| 120 ± 5 h | 1 | 23 | 1 | 92.00% | 80.00% | 92.00% | 80.00% | - | |
| 144 ± 5 h | 0 | 1 | 1 | 50.00% | 96.97% | 50.00% | 96.97% | - | |
| 76.50% | 91.09% | 76.50% | 91.09% | 88.57% | |||||
| 108 ± 5 h = the optimal time of 108 h (±5 h) for embryo transfer. 120 ± 5 h = the optimal time of 120 h (±5 h) for embryo transfer. 144 ± 5 h = the optimal time of 144 h (±5 h) for embryo transfer. Actual Class = the actual clinical status of the subjects. Predicted Class = the predicted clinical status of the subjects using the algorithm. TP = True Positives. FP = False Positives. FN = False Negatives. TN = True Negatives. Sensitivity (SEN) = TP / (TP + FN). Specificity (SPE) = TN / (TN + FP). Positive Predictive Value (PPV) = TP / (TP + FP). Negative Predictive Value (NPV) = TN / (TN + FN). Accuracy (ACC) = (TP + TN) / (TP + FP + TN + FN) | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Lu, F.; Yang, W.-J.; Chen, W.-M.; Yang, P.E.; Kang, S.-T.; Wang, T.; Chang, P.-C.; Feng, C.-T.; Yang, J.-H.; et al. Development of a Novel Endometrial Signature Based on Endometrial microRNA for Determining the Optimal Timing for Embryo Transfer. Biomedicines 2024, 12, 700. https://doi.org/10.3390/biomedicines12030700
Chen C-H, Lu F, Yang W-J, Chen W-M, Yang PE, Kang S-T, Wang T, Chang P-C, Feng C-T, Yang J-H, et al. Development of a Novel Endometrial Signature Based on Endometrial microRNA for Determining the Optimal Timing for Embryo Transfer. Biomedicines. 2024; 12(3):700. https://doi.org/10.3390/biomedicines12030700
Chicago/Turabian StyleChen, Ching-Hung, Farn Lu, Wen-Jui Yang, Wei-Ming Chen, Pok Eric Yang, Shih-Ting Kang, Tiffany Wang, Po-Chang Chang, Chi-Ting Feng, Jung-Hsuan Yang, and et al. 2024. "Development of a Novel Endometrial Signature Based on Endometrial microRNA for Determining the Optimal Timing for Embryo Transfer" Biomedicines 12, no. 3: 700. https://doi.org/10.3390/biomedicines12030700