
Plasma Somatostatin Levels Increase during Scoliosis Surgery, but Not Herniated Disc Operations: Results of a Pilot Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgical Treatment for Scoliosis, Disc Hernia, and Visual Analog Scale (VAS)
2.3. Medication
2.4. Blood Sampling
2.5. Determining Plasma SST-LI by RIA
2.6. Statistical Analysis
3. Results
3.1. Pain Intensity Significantly Increases and Positively Correlates with the Cobb Angle after Scoliosis Surgery
3.2. Plasma SST-LI Significantly Increases and Negatively Correlates with the Initial Cobb Angle in Scoliosis Surgery
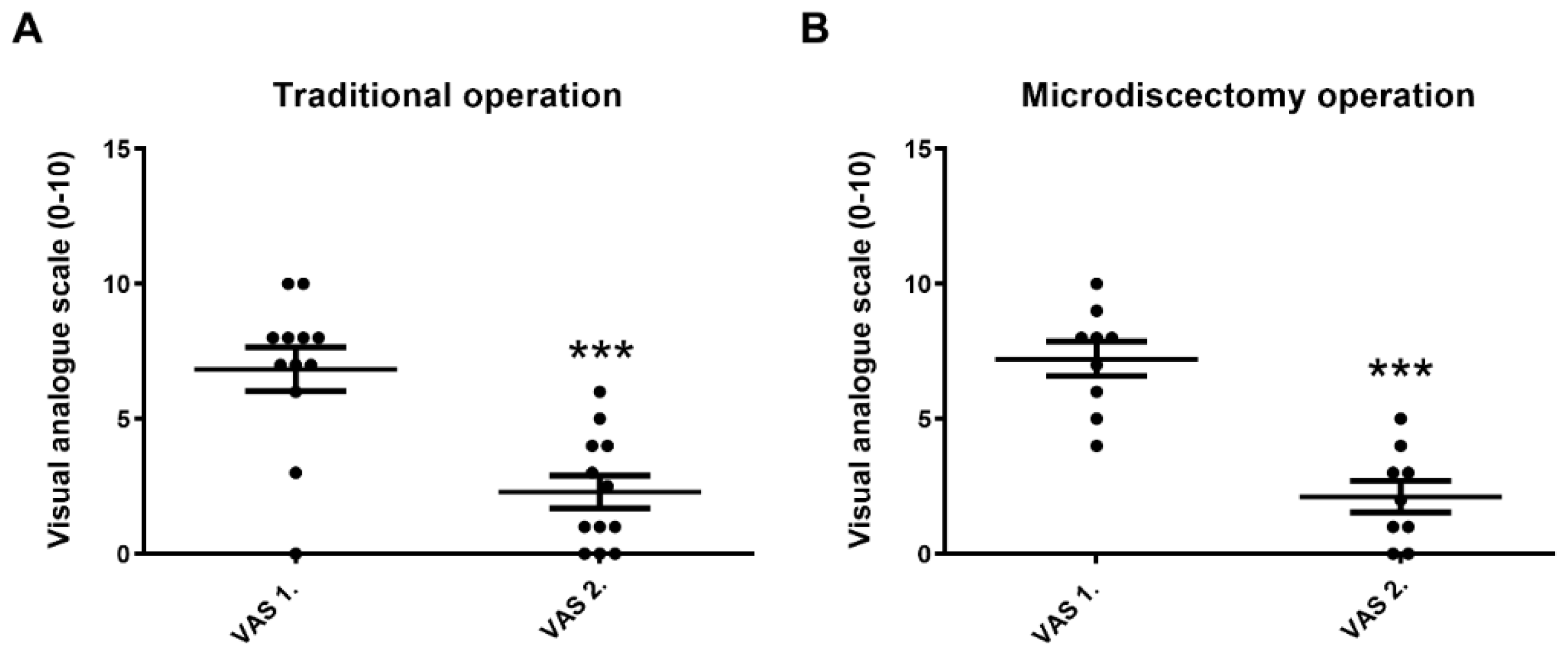
3.3. VAS 2. Significantly Decreases in Both Traditional and Microdiscectomy Groups after Disc Hernia Surgery
3.4. Plasma SST-LI Does Not Change Significantly after Traditional or after Microdiscectomy Type of Disc Hernia Operations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Glossary
References
- Pintér, E.; Szolcsányi, J. Plasma extravasation in the skin and pelvic organs evoked by antidromic stimulation of the lumbosacral dorsal roots of the rat. Neuroscience 1995, 68, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Maggi, C.A. Tachykinins and calcitonin gene-related peptide (CGRP) as cotransmitters released from peripheral endings of sensory nerves. Prog. Neurobiol. 1995, 45, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Szolcsányi, J. Forty years in capsaicin research for sensory pharmacology and physiology. Neuropeptides 2004, 38, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Than, M.; Németh, J.; Szilvassy, Z.; Pintér, E.; Helyes, Z.; Szolcsányi, J. Systemic anti-inflammatory effect of somatostatin released from capsaicin-sensitive vagal and sciatic sensory fibres of the rat and guinea-pig. Eur. J. Pharmacol. 2000, 399, 251–258. [Google Scholar] [CrossRef]
- Szolcsányi, J.; Pintér, E.; Helyes, Z.; Oroszi, G.; Németh, J. Systemic anti-inflammatory effect induced by counter-irritation through a local release of somatostatin from nociceptors. Br. J. Pharmacol. 1998, 125, 916–922. [Google Scholar] [CrossRef] [Green Version]
- Szolcsányi, J.; Helyes, Z.; Oroszi, G.; Németh, J.; Pintér, E. Release of somatostatin and its role in the mediation of the anti-inflammatory effect induced by antidromic stimulation of sensory fibres of rat sciatic nerve. Br. J. Pharmacol. 1998, 123, 936–942. [Google Scholar] [CrossRef] [Green Version]
- Karalis, K.; Mastorakos, G.; Chrousos, G.P.; Tolis, G. Somatostatin analogues suppress the inflammatory reaction in vivo. J. Clin. Investig. 1994, 93, 2000–2006. [Google Scholar] [CrossRef] [Green Version]
- Patel, Y.C. Somatostatin and its receptor family. Front. Neuroendocrinol. 1999, 20, 157–198. [Google Scholar] [CrossRef]
- Selmer, I.; Schindler, M.; Allen, J.P.; Humphrey, P.P.; Emson, P.C. Advances in understanding neuronal somatostatin receptors. Regul. Pept. 2000, 90, 1–18. [Google Scholar] [CrossRef]
- Yamada, Y.; Kagimoto, S.; Kubota, A.; Yasuda, K.; Masuda, K.; Someya, Y.; Ihara, Y.; Li, Q.; Imura, H.; Seino, S.; et al. Cloning, functional expression and pharmacological characterization of fourth (hSSTR4) and fifth (hSSTR5) human somatostatin receptor subtype. Biochem. Biophys. Res. Commun. 1993, 195, 844–852. [Google Scholar] [CrossRef]
- Helyes, Z.; Szabó, A.; Németh, J.; Jakab, B.; Pintér, E.; Bánvölgyi, A.; Kereskai, L.; Kéri, G.; Szolcsányi, J. Anti-inflammatory and analgesic effects of somatostatin released from capsaicin-sensitive sensory nerve terminals in Freund’s adjuvant-induced chronic arthritis model of the rat. Arthritis Rheum. 2004, 50, 1677–1685. [Google Scholar] [CrossRef]
- Sütő, B.; Bagoly, T.; Börzsei, R.; Lengl, O.; Szolcsányi, J.; Németh, T.; Lobil, C.; Bardonicsek, Z.; Pinter, E. Surgery and sepsis increase somatostatin-like immunoreactivity in the human plasma. Peptides 2010, 31, 1208–1212. [Google Scholar] [CrossRef]
- Sütő, B.; Szitter, I.; Bagoly, T.; Pintér, E.; Szolcsányi, J.; Loibl, C.; Nemeth, T.; Tanczos, K.; Molnar, T.; Leiner, T.; et al. Plasma somatostatin-like immunoreactivity increases in the plasma of septic patients and rats with systemic inflammatory reaction: Experimental evidence for its sensory origin and protective role. Peptides 2014, 54, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Szolcsányi, J.; Pintér, E.; Helyes, Z.; Pethő, G. Inhibition of the function of TRPV1-expressing nociceptive sensory neurons by somatostatin 4 receptor agonism: Mechanism and therapeutical implications. Curr. Top. Med. Chem. 2011, 11, 2253–2263. [Google Scholar] [CrossRef] [PubMed]
- Pethő, G.; Bölcskei, K.; Füredi, R.; Botz, B.; Bagoly, T.; Pintér, E.; Szolcsányi, J. Evidence for a novel, neurohumoral antinociceptive mechanism mediated by peripheral capsaicin-sensitive nociceptors in conscious rats. Neuropeptides 2017, 62, 1–10. [Google Scholar] [CrossRef]
- Helyes, Z.; Thán, M.; Oroszi, G.; Pintér, E.; Németh, J.; Kéri, G.; Szolcsányi, J. Anti-nociceptive effect induced by somatostatin released from sensory nerve terminals and by synthetic somatostatin analogs in the rat. Neurosci. Lett. 2000, 278, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Elekes, K.; Helyes, Z.; Kereskai, L.; Sándor, K.; Pintér, E.; Pozsgai, G.; Tékus, V.; Bánvölgyi, A.; Németh, J.; Szuts, T.; et al. Inhibitory effects of synthetic somatostatin receptor subtype 4 agonists on acute and chronic airway inflammation and hyperreactivity in the mouse. Eur. J. Pharmacol. 2008, 578, 313–322. [Google Scholar] [CrossRef]
- Liu, R.; Wei, N.; Guo, W.; Qiang, O.; Li, X.; Ou, Y.; Huang, W.; Tang, C.W. Octreotide alleviates obesity by reducing intestinal glucose absorption and inhibiting low-grade inflammation. Eur. J. Nutr. 2013, 52, 1067–1075. [Google Scholar] [CrossRef]
- Takahashi, M.; Takeda, M.; Matsumoto, S. Somatostatin enhances tooth-pulp-evoked cervical dorsal horn neuronal activity in the rat via inhibition of GABAergic interneurons. Brain Res. Bull. 2014, 100, 76–83. [Google Scholar] [CrossRef]
- Chatterjee, J.; Laufer, B.; Beck, J.G.; Helyes, Z.; Pintér, E.; Szolcsányi, J.; Horváth, A.; Mandl, J.; Reubi, J.C.; Kéri, G.; et al. N-Methylated sst2 Selective Somatostatin Cyclic Peptide Analogue as a Potent Candidate for Treating Neurogenic Inflammation. ACS Med. Chem. Lett. 2011, 2, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Arias-Díaz, J.; Vara, E.; Torres-Melero, J.; García, C.; Hernández, J.; Balibrea, J.L. Local production of oxygen free radicals and nitric oxide in rat diaphragm during sepsis: Effects of pentoxifylline and somatostatin. Eur. J. Surg. 1997, 163, 619–625. [Google Scholar] [PubMed]
- Zhang, Y.S.; Zhao, G.H.; Ding, L.; Liang, L.; Wang, M.H. Effect of treatment with somatostatin on sepsis in rats. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2004, 16, 364–365. [Google Scholar]
- Zhu, T.J.; Dong, G.R.; Huang, G.Q.; Fan, X.P.; Liu, B.; Zhang, Z.L. The effects of somatostatin on serum interleukin-6 and tumor necrosis factor-alpha in lipopolysaccharide-induced septic shock: Experiment with rats. Zhonghua Yi Xue Za Zhi 2007, 87, 345–347. [Google Scholar] [PubMed]
- Antal, A.; Németh, J.; Szolcsányi, J.; Pozsgai, G.; Pintér, E. Abdominal surgery performed under general anesthesia increases somatostatin-like immunoreactivity in human serum. Neuroimmunomodulation 2008, 15, 153–156. [Google Scholar] [CrossRef]
- Boros, M.; Kemény, Á.; Sebők, B.; Bagoly, T.; Perkecz, A.; Petőházi, Z.; Maász, G.; Schmidt, J.; Márk, L.; László, T.; et al. Sulphurous medicinal waters increase somatostatin release; it is a possible mechanism of anti-inflammatory effect of balneotherapy in psoriasis. Eur. J. Integr. Med. 2013, 5, 109–118. [Google Scholar] [CrossRef]
- Németh, J.; Helyes, Z.; Görcs, T.; Gardi, J.; Pintér, E.; Szolcsányi, J. Development of somatostatin radioimmunoassay for the measurement of plasma and tissue contents of hormone. Acta Physiol. Hung. 1996, 84, 313–315. [Google Scholar] [PubMed]
- Abdel-Magid, A.F. Treating pain with somatostatin receptor subtype 4 agonists. ACS Med. Chem. Lett. 2015, 6, 110–111. [Google Scholar] [CrossRef] [Green Version]
- Corsi, M.M.; Ticozzi, C.; Netti, C.; Fulgenzi, A.; Tiengo, M.; Gaja, G.; Guidobono, F.; Ferrero, M.E. The effect of somatostatin on experimental inflammation in rats. Anesth. Analg. 1997, 85, 1112–1115. [Google Scholar] [CrossRef]
- Wang, J.; Tian, W.; Wang, S.; Wei, W.; Wu, D.; Wang, H.; Wang, L.; Yang, R.; Ji, A.; Li, Y. Anti-inflammatory and retinal protective effects of capsaicin on ischaemia-induced injuries through the release of endogenous somatostatin. Clin. Exp. Pharmacol. Physiol. 2017, 44, 803–814. [Google Scholar] [CrossRef]
- Tsuda, K.; Sakurai, H.; Seino, Y.; Seino, S.; Tanigawa, K.; Kuzuya, H.; Imura, H. Somatostatin-like immunoreactivity in human peripheral plasma measured by radioimmunoassay following affinity chromatography. Diabetes 1981, 30, 471–474. [Google Scholar] [CrossRef]
- Barczewska, M.; Juranek, J.; Wojtkiewicz, J. Origins and Neurochemical Characteristics of Porcine Intervertebral Disc Sympathetic Innervation: A Preliminary Report. J. Mol. Neurosci. 2017, 63, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, C.A.; Gao, X.; Shoemaker, S.; Gordon, D.; Herring, J.A. Understanding Genetic Factors in Idiopathic Scoliosis, a Complex Disease of Childhood. Curr. Genomics 2008, 9, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burwell, R.G.; Dangerfield, P.H.; Moulton, A.; Anderson, S.I. Etiologic theories of idiopathic scoliosis: Autonomic nervous system and the leptin-sympathetic nervous system concept for the pathogenesis of adolescent idiopathic scoliosis. Stud. Health Technol. Inform. 2008, 140, 197–207. [Google Scholar]
- Carlton, S.M.; Du, J.; Davidson, E.; Zhou, S.; Coggeshall, R.E. Somatostatin receptors on peripheral primary afferent terminals: Inhibition of sensitized nociceptors. Pain 2001, 90, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Silveri, F.; Morosini, P.; Brecciaroli, D.; Cervini, C. Intra-articular injection of somatostatin in knee osteoarthritis: Clinical results and IGF-1 serum levels. Int. J. Clin. Pharmacol. Res. 1994, 14, 79–85. [Google Scholar] [PubMed]
- Casnici, C.; Lattuada, D.; Crotta, K.; Truzzi, M.C.; Corradini, C.; Ingegnoli, F.; Tonna, N.; Bianco, F.; Marelli, O. Anti-inflammatory Effect of Somatostatin Analogue Octreotide on Rheumatoid Arthritis Synoviocytes. Inflammation 2018, 41, 1648–1660. [Google Scholar] [CrossRef] [PubMed]
- Szőke, É.; Bálint, M.; Hetényi, C.; Markovics, A.; Elekes, K.; Pozsgai, G.; Szűts, T.; Kéri, G.; Őrfi, L.; Sándor, Z.; et al. Small molecule somatostatin receptor subtype 4 (sst4) agonists are novel anti-inflammatory and analgesic drug candidates. Neuropharmacology 2020, 178, 108198. [Google Scholar] [CrossRef]
- Hofland, L.J.; van Hagen, P.M.; Lamberts, S.W. Functional role of somatostatin receptors in neuroendocrine and immune cells. Ann. Med. 1999, 31 (Suppl. S2), 23–27. [Google Scholar]
- Ferone, D.; van Hagen, P.M.; Semino, C.; Dalm, V.A.; Barreca, A.; Colao, A.; Lamberts, S.W.J.; Minuto, F.; Hofland, L.J. Somatostatin receptor distribution and function in immune system. Dig. Liver Dis. 2004, 36 (Suppl. S1), 68–77. [Google Scholar] [CrossRef]
- Ling, L.; Qinghua, T.; Bin, H.; Hao, W.; Chunhui, W.; Rui, L.; Chengwei, T. Somatostatin Improved B Cells Mature in Macaques during Intestinal Ischemia-Reperfusion. PLoS ONE 2015, 10, e0133692. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scoliosis Patients | Disc Hernia Patients (Traditional Group) | Disc Hernia Patients (Microdiscectomy Group) | |
|---|---|---|---|
| Males | 2 | 8 | 5 |
| Females | 7 | 4 | 4 |
| Total | 9 | 12 | 9 |
| Mean age | 18.75 ± 9.06 | 55.2 ± 14.13 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sütő, B.; Kolumbán, B.; Szabó, É.; Pásztor, S.; Németh, T.; Bagoly, T.; Botz, B.; Pintér, E.; Helyes, Z. Plasma Somatostatin Levels Increase during Scoliosis Surgery, but Not Herniated Disc Operations: Results of a Pilot Study. Biomedicines 2023, 11, 2154. https://doi.org/10.3390/biomedicines11082154
Sütő B, Kolumbán B, Szabó É, Pásztor S, Németh T, Bagoly T, Botz B, Pintér E, Helyes Z. Plasma Somatostatin Levels Increase during Scoliosis Surgery, but Not Herniated Disc Operations: Results of a Pilot Study. Biomedicines. 2023; 11(8):2154. https://doi.org/10.3390/biomedicines11082154
Chicago/Turabian StyleSütő, Balázs, Bálint Kolumbán, Éva Szabó, Sára Pásztor, Timea Németh, Teréz Bagoly, Bálint Botz, Erika Pintér, and Zsuzsanna Helyes. 2023. "Plasma Somatostatin Levels Increase during Scoliosis Surgery, but Not Herniated Disc Operations: Results of a Pilot Study" Biomedicines 11, no. 8: 2154. https://doi.org/10.3390/biomedicines11082154