
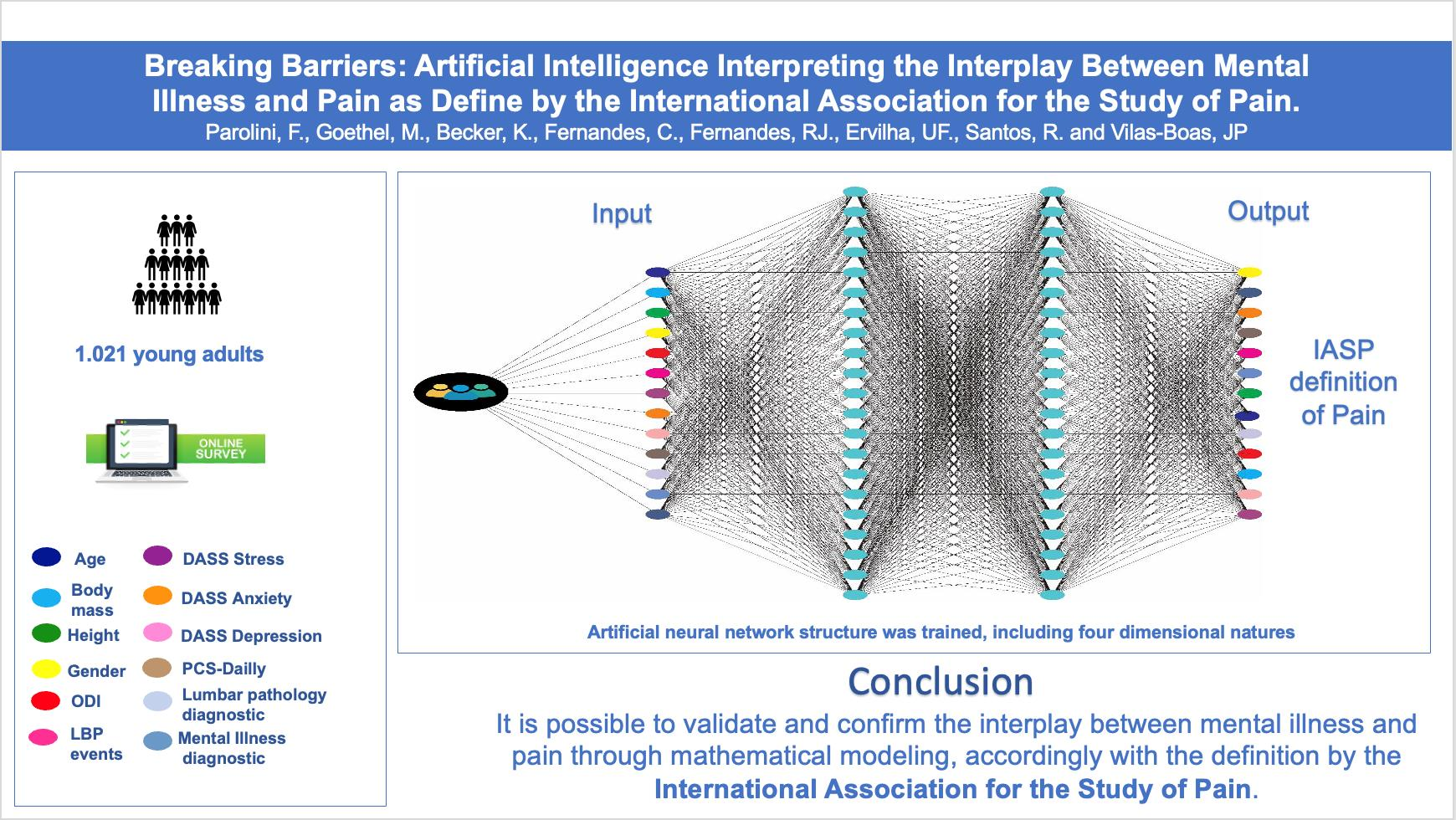
Breaking Barriers: Artificial Intelligence Interpreting the Interplay between Mental Illness and Pain as Defined by the International Association for the Study of Pain

 , ,
, ,  , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Instruments
2.3. Anomaly Detection Structure
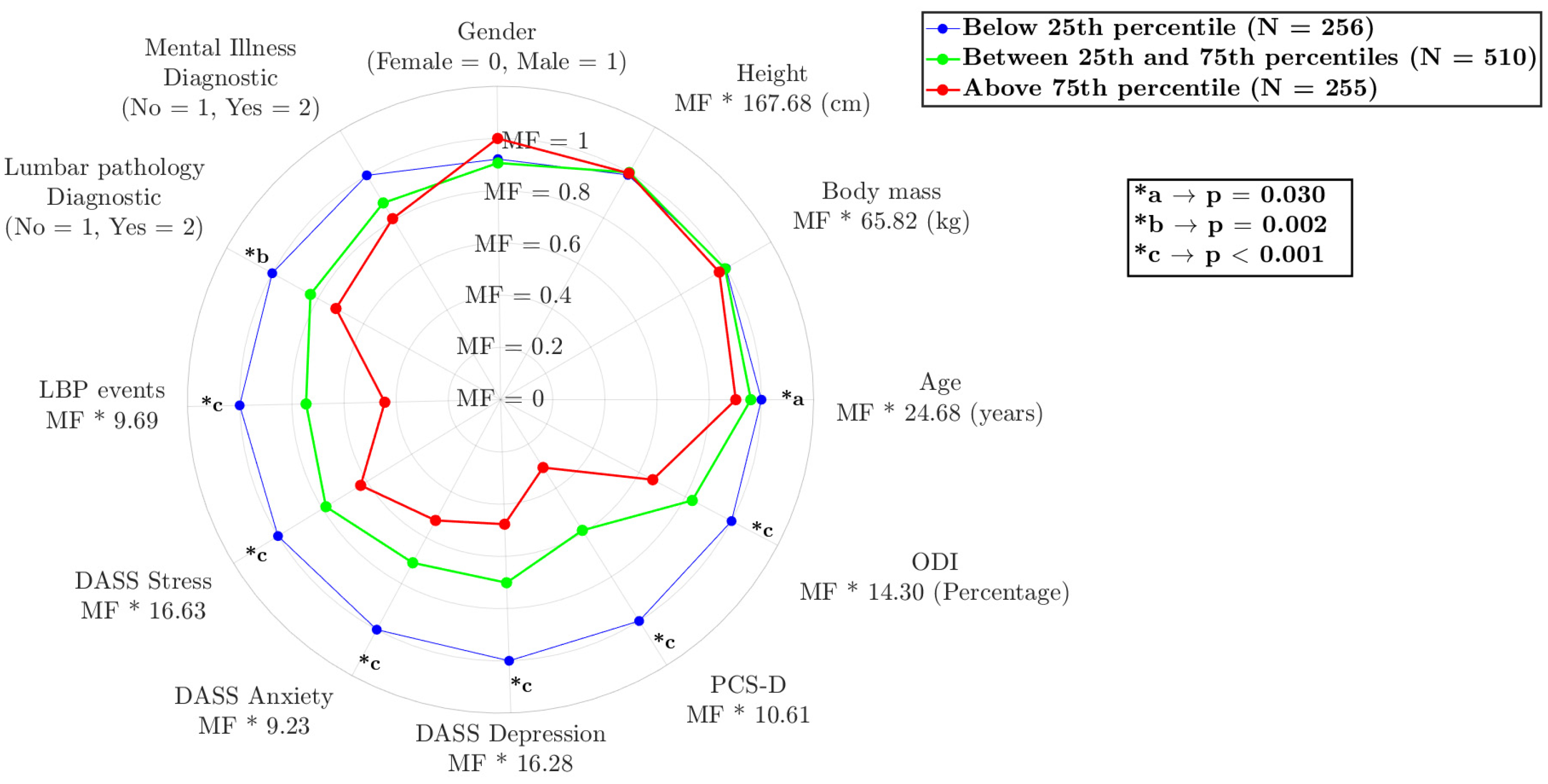
3. Results
Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumley, M.A.; Schubiner, H.; Lockhart, N.A.; Kidwell, K.M.; Harte, S.E.; Clauw, D.J.; Williams, D.A. Emotional awareness and expression therapy, cognitive behavioral therapy, and education for fibromyalgia: A cluster-randomized controlled trial. Pain 2017, 158, 2354–2363. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stein, M.B. Interoception in anxiety and depression. Brain Struct. Funct. 2010, 214, 451–463. [Google Scholar] [CrossRef] [Green Version]
- Mescouto, K.; Olson, R.E.; Hodges, P.W.; Setchell, V. A critical review of the biopsychosocial model of low back pain care: Time for a new approach? Disabil. Rehabil. 2022, 44, 3270–3284. [Google Scholar] [CrossRef] [PubMed]
- Ashar, Y.K.; Gordon, A.; Schubiner, H.; Uipi, C.; Knight, K.; Anderson, Z.; Carlisle, J.; Polisky, L.; Geuter, S.; Flood, T.F.; et al. Effect of Pain Reprocessing Therapy vs. Placebo and Usual Care for Patients with Chronic Back Pain: A Randomized Clinical Trial. JAMA Psychiatry 2022, 79, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Bushnell, M.; Čeko, M.; Low, L. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 2013, 14, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez, L.; Écija, C.; Catalá, P.; Peñacoba, C. Sedentary Behavior and Pain after Physical Activity in Women with Fibromyalgia—The Influence of Pain-Avoidance Goals and Catastrophizing. Biomedicines 2023, 11, 154. [Google Scholar]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, V.; Mogil, J.S.; Ringkamp, M.; Sluka, V.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Lovelace, M.D.; Varney, B.; Sundaram, G.; Franco, N.F.; Ng, M.L.; Pai, S.; Lim, C.K.; Guillemin, G.J.; Brew, B.J. Current Evidence for a Role of the Kynurenine Pathway of Tryptophan Metabolism in Multiple Sclerosis. Front. Immunol. 2016, 7, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, W.Y.; Stohler, C.S.; Herr, D.R. Role of the Prefrontal Cortex in Pain Processing. Mol. Neurobiol. 2019, 56, 1137–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, M.; Török, N.; Tóth, F.; Szabó, Á.; Vécsei, L. Co-Players in Chronic Pain: Neuroinflammation and the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9, 897. [Google Scholar] [CrossRef]
- Okafor, C.; Levin, M.J.; Boadi, P.; Cook, C.; George, S.; Klifto, C.; Anakwenze, O. Pain associated psychological distress is more strongly associated with shoulder pain and function than tear severity in patients undergoing rotator cuff repair. JSES Int. 2023, 7, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; McDermott, M.P.; Peirce-Sandner, S.; Burke, L.B.; Cowan, P.; Farrar, J.T.; Hertz, S.; Raja, S.N.; Rappaport, B.A.; et al. Interpreting the clinical importance of group differences in chronic pain clinical trials: IMMPACT recommendations. Pain 2009, 146, 238–244. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y.; Lindquist, M.A.; Roy, M.; Woo, C.W.; Kross, E. An fMRI-based neurologic signature of physical pain. N. Engl. J. Med. 2013, 15, 1388–1397. [Google Scholar] [CrossRef] [Green Version]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine learning in medicine. N. Engl. J. Med. 2019, 14, 1347–1358. [Google Scholar] [CrossRef]
- Smith, A.B.; Jones, C.D.; Johnson, L.M. Investigating the relationship between mental illness and pain using artificial intelligence: A systematic review. J. Pain Res. 2021, 14, 2385–2397. [Google Scholar]
- Baron, R.; Binder, A.; Wasner, G. Neuropathic pain: Diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol. 2010, 9, 807–819. [Google Scholar] [CrossRef]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Wang, Z.; Zhang, Y.; Wang, G. A Feature-Trajectory-Smoothed High-Speed Model for Video Anomaly Detection. Sensors 2023, 23, 1612. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.C.; Fassa, A.G.; Valle, N.C.J. Chronic low back pain in a Southern Brazilian adult population: Prevalence and associated factors. Cad. Saude Publica 2004, 112, 214–220. [Google Scholar]
- Malhotra, P.; Ramakrishnan, A.; Anand, G.; Vig, L.; Agarwal, P.; Shroff, G. LSTM-based encoder-decoder for multi-sensor anomaly detection. arXiv 2016, arXiv:1607.00148. [Google Scholar]
- Samariya, D.; Ma, D.; Aryal, S.; Zhao, X. Detection and explanation of anomalies in healthcare data. Health Inf. Sci. Syst. 2023, 11, 20. [Google Scholar] [CrossRef]
- Nagireddi, J.N.; Vyas, A.K.; Sanapati, M.R.; Soin, A.; Manchikanti, L. The Analysis of Pain Research through the Lens of Artificial Intelligence and Machine Learning. Pain Physician 2022, 25, 211–243. [Google Scholar]
- Taherdoost, H.; Madanchian, M. Artificial Intelligence and Sentiment Analysis: A Review in Competitive Research. Computers 2023, 12, 37. [Google Scholar] [CrossRef]
- Goethel, M.F.; Gonçalves, M.; Brietzke, C.; Cardozo, A.C.; Vilas-Boas, J.P.; Ervilha, U.F. A global view on how local muscular fatigue affects human performance. Proc. Natl. Acad. Sci. USA 2020, 117, 19866–19872. [Google Scholar] [CrossRef]
- Hooten, W.M. Chronic Pain and Mental Health Disorders: Shared Neural Mechanisms, Epidemiology, and Treatment. Mayo Clin. Proc. 2016, 91, 955–970. [Google Scholar] [CrossRef]
- Li, Y.; Cheng, H. Application of Anomaly Detection in Medical Data: A Review. Sensors 2021, 9, 7364–7380. [Google Scholar]
- Davidson, M.; Keating, J.L. A comparison of five low back disability questionnaires: Reliability and responsiveness. Phys. Ther. 2002, 82, 8–24. [Google Scholar] [CrossRef] [PubMed]
- Marijanović, I.; Kraljević, M.; Buhovac, T.; Cerić, T.; Mekić Abazović, A.; Alidžanović, J.; Gojković, Z.; Sokolović, E. Use of the Depression, Anxiety and Stress Scale (DASS-21) Questionnaire to Assess Levels of Depression, Anxiety, and Stress in Healthcare and Administrative Staff in 5 Oncology Institutions in Bosnia and Herzegovina during the 2020 COVID-19 Pandemic. Med. Sci. Monit. 2021, 27, 81–93. [Google Scholar] [CrossRef]
- Darnall, B.D.; Sturgeon, J.A.; Cook, K.F.; Taub, C.J.; Roy, A.; Burns, J.W.; Sullivan, M.; Macke, S.C. Development and Validation of a Daily Pain Catastrophizing Scale. J. Pain 2017, 18, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988; Volume 2. [Google Scholar]
- Doan, L.; Manders, T.; Wang, J. Neuroplasticity underlying the comorbidity of pain and depression. Neural Plast. 2015, 215, 504691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickinson, R.S.; Board, T.N.; Kay, P.R. Post-operative anxiety and depression levels in orthopaedic surgery: A study of 56 patients undergoing hip or knee arthroplasty. J. Eval. Clin. 2009, 15, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Kumar, A.; Gupta, S. Mental Health Prevention and Promotion-A Narrative Review. Front. Psychiatry 2022, 13, 898–909. [Google Scholar] [CrossRef]
- Quartana, P.J.; Campbell, C.M.; Edwards, R.R. Pain catastrophizing: A critical review. Expert Rev. Neurother. 2009, 9, 745–758. [Google Scholar] [CrossRef]
- Kalyan, K.; Jakhia, B.; Lele, R.D.; Joshi, M.; Chowdhary, A. Artificial neural network application in the diagnosis of disease conditions with liver ultrasound images. Adv. Bioinform. 2014, 2014, 708279. [Google Scholar] [CrossRef] [Green Version]
- Halilaj, E.; Rajagopal, A.; Fiterau, M.; Hicks, J.L.; Hastie, T.J.; Delp, S.L. Machine learning in human movement biomechanics: Best practices, common pitfalls, and new opportunities. J. Biomech. 2018, 81, 1–11. [Google Scholar] [CrossRef]
- Lillefjell, M.; Krokstad, S.; Espnes, G.A. Prediction of function in daily life following multidisciplinary rehabilitation for individuals with chronic musculoskeletal pain; a prospective study. BMC Musculoskelet. Disord. 2007, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Popescu, V.G.; Burdea, G.C.; Bouzit, M.; Hentz, V.R. A virtual-reality-based telerehabilitation system with force feedback. Technol. Biomed. 2000, 4, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Park, I.; Lee, H.J.; Kim, S.K.; Park, M.S.; Kim, Y.-S. Factors Related to Preoperative Shoulder Pain in Patients with Atraumatic Painful Rotator Cuff Tears. Clin. Shoulder Elb. 2019, 22, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Crombez, C.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.; Karoly, P. Fear-avoidance model of chronic pain: The next generation. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Baños, Y.; Pastor, M.Á.; Velasco, L.; López-Roig, S.; Peñacoba, C.; Lledo, A.; Rodríguez, C. To walk or not to walk: Insights from a qualitative description study with women suffering from fibromyalgia. Rheumatol. Int. 2016, 36, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Écija, C.; Luque-Reca, C.; Suso-Ribera, C.; Catala, P.; Peñacoba, C. Associations of Cognitive Fusion and Pain Catastrophizing with Fibromyalgia Impact through Fatigue, Pain Severity, and Depression: An Exploratory Study Using Structural Equation Modeling. J. Clin. Med. 2020, 9, 1763. [Google Scholar] [CrossRef]
- Pastor-Mira, M.A.; López-Roig, S.; Martínez-Zaragoza, F.; León, E.; Abad, E.; Lledó, A.; Peñacoba, C. Goal preferences, affect, activity patterns and health outcomes in women with fibromyalgia. Front. Psychol. 2019, 10, 1912. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [Green Version]
- Kuner, R.; Kuner, T. Cellular Circuits in the Brain and Their Modulation in Acute and Chronic Pain. Physiol. Rev. 2021, 101, 213–258. [Google Scholar] [CrossRef]
- Baliki, M.N.; Apkarian, A.V. Nociception, Pain, Negative Moods, and Behavior Selection. Neuron 2015, 87, 74–91. [Google Scholar] [CrossRef] [Green Version]
- Stegemann, A.; Liu, S.; Retana Romero, O.A.; Oswald, M.J.; Han, Y.; Beretta, C.A.; Gan, Z.; Tan, L.L.; Wisden, W.; Gräff, J.; et al. Prefrontal engrams of long-term fear memory perpetuate pain perception. Nat. Neurosci. 2022, 26, 820–829. [Google Scholar] [CrossRef]
- Olango, W.M.; Finn, D.P. Neurobiology of stress-induced hyperalgesia. Behav. Neurobiol. Chronic Pain 2014, 20, 251–280. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Variables | Comparison | p | d | |
|---|---|---|---|---|
| Age | G1–22 (8) | G2 | 0.322 | 1.494 |
| G3 | 0.000 | 0.212 | ||
| G2–22 (8) | G1 | 0.322 | 1.494 | |
| G3 | 0.008 | 0.179 | ||
| G3–21 (5) | G1 G2 | 0.000 | 0.212 | |
| 0.008 | 0.179 | |||
| Body mass | G1–62 (21) | G2 | 0.012 | 1.503 |
| G3 | 0.001 | 0.301 | ||
| G2–63 (16) | G1 | 0.012 | 1.503 | |
| G3 | 0.437 | 0.191 | ||
| G3–60 (12) | G1 | 0.001 | 0.301 | |
| G2 | 0.437 | 0.191 | ||
| Height | G1–167 (11) | G2 | 0.801 | 1.403 |
| G3 | 1.000 | 0.177 | ||
| G2–165 (12) | G1 | 0.801 | 1.403 | |
| G3 | 1.000 | 0.054 | ||
| G3–165 (12) | G1 | 1.000 | 0.177 | |
| G2 | 1.000 | 0.054 | ||
| Gender | G1 * | G2 | 1.000 | 0.041 |
| G3 | 1.000 | 0.138 | ||
| G2 * | G1 | 1.000 | 0.041 | |
| G3 | 1.000 | 0.034 | ||
| G3 * | G1 | 1.000 | 0.138 | |
| G2 | 1.000 | 0.034 | ||
| Mental illness diagnosis | G1 * | G2 | 0.054 | 0.111 |
| G3 | 0.060 | 0.158 | ||
| G2 * | G1 | 0.054 | 0.111 | |
| G3 | 1.000 | 0.033 | ||
| G3 * | G1 | 0.060 | 0.158 | |
| G2 | 1.000 | 0.033 | ||
| Lumbar pathology diagnosis | G1 * | G2 | 0.041 | 1.421 |
| G3 | 0.000 | 0.200 | ||
| G2 * | G1 | 0.041 | 1.421 | |
| G3 | 0.142 | 0.136 | ||
| G3 * | G1 | 0.000 | 0.200 | |
| G2 | 0.142 | 0.136 | ||
| LBP events | G1–4 (9) | G2 | 0.000 | 1.469 |
| G3 | 0.000 | 0.260 | ||
| G2–4 (4) | G1 | 0.000 | 1.469 | |
| G3 | 0.028 | 0.280 | ||
| G3–4 (4) | G1 | 0.000 | 0.260 | |
| G2 | 0.028 | 0.280 | ||
| DASS—stress | G1–14 (16) | G2 | 0.000 | 1.686 |
| G3 | 0.000 | 0.517 | ||
| G2–10 (10) | G1 | 0.000 | 1.686 | |
| G3 | 0.015 | 0.424 | ||
| G3–10 (8) | G1 | 0.000 | 0.517 | |
| G2 | 0.015 | 0.424 | ||
| DASS—anxiety | G1–8 (12) | G2 | 0.000 | 1.677 |
| G3 | 0.000 | 0.506 | ||
| G2–4 (6) | G1 | 0.000 | 1.677 | |
| G3 | 0.021 | 0.413 | ||
| G3–2 (8) | G1 | 0.000 | 0.506 | |
| G2 | 0.021 | 0.413 | ||
| DASS—depression | G1–12 (20) | G2 | 0.000 | 1.757 |
| G3 | 0.000 | 0.596 | ||
| G2–6 (10) | G1 | 0.000 | 1.757 | |
| G3 | 0.001 | 0.510 | ||
| G3–6 (8) | G1 | 0.000 | 0.596 | |
| G2 | 0.001 | 0.510 | ||
| PCS-D | G1–2 (15) | G2 | 0.000 | 1.523 |
| G3 | 0.000 | 0.326 | ||
| G2–1 (8) | G1 | 0.000 | 1.523 | |
| G3 | 0.000 | 0.218 | ||
| G3–1 (5) | G1 G2 | 0.000 0.000 | 0.326 0.218 | |
| ODI | G1–10 (18) | G2 G3 | 0.015 | 1.416 |
| 0.000 | 0.193 | |||
| G2–10 (16) | G1 | 0.015 | 1.416 | |
| G3 | 0.036 | 0.072 | ||
| G3–8 (10) | G1 G2 | 0.000 0.036 | 0.193 0.072 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parolini, F.; Goethel, M.; Becker, K.; Fernandes, C.; Fernandes, R.J.; Ervilha, U.F.; Santos, R.; Vilas-Boas, J.P. Breaking Barriers: Artificial Intelligence Interpreting the Interplay between Mental Illness and Pain as Defined by the International Association for the Study of Pain. Biomedicines 2023, 11, 2042. https://doi.org/10.3390/biomedicines11072042
Parolini F, Goethel M, Becker K, Fernandes C, Fernandes RJ, Ervilha UF, Santos R, Vilas-Boas JP. Breaking Barriers: Artificial Intelligence Interpreting the Interplay between Mental Illness and Pain as Defined by the International Association for the Study of Pain. Biomedicines. 2023; 11(7):2042. https://doi.org/10.3390/biomedicines11072042
Chicago/Turabian StyleParolini, Franciele, Márcio Goethel, Klaus Becker, Cristofthe Fernandes, Ricardo J. Fernandes, Ulysses F. Ervilha, Rubim Santos, and João Paulo Vilas-Boas. 2023. "Breaking Barriers: Artificial Intelligence Interpreting the Interplay between Mental Illness and Pain as Defined by the International Association for the Study of Pain" Biomedicines 11, no. 7: 2042. https://doi.org/10.3390/biomedicines11072042