
An Observational Study on Chronic Pain Biomarkers in Fibromyalgia and Osteoarthritis Patients: Which Role for Mu Opioid Receptor’s Expression on NK Cells?
 , ,
, ,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Clinical Measurements
2.4. Blood Collection
2.5. Immunophenotyping Analysis
2.6. Lymphocytes Isolation
2.7. Proteins Extraction
2.8. Western Blot Analysis
2.9. Statistical Analysis
2.9.1. Statistical Analysis for Immunophenotyping
2.9.2. Statistical Analysis for Clinical Correlations Evaluation
3. Results
3.1. Patients’ Characteristics
3.2. Biological Results
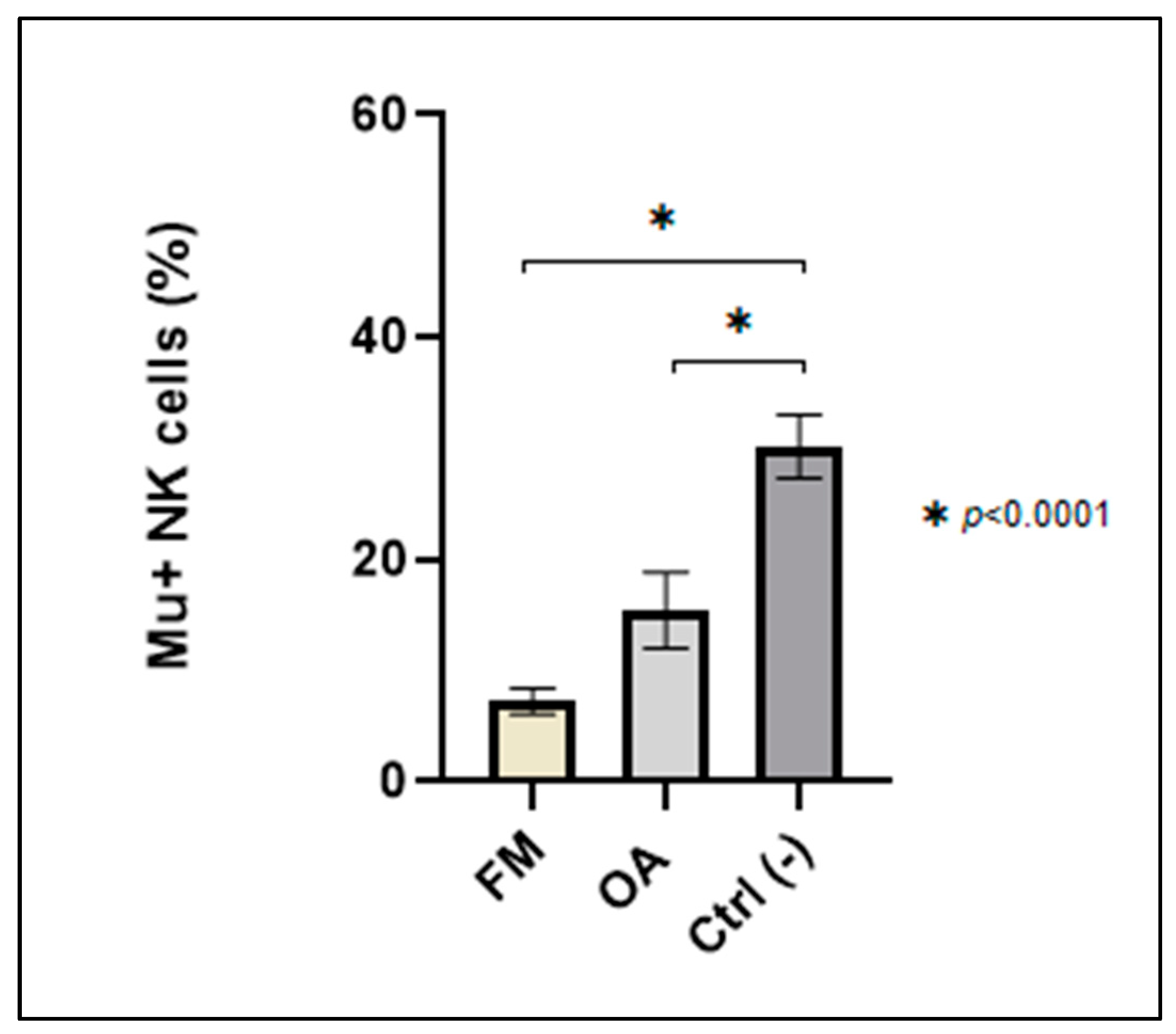
3.2.1. Immunophenotyping Analysis: Mu+ NK Cells Percentage of Expression
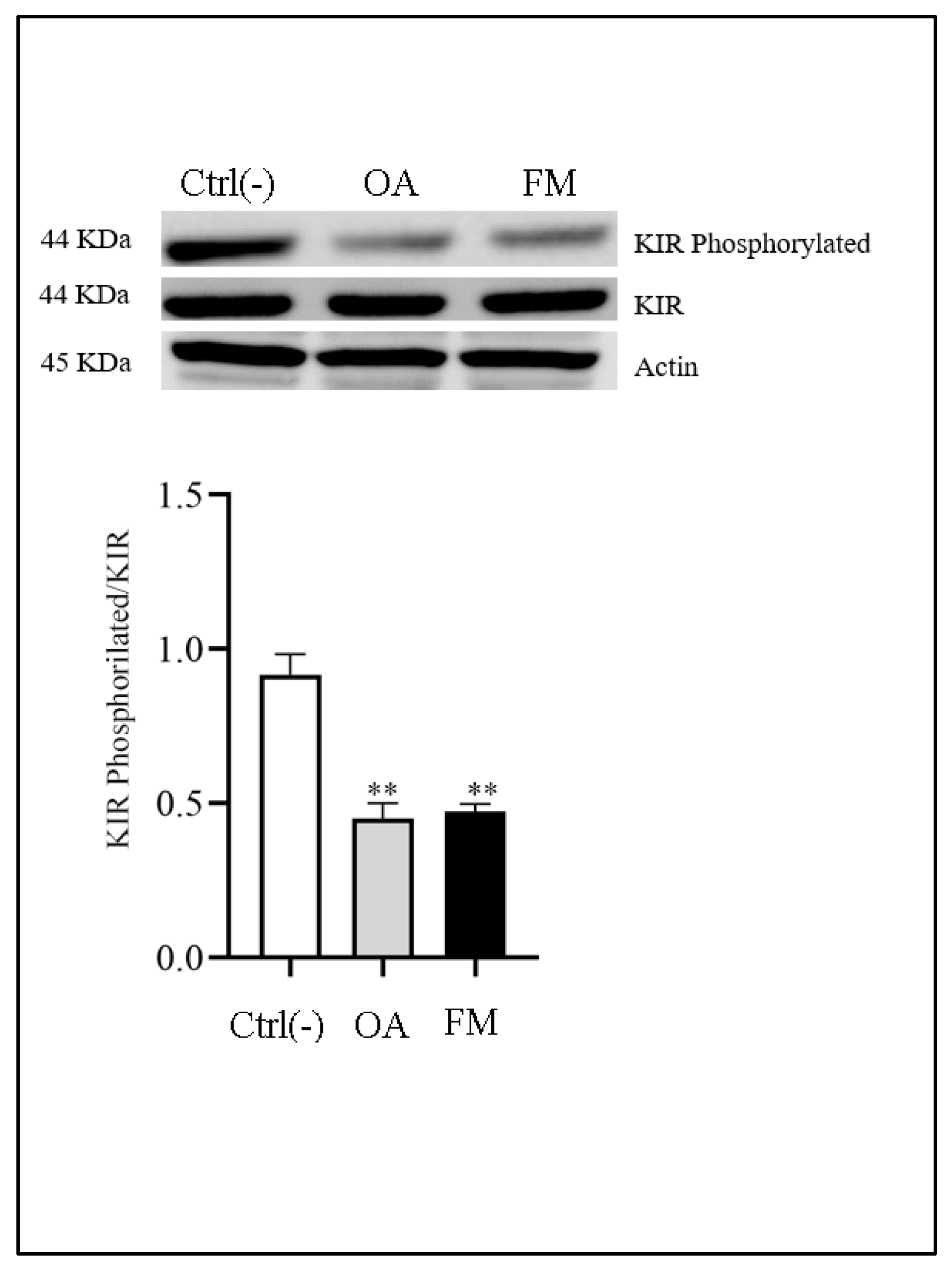
3.2.2. Western Blot Analysis
3.3. Mu+ NK Cells Expression and Correlations Analysis
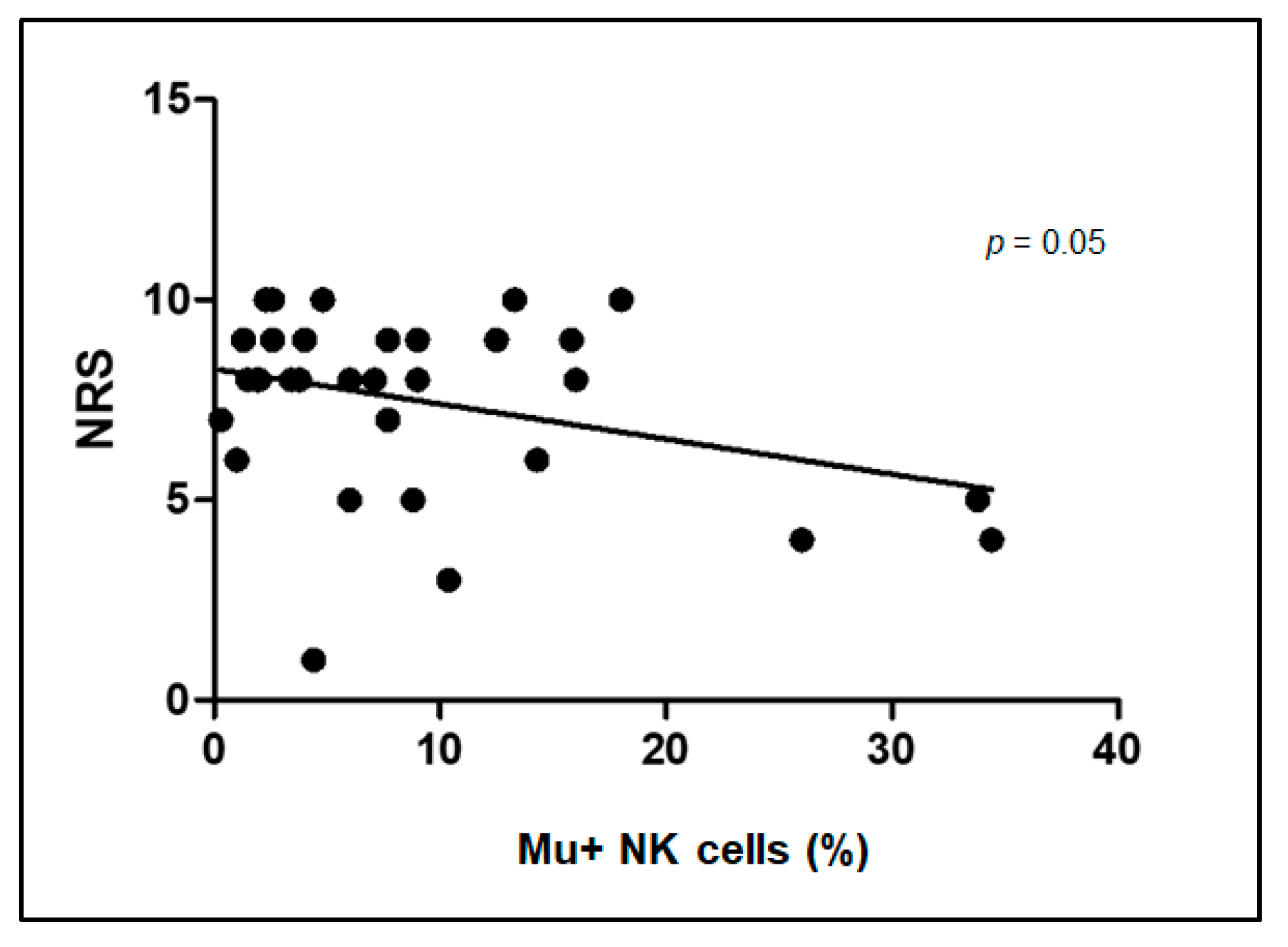
3.3.1. Correlation between Intensity of Pain (NRS Scale) and Mu+ NK Cells Percentage of Expression
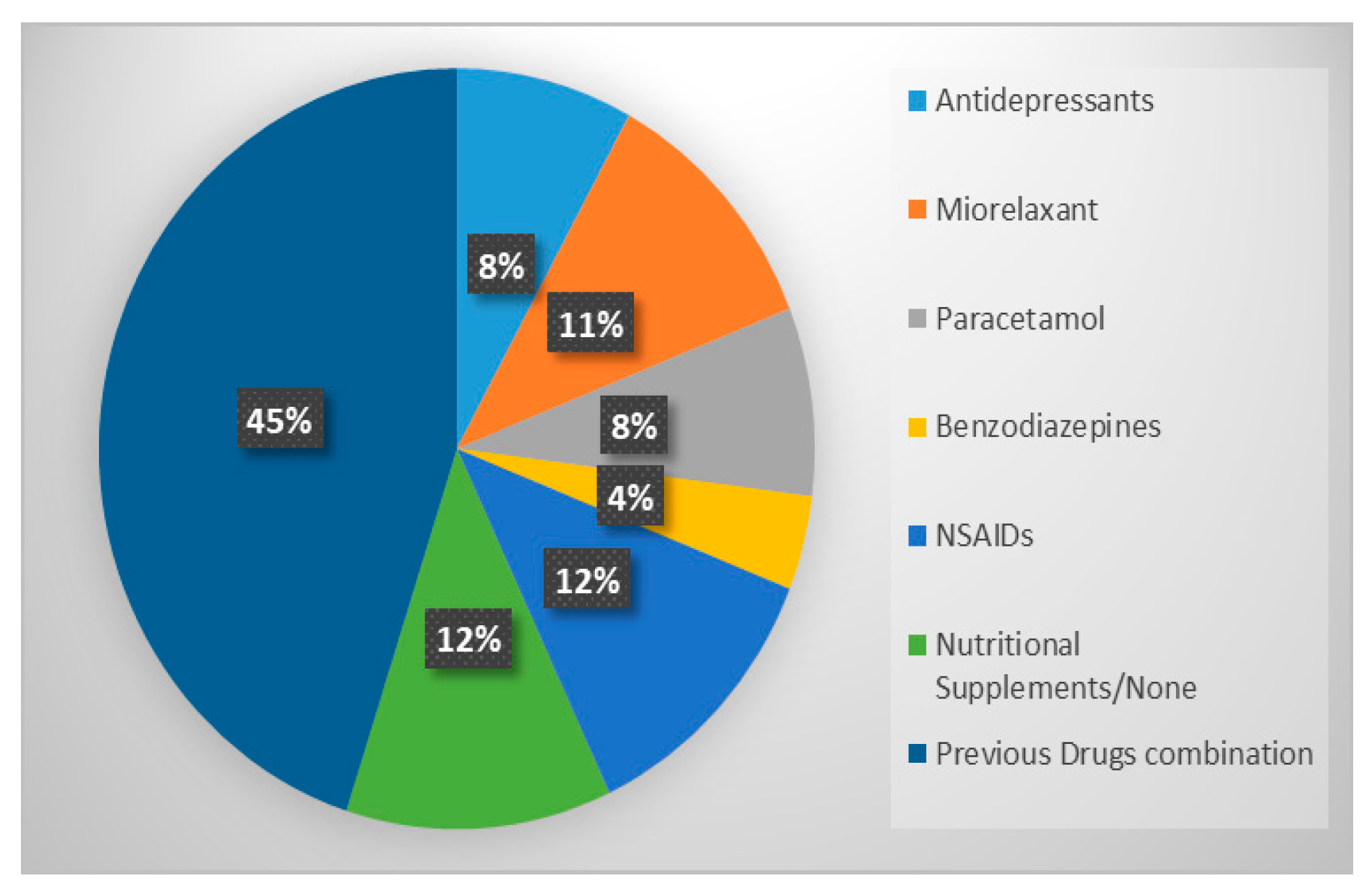
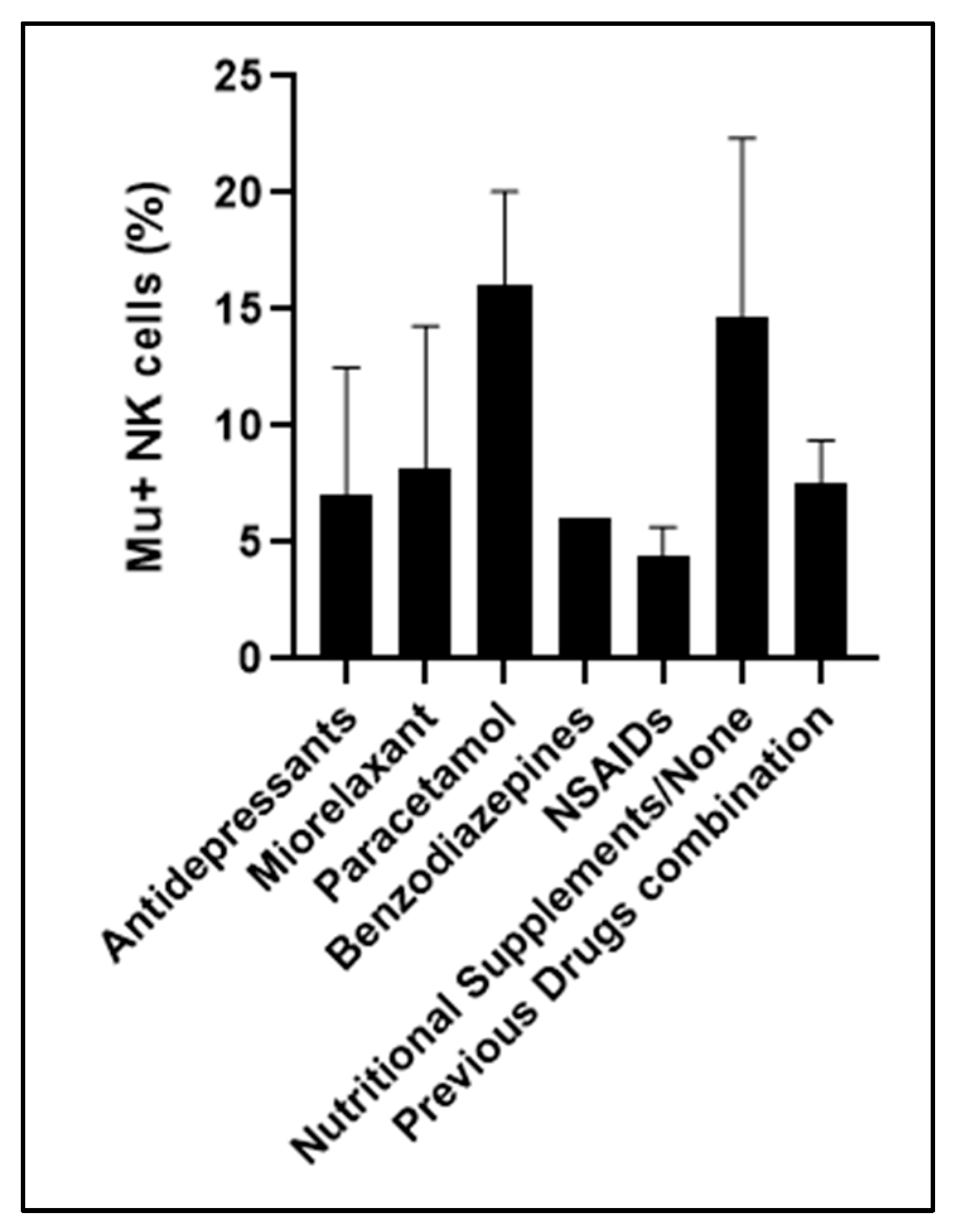
3.3.2. Comparison between Therapy before Enrollment and Mu+ NK Cells Percentage of Expression
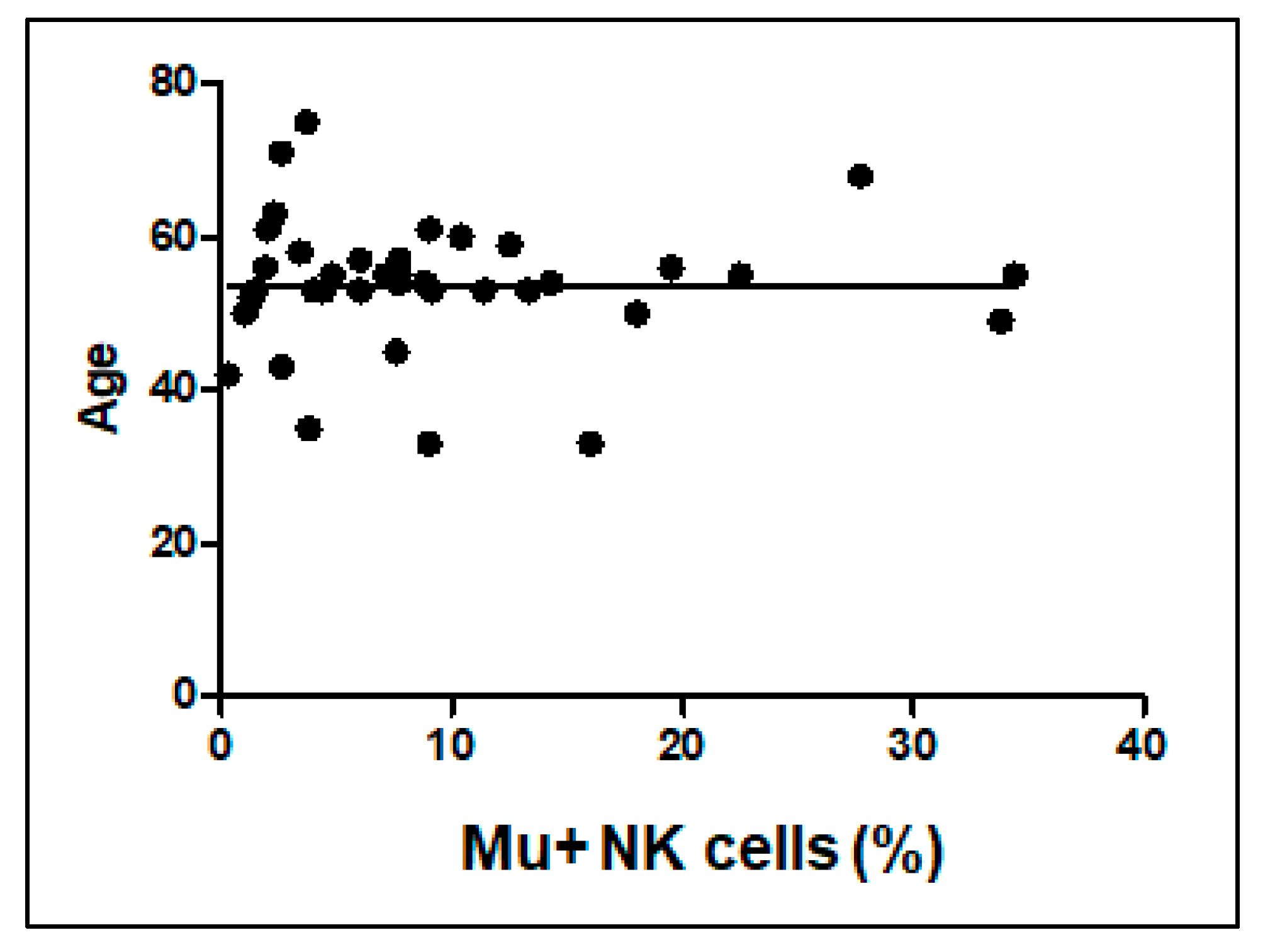
3.3.3. Correlations between Patients’ Age with Mu+ NK Cells Percentage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Henschke, N.; Kamper, S.J.; Maher, C.G. The Epidemiology and Economic Consequences of Pain. Mayo Clin. Proc. 2015, 90, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treede, R.-D. The International Association for the Study of Pain definition of pain: As valid in 2018 as in 1979, but in need of regularly updated footnotes. PAIN Rep. 2018, 3, e643. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Mattes, W.; Goodsaid, F. Regulatory landscapes for biomarkers and diagnostic tests: Qualification, approval, and role in clinical practice. Exp. Biol. Med. 2018, 243, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Malafoglia, V.; Tenti, M.; Ilari, S.; Balzani, E.; Fanelli, A.; Muscoli, C.; Raffaeli, W.; Bonci, A. Opportunities and challenges for nonaddictive interventions in chronic pain. Curr. Opin. Pharmacol. 2021, 57, 184–191. [Google Scholar] [CrossRef]
- Bäckryd, E. Pain in the Blood? Envisioning Mechanism-Based Diagnoses and Biomarkers in Clinical Pain Medicine. Diagnostics 2015, 5, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Malafoglia, V.; Ilari, S.; Vitiello, L.; Tenti, M.; Balzani, E.; Muscoli, C.; Raffaeli, W.; Bonci, A. The Interplay between Chronic Pain, Opioids, and the Immune System. Neuroscientist 2021, 28, 613–627. [Google Scholar] [CrossRef] [PubMed]
- Raffaeli, W.; Malafoglia, V.; Bonci, A.; Tenti, M.; Ilari, S.; Gremigni, P.; Iannuccelli, C.; Gioia, C.; Di Franco, M.; Mollace, V.; et al. Identification of MOR-Positive B Cell as Possible Innovative Biomarker (Mu Lympho-Marker) for Chronic Pain Diagnosis in Patients with Fibromyalgia and Osteoarthritis Diseases. Int. J. Mol. Sci. 2020, 21, 1499. [Google Scholar] [CrossRef] [Green Version]
- Björkström, N.K.; Strunz, B.; Ljunggren, H.-G. Natural killer cells in antiviral immunity. Nat. Rev. Immunol. 2022, 22, 112–123. [Google Scholar] [CrossRef]
- Fang, F.; Xie, S.; Chen, M.; Li, Y.; Yue, J.; Ma, J.; Shu, X.; He, Y.; Xiao, W.; Tian, Z. Advances in NK cell production. Cell. Mol. Immunol. 2022, 19, 460–481. [Google Scholar] [CrossRef]
- Mesiano, G.; Zini, R.; Montagner, G.; Bianchi, N.; Manfredini, R.; Chillemi, A.; Aglietta, M.; Grignani, G.; Lampronti, I.; Fiorino, E.; et al. Analytic and Dynamic Secretory Profile of Patient-Derived Cytokine-lnduced Killer Cells. Mol. Med. 2017, 23, 235–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garofalo, C.; De Marco, C.; Cristiani, C.M. NK Cells in the Tumor Microenvironment as New Potential Players Mediating Chemotherapy Effects in Metastatic Melanoma. Front. Oncol. 2021, 11, 754541. [Google Scholar] [CrossRef]
- Souza-Fonseca-Guimaraes, F.; Adib-Conquy, M.; Cavaillon, J.-M. Natural Killer (NK) Cells in Antibacterial Innate Immunity: Angels or Devils? Mol. Med. 2011, 18, 270–285. [Google Scholar] [CrossRef]
- Maher, D.P.; Walia, D.; Heller, N.M. Suppression of Human Natural Killer Cells by Different Classes of Opioids. Obstet. Anesth. Dig. 2019, 128, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Provinciali, M.; Di Stefano, G.; Stronati, S.; Raffaeli, W.; Pari, G.; Fabris, N. Role of prolactin in the modulation of NK and lak cell activity after short- or long-term morphine administration in neoplastic patients. Int. J. Immunopharmacol. 1996, 18, 577–586. [Google Scholar] [CrossRef]
- Campana, G.; Sarti, D.; Spampinato, S.; Raffaeli, W. Long-term intrathecal morphine and bupivacaine upregulate MOR gene expression in lymphocytes. Int. Immunopharmacol. 2010, 10, 1149–1152. [Google Scholar] [CrossRef] [PubMed]
- Gaveriaux-Ruff, C.; Kieffer, B. Opioid receptor genes inactivated in mice: The highlights. Neuropeptides 2002, 36, 62–71. [Google Scholar] [CrossRef]
- Brejchova, J.; Holan, V.; Svoboda, P. Expression of Opioid Receptors in Cells of the Immune System. Int. J. Mol. Sci. 2020, 22, 315. [Google Scholar] [CrossRef]
- Lewis, S.S.; Loram, L.C.; Hutchinson, M.; Li, C.-M.; Zhang, Y.; Maier, S.F.; Huang, Y.; Rice, K.C.; Watkins, L.R. (+)-Naloxone, an Opioid-Inactive Toll-Like Receptor 4 Signaling Inhibitor, Reverses Multiple Models of Chronic Neuropathic Pain in Rats. J. Pain 2012, 13, 498–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, D.P.; Walia, D.; Heller, N.M. Morphine decreases the function of primary human natural killer cells by both TLR4 and opioid receptor signaling. Brain Behav. Immun. 2020, 83, 298–302. [Google Scholar] [CrossRef]
- Tabellini, G.; Borsani, E.; Benassi, M.; Patrizi, O.; Ricotta, D.; Caimi, L.; Lanzi, R.; Micheli, F.; Iorno, V.; Bettaglio, R.; et al. Effects of opioid therapy on human natural killer cells. Int. Immunopharmacol. 2014, 18, 169–174. [Google Scholar] [CrossRef]
- Yoon, J.J.; Song, J.A.; Park, S.Y.; Choi, J.I. Cytotoxic activity and subset populations of peripheral blood natural killer cells in patients with chronic pain. Korean J. Pain 2018, 31, 43–49. [Google Scholar] [CrossRef]
- Plein, L.M.; Rittner, H.L. Opioids and the immune system—Friend or foe. Br. J. Pharmacol. 2017, 175, 2717–2725. [Google Scholar] [CrossRef] [Green Version]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- Long, E.O. Negative signaling by inhibitory receptors: The NK cell paradigm. Immunol. Rev. 2008, 224, 70–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thudium, C.S.; Löfvall, H.; Karsdal, M.A.; Bay-Jensen, A.-C.; Bihlet, A.R. Protein biomarkers associated with pain mechanisms in osteoarthritis. J. Proteom. 2019, 190, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Romero, E.A.; Battaglino, A.P.; Campanella, W.; Turroni, S.; Bishop, M.D.; Villafañe, J.H. Impact on Blood Tests of Lower Limb Joint Replacement for the Treatment of Osteoarthritis. Top. Geriatr. Rehabil. 2021, 37, 227–229. [Google Scholar] [CrossRef]
- Blanca, I.R.; Bere, E.W.; Young, H.A.; Ortaldo, J.R. Human B Cell Activation by Autologous NK Cells Is Regulated by CD40-CD40 Ligand Interaction: Role of Memory B Cells and CD5+ B Cells. J. Immunol. 2001, 167, 6132–6139. [Google Scholar] [CrossRef] [Green Version]
- Gao, N.; Dang, T.; Dunnick, W.A.; Collins, J.T.; Blazar, B.R.; Yuan, D. Receptors and Counterreceptors Involved in NK-B Cell Interactions. J. Immunol. 2005, 174, 4113–4119. [Google Scholar] [CrossRef] [Green Version]
- Jennings, P.; Yuan, D. NK Cell Enhancement of Antigen Presentation by B Lymphocytes. J. Immunol. 2009, 182, 2879–2887. [Google Scholar] [CrossRef] [Green Version]
- Raffaeli, W.; Tenti, M.; Corraro, A.; Malafoglia, V.; Ilari, S.; Balzani, E.; Bonci, A. Chronic Pain: What Does It Mean? A Review on the Use of the Term Chronic Pain in Clinical Practice. J. Pain Res. 2021, 14, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Romero, E.A.; Martínez Rolando, L.; Villafañe, J.H. Impact of Lockdown on Patients with Fibromyalgia. Electron. J. Gen. Med. 2022, 19, em366. [Google Scholar] [CrossRef] [PubMed]
- Romero, E.S.; Oliva, E.M.; Pérez, J.A.; Pérez, S.M.; Turroni, S.; Marchese, L.; Villafañe, J. Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature. Nutrients 2021, 13, 716. [Google Scholar] [CrossRef] [PubMed]
- Clos-Garcia, M.; Andrés-Marin, N.; Fernández-Eulate, G.; Abecia, L.; Lavín, J.L.; van Liempd, S.; Cabrera, D.; Royo, F.; Valero, A.; Errazquin, N.; et al. Gut microbiome and serum metabolome analyses identify molecular biomarkers and altered glutamate metabolism in fibromyalgia. Ebiomedicine 2019, 46, 499–511. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | |
|---|---|
| Diagnosis | % of Patinets (n = 64) |
| Fibromyalgia (FM) | 45% (n= 29) |
| Osteoatrithis (OA) | 19% (n = 12) |
| No pain | 36% (n = 23) |
| Gender | |
| Male | 0% (n = 0) |
| Female | 100% (n = 64) |
| AGE (years) | |
| 20–29 | 0% (n = 0) |
| 30–39 | 8% (n = 3) |
| 40–49 | 10.5% (n = 4) |
| 50–59 | 63% (n = 24) |
| 60–69 | 13.5% (n = 5) |
| 70–79 | 5% (n = 2) |
| mean 54 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malafoglia, V.; Ilari, S.; Gioia, C.; Vitiello, L.; Tenti, M.; Iannuccelli, C.; Cristiani, C.M.; Garofalo, C.; Passacatini, L.C.; Viglietto, G.; et al. An Observational Study on Chronic Pain Biomarkers in Fibromyalgia and Osteoarthritis Patients: Which Role for Mu Opioid Receptor’s Expression on NK Cells? Biomedicines 2023, 11, 931. https://doi.org/10.3390/biomedicines11030931
Malafoglia V, Ilari S, Gioia C, Vitiello L, Tenti M, Iannuccelli C, Cristiani CM, Garofalo C, Passacatini LC, Viglietto G, et al. An Observational Study on Chronic Pain Biomarkers in Fibromyalgia and Osteoarthritis Patients: Which Role for Mu Opioid Receptor’s Expression on NK Cells? Biomedicines. 2023; 11(3):931. https://doi.org/10.3390/biomedicines11030931
Chicago/Turabian StyleMalafoglia, Valentina, Sara Ilari, Chiara Gioia, Laura Vitiello, Michael Tenti, Cristina Iannuccelli, Costanza Maria Cristiani, Cinzia Garofalo, Lucia Carmela Passacatini, Giuseppe Viglietto, and et al. 2023. "An Observational Study on Chronic Pain Biomarkers in Fibromyalgia and Osteoarthritis Patients: Which Role for Mu Opioid Receptor’s Expression on NK Cells?" Biomedicines 11, no. 3: 931. https://doi.org/10.3390/biomedicines11030931