
Efficacy of Low-Dose Naltrexone and Predictors of Treatment Success or Discontinuation in Fibromyalgia and Other Chronic Pain Conditions: A Fourteen-Year, Enterprise-Wide Retrospective Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Data Collection
2.3. Statistical Analyses
2.4. Subgroup Analysis
3. Results
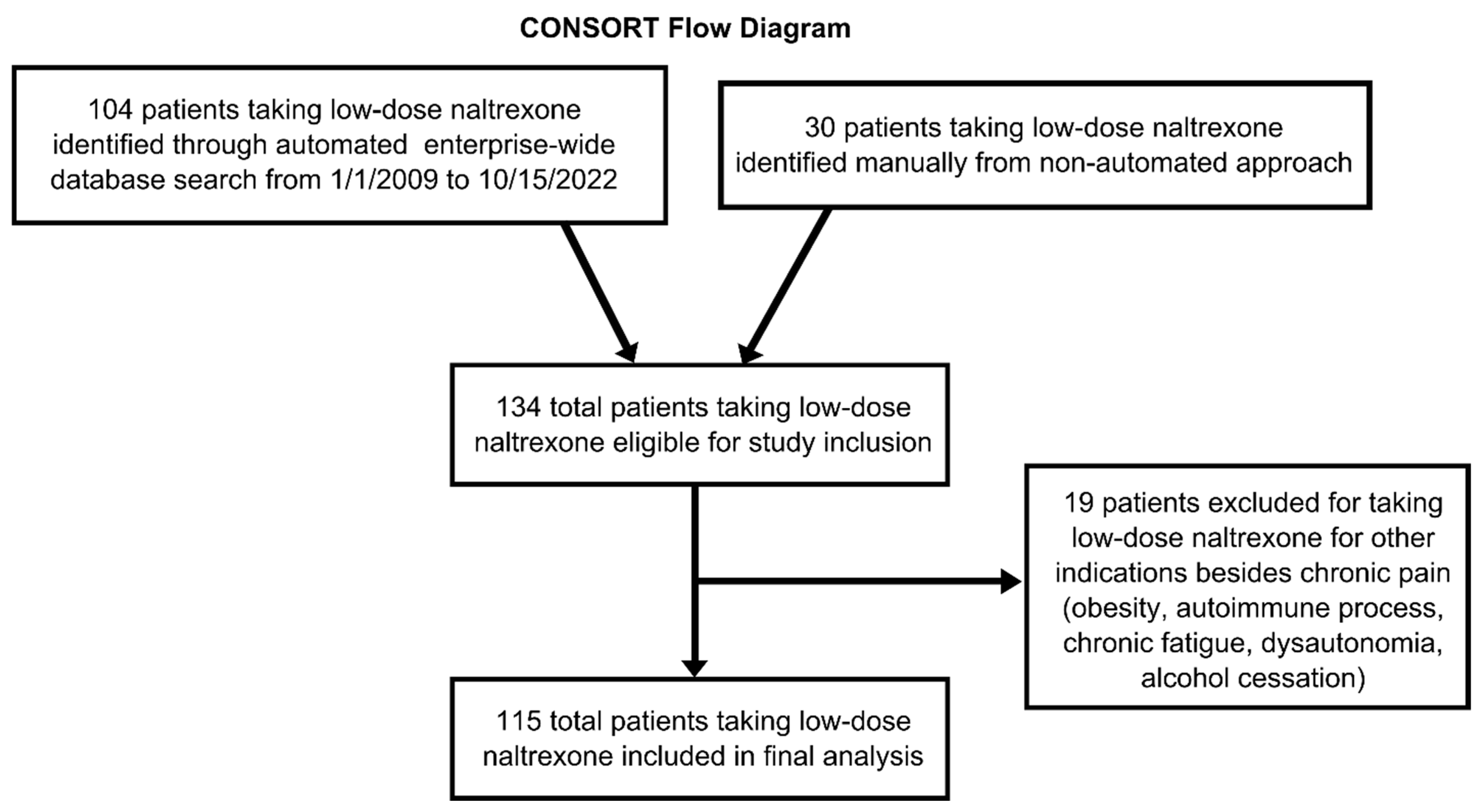
3.1. Data Collection
3.2. Patient and Prescription Characteristics
3.3. Adverse Effects
3.4. Logistic Regression
3.5. LDN-Only versus LDN-Plus-Concomitant Analgesics Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Ross, K.; Anderson, J.; Russell, I.J.; Hebert, L. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheumatol. 1995, 38, 19–28. [Google Scholar] [CrossRef]
- Vincent, A.; Lahr, B.D.; Wolfe, F.; Clauw, D.J.; Whipple, M.O.; Oh, T.H.; Barton, D.L.; St Sauver, J. Prevalence of fibromyalgia: A population-based study in Olmsted County, Minnesota, utilizing the Rochester Epidemiology Project. Arthritis Care Res. 2013, 65, 786–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Mil. Med. 2016, 181, 397–399. [CrossRef] [Green Version]
- Gyorfi, M.; Rupp, A.; Abd-Elsayed, A. Fibromyalgia Pathophysiology. Biomedicines 2022, 10, 3070. [Google Scholar] [CrossRef] [PubMed]
- Leow-Dyke, S.; Allen, C.; Denes, A.; Nilsson, O.; Maysami, S.; Bowie, A.G.; Rothwell, N.J.; Pinteaux, E. Neuronal Toll-like receptor 4 signaling induces brain endothelial activation and neutrophil transmigration in vitro. J. Neuroinflamm. 2012, 9, 230. [Google Scholar] [CrossRef] [Green Version]
- Von Hehn, C.A.; Baron, R.; Woolf, C.J. Deconstructing the neuropathic pain phenotype to reveal neural mechanisms. Neuron 2012, 73, 638–652. [Google Scholar] [CrossRef] [Green Version]
- Dantzer, R. Cytokine, sickness behavior, and depression. Immunol. Allergy Clin. N. Am. 2009, 29, 247–264. [Google Scholar] [CrossRef] [Green Version]
- Ge, L.; D’Souza, R.S.; Oh, T.; Vincent, A.; Mohabbat, A.B.; Eldrige, J.; Jiang, L.; Whipple, M.O.; McAllister, S.J.; Wang, Z.; et al. Tobacco Use in Fibromyalgia Is Associated With Cognitive Dysfunction: A Prospective Questionnaire Study. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Souza, R.S.; Lin, G.; Oh, T.; Vincent, A.; Orhurhu, V.; Jiang, L.; Mauck, W.D.; Qu, W. Fibromyalgia Symptom Severity and Psychosocial Outcomes in Fibromyalgia Patients with Hypovitaminosis D: A Prospective Questionnaire Study. Pain Med. 2020, 21, 3470–3478. [Google Scholar] [CrossRef]
- D’Souza, R.S.; Whipple, M.O.; Vincent, A.S. Therapy and Symptom Burden in Patients with Fibromyalgia: A Prospective Questionnaire Study. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 1036–1041. [Google Scholar] [CrossRef]
- Jiang, L.; D’Souza, R.S.; Oh, T.; Vincent, A.; Mohabbat, A.B.; Ashmore, Z.; Mauck, W.D.; Ge, L.; Whipple, M.O.; McAllister, S.J.; et al. Sex-Related Differences in Symptoms and Psychosocial Outcomes in Patients With Fibromyalgia: A Prospective Questionnaire Study. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 767–774. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, R.S.; Langford, B.; Wilson, R.E.; Her, Y.F.; Schappell, J.; Eller, J.S.; Evans, T.C.; Hagedorn, J.M. The state-of-the-art pharmacotherapeutic options for the treatment of chronic non-cancer pain. Expert Opin. Pharmacother. 2022, 23, 775–789. [Google Scholar] [CrossRef]
- Hutchinson, M.R.; Zhang, Y.; Brown, K.; Coats, B.D.; Shridhar, M.; Sholar, P.W.; Patel, S.J.; Crysdale, N.Y.; Harrison, J.A.; Maier, S.F.; et al. Non-stereoselective reversal of neuropathic pain by naloxone and naltrexone: Involvement of toll-like receptor 4 (TLR4). Eur. J. Neurosci. 2008, 28, 20–29. [Google Scholar] [CrossRef] [Green Version]
- San-Emeterio, E.P.; Hurle, M.A. Modulation of brain apoptosis-related proteins by the opioid antagonist naltrexone in mice. Neurosci. Lett. 2006, 403, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Parkitny, L.; Younger, J. Reduced Pro-Inflammatory Cytokines after Eight Weeks of Low-Dose Naltrexone for Fibromyalgia. Biomedicines 2017, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Toljan, K.; Vrooman, B. Low-Dose Naltrexone (LDN)-Review of Therapeutic Utilization. Med. Sci. 2018, 6, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younger, J.; Parkitny, L.; McLain, D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clin. Rheumatol. 2014, 33, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Kim, P.S.; Fishman, M.A. Low-Dose Naltrexone for Chronic Pain: Update and Systemic Review. Curr. Pain Headache Rep. 2020, 24, 64. [Google Scholar] [CrossRef]
- Bruun, K.D.; Amris, K.; Vaegter, H.B.; Blichfeldt-Eckhardt, M.R.; Holsgaard-Larsen, A.; Christensen, R.; Toft, P. Low-dose naltrexone for the treatment of fibromyalgia: Protocol for a double-blind, randomized, placebo-controlled trial. Trials 2021, 22, 804. [Google Scholar] [CrossRef]
- Chindalore, V.L.; Craven, R.A.; Yu, K.P.; Butera, P.G.; Burns, L.H.; Friedmann, N. Adding ultralow-dose naltrexone to oxycodone enhances and prolongs analgesia: A randomized, controlled trial of Oxytrex. J. Pain 2005, 6, 392–399. [Google Scholar] [CrossRef]
- Largent-Milnes, T.M.; Guo, W.; Wang, H.Y.; Burns, L.H.; Vanderah, T.W. Oxycodone plus ultra-low-dose naltrexone attenuates neuropathic pain and associated mu-opioid receptor-Gs coupling. J. Pain 2008, 9, 700–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chopra, P.; Cooper, M.S. Treatment of Complex Regional Pain Syndrome (CRPS) using low dose naltrexone (LDN). J. Neuroimmune Pharmacol. 2013, 8, 470–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.P.; Stock, H.; Bingaman, S.; Mauger, D.; Rogosnitzky, M.; Zagon, I.S. Low-dose naltrexone therapy improves active Crohn’s disease. Am. J. Gastroenterol. 2007, 102, 820–828. [Google Scholar] [CrossRef]
- Smith, J.P.; Bingaman, S.I.; Ruggiero, F.; Mauger, D.T.; Mukherjee, A.; McGovern, C.O.; Zagon, I.S. Therapy with the opioid antagonist naltrexone promotes mucosal healing in active Crohn’s disease: A randomized placebo-controlled trial. Dig. Dis. Sci. 2011, 56, 2088–2097. [Google Scholar] [CrossRef] [PubMed]
- Raknes, G.; Smabrekke, L. Low dose naltrexone: Effects on medication in rheumatoid and seropositive arthritis. A nationwide register-based controlled quasi-experimental before-after study. PLoS ONE 2019, 14, e0212460. [Google Scholar] [CrossRef] [Green Version]
- Gironi, M.; Martinelli-Boneschi, F.; Sacerdote, P.; Solaro, C.; Zaffaroni, M.; Cavarretta, R.; Moiola, L.; Bucello, S.; Radaelli, M.; Pilato, V.; et al. A pilot trial of low-dose naltrexone in primary progressive multiple sclerosis. Mult. Scler. 2008, 14, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Dieckmann, G.; Ozmen, M.C.; Cox, S.M.; Engert, R.C.; Hamrah, P. Low-dose naltrexone is effective and well-tolerated for modulating symptoms in patients with neuropathic corneal pain. Ocul. Surf. 2021, 20, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Neuman, D.L.; Chadwick, A.L. Utilization of Low-Dose Naltrexone for Burning Mouth Syndrome: A Case Report. A&A Pract. 2021, 15, e01475. [Google Scholar] [CrossRef]
- Srinivasan, A.; Dutta, P.; Bansal, D.; Chakrabarti, A.; Bhansali, A.K.; Hota, D. Efficacy and safety of low-dose naltrexone in painful diabetic neuropathy: A randomized, double-blind, active-control, crossover clinical trial. J. Diabetes 2021, 13, 770–778. [Google Scholar] [CrossRef]
- Younger, J.; Mackey, S. Fibromyalgia symptoms are reduced by low-dose naltrexone: A pilot study. Pain Med. 2009, 10, 663–672. [Google Scholar] [CrossRef] [Green Version]
- Younger, J.; Noor, N.; McCue, R.; Mackey, S. Low-dose naltrexone for the treatment of fibromyalgia: Findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis Rheumatol. 2013, 65, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.J.; McAnally, H.B.; Okediji, P.; Rogosnitzky, M. Low-dose naltrexone, an opioid-receptor antagonist, is a broad-spectrum analgesic: A retrospective cohort study. Pain Manag. 2022, 12, 699–709. [Google Scholar] [CrossRef] [PubMed]
- O’Kelly, B.; Vidal, L.; McHugh, T.; Woo, J.; Avramovic, G.; Lambert, J.S. Safety and efficacy of low dose naltrexone in a long covid cohort; an interventional pre-post study. Brain Behav. Immun. Health 2022, 24, 100485. [Google Scholar] [CrossRef] [PubMed]
- Metz, M.J.; Daimon, C.M.; Hentges, S.T. Reported Benefits of Low-Dose Naltrexone Appear to Be Independent of the Endogenous Opioid System Involving Proopiomelanocortin Neurons and β-Endorphin. eNeuro 2021, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ploesser, J.; Weinstock, L.B.; Thomas, E. Low dose naltrexone: Side effects and efficacy in gastrointestinal disorders. Int. J. Pharm. Compd. 2010, 14, 171–173. [Google Scholar] [PubMed]
- Webster, L.R.; Butera, P.G.; Moran, L.V.; Wu, N.; Burns, L.H.; Friedmann, N. Oxytrex minimizes physical dependence while providing effective analgesia: A randomized controlled trial in low back pain. J. Pain 2006, 7, 937–946. [Google Scholar] [CrossRef]
- Cuomo, A.; Bimonte, S.; Forte, C.A.; Botti, G.; Cascella, M. Multimodal approaches and tailored therapies for pain management: The trolley analgesic model. J. Pain Res. 2019, 12, 711–714. [Google Scholar] [CrossRef]
- Argoff, C.E.; Albrecht, P.; Irving, G.; Rice, F. Multimodal analgesia for chronic pain: Rationale and future directions. Pain Med. 2009, 10 (Suppl. S2), S53–S66. [Google Scholar] [CrossRef] [Green Version]
- Kaye, A.D.; Urman, R.D.; Rappaport, Y.; Siddaiah, H.; Cornett, E.M.; Belani, K.; Salinas, O.J.; Fox, C.J. Multimodal analgesia as an essential part of enhanced recovery protocols in the ambulatory settings. J. Anaesthesiol. Clin. Pharmacol. 2019, 35 (Suppl. S1), S40–S45. [Google Scholar] [CrossRef]
- Colloca, L. The Placebo Effect in Pain Therapies. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 191–211. [Google Scholar] [CrossRef]
- D’Souza, R.S.; Gurrieri, C.; Johnson, R.L.; Warner, N.; Wittwer, E. Intraoperative methadone administration and postoperative pain control: A systematic review and meta-analysis. Pain 2020, 161, 237–243. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, R.; Esfahani, K.; Dunn, L. Pro-Con Debate: Role of Methadone in Enhanced Recovery After Surgery Protocols—Superior Analgesic or Harmful Drug? Anesth. Analg. 2023, in press. [Google Scholar]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrero, J.F.; Laird, J.M.; López-García, J.A. Wind-up of spinal cord neurones and pain sensation: Much ado about something? Prog. Neurobiol. 2000, 61, 169–203. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample with Data (n) | Mean (SD) or n (%) | ||
|---|---|---|---|
| Age (y) | 98 | 48 | 16 |
| Gender | 115 | ||
| Female | 99 | 86% | |
| Male | 14 | 12% | |
| Non-binary | 1 | 1% | |
| Transgender | 1 | 1% | |
| Specialty of Prescriber | 115 | ||
| Integrative Medicine/Fibromyalgia Clinic | 33 | 29% | |
| Primary Care/Family Medicine | 22 | 19% | |
| Neurology | 22 | 19% | |
| Pain Medicine | 15 | 13% | |
| Gastroenterology | 3 | 3% | |
| Rheumatology | 3 | 3% | |
| PM&R | 2 | 2% | |
| Unknown | 15 | 13% | |
| Indication | 115 | ||
| Fibromyalgia | 70 | 61% | |
| Chronic Pain | 13 | 11% | |
| ME/CFS | 9 | 8% | |
| Multiple Sclerosis | 7 | 6% | |
| Myofascial Pain Syndrome | 4 | 3% | |
| Chronic Abdominal Pain | 3 | 3% | |
| CRPS | 2 | 2% | |
| Chronic Neck Pain | 2 | 2% | |
| Chronic Low Back Pain | 1 | 1% | |
| Chronic Leg Pain | 1 | 1% | |
| Postprandial Pain | 1 | 1% | |
| Chronic Migraine | 1 | 1% | |
| Pityriasis Rubra Pilaris Type 2 Adult | 1 | 1% | |
| Sample with Data (n) | Mean (SD) or n (%) | ||
|---|---|---|---|
| Started Prescription | 98 | 92 | 94% |
| Starting Naltrexone Daily Dose (mg) | 107 | 2.9 | 1.6 |
| (Minimum–Maximum) | (0.3–6.0) | ||
| Final Naltrexone Daily Dose (mg) | 109 | 4.2 | 1.0 |
| (Minimum–Maximum) | (0.8–9.0) | ||
| Perceived Benefit | 68 | 44 | 65% |
| Reported Side Effects | 98 | 11 | 11% |
| Concomitant Medications | 112 | ||
| Any Analgesic | 67 | 60% | |
| Gabapentinoid | 41 | 37% | |
| SNRI | 18 | 16% | |
| Muscle Relaxant | 17 | 15% | |
| Opioid | 12 | 11% | |
| Tramadol | 12 | 11% | |
| Tricyclic Antidepressant | 9 | 8% | |
| Discontinued Naltrexone | 97 | 36 | 37% |
| Length of Trial (days) | 36 | 179 | 160 |
| (Minimum–Maximum) | (7–720) | ||
| n | |
|---|---|
| Nausea/vomiting | 4 |
| Headaches | 3 |
| Anxiety | 3 |
| Restlessness | 2 |
| Dizziness | 2 |
| Insomnia | 2 |
| Sweats/hot flashes | 2 |
| Fatigue | 1 |
| Chills | 1 |
| Nightmares | 1 |
| Decreased appetite | 1 |
| Leg pain | 1 |
| Bloating | 1 |
| Constipation | 1 |
| Depression | 1 |
| Hypertension | 1 |
| Odds of Perceived Benefit | ||||
|---|---|---|---|---|
| Variable | n | Odds Ratio | (95% CI) | p-Value |
| Gender | 68 | 1.06 | (0.25–3.95) | 0.94 |
| Age | 59 | 1.00 | (0.97–1.04) | 0.82 |
| Any Concomitant Analgesic | 68 | 0.87 | (0.30–2.39) | 0.78 |
| Gabapentinoid | 68 | 1.14 | (0.41–3.36) | 0.80 |
| Opioid | 68 | 0.70 | (0.14–3.83) | 0.66 |
| Tricyclic Antidepressant | 68 | 0.24 | (0.03–1.32) | 0.11 |
| Tramadol | 68 | 2.08 | (0.45–14.81) | 0.39 |
| SNRI | 68 | 0.72 | (0.20–2.71) | 0.61 |
| Muscle Relaxant | 68 | 0.90 | (0.20–4.72) | 0.89 |
| Final LDN Dose | 67 | 1.16 | (0.70–2.00) | 0.56 |
| Odds of Discontinuation | ||||
| Variable | n | Odds Ratio | (95% CI) | p-value |
| Gender | 97 | 1.22 | (0.39–4.21) | 0.74 |
| Age | 82 | 1.01 | (0.98–1.04) | 0.51 |
| Any Concomitant Analgesic | 97 | 1.59 | (0.68–3.82) | 0.29 |
| Gabapentinoid | 97 | 1.13 | (0.48–2.64) | 0.78 |
| Opioid | 97 | 1.81 | (0.47–6.97) | 0.38 |
| Tricyclic Antidepressant | 97 | 1.78 | (0.40–8.00) | 0.44 |
| Tramadol | 97 | 1.81 | (0.47–6.97) | 0.38 |
| SNRI | 97 | 1.89 | (0.63–5.68) | 0.25 |
| Muscle Relaxant | 97 | 1.16 | (0.36–3.53) | 0.80 |
| Final LDN Dose | 96 | 0.77 | (0.48–1.19) | 0.26 |
| LDN-Only Subgroup (n = 45) | LDN-Plus-Concomitant Analgesics Subgroup (n = 67) | |||||||
|---|---|---|---|---|---|---|---|---|
| Sample with Data (n) | Mean (SD) or n (%) | Sample with Data (n) | Mean (SD) or n (%) | T-Test or Χ2 | p-Value | |||
| Age (y) | 41 | 45 | 14 | 56 | 50 | 15 | −1.60 | 0.11 |
| Gender | 45 | 67 | 3.98 | 0.05 | ||||
| Female | 43 | 96% | 53 | 79% | ||||
| Male | 1 | 2% | 13 | 19% | ||||
| Non-binary | 1 | 2% | 0 | 0% | ||||
| Transgender | 0 | 0% | 1 | 1% | ||||
| Indication | 45 | 67 | 9.66 | 0.72 | ||||
| Fibromyalgia | 30 | 67% | 38 | 57% | ||||
| Chronic Pain | 4 | 9% | 8 | 12% | ||||
| ME/CFS | 3 | 7% | 6 | 9% | ||||
| Multiple Sclerosis | 3 | 7% | 3 | 4% | ||||
| Myofascial Pain Syndrome | 0 | 0% | 4 | 6% | ||||
| Chronic Abdominal Pain | 1 | 2% | 2 | 3% | ||||
| CRPS | 1 | 2% | 1 | 1% | ||||
| Chronic Neck Pain | 1 | 2% | 1 | 1% | ||||
| Chronic Low Back Pain | 0 | 0% | 1 | 1% | ||||
| Chronic Leg Pain | 0 | 0% | 1 | 1% | ||||
| Postprandial Pain | 1 | 2% | 0 | 0% | ||||
| Chronic Migraine | 1 | 2% | 0 | 0% | ||||
| Pityriasis Rubra Pilaris Type 2 | 0 | 0% | 1 | 1% | ||||
| Started LDN Prescription | 40 | 38 | 95% | 56 | 54 | 96% | <0.01 | >0.99 |
| Starting LDN Daily Dose (mg) | 43 | 3.2 | 1.6 | 63 | 2.7 | 1.6 | 1.46 | 0.15 |
| (Minimum–Maximum) | (0.5–6.0) | (0.3–4.5) | ||||||
| Final LDN Daily Dose (mg) | 44 | 4.3 | 1.1 | 64 | 4.2 | 0.9 | 0.76 | 0.45 |
| (Minimum–Maximum) | (1.0–9.0) | (0.8–6.0) | ||||||
| Perceived Benefit | 27 | 18 | 67% | 41 | 26 | 63% | <0.01 | >0.99 |
| Reported Side Effects | 40 | 3 | 8% | 56 | 8 | 14% | 0.46 | 0.50 |
| Discontinued LDN | 39 | 12 | 31% | 58 | 24 | 41% | 0.72 | 0.40 |
| Length of Trial (days) | 12 | 171 | 151 | 20 | 182 | 167 | −0.17 | 0.87 |
| (Minimum–Maximum) | (10–360) | (7–720) | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Driver, C.N.; D’Souza, R.S. Efficacy of Low-Dose Naltrexone and Predictors of Treatment Success or Discontinuation in Fibromyalgia and Other Chronic Pain Conditions: A Fourteen-Year, Enterprise-Wide Retrospective Analysis. Biomedicines 2023, 11, 1087. https://doi.org/10.3390/biomedicines11041087
Driver CN, D’Souza RS. Efficacy of Low-Dose Naltrexone and Predictors of Treatment Success or Discontinuation in Fibromyalgia and Other Chronic Pain Conditions: A Fourteen-Year, Enterprise-Wide Retrospective Analysis. Biomedicines. 2023; 11(4):1087. https://doi.org/10.3390/biomedicines11041087
Chicago/Turabian StyleDriver, C. Noelle, and Ryan S. D’Souza. 2023. "Efficacy of Low-Dose Naltrexone and Predictors of Treatment Success or Discontinuation in Fibromyalgia and Other Chronic Pain Conditions: A Fourteen-Year, Enterprise-Wide Retrospective Analysis" Biomedicines 11, no. 4: 1087. https://doi.org/10.3390/biomedicines11041087