
Neck Pain in Fibromyalgia: Treatment with Exercise and Mesotherapy
 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Clinical Evaluation
2.5. Mesotherapy Procedure
2.6. Rehabilitation Protocol
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia Pathogenesis and Treatment Options Update. Curr. Pain Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Fibromialgia: Prevalencia, perfiles epidemiológicos y costes económicos. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Scaturro, D.; Vitagliani, F.; Tomasello, S.; Filippetti, M.; Picelli, A.; Smania, N.; Mauro, G.L. Can the Combination of Rehabilitation and Vitamin D Supplementation Improve Fibromyalgia Symptoms at All Ages? J. Funct. Morphol. Kinesiol. 2022, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- Sumpton, J.E.; Moulin, D.E. Chapter 33—Fibromyalgia. Handb. Clin. Neurol. 2014, 119, 513–527. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Hooten, W.M. Advances in the diagnosis and management of neck pain. BMJ 2017, 358, j3221. [Google Scholar] [CrossRef]
- Nagakura, Y.; Takahashi, M.; Noto, T.; Sekizawa, T.; Oe, T.; Yoshimi, E.; Tamaki, K.; Shimizu, Y. Different pathophysiology underlying animal models of fibromyalgia and neuropathic pain: Comparison of reserpine-induced myalgia and chronic constriction injury rats. Behav. Brain Res. 2012, 226, 242–249. [Google Scholar] [CrossRef]
- Banati, R.B. Brain plasticity and microglia: Is transsynaptic glial activation in the thalamus after limb denervation linked to cortical plasticity and central sensitisation? J. Physiol. 2002, 96, 289–299. [Google Scholar] [CrossRef]
- Yao, X.; Li, L.; Kandhare, A.D.; Mukherjee-Kandhare, A.A.; Bodhankar, S.L. Attenuation of reserpine-induced fibromyalgia via ROS and serotonergic pathway modulation by fisetin, a plant flavonoid polyphenol. Exp. Ther. Med. 2020, 19, 1343–1355. [Google Scholar] [CrossRef] [Green Version]
- Starobova, H.; Nadar, E.I.; Vetter, I. The NLRP3 Inflammasome: Role and Therapeutic Potential in Pain Treatment. Front. Physiol. 2020, 11, 1016. [Google Scholar] [CrossRef]
- Calzaferri, F.; Ruiz-Ruiz, C.; De Diego, A.M.G.; De Pascual, R.; Méndez-López, I.; Cano-Abad, M.F.; Maneu, V.; Ríos, C.D.L.; Gandía, L.; García, A.G. The purinergic P2X7 receptor as a potential drug target to combat neuroinflammation in neurodegenerative diseases. Med. Res. Rev. 2020, 40, 2427–2465. [Google Scholar] [CrossRef]
- Bohár, Z.; Nagy-Grócz, G.; Fejes-Szabó, A.; Tar, L.; László, A.M.; Büki, A.; Szabadi, N.; Vraukó, V.; Vécsei, L.; Párdutz, A. Diverse effects of Brilliant Blue G administration in models of trigeminal activation in the rat. J. Neural Transm. 2015, 122, 1621–1631. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, R.; Fusco, R.; Siracusa, R.; Impellizzeri, D.; Peritore, A.; Gugliandolo, E.; Interdonato, L.; Sforza, A.; Crupi, R.; Cuzzocrea, S.; et al. Inhibition of P2X7 Purinergic Receptor Ameliorates Fibromyalgia Syndrome by Suppressing NLRP3 Pathway. Int. J. Mol. Sci. 2021, 22, 6471. [Google Scholar] [CrossRef] [PubMed]
- Nadal-Nicolás, Y.; Rubio-Arias, J.; Martínez-Olcina, M.; Reche-García, C.; Hernández-García, M.; Martínez-Rodríguez, A. Effects of Manual Therapy on Fatigue, Pain, and Psychological Aspects in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 4611. [Google Scholar] [CrossRef] [PubMed]
- Uysal, S.C.; Tüzün, E.H.; Eker, L.; Angın, E. Effectiveness of the muscle energy technique on respiratory muscle strength and endurance in patients with fibromyalgia. J. Back Musculoskelet. Rehabil. 2019, 32, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Suvarnnato, T.; Punttakul, R.; Uthaikhup, S.; Boucaut, R. Effect of specific deep cervical muscle exercises on functional disability, pain intensity, craniovertebral angle, and neck-muscle strength in chronic mechanical neck pain: A randomized controlled trial. J. Pain Res. 2019, 12, 915–925. [Google Scholar] [CrossRef] [Green Version]
- Childress, M.A.; Stuek, S.J. Neck Pain: Initial Evaluation and Management. Am. Fam. Physician 2020, 102, 150–156. [Google Scholar] [PubMed]
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.-A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 1–13. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Gard, G. Body awareness therapy for patients with fibromyalgia and chronic pain. Disabil. Rehabil. 2005, 27, 725–728. [Google Scholar] [CrossRef]
- Asaro, C.; Scaturro, D.; Tomasello, S.; Tumminelli, L.; Letizia Mauro, G. Synergistic Effect of Physical Therapy Plus Pharmacological Therapy with Eperisone in Tension-Type Cervicalgia. Muscles Ligaments Tendons J. 2019, 9, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Bravo, C.; Skjaerven, L.H.; Sein-Echaluce, L.G.; Catalan-Matamoros, D. Effectiveness of movement and body awareness therapies in patients with fibromyalgia: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2019, 55, 646–657. [Google Scholar] [CrossRef]
- Pulido-Martos, M.; Luque-Reca, O.; Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Acosta-Manzano, P.; Gavilán-Carrera, B.; McVeigh, J.G.; Geenen, R.; Delgado-Fernández, M.; et al. Physical and psychological paths toward less severe fibromyalgia: A structural equation model. Ann. Phys. Rehabil. Med. 2020, 63, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Araújo, F.M.; DeSantana, J.M. Physical therapy modalities for treating fibromyalgia. F1000Research 2019, 298, 2030. [Google Scholar] [CrossRef]
- Mercieca, C.; Borg, A.A. EULAR recommendations underplay importance of severe anxiety and depression in fibromyalgia treatment. Ann. Rheum. Dis. 2017, 76, e53. [Google Scholar] [CrossRef]
- Roberts, M.A. CMTL Effects of Patterns of Pressure Application on Resting Electromyography during Massage. Int. J. Ther. Massag. Bodyw. 2011, 30, 4. [Google Scholar]
- Paolucci, T.; Bellomo, R.G.; A Centra, M.; Giannandrea, N.; Pezzi, L.; Saggini, R. Mesotherapy in the treatment of musculoskeletal pain in rehabilitation: The state of the art. J. Pain Res. 2019, 12, 2391–2401. [Google Scholar] [CrossRef]
- Faetani, L.; Ghizzoni, D.; Ammendolia, A.; Costantino, C. Safety and efficacy of mesotherapy in musculoskeletal disorders: A systematic review of randomized controlled trials with meta-analysis. J. Rehabil. Med. 2021, 53, jrm00182. [Google Scholar] [CrossRef]
- E Ferrara, P.; Nigito, C.; Maccauro, G.; Ferriero, G.; Foti, C.; Ronconi, G. Efficacy of diclofenac mesotherapy for the treatment of chronic neck pain in spondylartrosis. Minerva Med. 2019, 110, 262–264. [Google Scholar] [CrossRef]
- Akbas, I.; Kocak, A.O.; Kocak, M.B.; Cakir, Z. Comparison of intradermal mesotherapy with systemic therapy in the treatment of low back pain: A prospective randomized study. Am. J. Emerg. Med. 2020, 38, 1431–1435. [Google Scholar] [CrossRef]
- Ronconi, G.; Ferriero, G.; Nigito, C.; Foti, C.; Maccauro, G.; E Ferrara, P. Efficacy of intradermal administration of diclofenac for the treatment of nonspecific chronic low back pain: Results from a retrospective observational study. Eur. J. Phys. Rehabil. Med. 2019, 55, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.E.; Ferriero, G.; Salini, S.; Foti, G.; Maccauro, G.; Mammucari, M.; Ronconi, G. Treatment of chronic persistent spinal pain with diclofenac mesotherapy in patients with spondylarthrosis. J. Biol. Regul. Homeost. Agents. 2020, 34. online ahead of print. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Young, I.A.; Dunning, J.; Butts, R.; Mourad, F.; Cleland, J.A. Reliability, construct validity, and responsiveness of the neck disability index and nric pain rating scale in patients with mechanical neck pain without upper extremity symptoms. Physiother. Theory Pract. 2018, 35, 1328–1335. [Google Scholar] [CrossRef]
- Assumpção, A.; Matsutani, L.A.; Yuan, S.L.; Santo, A.S.; Sauer, J.; Mango, P.; Marques, A.P. Muscle stretching exercises and resistance training in fibromyalgia: Which is better? A three-arm randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 663–670. [Google Scholar] [CrossRef]
- Hoffman, D.L.; Dukes, E.M. The health status burden of people with fibromyalgia: A review of studies that assessed health status with the SF-36 or the SF-12. Int. J. Clin. Pract. 2008, 62, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Kocak, A.O. Intradermal mesotherapy versus systemic therapy in the treatment of musculoskeletal pain: A prospective randomized study. Am. J. Emerg. Med. 2019, 37, 2061–2065. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.L.; Gaesser, G.A.; Butcher, J.D.; Despres, J.-P.; Dishman, R.K.; Franklin, B.A.; Garber, C.E. ACSM Position Stand: The Recommended Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory and Muscular Fitness, and Flexibility in Healthy Adults. Med. Sci. Sports Exerc. 1998, 30, 975–991. [Google Scholar] [CrossRef]
- Scaturro, D.; Guggino, G.; Tumminelli, L.G.; Ciccia, F.; Mauro, G.L. An intense physical rehabilitation programme determines pain relief and improves the global quality of life in patients with fibromyalgia. Clin. Exp. Rheumatol. 2019, 37, 670–675. [Google Scholar] [PubMed]
- da Silva, A.G.; Machado, E.R.; de Almeida, L.M.; Nunes, R.M.M.; Pena Giesbrecht, P.C.; Mamed Costa, R.; Costa, H.B.; Romano, W.; Kuster, R.M. A clinical trial with Brazilian Arnica (Solidago chilensis Meyen) glycolic ex-tract in the treatment of tendonitis of flexor and extensor tendons of wrist and hand. Phytother. Res. 2015, 29, 864–869. [Google Scholar] [CrossRef]
- Costantino, C.; Marangio, E.; Coruzzi, G. Mesotherapy versus Systemic Therapy in the Treatment of Acute Low Back Pain: A Randomized Trial. Evid Based Complement Alternat Med. 2011, 2011, 317183. [Google Scholar] [CrossRef] [Green Version]
- Viscito, R.; Ferrara, P.E.; Ljoka, C.; Pascuzzo, R.; Maggi, L.; Ronconi, G.; Foti, C. Mesotherapy as a treatment of pain and disability in patients affected by neck pain in spondylartrosis. Ig. Sanita Pubblica 2018, 74, 95–101. [Google Scholar]
- Ferrara, P.E.; Ronconi, G.; Viscito, R.; Pascuzzo, R.; Rosulescu, E.; Ljoka, C.; Maggi, L.; Ferreiro, G.; Foti, G. Efficacy of mesotherapy using drugs versus normal saline solution in chronic spinal pain: A retrospective study. Int. J. Rehabil. Res. 2017, 40, 171–174. [Google Scholar] [CrossRef]
- Crenna, P.; Mancia, P. Reflex actions in mesotherapy. J. Mesother. 1981, 1, 29–40. [Google Scholar]
- Mammucari, M.; Gatti, A.; Maggiori, S.; A Bartoletti, C.; Sabato, A.F. Mesotherapy, definition, rationale and clinical role: A consensus report from the Italian Society of Mesotherapy. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 682–694. [Google Scholar]
- Mammucari, M.; Gatti, A.; Maggiori, S.; Sabato, A.F. Role of mesotherapy in musculoskeletal pain: Opinions from the italian society of mesotherapy. Evid. Based Complem. Altern. Med. 2012, 2012, 436959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borchers, A.T.; Gershwin, M.E. Fibromyalgia: A Critical and Comprehensive Review. Clin. Rev. Allergy Immunol. 2015, 49, 100–151. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Reina, M.D.; Núñez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Exercise therapy in fibromyalgia syndrome: A systematic review and meta-analysis of randomized clinical trials. BioMed Res. Int. 2017, 2356346. [Google Scholar] [CrossRef] [Green Version]
- Kayo, A.H.; Peccin, M.S.; Sanches, C.M.; Trevisani, V.F.M. Effectiveness of physical activity in reducing pain in patients with fibromyalgia: A blinded randomized clinical trial. Rheumatol. Int. 2012, 32, 2285–2292. [Google Scholar] [CrossRef]
- Paolucci, T.; Piccinini, G.; Trifan, P.; Zangrando, F.; Saraceni, V. Efficacy of Trigger Points Mesotherapy for the Treatment of Chronic Neck Pain: A Short Term Retrospective Study. Int. J. Phys. Ther. Rehabil. 2016, 2, 113. [Google Scholar] [CrossRef] [PubMed]
- Plachouri, K.; Georgiou, S. Mesotherapy: Safety profile and management of complications. J. Cosmet. Dermatol. 2019, 18, 1601–1605. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (n = 78) | Treatment Group (n = 39) | Placebo Group (n = 39) | p-Value |
|---|---|---|---|---|
| Age, mean ± SD | 49.3 ± 6.2 | 50.1 ± 4.7 | 48.7 ± 4.4 | 0.18 |
| Sex, n (%) | 0.21 | |||
| Female | 71 (91.1) | 34 (87.2) | 37 (94.8) | |
| Male | 7 (8.9) | 5 (12.8) | 2 (5.2) | |
| BMI (Kg/m2), mean ± SD | 27.6 ± 3.4 | 28.3 ± 4.1 | 27.3 ± 3.8 | 0.27 |
| Comorbidity, n (%) | <0.05 | |||
| Yes | 45 (57.7) | 20 (51.3) | 25 (64.1) | |
| No | 33 (42.3) | 19 (48.7) | 14 (35.9) | |
| Muscle tension, n (%) | 0.38 | |||
| Yes | 68 (87.2) | 35 (89.7) | 33 (84.6) | |
| No | 10 (12.8) | 4 (10.3) | 6 (15.4) | |
| NRS, mean ± SD | 7.3 ± 2.1 | 7.4 ± 1.2 | 7.5 ± 1.4 | 0.73 |
| NDI, mean ± SD | 36.2 ± 5.3 | 35.6 ± 5.2 | 37.4 ± 5.4 | 0.14 |
| SF-12 scale, mean ± SD | 17.4 ± 8.2 | 18.3 ± 4.1 | 18.6 ± 3.8 | 0.74 |
| FIQ, mean ± SD | 55.9 ± 6.1 | 55.7 ± 7.7 | 56.4 ± 5.8 | 0.65 |
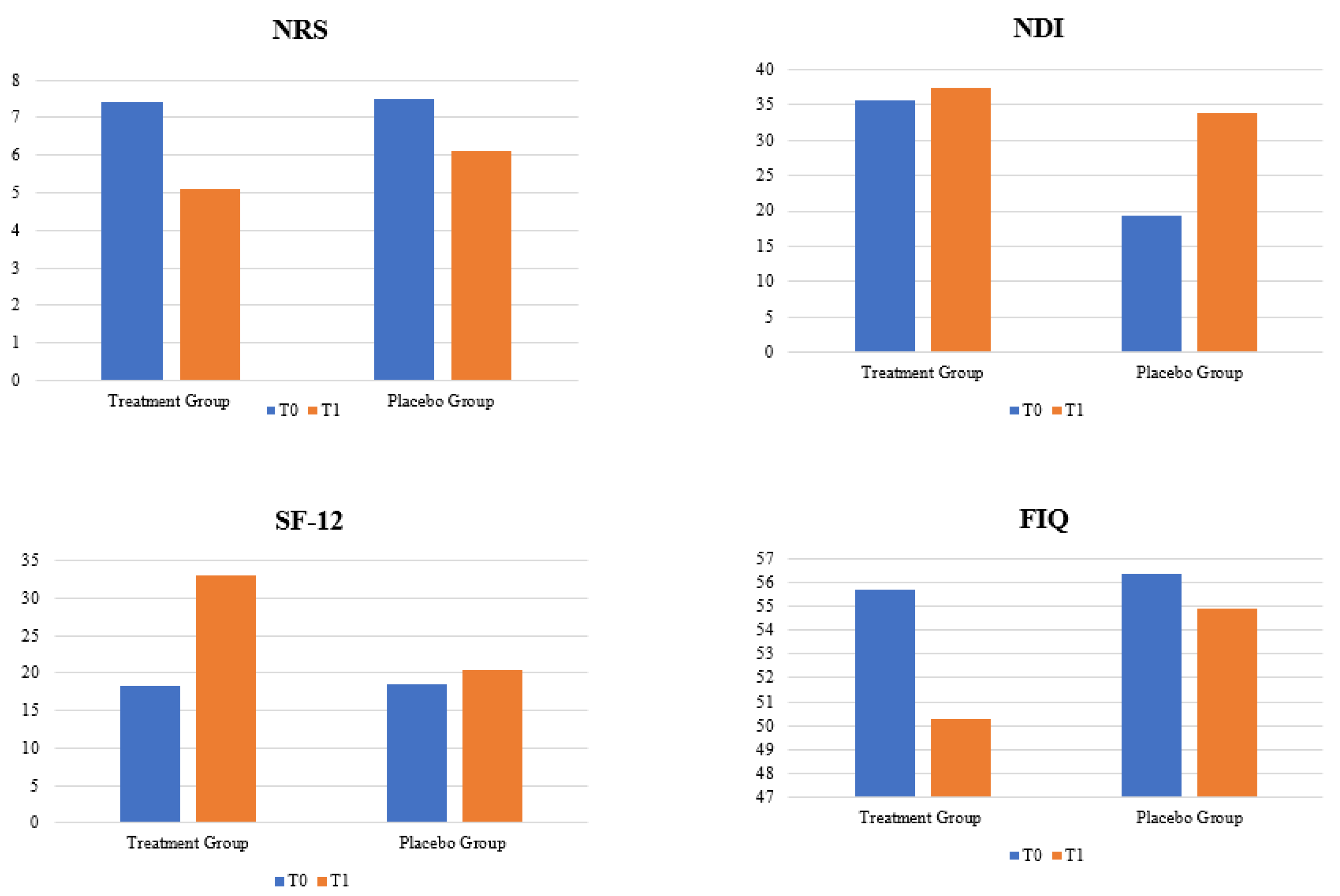
| Characteristics | Treatment Group (n = 39) | Placebo Group (n = 39) |
|---|---|---|
| NRS, mean ± SD | ||
| T0 | 7.4 ± 1.2 | 7.5 ± 1.4 |
| T1 | 5.1 ± 1.11 | 6.1 ± 1.6 |
| p-value | <0.05 | <0.05 |
| NDI, mean ± SD | ||
| T0 | 35.6 ± 5.2 | 37.4 ± 5.4 |
| T1 | 19.3 ± 3.4 | 33.8 ± 4.8 |
| p-value | <0.05 | 0.11 |
| SF-12, mean ± SD | ||
| T0 | 18.3 ± 4.1 | 18.6 ± 3.8 |
| T1 | 33.1 ± 2.4 | 20.3 ± 4.8 |
| p-value | <0.05 | 0.09 |
| FIQ, mean ± SD | ||
| T0 | 55.7 ± 7.7 | 56.4 ± 5.8 |
| T1 | 50.3 ± 4.7 | 54.9 ± 4.5 |
| p-value | 0.09 | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaturro, D.; Vitagliani, F.; Signa, G.; Tomasello, S.; Tumminelli, L.G.; Picelli, A.; Smania, N.; Letizia Mauro, G. Neck Pain in Fibromyalgia: Treatment with Exercise and Mesotherapy. Biomedicines 2023, 11, 892. https://doi.org/10.3390/biomedicines11030892
Scaturro D, Vitagliani F, Signa G, Tomasello S, Tumminelli LG, Picelli A, Smania N, Letizia Mauro G. Neck Pain in Fibromyalgia: Treatment with Exercise and Mesotherapy. Biomedicines. 2023; 11(3):892. https://doi.org/10.3390/biomedicines11030892
Chicago/Turabian StyleScaturro, Dalila, Fabio Vitagliani, Gabriele Signa, Sofia Tomasello, Luigi Giuseppe Tumminelli, Alessandro Picelli, Nicola Smania, and Giulia Letizia Mauro. 2023. "Neck Pain in Fibromyalgia: Treatment with Exercise and Mesotherapy" Biomedicines 11, no. 3: 892. https://doi.org/10.3390/biomedicines11030892