1. Introduction
To date, sodium–glucose cotransporter 2 inhibitors (SGLT2i) have demonstrated a major therapeutic advance in patients with heart failure (HF). Large-scale randomized controlled trials (RCTs) have shown that they reduce the risk of hospitalization for HF or cardiovascular death in patients with HF with reduced left ventricular ejection fraction (HFrEF) [
1,
2]. Thus, dapagliflozin and empagliflozin, an example of SGLT2i, have received a class I indication for HFrEF patients in international guidelines [
3,
4]. The EMPEROR-Preserved trial with empagliflozin and DELIVER trial with dapagliflozin have shown a reduction in HF hospitalization in patients with HF with preserved left ventricular ejection fraction (HFpEF) [
5,
6]. Furthermore, a reduction in HF hospitalization was reported in patients with HF, independently of the presence of diabetes mellitus (DM). Thus, SGLT2i are prescribed in patients with chronic HF accompanying a wide range of values of left ventricular ejection fraction (LVEF). Recently, several RCTs suggested that SGLT2i might exert a beneficial effect on the cardiovascular outcome even in hospitalized or recently discharged patients with HF, in addition to those with chronic HF [
7,
8,
9].
However, our team previously found that some studies that initiated SGLT2i terminated SGLT2i for a variety of reasons [
10,
11]. Patients who terminated SGLT2i had worse clinical outcomes compared with those who continued SGLT2i. Thus, we should pay attention to the negative aspect of SGLT2i therapy. Given their pleiotropic effect, several adverse drug reactions including genital and urinary tract infection [
12], volume depletion [
13], diabetic ketoacidosis (DKA) [
14], bone fractures [
15], and amputation [
16] might be increased.
Previous large-scale RCTs demonstrated that there was no notable excess of serious treatment-emergent adverse events during SGLT2i therapy. Nevertheless, minor adverse effects of SGLT2i treatment are potentially numerous, and real-world data that reflect actual practice should be useful in identifying them. Of note, although clinical implication of early administration of SGLT2i was investigated in several RCTs including the SOLOIST-WHF trial and EMPULSE trial, whether early-administered SGLT2i can be continued over a longer observational period remains uncertain.
An abundant number of comorbidities including HF and other baseline characteristics may affect the extent of SGLT2i treatment and disturb continuation of SGLT2i therapy. Such risk factors associated with the termination of SGLT2i are of great importance for clinicians in determining whether to initiate SGLT2i and managing patients receiving SGLT2i over a long-term therapeutic period. In the present study, we investigated the factors associated with post-discharge discontinuation of SGLT2i, which was initiated during index hospitalization soon after the stabilization of HF.
2. Materials and Methods
This was a single-center, retrospective observational study to investigate the baseline factors associated with the discontinuation of SGLT2i, which was initiated during index hospitalization. This study was carried out in accordance with the principles outlined in the Declaration of Helsinki, and the institutional ethics board of Toyama University Hospital approved the study protocol (#R2015154, approval date 11 April 2016). Written informed consent was obtained from all of the participants beforehand.
2.1. Study Population
Patients who had been admitted for HF, which was diagnosed according to the Framingham criteria, at our institute between April 2016 and September 2021 were included in this study. Most of the patients had New York Heart Association (NYHA) class III/IV symptoms upon admission. All patients were treated with guideline-directed medical therapy for HF, including renin–angiotensin system inhibitors or angiotensin receptor–neprilysin inhibitors, beta-blockers, mineralocorticoid receptor antagonists, and diuretics, if applicable. Patients who newly received SGLT2i during their index hospitalization immediately following the stabilization of hemodynamics were followed-up for 12 months following index discharge (defined as day 0).
2.2. Exclusion Criteria
We excluded the following patients: age < 20 years, end-stage renal failure with estimated glomerular filtration rate (eGFR) < 15 mL/min/1.73 m2, use of durable left ventricular assist devices, pregnancy or breastfeeding, and current use of SGLT2i during index hospitalization. Patients who stopped taking SGLT2i during index hospitalization were excluded. Adjustment of medical therapy was permitted as a real-world clinical practice. Patients who were lost to follow-up during the 12-month observational period were also excluded. Patients who died due to non-cardiovascular disease were excluded.
2.3. Study Design and Data Collection
Baseline characteristics including demographics and laboratory data at index discharge were retrieved. The eGFR was calculated using the guidelines from the Chronic Kidney Disease Epidemiology Collaboration. Plasma B-type natriuretic peptide (BNP) level and eGFR were retrospectively retrieved at the 12-month follow-up. Standard echocardiographic findings during index hospitalization were retrieved. For the present analysis, participants were divided into HFrEF (LVEF < 40%), HfmrEF (LVEF 40–49%), and HfpEF (LVEF ≥ 50%) groups. We defined DM as patients satisfying glycated hemoglobin (HbA1c) ≥ 6.5% or receiving antidiabetic treatment. Bacterial infections included symptomatic bacteriuria or cases where bacterial cultures from sources such as blood, urine, or stool were positive. When patients died from cardiovascular causes, they were censored at the time of events.
2.4. Study Endpoints
The primary outcome was a discontinuation of SGLT2i during the 12 months following their index discharge. Baseline characteristics that would significantly affect the primary outcome were investigated. The secondary outcome was the changes in plasma BNP level and eGFR during the observational period.
2.5. Statistical Analyses
Statistical analysis was conducted using JMP® 15.0 (SAS Institute Inc., Cary, NC, USA). The level of significance was set at two-tailed p < 0.050. Continuous variables are presented as the median and interquartile range unless specifically stated. Categorical variables are presented as absolute numbers and percentages. The Wilcoxon test was used to compare continuous parameters, and Pearson’s χ2 test was used for comparison of categorical variables.
Univariable and multivariable analyses with logistic regression models were conducted to calculate the adjusted odds ratio to assess the influence of various baseline parameters on the discontinuation of SGLT2i. Variables deemed as significant (p < 0.050) in the univariate analyses were enrolled in the multivariate analyses. Time-to-event outcomes were evaluated using Kaplan–Meier estimates and the two treatment groups were compared with the use of log-rank test statistics.
3. Results
3.1. Follow-Up and Patient Characteristics
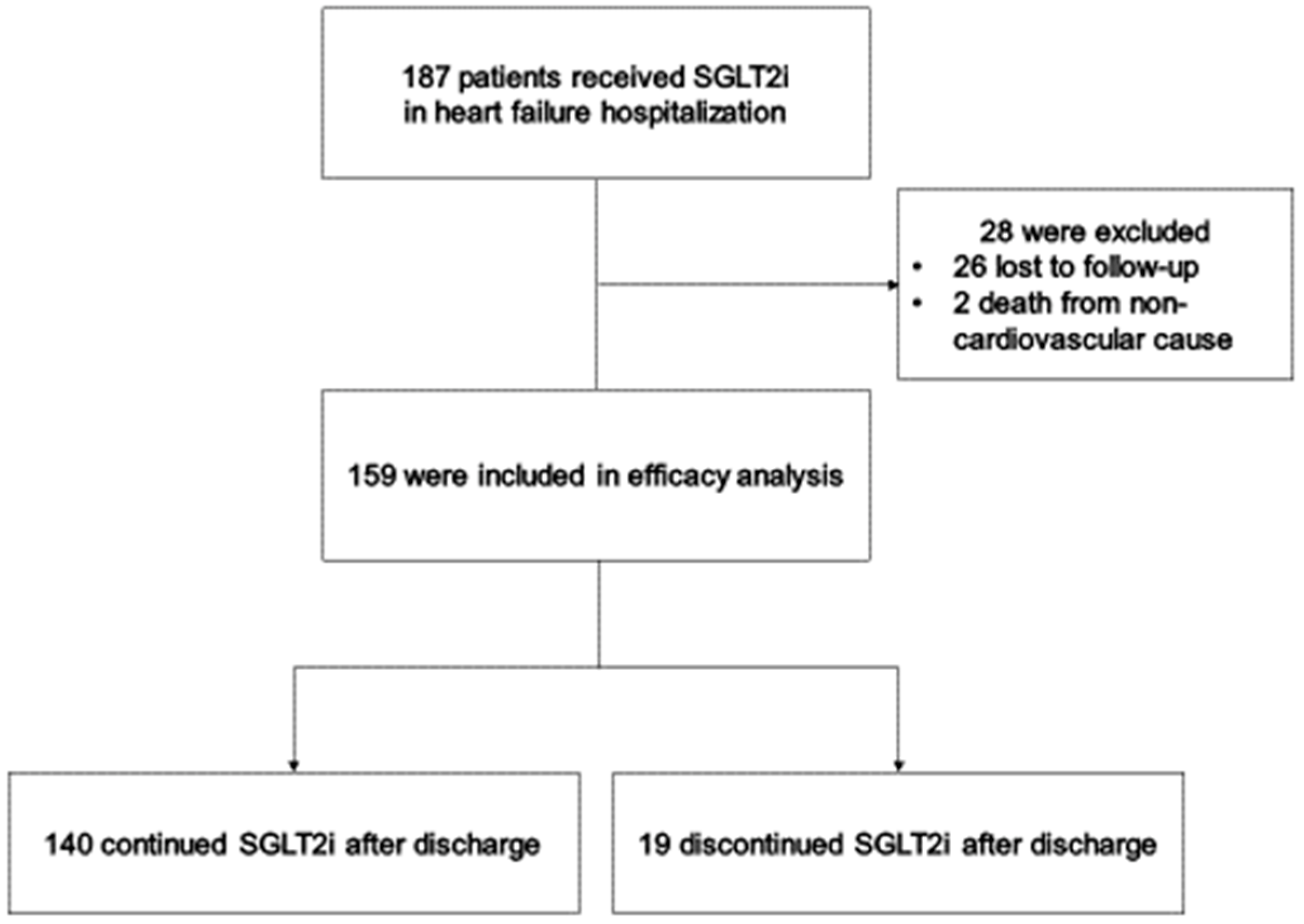
Totally, 187 patients met the inclusion criteria. Of them, 2 died from non-cardiovascular causes, and 26 patients were lost to follow-up during the observational period. Finally, 159 patients were included in this study (
Figure 1).
Table 1 lists the baseline characteristics obtained at index discharge. The median age was 73 (64–81) years and 36% of patients were women. NYHA class III/IV symptoms were noted in 36 patients (23%). HFrEF was noted in 62 patients (39%), HFmrEF in 42 patients (26%), and HFpEF in 55 patients (35%). DM was noted in 123 patients (77%) (all of them were type 2). As for the types of SGLT2i, 37 patients received canagliflozin, 82 received dapagliflozin, and 40 received empagliflozin. All patients receiving canagliflozin had a history of DM.
3.2. Causes of Primary Outcome
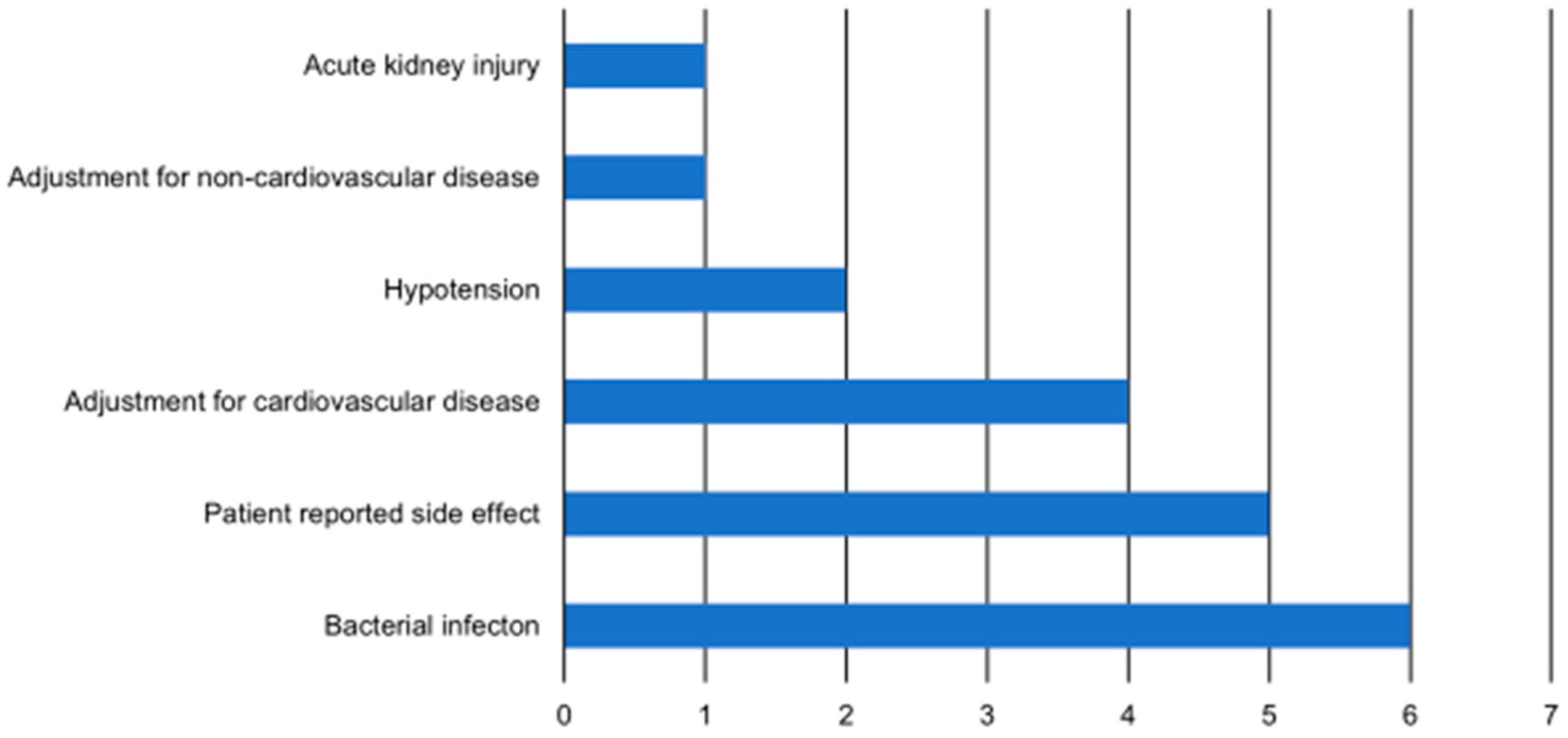
As a primary outcome, a total 19 of patients (12.0%) encountered the discontinuation of SGLT2i. The most common reasons for SGLT2i discontinuation were bacterial infection (
n = 6, 32%), followed by patient-reported side effects (
n = 5, 26%). The side effects reported by patients included nocturia, anorexia, pruritus, and tiredness. Adjustment for treatment of cardiovascular disease was the third most common reason (
n = 4, 21%) (
Figure 2).
3.3. Prediction of Primary Outcome
Baseline characteristics stratified by achievement of primary endpoint are summarized in
Table 1. The level of serum albumin was lower in the discontinuation group than the continuation group. Medications for HF and DM were not statistically different between the two groups. There were no significant differences in the plasma BNP and eGFR levels at baseline between both groups.
Univariable and multivariable analyses demonstrated that serum albumin level (odds ratio = 0.23, 95% confidence interval = 0.07–0.76,
p = 0.016) was independently and negatively associated with the discontinuation of SGLT2i, and furosemide dosage (odds ratio = 1.02, 95% = confidence interval 1.00–1.05,
p = 0.046) was positively associated with the discontinuation of SGLT2i (
Table 2). Prevalence of DM was not associated with the primary outcome.
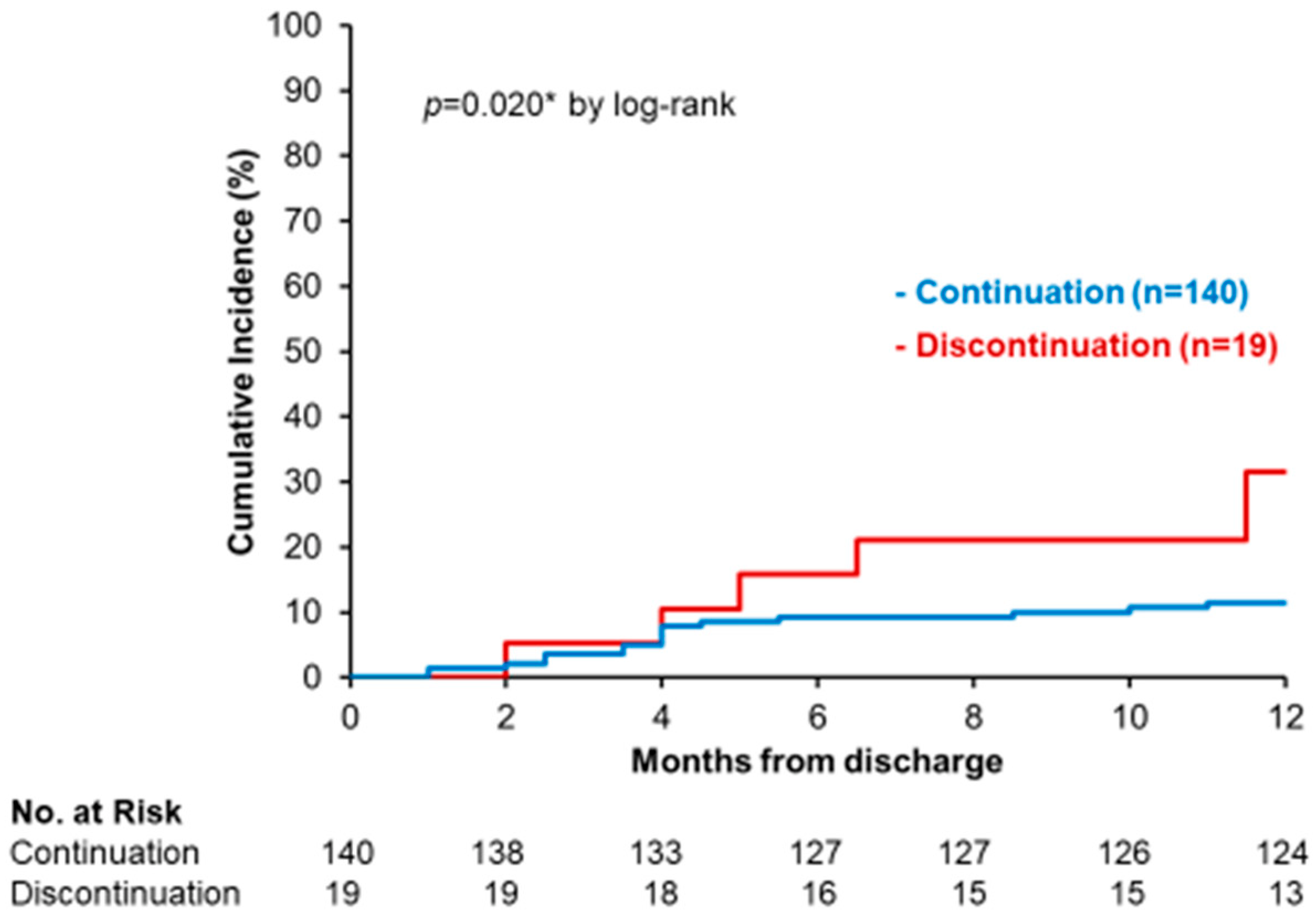
3.4. Impact of SGLT2i Discontinuation on Clinical Outcomes
Patients in the discontinued SGLT2i group had a higher incidence of recurrent HF hospitalization or cardiovascular death (32% vs. 11%,
p = 0.020;
Figure 3).
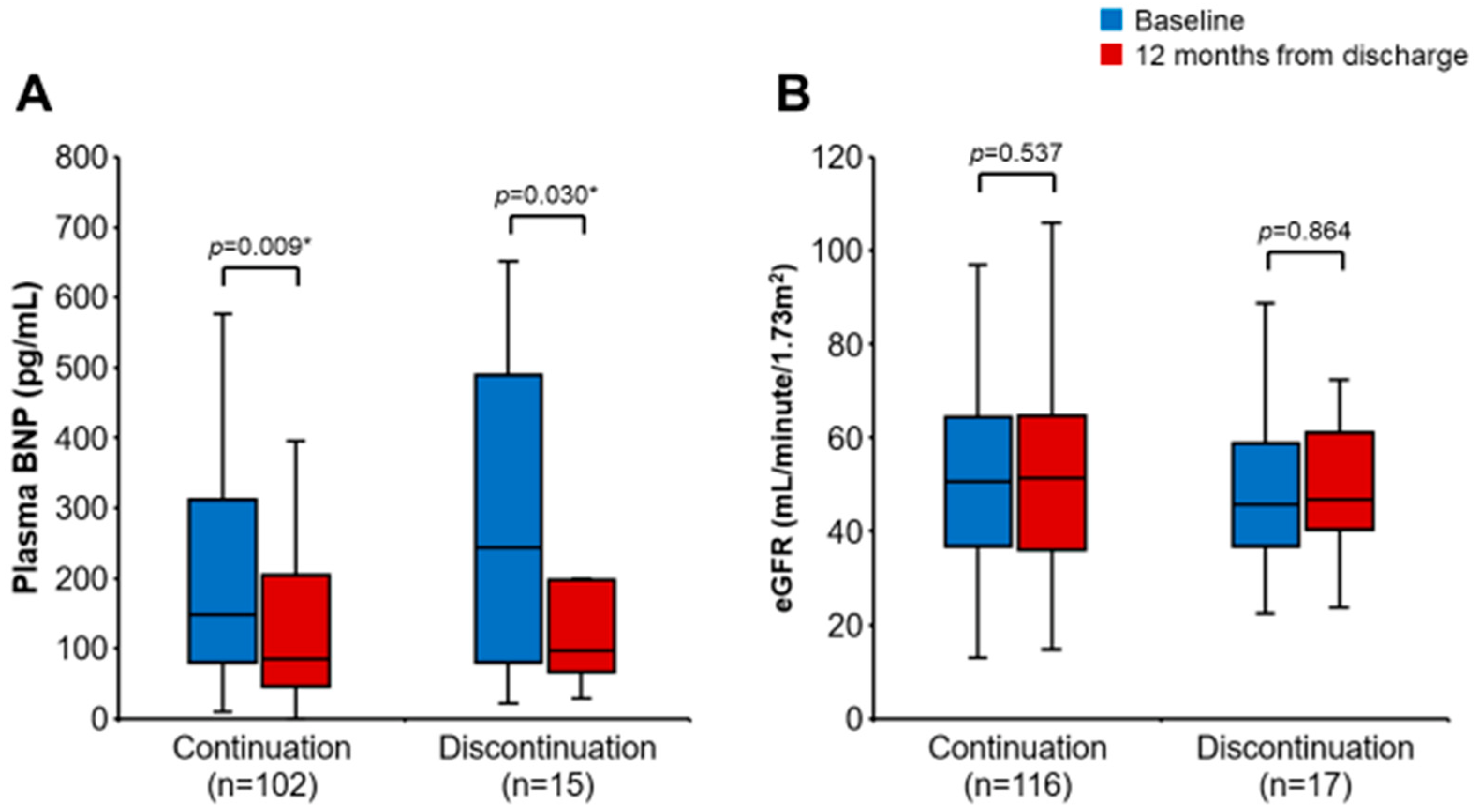
The changes in plasma BNP and eGFR were assessed in 117 and 133 patients, respectively, by excluding those who died during the observational period and those whose laboratory data were not retrieved. Changes in plasma BNP level from baseline are shown in
Figure 4. Plasma BNP levels decreased in patients with both continuation and discontinuation of SGLT2i from baseline to 12 months. The changes in plasma BNP were not different between the continued SGLT2i group and the discontinued SGLT2i group (−20.5 vs. −96.0 pg/mL,
p = 0.096). On the other hand, there were no significant changes in eGFR throughout the 12-month observation period in both groups. The changes in eGFR were not different between the continued SGLT2i group and the discontinued SGLT2i group (+0.65 vs. −0.60 mL/min/1.73 m
2,
p = 0.767).
4. Discussion
We investigated the factors associated with post-discharge discontinuation of SGLT2i in patients with HF. SGLT2i were initiated soon after the stabilization of hemodynamics during index hospitalization for HF. Among baseline characteristics at index discharge, a lower serum albumin level and a higher dose of furosemide were associated with discontinuation of SGLT2i following index discharge. Patients with discontinued SGLT2i had a higher incidence of re-hospitalization for HF or cardiovascular death during the 12-month observational period following index discharge. The changes in plasma BNP and eGFR were not significantly different between the discontinued SGLT2i group and the continued SGLT2i group.
4.1. Discontinuation of SGLT2i
In this study, SGLT2i were discontinued for reasons other than death in 19 patients (12.0%). Our discontinuation rate of 12.0% is similar to previously reported rates of 10.5–23.2% in large-scale RCTs [
1,
2,
5,
6]. However, the median follow-up durations of these RCTs (16.0–27.9 months) were longer than ours (12.0 months), and the risk of SGLT2i discontinuation in this study might be higher than in previous RCTs. In the SOLOIST-WHF trial and EMPULSE trial, both of which investigated the clinical implication of early initiation of SGLT2i, the rates of adverse events leading to the discontinuation of SGLT2i were lower than those in the present study (8.5% and 4.8%, respectively) [
7,
8]. These findings suggest difficulty in continuing SGLT2i in real-world populations.
A possible explanation for the high frequency of SGLT2i discontinuation was that our patients were included in this study soon after an episode of decompensated HF. Our population might be distinct from patients with chronic HF in most of the previous trials, since our patients were at a higher risk of cardiovascular events compared to patients in many of the other trials. Additionally, our population may have a higher risk of SGLT2i withdrawal in the vulnerable period, in which patients may have unstable volume status, renal function, and blood pressure and other HF therapies may require adjustment. Similarly, a subset of the DELIVER trial, which evaluated the response to dapagliflozin in hospitalized or recently discharged patients, reported that serious adverse events were more common in recently hospitalized patients compared with those without episodes of recent hospitalization [
17].
4.2. Diabetes and SGLT2i Discontinuation
Importantly, prevalence of DM was no longer a predictor of SGLT2i discontinuation in this study. Further, no patients stopped SGLT2i because of major hypoglycemia or DKA. Our observation regarding the safety of SGLT2i is consistent with previous trials and reports that the rate of SGLT2i discontinuation is not significantly different between participants with and without diabetes.
4.3. Hypoalbuminemia and SGLT2i Discontinuation
We demonstrated that a lower serum albumin level and a higher dose of furosemide were associated with SGLT2i discontinuation. It is worth noting that both low serum albumin levels and high doses of furosemide at baseline are strongly associated with an increased risk of HF [
18,
19,
20]. In addition, SGLT2i therapy for patients with malnutrition might not be encouraged due to its potential to progress catabolism. Although subsets of the DAPA-HF trial and DELIVER trial demonstrated that dapagliflozin improved cardiovascular outcomes regardless of frailty status [
21,
22], few studies assessed the efficacy and safety of SGLT2i in malnourished patients. Our finding suggests that caution should be exercised in using SGLT2i in patients with both HF and malnutrition.
4.4. High Dose of Loop Diuretics and SGLT2i Discontinuation
High incidence of SGLT2 discontinuation in patients with high doses of furosemide may be associated with adverse events of volume depletion. Although individual RCTs reported that the frequency of adverse events related to volume depletion did not differ between patients with SGLT2i and those without SGLT2i, a meta-analysis indicated that there is an increase in hypovolemia associated with SGLT2i treatment [
13]. Moreover, a previous study reported that SGLT2i therapy resulted in a significant augmentation of natriuresis when combined with loop diuretics [
23]. Inhibition of compensatory absorption of sodium in the Henle’s loop or distal tubule by loop diuretics in patients receiving SGLT2 may explain the findings of the study.
Therefore, co-administration of SGLT2i and high-dose loop diuretics might act complementarily via double blocking of proximal tubules and Henle’s loop, resulting in rapid volume depletion. This diuretic profile offers significant advantages in the management of volume status in patients with HF, whereas a robust diuretic response may result in excessive fluid loss. In this study, unexpected changes in plasma volume caused by co-administration of SGLT2i and high-dose loop diuretics may have led to SGLT2i discontinuation.
4.5. Outcomes of SGLT2i Discontinuation
In our study, patients who discontinued SGLT2i had a higher risk of re-hospitalization for HF or cardiovascular death. This result should be interpreted with caution since this is a retrospective observational study. We found that lower serum albumin levels and higher doses of furosemide were independently associated with SGLT2i discontinuation, and were also associated with an increased risk of HF. Patients who discontinued SGLT2i may be at higher risk of cardiovascular events than those who continued SGLT2i, making it difficult to assess the association between SGLT2i discontinuation and cardiovascular outcome in this study.
On the other hand, we previously reported that patients who discontinued SGLT2i at discharge from hospitalization for HF were more likely to be re-hospitalized for HF than those who continued SGLT2i [
11]. Previous findings may support a direct and independent prophylactic effect of SGLT2i on cardiovascular events for post-discharge patients in this study. RCTs demonstrated that SGLT2i improved cardiovascular outcomes, whereas few studies reported the effect of discontinuing SGLT2i on cardiovascular events. Additional research to confirm these findings and to understand the importance of continuing SGLT2i after discharge from hospitalization for HF is needed.
4.6. Limitations
This study has several limitations. First, this study was conducted retrospectively in a single center, and both overall sample size and number of patients reaching the primary outcome were small. Given the low event number, the number of potential confounders included in the multivariate analyses was limited. Similarly, limited patients were included in the analysis for secondary outcome. Furthermore, it is not possible to establish a cause–effect relationship given the retrospective observational study design. Second, other HF medications were also adjusted during the observational period in this study. Thus, it is challenging to assess the effect of SGLT2i alone. Lastly, our population received multiple types of SGLT2i in the present study. No RCTs have evaluated the efficacy of canagliflozin in patients with HF. It remains unclear whether such beneficial effects are consistent across individual SGLT2i. However, a recent retrospective cohort study reported that there was no significant difference in the risk of cardiovascular events including HF among patients taking dapagliflozin, canagliflozin, and empagliflozin [
24].
5. Conclusions
In this study, we found that 12.0% of patients who initiated SGLT2i soon after the stabilization of their HF during index hospitalization terminated SGLT2i therapy within 12 months following index discharge. The rate of discontinuation of SGLT2i is slightly higher than those of previous RCTs. The most common reason for the discontinuation of SGLT2i was bacterial infection. Lower serum albumin levels and higher doses of furosemide at the time of index discharge were independently associated with SGLT2 discontinuation after discharge from hospitalization for HF. Furthermore, SGLT2i discontinuation was associated with an increased risk of re-hospitalization for HF or cardiovascular death. Special attention should be paid when initiating and managing SGLT2i for those with such risk factors.
Author Contributions
M.N. (Masaki Nakagaito) wrote the draft. T.I. analyzed and interpreted the patient data. R.U. and M.N. (Makiko Nakamura) collected data and reviewed the draft. K.K. supervised the study. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Board of Toyama University Hospital (#R2015154; date of approval: 11 April 2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Voors, A.A.; Angermann, C.E.; Teerlink, J.R.; Collins, S.P.; Kosiborod, M.; Biegus, J.; Ferreira, J.P.; Nassif, M.E.; Psotka, M.A.; Tromp, J.; et al. The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: A multinational randomized trial. Nat. Med. 2022, 28, 568–574. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Schulze, P.C.; Bogoviku, J.; Westphal, J.; Aftanski, P.; Haertel, F.; Grund, S.; von Haehling, S.; Schumacher, U.; Möbius-Winkler, S.; Busch, M. Effects of Early Empagliflozin Initiation on Diuresis and Kidney Function in Patients with Acute Decompensated Heart Failure (EMPAG-HF). Circulation 2022, 146, 289–298. [Google Scholar] [CrossRef]
- Nakagaito, M.; Imamura, T.; Joho, S.; Ushijima, R.; Nakamura, M.; Kinugawa, K. Factors Associated with Recurrent Heart Failure during Incorporating SGLT2 Inhibitors in Patients Hospitalized for Acute Decompensated Heart Failure. J. Clin. Med. 2022, 11, 5027. [Google Scholar] [CrossRef]
- Nakagaito, M.; Imamura, T.; Joho, S.; Ushijima, R.; Nakamura, M.; Kinugawa, K. Efficacy of Continuing SGLT2 Inhibitors on Outcomes in Patients with Acute Decompensated Heart Failure. Int. Heart J. 2021, 62, 885–890. [Google Scholar] [CrossRef]
- Liu, J.; Li, L.; Li, S.; Jia, P.; Deng, K.; Chen, W.; Sun, X. Effects of SGLT2 inhibitors on UTIs and genital infections in type 2 diabetes mellitus: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 2824. [Google Scholar] [CrossRef]
- Rong, X.; Zhu, Y.; Wen, B.; Liu, K.; Li, X.; Gou, Q.; Chen, X. Risk of hypovolemia associated with sodium-glucose cotransporter-2 inhibitors treatment: A meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 2022, 9, 973129. [Google Scholar] [CrossRef]
- Liu, J.; Li, L.; Li, S.; Wang, Y.; Qin, X.; Deng, K.; Liu, Y.; Zou, K.; Sun, X. Sodium-glucose co-transporter-2 inhibitors and the risk of diabetic ketoacidosis in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 2020, 22, 1619–1627. [Google Scholar] [CrossRef]
- Adimadhyam, S.; Lee, T.A.; Calip, G.S.; Smith Marsh, D.E.; Layden, B.T.; Schumock, G.T. Sodium-glucose co-transporter 2 inhibitors and the risk of fractures: A propensity score-matched cohort study. Pharmacoepidemiol. Drug Saf. 2019, 28, 1629–1639. [Google Scholar] [CrossRef]
- Khouri, C.; Cracowski, J.L.; Roustit, M. SGLT-2 inhibitors and the risk of lower-limb amputation: Is this a class effect? Diabetes Obes. Metab. 2018, 20, 1531–1534. [Google Scholar] [CrossRef]
- Cunningham, J.W.; Vaduganathan, M.; Claggett, B.L.; Kulac, I.J.; Desai, A.S.; Jhund, P.S.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; et al. Dapagliflozin in Patients Recently Hospitalized wth Heart Failure and Mildly Reduced or Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2022, 80, 1302–1310. [Google Scholar] [CrossRef]
- Gopal, D.M.; Kalogeropoulos, A.P.; Georgiopoulou, V.V.; Tang, W.W.; Methvin, A.; Smith, A.L.; Bauer, D.C.; Newman, A.B.; Kim, L.; Harris, T.B.; et al. Serum albumin concentration and heart failure risk the Health, Aging, and Body Composition Study. Am. Heart J. 2010, 160, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Uthamalingam, S.; Kandala, J.; Daley, M.; Patvardhan, E.; Capodilupo, R.; Moore, S.A.; Januzzi, J.L., Jr. Serum albumin and mortality in acutely decompensated heart failure. Am. Heart J. 2010, 160, 1149–1155. [Google Scholar] [CrossRef]
- Hasselblad, V.; Gattis Stough, W.; Shah, M.R.; Lokhnygina, Y.; O’Connor, C.M.; Califf, R.M.; Adams, K.F., Jr. Relation between dose of loop diuretics and outcomes in a heart failure population: Results of the ESCAPE trial. Eur. J. Heart Fail. 2007, 9, 1064–1069. [Google Scholar] [CrossRef]
- Butt, J.H.; Dewan, M.P.; Merkely, B.; Belohlávek, J.; Drożdż, J.; Kitakaze, M.; Inzucchi, S.E.; Kosiborod, M.N.; Martinez, F.A.; Tereshchenko, S.; et al. Efficacy and Safety of Dapagliflozin According to Frailty in Heart Failure with Reduced Ejection Fraction: A Post Hoc Analysis of the DAPA-HF Trial. Ann. Intern. Med. 2022, 175, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.H.; Jhund, P.S.; Belohlávek, J.; de Boer, R.A.; Chiang, C.-E.; Desai, A.S.; Drożdzż, J.; Hernandez, A.F.; Inzucchi, S.E.; Katova, T.; et al. Efficacy and Safety of Dapagliflozin According to Frailty in Patients with Heart Failure: A Prespecified Analysis of the DELIVER Trial. Circulation 2022, 146, 1210–1224. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.; Rao, V.S.; Ivey-Miranda, J.; Fleming, J.; Mahoney, D.; Maulion, C.; Suda, N.; Siwakoti, K.; Ahmad, T.; Jacoby, D.; et al. Empagliflozin in Heart Failure: Diuretic and Cardiorenal Effects. Circulation 2020, 142, 1028–1039. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Kaneko, H.; Okada, A.; Itoh, H.; Matsuoka, S.; Fujiu, K.; Michihata, N.; Jo, T.; Takeda, N.; Morita, H.; et al. Comparison of cardiovascular outcomes between SGLT2 inhibitors in diabetes mellitus. Cardiovasc. Diabetol. 2022, 21, 67. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).







{kind=link}
{kind=link}
{kind=link}
{kind=link}