1. Introduction
Chronic kidney disease (CKD) is a major global health problem for which there are no curative drug treatments. Lifestyle-related diseases, such as obesity, hypertension, diabetes, and dyslipidemia, are currently important risk factors for CKD [
1]. Evidence supports a pathophysiological role for overactivation of the mineralocorticoid receptor in cardiorenal diseases, including CKD and diabetes, through inflammation and fibrosis that lead to progressive kidney and cardiovascular dysfunction [
2]. A nonsteroidal, selective mineralocorticoid receptor antagonist (MRA), finerenone, had more potent anti-inflammatory and anti-fibrotic effects than steroidal mineralocorticoid receptor antagonists in preclinical models [
3]. Very recently, the treatment with a selective MRA resulted in lower risks of CKD progression than placebo in patients with CKD and type 2 diabetes [
4]. The treatments for diabetes and obesity, such as sodium-glucose co-transporter 2 (SGLT2) inhibitors and glucagon-like peptide-1 receptor agonists (GLP-1RA), are emerging as promising treatment options in CKD and diabetic kidney disease (DKD) [
5,
6,
7,
8,
9,
10,
11]. The therapeutic intervention for risk factors, such as hypertension, obesity, and diabetes, have shown to reduce the onset and progression of CKD and DKA, and also have elucidated the molecular mechanisms for the progression of CKD and DKD.
Hyperuricemia is also a lifestyle-related disease, but most patients with hyperuricemia have no symptoms. Some studies recommend lower serum uric acid (UA) values < 5 mg/dL for the apparently healthy population, while the European League Against Rheumatism recommends a target of <6.0 mg/dL with medication for anti-hyperuricemia [
12,
13,
14]. Can the therapeutic intervention for hyperuricemia, the remaining risk factor for CKD, affect the progression of CKD? In the meta-analysis, the relative risk (RR) of CKD was 1.22 (95% confidence interval [CI], 1.16 to 1.28) per 1 mg/dL serum UA level increment [
15]. Another meta-analysis showed a significant positive association between elevated serum UA levels and the new-onset CKD at follow-ups (odds ratio [OR], 1.15; 95% CI, 1.05 to 1.25) [
16]. Hyperuricemia was found be an independent predictor for the development of newly diagnosed CKD. The meta-analyses which studied whether UA-lowering treatment (ULT) reduces the progression of CKD showed insufficient data on incidence of end-stage renal disease (ESRD) for analysis and the heterogeneity across included studies, suggesting that adequately powered randomized controlled trials (RCTs) are needed to establish whether ULT has beneficial renal effects [
17,
18]. The RCTs included in these meta-analyses on the effect of UTL on the onset and progression of CKD primarily used xanthin oxidase (XO) inhibitors, such as allopurinol and febuxostat.
A case–control study of 100 patients with primary gout and 72 healthy controls was undertaken [
19]. Most patients with gout showed lower UA clearance, fractional excretion of UA, excretion of UA per volume of glomerular filtration, and urinary UA to creatinine ratio than controls, suggesting that renal underexcretion is the main mechanism for the development of primary hyperuricemia. Therefore, considering the pathology of hyperuricemia, it was more reasonable to use uricosuric agents, such as benzbromarone, than XO inhibitors for the treatment of hyperuricemia. However, the reports on fulminant or sub-fulminant hepatitis due to benzbromarone kept us from using uricosuric agents for hyperuricemia patients [
20,
21].
Dotinurad, a novel selective urate reabsorption inhibitor (SURI) that has a potential for the treatment of hyperuricemia, reduces serum UA levels by selectively inhibiting urate transporter 1 (URAT1) [
22]. The RCT to evaluate the efficacy and safety of dotinurad in hyperuricemic Japanese patients (
n = 80) with or without gout was performed [
23], and dotinurad has been shown to have a substantial serum UA lowering effect in patients with hyperuricemia without serious adverse event. Very recently, we experienced a type 2 diabetic patients with CKD stage G4 whose serum creatinine and estimated glomerular filtration rate (eGFR) were remarkably improved by the additional use of dotinurad to SGLT2 inhibitor, GLP-1RA, angiotensin receptor blocker (ARB), and MRA, finerenone [
24].
Here, we aimed to study the Influences of dotinurad on metabolic parameters, including the markers for renal function and UA excretion in patients with hyperuricemia.
4. Discussion
Almost 60% of our patients had type 2 diabetes, and over 70% of patients have CKD; therefore, present study could observe the effect of a novel selective URAT1 inhibitor, dotinurad on metabolic and renal parameters in CKD and DKD patients. In other words, this study may clarify a clinical significance of URAT1 in CKD and DKD. Renal excretion of UA is the major regulator of serum UA concentration [
28,
29,
30]. In humans, reabsorption of UA into the blood plays a crucial role to regulate serum UA. The UA exchange is mediated by various molecules, such as URAT1, glucose transporter 9 (GLUT9), and ABCG2, expressed in renal proximal tubule [
31,
32,
33,
34]. Renal UA reabsorption is mainly mediated by URAT1 and GLUT9 [
33,
35,
36]. URAT1 is found in the apical membrane of proximal tubule epithelial cells [
37]. In addition, ABCG2 has been identified as a high-capacity UA exporter that mediates renal and/or extra-renal UA excretion [
38]. ABCG2 is now known to be involved as well in UA excretion into the intestine [
38].
We found that dotinurad improved UACR in addition to serum UA in all patients and patients who had not used UA-lowering drugs. An increase in urinary UA excretion measured by urinary UA/creatine can indicate the inhibitory effect of URAT1 by dotinurad. Dotinurad significantly increased urinary UA/creatine in all patients, especially in patients who switched from XO inhibitors. As almost 88% of our patients were UA underexcretion type, such patients should have been treated by uricosuric agents. As the effect of dotinurad on urinary UA/creatinine in each hyperuricemia phenotype showed, dotinurad significantly increased urinary UA/creatinine in patients with UA underexcretion type. More interesting is the effect of dotinurad on urinary UA/creatinine and serum UA levels in patients with renal UA overload type. In patients with renal UA overload type, there were no significant changes in urinary UA/creatinine by dotinurad. However, dotinurad remarkably reduced serum UA as compared with baseline. On the other hand, in patients with UA underexcretion type, despite significant increase in urinary UA/creatine, the decrease in serum UA levels was modest. This suggests that expression and/or function of URAT1 in patients with UA underexcretion type may be higher than those in patients with renal UA overload type. In short, while the same dose of dotinurad increases urinary UA excretion, the effect on serum UA levels may be insufficient in patients with UA underexcretion type with higher expressed URAT1; the same dose of dotinurad increases urinary UA excretion, but the effect on serum UA levels may be greater in patients with renal UA overload type with lower expressed URAT1. The increased protein level of URAT1 was observed in obesity/metabolic syndrome model mice [
39]. Upon high-purine load, insulin resistance enhances UA reabsorption as manifested by up-regulated URAT1 expression and reduces UA excretion in the Otsuka-Long-Evans-Tokushima Fatty rats [
40]. UA underexcretion type may be associated with insulin resistance, which is strongly involved in the development of CKD and DKD. Furthermore, this result suggests that dotinurad is effective to reduce serum UA by using appropriate dose in patients with both UA underexcretion type and renal UA overload type.
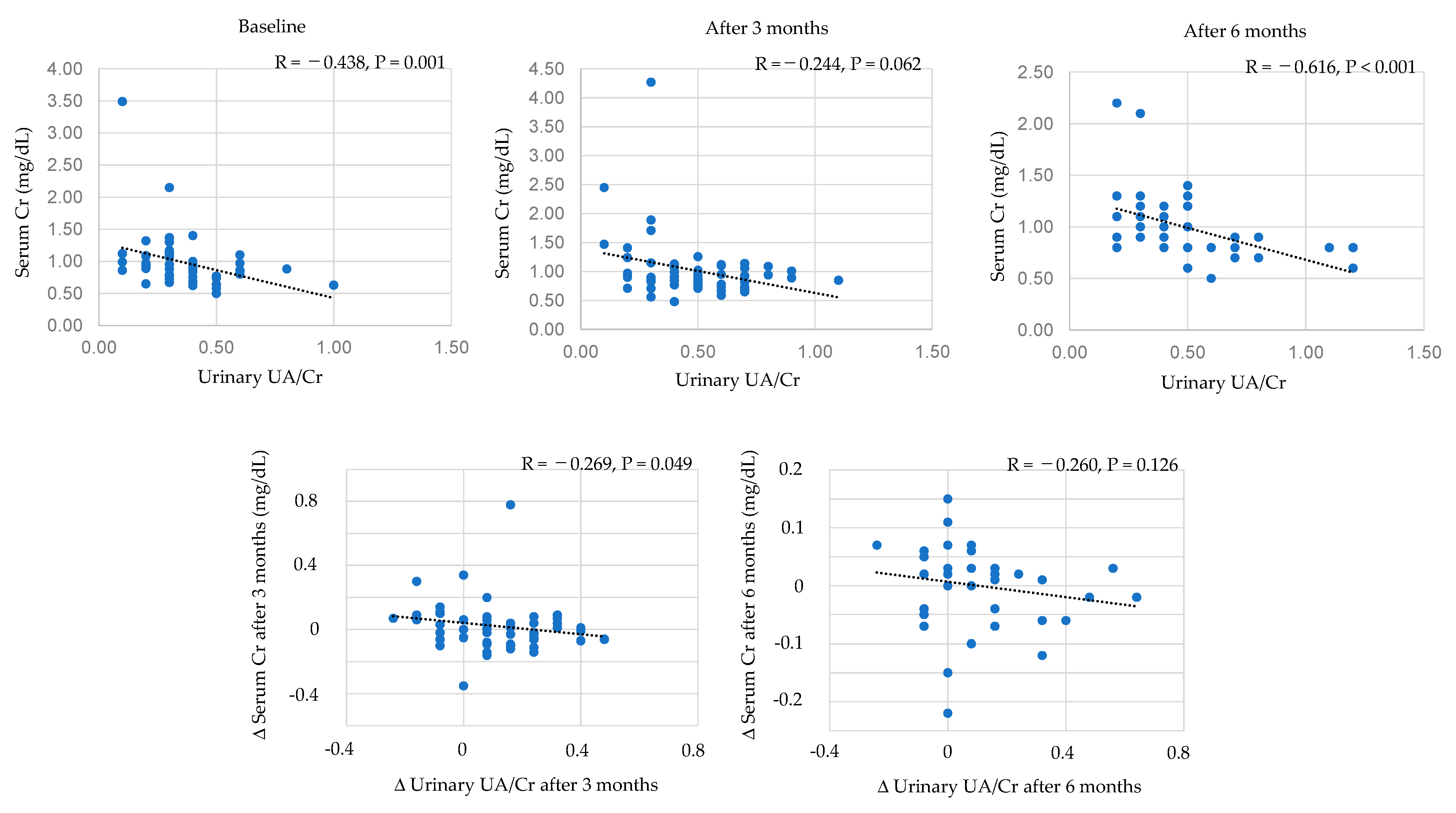
We analyzed the correlation of urinary UA/creatinine with the markers for CKD/DKD, such as serum creatinine levels and eGFR. Urinary UA/creatinine was strongly associated with lower serum creatinine levels and higher eGFR, and the increase in urinary UA/creatinine by dotinurad was also associated with an improvement of serum creatinine levels and eGFR. However, the influence of serum UA on serum creatinine levels was weak, and serum UA levels were not associated with eGFR. This suggests that urinary UA excretion may perform a more crucial role in progression of CKD/DKA as compared with serum UA levels.
We found an improvement in serum lipids, such as reduction in LDL-C and non-HDL-C by dotinurad, in patients who had not used UA-lowering drugs. The meta-analysis showed that hyperuricemia increased the likelihood of dyslipidemia, and the pooled OR for the highest UA level vs. the lowest UA level was 1.84 (95%CI, 1.49 to 2.28) [
41]. A reduction in serum UA by dotinurad may improve serum lipids. We found an improvement in systolic blood pressure by dotinurad in patients who switched from XO inhibitors. The meta-analysis showed that hyperuricemia was associated with a higher risk of incident hypertension [
42]. Adjusted RR was 1.15 (95%CI, 1.06 to 1.26) for a 1 mg/dL increase in serum UA. Another meta-analysis showed that hyperuricemia was associated with an increased risk for incident hypertension (adjusted RR, 1.41; 95%CI, 1.23 to 1.58) [
43]. For a 1 mg/dL increase in UA level, the pooled RR for incident hypertension after adjusting for potential confounding was 1.13 (95%CI, 1.06 to 1.20). Hyperuricemia may be also responsible for microvascular damage through stimulation of the renin-angiotensin system (RAS), inhibition of endothelial nitric oxide, and proliferative effects on vascular smooth muscle cells [
44]. Did the reduction in serum UA by dotinurad improve systolic blood pressure in our patients who switched from XO inhibitors? The answer is “No”. Serum UA significantly increased in patients who switched from XO inhibitors. Why was systolic blood pressure reduced by dotinurad? We also observed a reduction in body weight by dotinurad in patients who switched from XO inhibitors. As one of the causes that SGLT2 inhibitors suppress the progression of CKD, lowering of serum UA by SGLT2 has been suggested [
9]. SGLT2 inhibitors increase the concentration of glucose in the proximal tubules, and glucose may compete with UA for apical GLUT9, reducing UA reabsorption [
28,
45] (
Figure 8A). Dotinurad selectively inhibits URAT1 and increases the concentration of UA in the proximal tubules, and UA may compete with glucose for apical GLUT9, reducing glucose reabsorption (
Figure 8B), which may induce an improvement of serum lipids, blood pressure, body weight, and UACR-like SGLT2 inhibitors [
9]. In present study, HbA1c significantly decreased in patients who had not taken SGLT2 inhibitors at 6 months after the start of dotinurad, supporting our hypothesis. SGL2 inhibitors improve body weight, dyslipidemia, blood pressure, and UACR [
9]. An improvement in body weight, dyslipidemia, blood pressure, and UACR after the start of dotinurad might have been induced by reduced glucose reabsorption by GLUT9.
We adjusted confounding variables, such as concurrent medications, for other lifestyle-related diseases except for hyperuricemia because such treatments have an effect on CKD outcome and metabolic parameters. Hyperuricemia was strongly associated with metabolic syndrome [
28] and metabolic syndrome, and each factor of metabolic syndrome induce the development and progression of CKD (
Figure 9A). CKD also induces the development and progression of hyperuricemia, dyslipidemia, impaired glucose metabolism, and hypertension [
28,
46].
Anti-hypertensive drugs, such as ARB and calcium channel blockers, have a favorable impact on blood pressure and renal parameters for CKD [
47,
48] (
Figure 9A). Therefore, we analyzed the effects of dotinurad on metabolic parameters by dividing into patients with and without anti-hypertensive drugs. UACR tended to decrease in patients with anti-hypertensive drugs, suggesting a synergetic effect of dotinurad and anti-hypertensive drugs on UACR. Systolic blood pressure tended to decrease in patients without anti-hypertensive drugs, suggesting that dotinurad reduced blood pressure by possibly a relative inhibition of GLUT9, which was supported by reduction in body weight and serum TG in this population. In this population, serum creatine significantly increased and eGFR significantly decreased after 3 months, which may be due to reduced glomerular hyperfiltration because they lost body weight.
Anti-hyperlipidemic drugs, such as statins, fibrates, and ezetimibe, have beneficial effects on dyslipidemia and CKD [
49,
50,
51,
52] (
Figure 9A). Diastolic blood pressure and UACR tended to decrease in patients with anti-hyperlipidemic drugs, suggesting a synergetic effect of dotinurad and anti-hypertensive drugs on blood pressure and UACR. Body weight tended to decrease and HbA1c significantly decreased in patients without anti-hyperlipidemic drugs, which may be also due to a relative inhibition of GLUT9.
SGLT2 inhibitors have beneficial effects on hyperuricemia, dyslipidemia, glucose metabolism, blood pressure, and CKD [
9] (
Figure 9A). Diastolic blood pressure tended to decrease in patients with SGLT2 inhibitors. Interestingly, HbA1c significantly decreased in patients without SGLT2 inhibitors, which may be also due to a relative inhibition of GLUT9.
Body weight, HbA1c tended to decrease and eGFR tended to increase in patients who had not taken anti-hypertensive and anti-hyperlipidemic drugs, and SGLT2 inhibitors, supporting a significance of a relative inhibition of GLUT-9 by dotinurad for an improvement of metabolic and renal parameters.
The summery of effects of dotinurad with and without concurrent medications for other lifestyle-related diseases except for hyperuricemia were shown in
Figure 9B. An improvement of UACR seems to be due to a synergetic effect of dotinurad and anti-hypertensive, and anti-hyperlipidemic drugs. An improvement of body weight, dyslipidemia, glucose metabolism, and eGFR may be induced by a relative inhibition of GLUT9 or other mechanism, such as an increase in urinary UA excretion by dotinurad. However, such suggestion may be still premature because CKD is multifactorial disease and multi-disciplinary treatments are required for suppression of CKD. Further studies, preferably with a great number of patients, should be performed in the future.
ABCG2 is a high-capacity UA exporter, the dysfunction of which raises hyperuricemia risk [
26] (
Figure 8). Dotinurad had no effect on ABCG2 [
22]. However, other UA-lowering drugs, such as benzbromarone (uricosuric agent) and febuxostat (XO inhibitor), have been reported to inhibit ABCG2 completely [
53]. Topiroxostat (XO inhibitor) also inhibited ABCG2 by over 80% [
53]. CKD patients accumulate uremic toxins in the body. ABCG2 was a major transporter of the uremic toxin, indoxyl sulfate (IS) [
54] (
Figure 8). ABCG2 regulates the pathophysiological excretion of IS and strongly affects CKD survival rates [
55]. High selectivity of dotinurad for URAT1 may be beneficial for suppression of progression of CKD.
Limitations of the study need to be addressed. This is a cross-sectional study, limiting inferences of causality and its direction. Although we did not change treatments for diabetes and hypertension, dyslipidemia intentionally during the study period, we cannot deny the beneficial role of the concomitant assumption of other drugs including aspect of synergism and/or the possible interaction between dotinurad and other treatments for metabolic parameters. We classified hyperuricemic patients into “UA overproduction type” and “UA underexcretion type” based on urinary UA/creatinine ≥ or <0.5, which may be weak. We should have measured 24 h urine UA, and should have analyzed urate transporter variants. To elucidate this in further studies, preferentially, RCT, that including a large number of patients, should be performed in the future.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}