
Autopsies Revealed Pathological Features of COVID-19 in Unvaccinated vs. Vaccinated Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Autopsy Procedures
2.3. SARS-CoV-2 RT-PCR
2.4. Histological Anlysis
2.5. Immunohistochemistry
2.6. Statistical Analyses
3. Results
3.1. Patients Demographics and Clinical Characteristics
3.2. Cause of Death
3.3. Postmortem SARS-CoV-2 PCR Analysis
3.4. Autopsy and Microscopic Examination
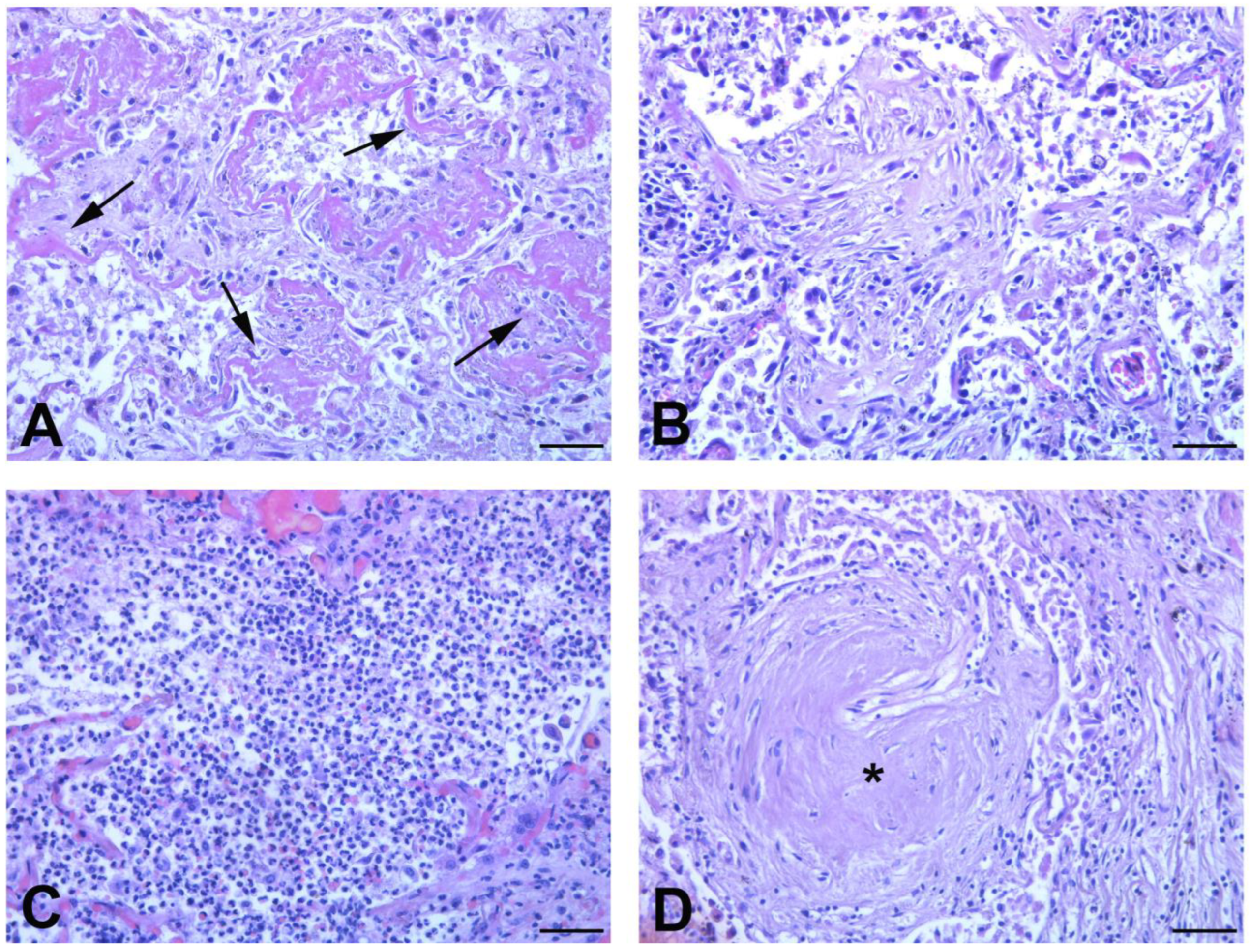
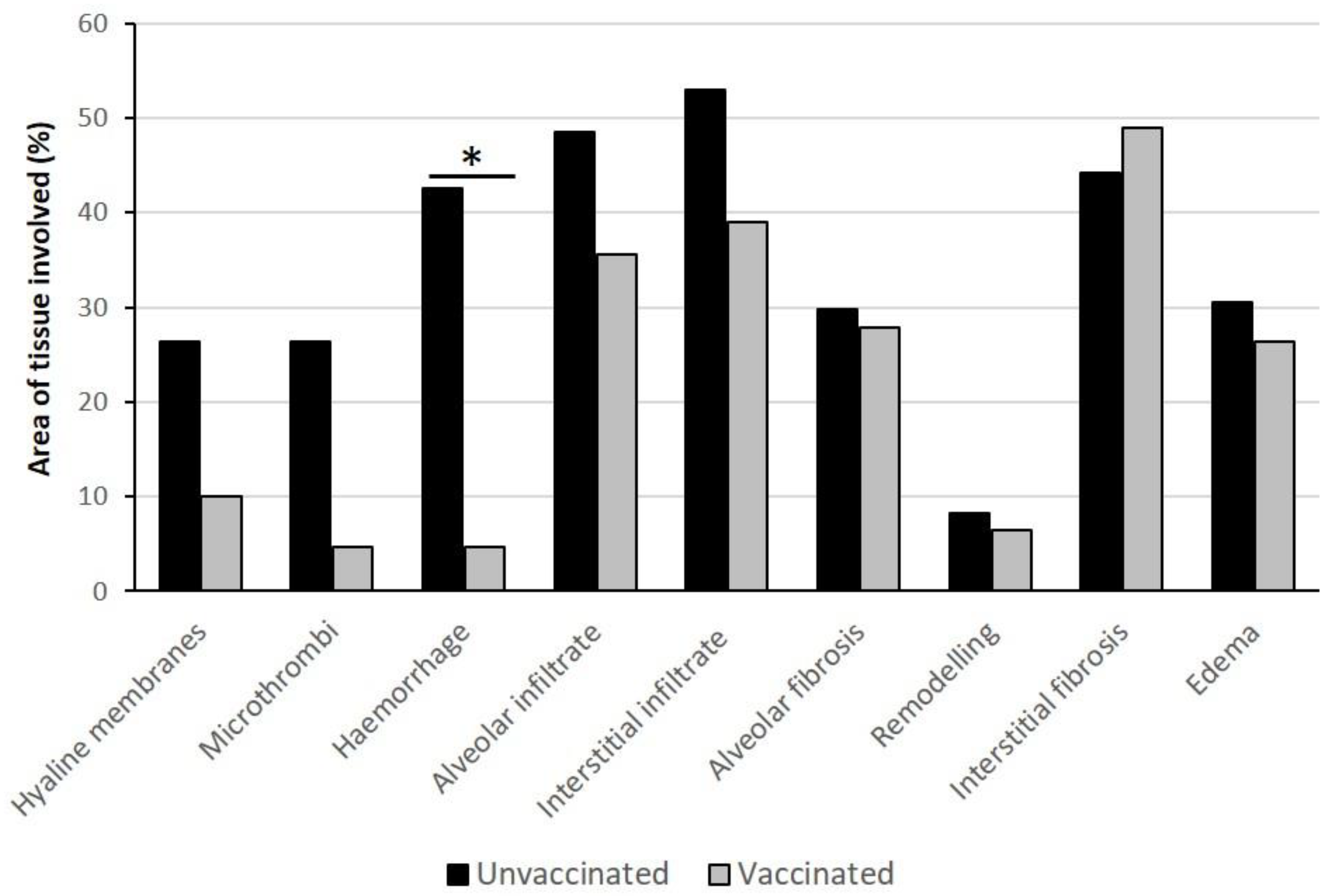
3.4.1. Lung Findings
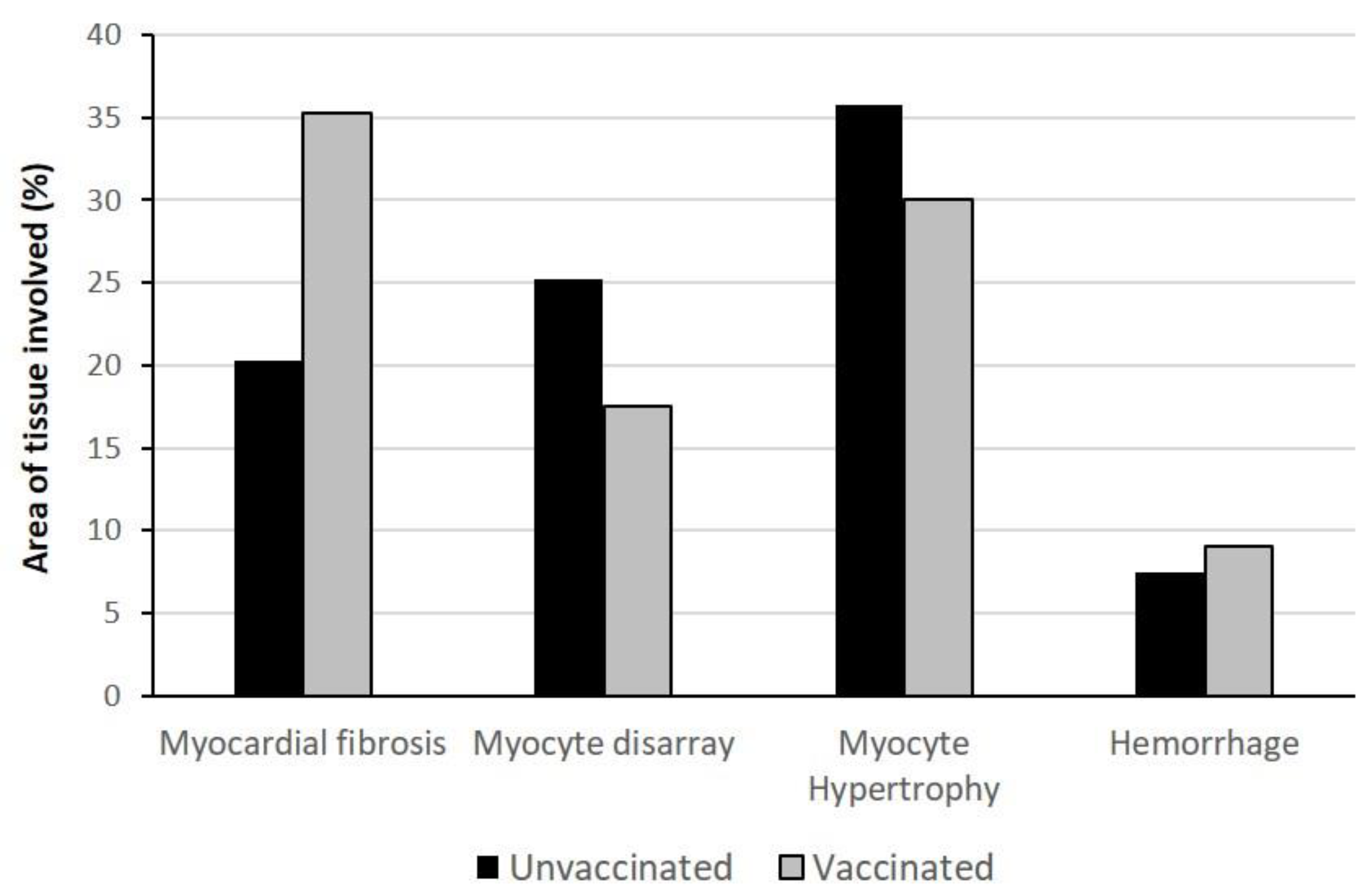
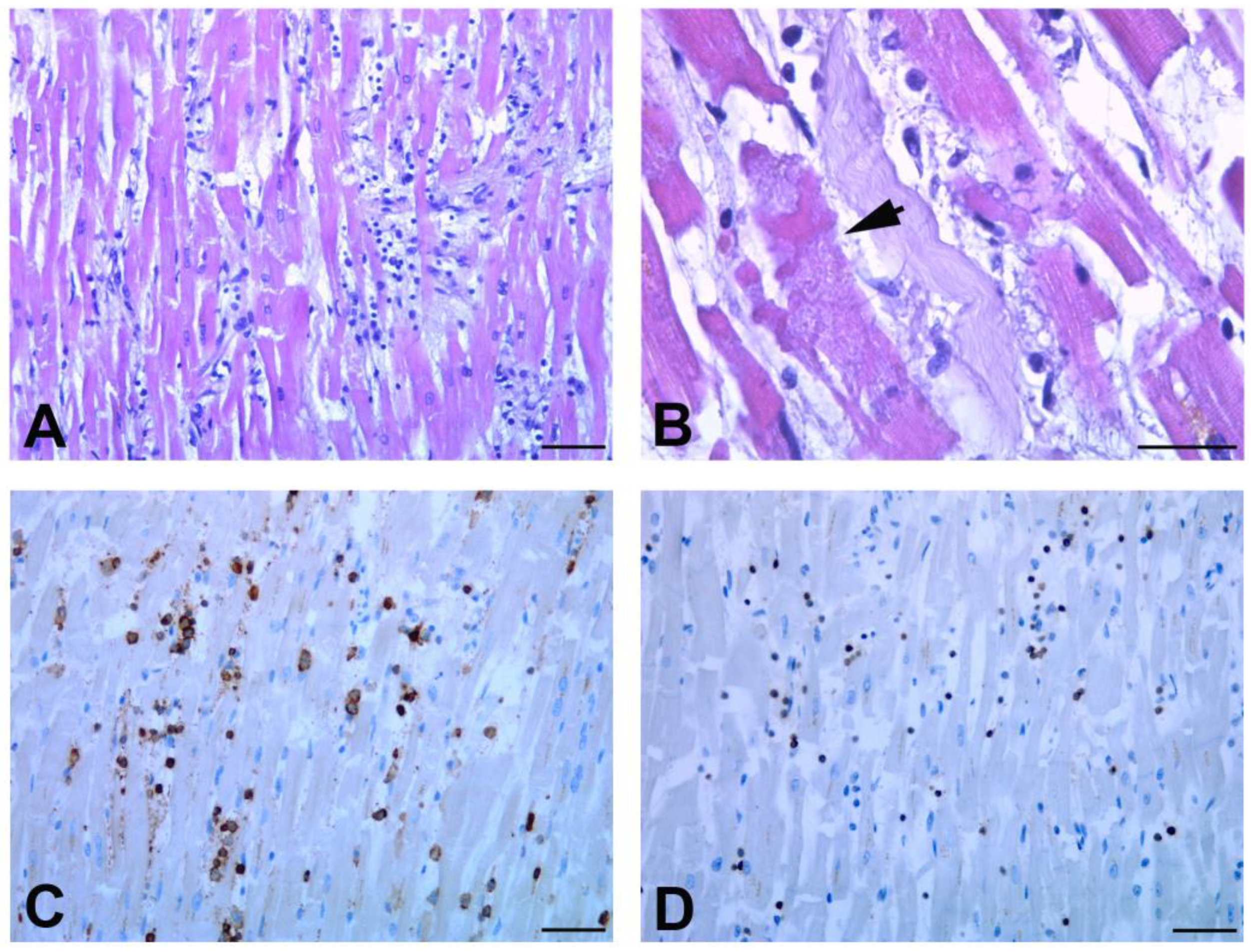
3.4.2. Heart Findings
3.4.3. Other Organs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Falasca, L.; Nardacci, R.; Colombo, D.; Lalle, E.; Di Caro, A.; Nicastri, E.; Antinori, A.; Petrosillo, N.; Marchioni, L.; Biava, G.; et al. Postmortem Findings in Italian Patients With COVID-19: A Descriptive Full Autopsy Study of Cases With and Without Comorbidities. J. Infect. Dis. 2020, 222, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.; Gomersall, C.D.; Fowler, R.A. Care for Critically Ill Patients With COVID-19. JAMA 2020, 323, 1499–1500. [Google Scholar] [CrossRef]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination With BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef] [PubMed]
- Pilishvili, T.; Gierke, R.; Fleming-Dutra, K.E.; Farrar, J.L.; Mohr, N.M.; Talan, D.A.; Krishnadasan, A.; Harland, K.K.; Smithline, H.A.; Hou, P.C.; et al. Vaccine Effectiveness among Healthcare Personnel Study Team Effectiveness of mRNA COVID-19 Vaccine among, U.S. Health Care Personnel. N. Engl. J. Med. 2021, 385, e90. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.L.; Lutrick, K.; et al. Prevention and Attenuation of COVID-19 with the BNT162b2 and mRNA-1273 Vaccines. N. Engl. J. Med. 2021, 385, 320–329. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Chung, H.; He, S.; Nasreen, S.; Sundaram, M.E.; Buchan, S.A.; Wilson, S.E.; Chen, B.; Calzavara, A.; Fell, D.B.; Austin, P.C.; et al. Canadian Immunization Research Network (CIRN) Provincial Collaborative Network (PCN) Investigators. Effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe COVID-19 outcomes in Ontario, Canada: Test negative design study. BMJ 2021, 374, n1943. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef] [PubMed]
- EMA Recommends First COVID-19 Vaccine for Authorisation in the EU. Available online: https://www.ema.europa.eu/en/news/ema-recommends-first-COVID-19-vaccine-authorisation-eu (accessed on 21 December 2020).
- Istituto Superiore di Sanità. Epidemia COVID-19: Sorveglianza, Impatto Delle Infezioni Ed Efficacia Vaccinale. Aggiornamento nazionale 23 Febbraio 2022. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_23-febbraio-2022.pdf (accessed on 23 February 2022).
- World Health Organization (WHO). International Guidelines for Certification and Classification (coding) of COVID-19 as Cause of Death. Available online: https://www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf?ua=1 (accessed on 20 April 2020).
- Whimster, W.F.; Macfarlane, A.J. Normal lung weights in a white population. Am. Rev. Respir. Dis. 1974, 110, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, T.; Eriksson, A.; Wingren, C.J. Multivariate linear regression modelling of lung weight in 24,056 Swedish medico-legal autopsy cases. J. Forensic. Leg. Med. 2017, 46, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Molina, D.K.; DiMaio, V.J. Normal organ weights in men: Part II-the brain, lungs, liver, spleen, and kidneys. Am. J. Forensic. Med. Pathol. 2012, 33, 368–372. [Google Scholar] [CrossRef]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart. J. 2013, 33, 2648a–2648d. [Google Scholar] [CrossRef]
- Okabe, M.; Fukuda, K.; Arakawa, K.; Kikuchi, M. Chronic variant of myocarditis associated with hepatitis C virus infection. Circulation 1997, 96, 22–24. [Google Scholar] [CrossRef]
- Klindt, C.; Jensen, B.E.; Brandenburger, T.; Feldt, T.; Killer, A.; Schimmöller, L.; Antoch, G.; Senff, T.; Hauka, S.; Timm, J.; et al. Secondary sclerosing cholangitis as a complication of severe COVID-19: A case report and review of the literature. Clin. Case Rep. 2021, 9, e04068. [Google Scholar] [CrossRef]
- Colombo, D.; Falasca, L.; Marchioni, L.; Tammaro, A.; Adebanjo, G.A.R.; Ippolito, G.; Zumla, A.; Piacentini, M.; Nardacci, R.; Del Nonno, F. Neuropathology and Inflammatory Cell Characterization in 10 Autoptic COVID-19 Brains. Cells 2021, 10, 2262. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. COVID-19 ISS Open Data—EpiCentro. Available online: https://www.epicentro.iss.it/coronavirus/open-data/covid_19-iss.xlsx (accessed on 31 October 2021).
- Satturwar, S.; Fowkes, M.; Farver, C.; Wilson, A.M.; Eccher, A.; Girolami, I.; Pujadas, E.; Bryce, C.; Salem, F.; El Jamal, S.M.; et al. Postmortem Findings Associated With SARS-CoV-2: Systematic Review and Meta-analysis. Am. J. Surg. Pathol. 2021, 45, 587–603. [Google Scholar] [CrossRef]
- Fauvel, C.; Trimaille, A.; Weizman, O.; Pezel, T.; Mika, D.; Waldmann, V.; Cohen, A.; Bonnet, G. Cardiovascular manifestations secondary to COVID-19: A narrative review. Respir. Med. Res. 2022, 81, 100904. [Google Scholar] [CrossRef]
- Basso, C.; Leone, O.; Rizzo, S.; De Gaspari, M.; van der Wal, A.C.; Aubry, M.C.; Bois, M.C.; Lin, P.T.; Maleszewski, J.J.; Stone, J.R. Pathological features of COVID-19-associated myocardial injury: A multicentre cardiovascular pathology study. Eur. Heart J. 2020, 41, 3827–3835. [Google Scholar] [CrossRef] [PubMed]
- Bearse, M.; Hung, Y.P.; Krauson, A.J.; Bonanno, L.; Boyraz, B.; Harris, C.K.; Helland, T.L.; Hilburn, C.F.; Hutchison, B.; Jobbagy, S.; et al. Factors associated with myocardial SARS-CoV-2 infection, myocarditis, and cardiac inflammation in patients with COVID-19. Mod. Pathol. 2021, 34, 1345–1357. [Google Scholar] [CrossRef] [PubMed]
- Werlein, C.; Ackermann, M.; Stark, H.; Shah, H.R.; Tzankov, A.; Haslbauer, J.D.; von Stillfried, S.; Bülow, R.D.; El-Armouche, A.; Kuenzel, S.; et al. Inflammation and vascular remodeling in COVID-19 hearts. Angiogenesis 2022, 12, 1–16. [Google Scholar] [CrossRef]
- Pawelec, G. Age and immunity: What is “immunosenescence”? Exp. Gerontol. 2018, 105, 4–9. [Google Scholar] [CrossRef]
- Reali, E.; Ferrando-Martinez, S.; Catalfamo, M. Editorial: The Interplay Between Immune Activation and Cardiovascular Disease During Infection, Autoimmunity and Aging: The Role of T Cells. Front. Immunol. 2021, 12, 719517. [Google Scholar] [CrossRef]
- Barcena, M.L.; Aslam, M.; Pozdniakova, S.; Norman, K.; Ladilov, Y. Cardiovascular Inflam-maging: Mechanisms and Translational Aspects. Cells 2022, 11, 1010. [Google Scholar] [CrossRef]
- Fraser, M.; Agdamag, A.C.C.; Maharaj, V.R.; Mutschler, M.; Charpentier, V.; Chowdhury, M.; Alexy, T. COVID-19-Associated Myocarditis: An Evolving Concern in Cardiology and Beyond. Biology 2022, 11, 520. [Google Scholar] [CrossRef]
- Trimaille, A.; Ribeyrolles, S.; Fauvel, C.; Chaumont, C.; Weizman, O.; Pommier, T.; Cellier, J.; Geneste, L.; Panagides, V.; Marsou, W.; et al. The Critical COVID-France Investigators. Cardiovascular Characteristics and Outcomes of Young Patients with COVID-19. J. Cardiovasc. Dev. Dis. 2021, 8, 165. [Google Scholar] [CrossRef]
- Wang, X.M.; Mannan, R.; Xiao, L.; Abdulfatah, E.; Qiao, Y.; Farver, C.; Myers, J.L.; Zelenka-Wang, S.; McMurry, L.; Su, F.; et al. Characterization of SARS-CoV-2 and host entry factors distribution in a COVID-19 autopsy series. Commun. Med. 2021, 1, 24. [Google Scholar] [CrossRef]
- Stein, S.R.; Ramelli, S.C.; Grazioli, A.; Chung, J.Y.; Singh, M.; Yinda, C.K.; Winkler, C.W.; Sun, J.; Dickey, J.M.; Ylaya, K.; et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 2022, 612, 758–763. [Google Scholar] [CrossRef]
- Wong, D.W.L.; Klinkhammer, B.M.; Djudjaj, S.; Villwock, S.; Timm, M.C.; Buhl, E.M.; Wucherpfennig, S.; Cacchi, C.; Braunschweig, T.; Knüchel-Clarke, R.; et al. Multisystemic Cellular Tropism of SARS-CoV-2 in Autopsies of COVID-19 Patients. Cells 2021, 10, 1900. [Google Scholar] [CrossRef] [PubMed]
- Van Cleemput, J.; van Snippenberg, W.; Lambrechts, L.; Dendooven, A.; D’Onofrio, V.; Couck, L.; Trypsteen, W.; Vanrusselt, J.; Theuns, S.; Vereecke, N.; et al. Author Correction: Organ-specific genome diversity of replication-competent SARS-CoV-2. Nat. Commun. 2022, 13, 6247. [Google Scholar] [CrossRef] [PubMed]
- Hopfer, H.; Herzig, M.C.; Gosert, R.; Menter, T.; Hench, J.; Tzankov, A.; Hirsch, H.H.; Miller, S.E. Hunting coronavirus by transmission electron microscopy—A guide to SARS-CoV-2-associated ultrastructural pathology in COVID-19 tissues. Histopathology 2021, 78, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Del Nonno, F.; Nardacci, R.; Colombo, D.; Visco-Comandini, U.; Cicalini, S.; Antinori, A.; Marchioni, L.; D’Offizi, G.; Piacentini, M.; Falasca, L. Hepatic Failure in COVID-19: Is Iron Overload the Dangerous Trigger? Cells 2021, 10, 1103. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet. Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]
- Middleton, E.A.; Zimmerman, G.A. COVID-19-Associated Acute Respiratory Distress Syndrome: Lessons from Tissues and Cells. Crit. Care Clin. 2021, 37, 777. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° | Age/ Sex | Time since Second Vaccine Dose | Comorbidities | Symptoms Before Hospital Stay | SARS-CoV2 positivity Before Hospitalization | Hospital Stay (Days) | Pulmonary Imaging | Oxygen/Intensive Care | Certified Cause of Death |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 78 F | 195 days (6.5 months) | Patient bedridden for 10 years for Parkinson; implant for deep brain stimulation (DBS) | Fever and pneumonia | Not known | Deceased at the ER | / | / | Acute respiratory distress syndrome due to COVID-19 |
| 2 | 81 M | 270 days (9 months) | Chronic ischemic cardiomyopathy; Hospitalized for malignancy | Pneumonia during hospitalization in the oncological unit | Negative * | 11 1 | CT: bilateral multifocal ground-glass opacities | Oxygen therapy | Myocardial infarction, respiratory failure due to bacterial bronchopneumonia and abdominal fibromatosis |
| 3 | 60 F | 188 days (6.5 months) | Hypertension; Paroxysmal AFib; Hypotiroidism; rheumatoid arthritis; incarcerated umbilical hernia; active cancer in the past 5 years | Syncopal episode | 11 days | Deceased at the ER | CT: bilateral basal ground-glass opacities | Orotracheal intubation | Heart failure due to auricle thrombosis and small bowel ischemia |
| 4 | 66 M | 250 days (8.5 months) | ALD, hepatic cirrhosis, multiple cysts splenomegaly; multi-infarct leukoencephalopathy | / | Negative * | 15 | CT: Superior right lobe areas of ground-glass opacities | Refused | Respiratory failure due to bacterial pneumonia, cirrhotic cardiomyopathy and encephalopathy |
| 5 | 75 M | 298 days (10 months) | COPD; epilepsy; rheumatoid arthritis; cerebral vasculopathy; diabetes | 3 days fever | 3 days | 23 | CT: bilateral multifocal crazy paving | Refused | Rheumatoid arthritis related organizing pneumonia |
| N° | Age/Sex | Comorbidities | Symptoms Before Hospital Stay | SARS-CoV2 Positivity Before Hospitalization | Hospital Stay (Days) | Pulmonary Imaging | Oxygen/Intensive Care | Certified Cause of Death |
|---|---|---|---|---|---|---|---|---|
| 1 | 67 F | Emphysema | 4 days general malaise; hypotension with syncopal episodes | Not known | Deceased at the emergency room | CT: bilateral and diffuse crazy paving pattern | / | Myocarditis and acute respiratory distress syndrome due to COVID-19 |
| 2 | 53 F | / | 4 days progressive dyspnea | 15 days | Deceased at the emergency room | / | / | Myocarditis, acute respiratory distress syndrome, and haemorrhagic infarction due to COVID-19 |
| 3 | 51 M | ALD; atherosclerosis | dyspnea | Not known | 9 | RX: bilateral consolidations involving the majority of both lungs | Oxygen therapy with NIV; orotracheal intubation; | G.I. haemorrhage and lobar pneumonia |
| 4 | 49 M | Obesity (BMI ≥ 30) | 3 days progressive dyspnea | Not known | 18 | CT: bilateral and diffuse crazy paving pattern | Oxygen therapy with VMK 50%; NIV; orotracheal intubation; | Acute respiratory distress syndrome due to COVID-19 |
| 5 | 45 F | Obesity (BMI ≥ 30) | Fever; nausea | 9 days | 4 | CT: bilateral and multifocal ground-glass opacities | Orotracheal intubation | Acute respiratory distress syndrome due to COVID-19 |
| Unvaccinated Patients | Vaccinated Patients | ||
|---|---|---|---|
| Sample | p Value | ||
| Bronchi (median/range) | 23.37 (17.78–34.42) | 31.24 (26.35–34.49) | 0.1019 |
| Lungs (median/range) | 21.49 (14.51–32.59) | 30.54 (18.10–37.69) | 0.0016 * |
| Myocardium (median/range) | 33.93 (26.03–39.63) | 31.21 (27.12–35.30) | 0.6821 |
| N° | Sex | Weight (g) | Edema | Congestion | Right Lung Consolidation | Left Lung Consolidation | Bacterial Bronchopneumonia/ Pneumonia | Fibrosis | PA | PE | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Upper Lobe | Medium Lobe | Lower Lobe | Upper Lobe | Lower Lobe | |||||||||
| UNVACCINATED PATIENTS | |||||||||||||
| 1 | F | Right 576 Left 385 Total 961 | + | + | / | Diffuse | Diffuse | Diffuse | Focal | / | Bilateral, subpleural | / | / |
| 2 | F | Right 1200 * Left 638 Total 1838 * | + | / | Diffuse | Diffuse | Diffuse | Diffuse | Diffuse | / | Bilateral | + | / |
| 3 | M | Right 1027 * Left 1112 * Total 2139 * | + | + | Diffuse | Diffuse | Diffuse | Diffuse | Diffuse | Bilateral | Supleural | / | |
| 4 | M | Right 939 * Left 854 * Total 1793 * | / | + | Diffuse | Diffuse | Diffuse | Diffuse | Diffuse | / | Bilateral | / | / |
| 5 | F | Right 882 * Left 720 * Total 1602 * | + | + | Diffuse | Diffuse | Diffuse | Diffuse | Diffuse | / | Bilateral | / | / |
| VACCINATED PATIENTS | |||||||||||||
| 1 | F | Right 563 Left 583 Total 1146 | + | / | Diffuse | Diffuse | Diffuse | Diffuse | Diffuse | / | Bilateral | / | / |
| 2 | M | Right 702 Left 662 Total 1364 * | / | + | / | / | Focal | / | Diffuse | Lower lobes | Lower lobes | / | + |
| 3 | F | Right 510 Left 519 Total 1029 | + | + | Focal | Focal | Diffuse | / | Diffuse | Right lung | Lower left lung | / | / |
| 4 | M | Right 1080 * Left 662 Total 1742 * | + | + | Diffuse | Diffuse | Diffuse | / | / | Right lung | Focal | / | / |
| 5 | M | Right 620 Left 491 Total 1111 | / | + | Focal | / | Diffuse | Diffuse | Focal | Lower left lobe | Bilateral focal | / | / |
| N° | Sex | Weight (g) | Cardiac Hypertrophy | Dilatation of the Chambers | LV Wall Thickness (mm) | RV Wall Thickness (mm) | Consistency | Septum Thickness (mm) | Obstructive Modifications |
|---|---|---|---|---|---|---|---|---|---|
| UNVACCINATED PATIENTS | |||||||||
| 1 | F | 436 | / | / | 13 | 3 | Flabby | 10 | Mild aortic atherosclerosis |
| 2 | F | 470 | Concentric hypertrophy | / | 18 | 4 | Firm | 25 | Moderate aortic atherosclerosis |
| 3 | M | 424 | Eccentric hypertrophy | LV dilatation | 12 | 3 | Flabby | 11 | Mild aortic atherosclerosis |
| 4 | M | 797 | Concentric hypertrophy | / | 12 | 3 | Firm | 14 | Mild aortic atherosclerosis |
| 5 | F | 396 | Eccentric hypertrophy | Biventricular dilatation | 12 | 3 | Flabby | 12 | / |
| VACCINATED PATIENTS | |||||||||
| 1 | F | 450 | Eccentric hypertrophy | Biventricular dilatation | 12 | 4 | Flabby | 12 | Moderate aortic atherosclerosis; coronary stenosis above 50% |
| 2 | M | 355 | Eccentric hypertrophy | Biventricular dilatation | 10 | 3 | Flabby | 15 | Aortic and mitral valve stenosis; moderate aortic atherosclerosis |
| 3 | F | 427 | / | Biventricular dilatation | 8 | 3 | Flabby | 10 | Mild aortic atherosclerosis |
| 4 | M | 470 | Concentric hypertrophy | / | 18 | 5 | Firm | 20 | Moderate aortic atherosclerosis; coronary stenosis of one |
| 5 | M | 332 | / | Biventricular dilatation | 12 | 4 | Flabby | 12 | Mild aortic atherosclerosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo, D.; Del Nonno, F.; Marchioni, L.; Lalle, E.; Gallì, P.; Vaia, F.; Falasca, L. Autopsies Revealed Pathological Features of COVID-19 in Unvaccinated vs. Vaccinated Patients. Biomedicines 2023, 11, 551. https://doi.org/10.3390/biomedicines11020551
Colombo D, Del Nonno F, Marchioni L, Lalle E, Gallì P, Vaia F, Falasca L. Autopsies Revealed Pathological Features of COVID-19 in Unvaccinated vs. Vaccinated Patients. Biomedicines. 2023; 11(2):551. https://doi.org/10.3390/biomedicines11020551
Chicago/Turabian StyleColombo, Daniele, Franca Del Nonno, Luisa Marchioni, Eleonora Lalle, Paola Gallì, Francesco Vaia, and Laura Falasca. 2023. "Autopsies Revealed Pathological Features of COVID-19 in Unvaccinated vs. Vaccinated Patients" Biomedicines 11, no. 2: 551. https://doi.org/10.3390/biomedicines11020551