
The von Willebrand Factor Antigen Reflects the Juvenile Dermatomyositis Disease Activity Score
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
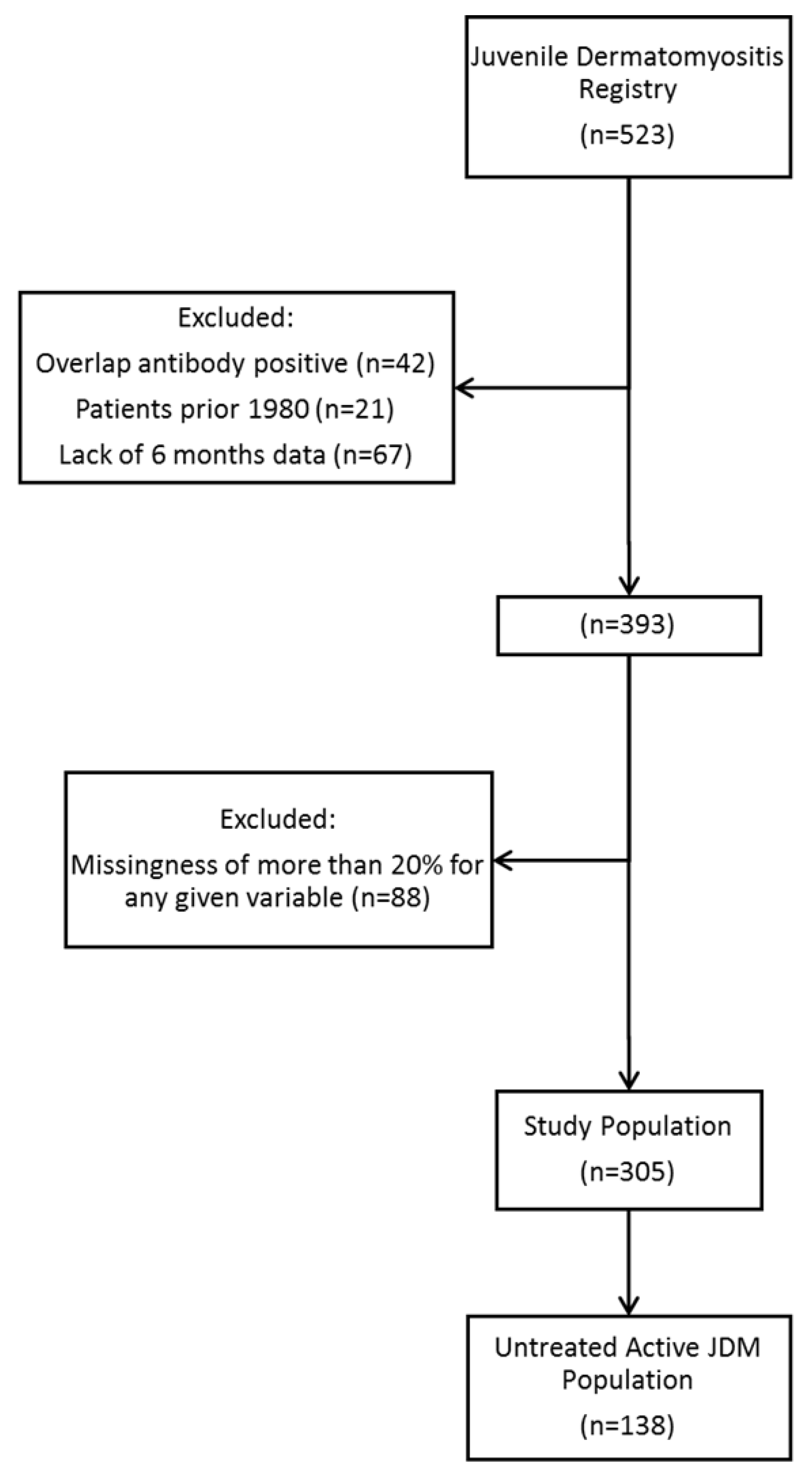
2.1. Study Design, Approval, and Population
2.2. Study Variables
2.3. Statistical Analysis
3. Results
3.1. Patient Background and Demographic Analysis
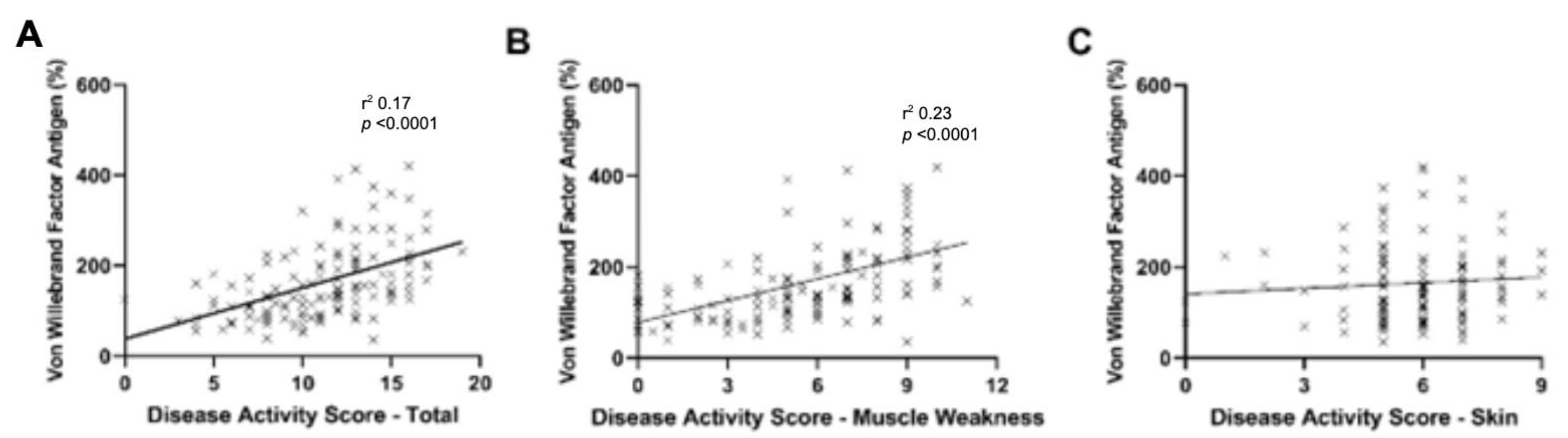
3.2. vWF:Ag Effect on DAS
3.3. Subcomponents Associated with vWF:Ag
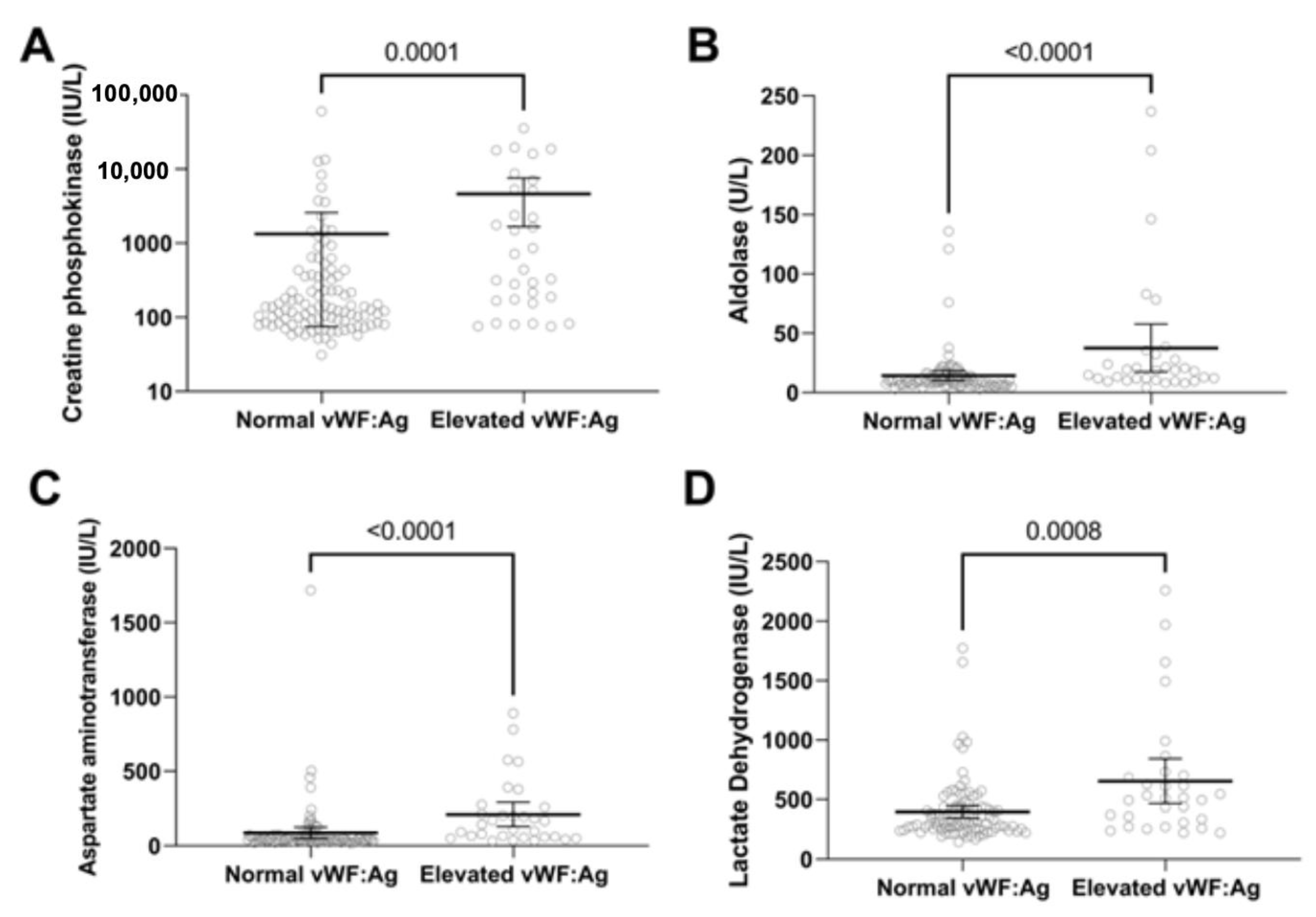
3.4. Untreated JDM with Active Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mendez, E.P.; Lipton, R.; Ramsey-Goldman, R.; Roettcher, P.; Bowyer, S.; Dyer, A.; Pachman, L.M.; NIAMS Juvenile DM Registry Physician Referral Group. US incidence of juvenile dermatomyositis, 1995-1998: Results from the National Institute of Arthritis and Musculoskeletal and Skin Diseases Registry. Arthritis Rheum 2003, 49, 300–305. [Google Scholar] [CrossRef]
- Tezak, Z.; Hoffman, E.P.; Lutz, J.L.; Fedczyna, T.O.; Stephan, D.; Bremer, E.G.; Krasnoselska-Riz, I.; Kumar, A.; Pachman, L.M. Gene expression profiling in DQA1*0501+ children with untreated dermatomyositis: A novel model of pathogenesis. J. Immunol. 2002, 168, 4154–4163. [Google Scholar] [CrossRef] [PubMed]
- Pachman, L.M.; Khojah, A.M. Advances in Juvenile Dermatomyositis: Myositis Specific Antibodies Aid in Understanding Disease Heterogeneity. J. Pediatr. 2018, 195, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Xia, Q.; Pan, M.; Zhao, X.; Li, X.; Shi, R.; Zhou, M.; Ding, X.; Kuwana, M.; Zheng, J. Gottron Papules and Gottron Sign with Ulceration: A Distinctive Cutaneous Feature in a Subset of Patients with Classic Dermatomyositis and Clinically Amyopathic Dermatomyositis. J. Rheumatol. 2016, 43, 1735–1742. [Google Scholar] [CrossRef]
- Tansley, S.L.; Simou, S.; Shaddick, G.; Betteridge, Z.E.; Almeida, B.; Gunawardena, H.; Thomson, W.; Beresford, M.W.; Midgley, A.; Muntoni, F.; et al. Autoantibodies in juvenile-onset myositis: Their diagnostic value and associated clinical phenotype in a large UK cohort. J. Autoimmun 2017, 84, 55–64. [Google Scholar] [CrossRef]
- Li, D.; Tansley, S.L. Juvenile Dermatomyositis-Clinical Phenotypes. Curr. Rheumatol. Rep. 2019, 21, 74. [Google Scholar] [CrossRef]
- Boyarchuk, O.; Kuka, A.; Yuryk, I. Clinical and autoantibody phenotypes of juvenile dermatomyositis. Reumatologia 2022, 60, 281–291. [Google Scholar] [CrossRef]
- Poddighe, D.; Dauyey, K. Macrophage activation syndrome in juvenile dermatomyositis: A systematic review. Rheumatol. Int. 2020, 40, 695–702. [Google Scholar] [CrossRef]
- Miyamae, T.; Ishiguro, N.; Yonezawa, M.; Tokushige, K.; Yamanaka, H. Pneumatosis Intestinalis Associated with Juvenile Dermatomyositis. Case Rep. Rheumatol. 2016, 2016, 6497357. [Google Scholar] [CrossRef] [Green Version]
- Briones, M.R.; Morgan, G.A.; Amoruso, M.C.; Rahmani, B.; Ryan, M.E.; Pachman, L.M. Decreased CD3-CD16+CD56+ natural killer cell counts in children with orbital myositis: A clue to disease activity. RMD Open 2017, 3, e000385. [Google Scholar] [CrossRef]
- Bode, R.K.; Klein-Gitelman, M.S.; Miller, M.L.; Lechman, T.S.; Pachman, L.M. Disease activity score for children with juvenile dermatomyositis: Reliability and validity evidence. Arthritis Rheum 2003, 49, 7–15. [Google Scholar] [CrossRef]
- Rider, L.G.; Werth, V.P.; Huber, A.M.; Alexanderson, H.; Rao, A.P.; Ruperto, N.; Herbelin, L.; Barohn, R.; Isenberg, D.; Miller, F.W. Measures of adult and juvenile dermatomyositis, polymyositis, and inclusion body myositis: Physician and Patient/Parent Global Activity, Manual Muscle Testing (MMT), Health Assessment Questionnaire (HAQ)/Childhood Health Assessment Questionnaire (C-HAQ), Childhood Myositis Assessment Scale (CMAS), Myositis Disease Activity Assessment Tool (MDAAT), Disease Activity Score (DAS), Short Form 36 (SF-36), Child Health Questionnaire (CHQ), physician global damage, Myositis Damage Index (MDI), Quantitative Muscle Testing (QMT), Myositis Functional Index-2 (FI-2), Myositis Activities Profile (MAP), Inclusion Body Myositis Functional Rating Scale (IBMFRS), Cutaneous Dermatomyositis Disease Area and Severity Index (CDASI), Cutaneous Assessment Tool (CAT), Dermatomyositis Skin Severity Index (DSSI), Skindex, and Dermatology Life Quality Index (DLQI). Arthritis Care Res. 2011, 63 (Suppl. S11), S118–S157. [Google Scholar] [CrossRef]
- Leclair, V.; Lundberg, I.E. New Myositis Classification Criteria-What We Have Learned Since Bohan and Peter. Curr. Rheumatol. Rep. 2018, 20, 18. [Google Scholar] [CrossRef]
- Lundberg, I.E.; Tjarnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2018, 77, e91. [Google Scholar] [CrossRef]
- Huber, A.M.; Feldman, B.M.; Rennebohm, R.M.; Hicks, J.E.; Lindsley, C.B.; Perez, M.D.; Zemel, L.S.; Wallace, C.A.; Ballinger, S.H.; Passo, M.H.; et al. Validation and clinical significance of the Childhood Myositis Assessment Scale for assessment of muscle function in the juvenile idiopathic inflammatory myopathies. Arthritis Rheum 2004, 50, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Chipman, J.; Evereklian, M.; Nghiem, K.; Stetler-Stevenson, M.; Rick, M.E.; Centola, M.; Miller, F.W.; Rider, L.G. Endothelial Activation Markers as Disease Activity and Damage Measures in Juvenile Dermatomyositis. J. Rheumatol. 2020, 47, 1011–1018. [Google Scholar] [CrossRef]
- Guzman, J.; Petty, R.E.; Malleson, P.N. Monitoring disease activity in juvenile dermatomyositis: The role of von Willebrand factor and muscle enzymes. J. Rheumatol. 1994, 21, 739–743. [Google Scholar]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (second of two parts). N. Engl. J. Med. 1975, 292, 403–407. [Google Scholar] [CrossRef]
- Ziegler, A.; Vens, M. Generalized estimating equations. Notes on the choice of the working correlation matrix. Methods Inf. Med. 2010, 49, 421–425, discussion 426–432. [Google Scholar] [CrossRef]
- Hardin, J.W.; Joseph, M. Generalized Estimating Equations; Chapman and Hall/CRC: Boca Raton, FL, USA, 2002. [Google Scholar]
- Garratty, G.; Glynn, S.A.; McEntire, R.; Retrovirus Epidemiology Donor, S. ABO and Rh(D) phenotype frequencies of different racial/ethnic groups in the United States. Transfusion 2004, 44, 703–706. [Google Scholar] [CrossRef]
- Khojah, A.; Morgan, G.; Pachman, L.M. Clues to Disease Activity in Juvenile Dermatomyositis: Neopterin and Other Biomarkers. Diagnostics 2021, 12, 8. [Google Scholar] [CrossRef]
- Xu, D.; Huang, C.C.; Kachaochana, A.; Morgan, G.A.; Bonaldo, M.F.; Soares, M.B.; Costa, F.; Sarwark, J.; Sredni, S.T.; Pachman, L.M. MicroRNA-10a Regulation of Proinflammatory Mediators: An Important Component of Untreated Juvenile Dermatomyositis. J. Rheumatol. 2016, 43, 161–168. [Google Scholar] [CrossRef]
- Roberson, E.D.O.; Mesa, R.A.; Morgan, G.A.; Cao, L.; Marin, W.; Pachman, L.M. Transcriptomes of peripheral blood mononuclear cells from juvenile dermatomyositis patients show elevated inflammation even when clinically inactive. Sci. Rep. 2022, 12, 275. [Google Scholar] [CrossRef] [PubMed]
- Salmela, A.; Ekstrand, A.; Joutsi-Korhonen, L.; Raisanen-Sokolowski, A.; Lassila, R. Activation of endothelium, coagulation and fibrinolysis is enhanced and associates with renal anti-neutrophil cytoplasmic antibody-associated vasculitis. Nephrol. Dial. Transplant. 2015, 30 (Suppl. S1), i53–i59. [Google Scholar] [CrossRef]
- Cellucci, T.; Tyrrell, P.N.; Pullenayegum, E.; Benseler, S.M. von Willebrand factor antigen--a possible biomarker of disease activity in childhood central nervous system vasculitis? Rheumatology 2012, 51, 1838–1845. [Google Scholar] [CrossRef]
- Brogan, P.; Eleftheriou, D. Vasculitis update: Pathogenesis and biomarkers. Pediatr. Nephrol. 2018, 33, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chung, D.W. Inflammation, von Willebrand factor, and ADAMTS13. Blood 2018, 132, 141–147. [Google Scholar] [CrossRef]
- Rostami, M.; Mansouritorghabeh, H.; Parsa-Kondelaji, M. High levels of Von Willebrand factor markers in COVID-19: A systematic review and meta-analysis. Clin. Exp. Med. 2022, 22, 347–357. [Google Scholar] [CrossRef]
- Ferlitsch, M.; Reiberger, T.; Hoke, M.; Salzl, P.; Schwengerer, B.; Ulbrich, G.; Payer, B.A.; Trauner, M.; Peck-Radosavljevic, M.; Ferlitsch, A. von Willebrand factor as new noninvasive predictor of portal hypertension, decompensation and mortality in patients with liver cirrhosis. Hepatology 2012, 56, 1439–1447. [Google Scholar] [CrossRef]
- Takaya, H.; Kawaratani, H.; Tsuji, Y.; Nakanishi, K.; Saikawa, S.; Sato, S.; Sawada, Y.; Kaji, K.; Okura, Y.; Shimozato, N.; et al. von Willebrand factor is a useful biomarker for liver fibrosis and prediction of hepatocellular carcinoma development in patients with hepatitis B and C. United Eur. Gastroenterol. J. 2018, 6, 1401–1409. [Google Scholar] [CrossRef] [Green Version]
- von Vischer, U.M. Willebrand factor, endothelial dysfunction, and cardiovascular disease. J. Thromb. Haemost. 2006, 4, 1186–1193. [Google Scholar] [CrossRef] [PubMed]
- Gragnano, F.; Sperlongano, S.; Golia, E.; Natale, F.; Bianchi, R.; Crisci, M.; Fimiani, F.; Pariggiano, I.; Diana, V.; Carbone, A.; et al. The Role of von Willebrand Factor in Vascular Inflammation: From Pathogenesis to Targeted Therapy. Mediators Inflamm. 2017, 2017, 5620314. [Google Scholar] [CrossRef]
- Khojah, A.; Liu, V.; Savani, S.I.; Morgan, G.; Shore, R.; Bellm, J.; Pachman, L.M. Association of p155/140 Autoantibody With Loss of Nailfold Capillaries but not Generalized Lipodystrophy: A Study of Ninety-Six Children With Juvenile Dermatomyositis. Arthritis Care Res. 2022, 74, 1065–1069. [Google Scholar] [CrossRef]
- Gill, J.C.; Endres-Brooks, J.; Bauer, P.J.; Marks, W.J., Jr.; Montgomery, R.R. The effect of ABO blood group on the diagnosis of von Willebrand disease. Blood 1987, 69, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Pachman, L.M.; Nolan, B.E.; DeRanieri, D.; Khojah, A.M. Juvenile Dermatomyositis: New Clues to Diagnosis and Therapy. Curr. Treatm. Opt. Rheumatol. 2021, 7, 39–62. [Google Scholar] [CrossRef]
- Pachman, L.M.; Abbott, K.; Sinacore, J.M.; Amoruso, L.; Dyer, A.; Lipton, R.; Ilowite, N.; Hom, C.; Cawkwell, G.; White, A.; et al. Duration of illness is an important variable for untreated children with juvenile dermatomyositis. J. Pediatr. 2006, 148, 247–253. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total JDM Population n = 305 | Untreated JDM n = 138 | |
|---|---|---|
| Demographics | ||
| Age at enrollment (yr), median (IQR) | 7.1 (4.4–10.3) | 6.1 (4.0–9.4) |
| Age at onset of symptoms (yr), median (IQR) | 5.6 (3.1–8.4) | 5.5 (3.4–8.4) |
| Sex | ||
| Male, n (%) | 84 (27.5) | 33 (23.9) |
| Female, n (%) | 221 (72.5) | 105 (76.1) |
| Race/Ethnicity | ||
| White, n (%) | 234 (76.7) | 101 (73.2) |
| Hispanic, n (%) | 48 (15.7) | 25 (18.1) |
| Black/African American, n (%) | 13 (4.3) | 6 (4.3) |
| Asian, n (%) | 6 (2.0) | 5 (3.6) |
| Other, n (%) | 4 (1.3) | 1 (0.7) |
| Clinical Factors | median (IQR) | median (IQR) |
| Duration of untreated disease (mo) | 4.3 (2.0–10.3) n = 302 | 6.0 (3.1–12.8) |
| Duration from 1st treatment to enrollment a (mo) | 9.0 (1.3–29.9) | n/a |
| DAS | ||
| DAS Total (0–20) | 11.0 (7.5–13.0) n = 273 | 12.0 (8.9–14.0) n = 133 |
| DAS Skin (0–9) | 6.0 (5.0–7.0) n = 273 | 6.0 (5.0–7.0) n = 133 |
| DAS Muscle (0–11) | 5.0 (2.0–8.0) n = 276 | 6.0 (3.0–8.0) n = 133 |
| Laboratory Disease Activity Indicators | ||
| Neopterin (nmol/liter) | 12.9 (7.0–19.4) n = 257 | 17.2 (11.0–23.9) n = 124 |
| ESR (mm/hr) | 12.0 (7.0–20.0) n = 218 | 15.0 (9.0–23.0) n = 104 |
| vWF:Ag (%) | 140.0 (99.8–203.5) n = 260 | 140.0 (99.0–206.3) |
| Muscle Enzymes | ||
| CK (IU/L) | 114.0 (71.0–341.5) n = 267 | 154.5 (85.5–631.8) n = 132 |
| LDH (IU/L) | 298.5 (223.0–433.3) n = 264 | 350.5 (264.0–527.3) n = 131 |
| AST(SGOT) (IU/L) | 40.5 (28.0–67.3) n = 250 | 49.0 (36.0–107.0) n = 125 |
| Aldolase (U/L) | 8.8 (6.3–14.0) n = 249 | 10.3 (7.6–18.0) n = 123 |
| DAS Total | DAS Skin | DAS Muscle | ||||
|---|---|---|---|---|---|---|
| Effect Size (95% CI) | p Value | Effect Size (95% CI) | p Value | Effect Size (95% CI) | p Value | |
| Age (yr) | −0.14 (−0.21, −0.06) | <0.001 | −0.01 (−0.06, 0.04) | 1.000 | −0.13 (−0.16, −0.09) | <0.001 |
| Treatment Status at 1st Visit | ||||||
| Untreated | Reference | Reference | Reference | |||
| Treated | 0.94 (0.13, 1.76) | 0.014 | 0.42 (−0.18, 1.02) | 0.385 | 0.52 (0.11, 0.94) | 0.005 |
| vWF:Ag | ||||||
| Elevated | 2.55 (1.83, 3.27) | <0.001 | 0.96 (0.59, 1.34) | <0.001 | 1.59 (1.13, 2.04) | <0.001 |
| Odds Ratio (95% CI) | p Value | |
|---|---|---|
| Duration of untreated disease (mo) | 0.95 (0.91, 0.995) | 0.025 |
| Treatment status at 1st visit | ||
| Untreated | Reference | |
| Treated | 1.03 (0.66, 1.61) | 1.000 |
| DAS Skin Elements | ||
| Skin Involvement Distribution | ||
| None | Reference | |
| Focal (including areas of joint related skin) | 1.46 (1.07, 2.00) | 0.013 |
| Diffuse (including extensor surfaces of limbs/shawl) | 1.38 (0.88, 2.17) | 0.211 |
| Generalized (including trunk involvement) | 2.58 (1.27, 5.23) | 0.006 |
| Eyelid blood vessel dilation, present | 1.32 (1.01, 1.72) | 0.036 |
| DAS Muscle Elements | ||
| Functional Status | ||
| Within Normal Limits | Reference | |
| Minimal Limitations | 1.81 (1.27, 2.58) | <0.001 |
| Mild Limitations | 2.59 (1.81, 3.70) | <0.001 |
| Moderate Limitations | 3.65 (2.14, 6.23) | <0.001 |
| Severe Limitations | 9.19 (3.33, 25.38) | <0.001 |
| Neck flexor weakness | 1.32 (0.997, 1.75) | 0.053 |
| Unable to clear scapula | 1.56 (1.22, 2.01) | <0.001 |
| Lower proximal muscle weakness | 1.40 (1.07, 1.83) | 0.009 |
| Gower’s Sign | 1.58 (1.13, 2.19) | 0.004 |
| Difficulty Swallowing | 2.57 (1.50, 4.38) | <0.001 |
| Normal vWF:Ag | Elevated vWF:Ag | p Value | |
|---|---|---|---|
| Number of subjects, n (%) | 103 (74.6%) | 35 (25.4%) | |
| Age at onset of symptoms in years, median (IQR) | 5.7 (3.9–8.7) | 8.4 (5.4–9.9) | 0.017 |
| Duration of untreated disease in months, median (IQR) | 6.4 (3.6–13.5) | 3.8 (1.9–7.2) | 0.004 |
| Sex, n (%) | |||
| Female | 76 (74%) | 29 (83%) | 0.277 |
| Male | 27 (26%) | 6 (17%) | |
| Race/ethnicity, n (%) | |||
| White | 79 (77%) | 22 (63%) | 0.184 |
| Hispanic | 17 (16%) | 3 (7%) | |
| African American | 3 (3%) | 8 (23%) | |
| Asian | 4 (4%) | 1 (3%) | |
| Others | 0 (0%) | 1(3%) |
| Normal vWF:Ag | Elevated vWF:Ag | p Value | |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| DAS | |||
| DAS Total | 11 (8–13) | 13 (12–16) | <0.0001 |
| DAS Skin | 6 (5–7) | 5.5 (5–7) | 0.704 |
| DAS Muscle | 5 (2.5–7) | 8 (6–9) | <0.0001 |
| Laboratory Disease Activity Indicators | |||
| Neopterin (nmol/L) | 15.3 (9.5–22.4) | 21.6 (14.8–28) | 0.0098 |
| ESR (mm/h) | 13 (8–18) | 23 | <0.0001 |
| Muscle Enzymes | |||
| CK (IU/L) | 130 (83–356) | 579 (169–5283) | 0.0001 |
| LDH (IU/L) | 315 (253–435) | 512 (307–703) | 0.0008 |
| AST(SGOT) (IU/L) | 44 (33–64) | 143 (58–258) | <0.0001 |
| Aldolase (U/L) | 9.6 (6.9–14.2) | 18.4 (11–31) | <0.0001 |
| Flow Cytometry (% lymphocytes) | |||
| Total T cells (CD3+) | 62.9 (57–68) | 69 (63–74) | 0.0008 |
| T helper cells (CD3+ CD4+) | 42 (37–48) | 48 (43–54) | 0.0006 |
| T cytotoxic cells (CD3+ CD8+) | 19 (16–22) | 20 (17.5–23) | 0.323 |
| B cells (CD19+) | 29.5 (24–35) | 25 (19.8–30.8) | 0.049 |
| NK cells (CD16+/CD56+) | 6 (4–9) | 4 (3–7) | 0.0097 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibbs, E.; Khojah, A.; Morgan, G.; Ehwerhemuepha, L.; Pachman, L.M. The von Willebrand Factor Antigen Reflects the Juvenile Dermatomyositis Disease Activity Score. Biomedicines 2023, 11, 552. https://doi.org/10.3390/biomedicines11020552
Gibbs E, Khojah A, Morgan G, Ehwerhemuepha L, Pachman LM. The von Willebrand Factor Antigen Reflects the Juvenile Dermatomyositis Disease Activity Score. Biomedicines. 2023; 11(2):552. https://doi.org/10.3390/biomedicines11020552
Chicago/Turabian StyleGibbs, Ellie, Amer Khojah, Gabrielle Morgan, Louis Ehwerhemuepha, and Lauren M. Pachman. 2023. "The von Willebrand Factor Antigen Reflects the Juvenile Dermatomyositis Disease Activity Score" Biomedicines 11, no. 2: 552. https://doi.org/10.3390/biomedicines11020552