
Comparison of the Prognostic Value of Inflammatory and Nutritional Indices in Nonmetastatic Renal Cell Carcinoma

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Data Collection and Variable Definitions
2.3. Assessment of the Inflammatory Biomarkers and Nutrition Status
2.4. Statistical Analysis
3. Results
3.1. Patient Background
3.2. The Optimal Thresholds for NLR, PLR, CAR and PNI
3.3. Correlation of Clinical Oncological Parameters with Inflammatory Biomarkers and Nutrition Status
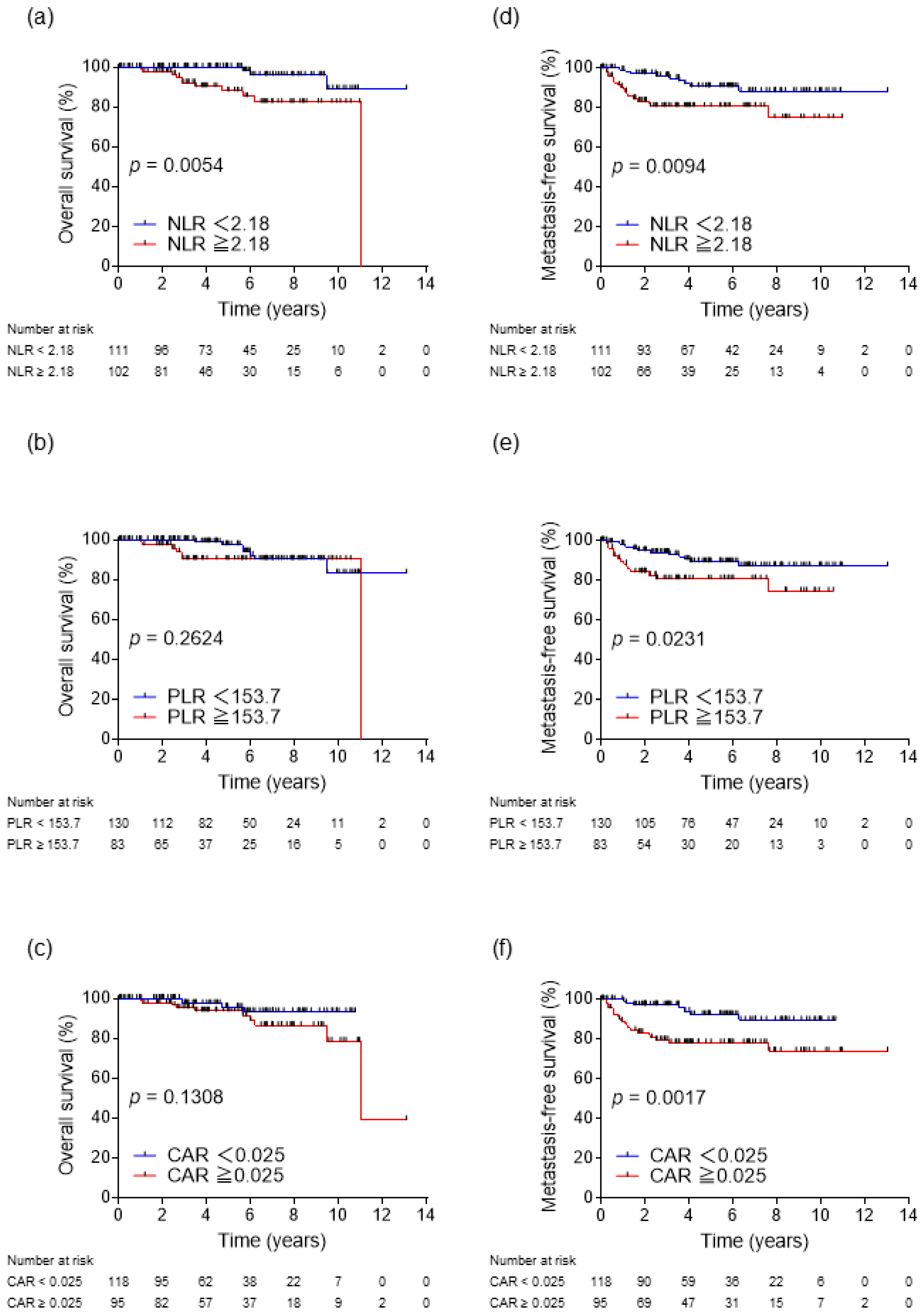
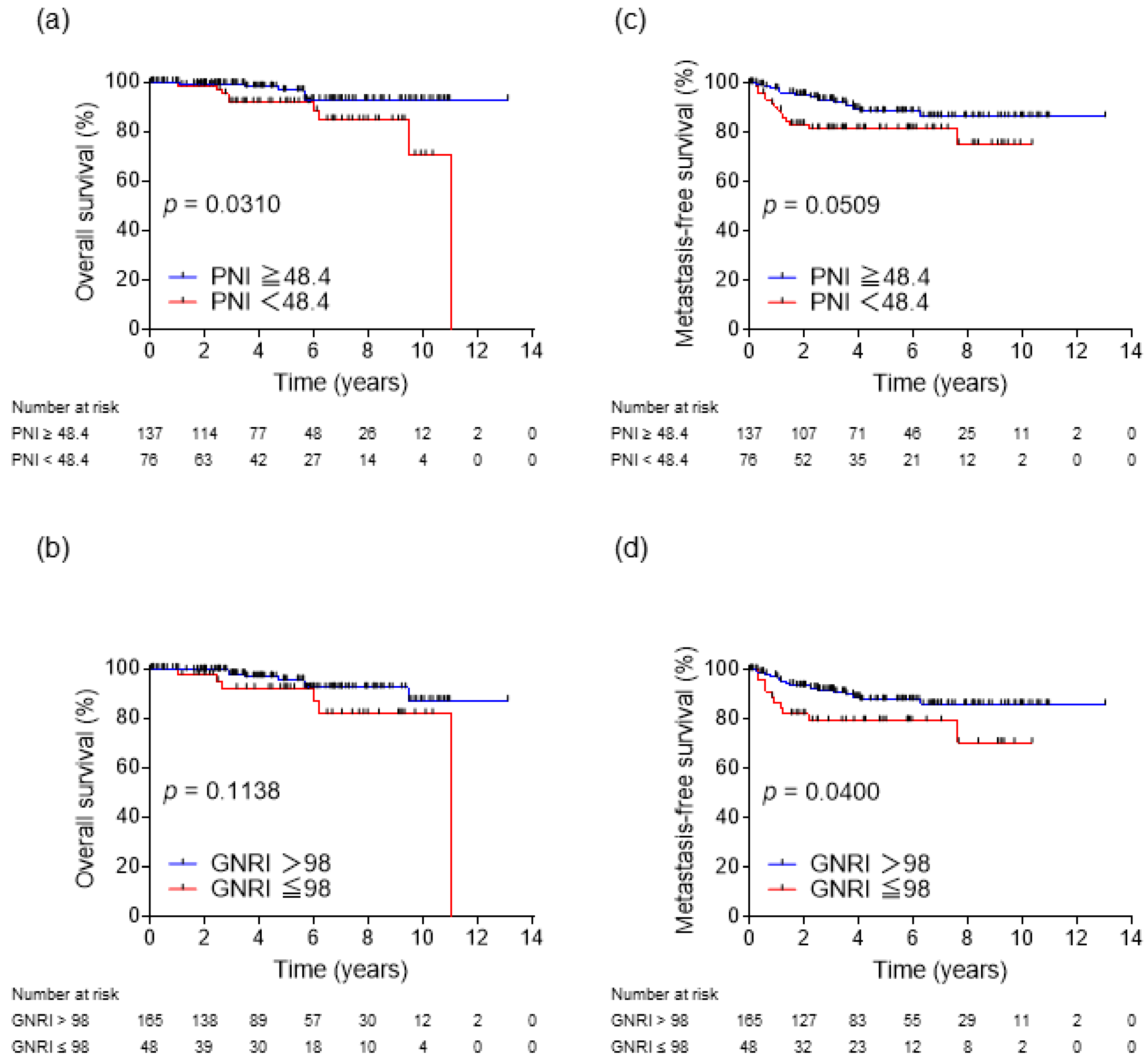
3.4. Survival Rates and Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frank, I.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Weaver, A.L.; Zincke, H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J. Urol. 2002, 168, 2395–2400. [Google Scholar] [CrossRef]
- Leibovich, B.C.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Frank, I.; Kwon, E.D.; Weaver, A.L.; Parker, A.S.; Zincke, H. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: A stratification tool for prospective clinical trials. Cancer 2003, 97, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Patard, J.J.; Kim, H.L.; Lam, J.S.; Dorey, F.J.; Pantuck, A.J.; Zisman, A.; Ficarra, V.; Han, K.R.; Cindolo, L.; De La Taille, A.; et al. Use of the University of California Los Angeles integrated staging system to predict survival in renal cell carcinoma: An international multicenter study. J. Clin. Oncol. 2004, 22, 3316–3322. [Google Scholar] [CrossRef] [PubMed]
- Karakiewicz, P.I.; Suardi, N.; Capitanio, U.; Jeldres, C.; Ficarra, V.; Cindolo, L.; de la Taille, A.; Tostain, J.; Mulders, P.F.; Bensalah, K.; et al. A preoperative prognostic model for patients treated with nephrectomy for renal cell carcinoma. Eur. Urol. 2009, 55, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.W.; Lee, J.H.; Shim, K.H.; Choo, S.H.; Choi, J.B.; Ahn, H.S.; Kim, S.J.; Kim, S.I. Prognostic significance of preoperative and follow-up neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in patients with non-metastatic clear cell renal cell carcinoma. Investig. Clin. Urol. 2019, 60, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Zhang, G.L. C-reactive protein to albumin ratio predicts the outcome in renal cell carcinoma: A meta-analysis. PLoS ONE 2019, 14, e0224266. [Google Scholar] [CrossRef]
- Mantzorou, M.; Koutelidakis, A.; Theocharis, S.; Giaginis, C. Clinical Value of Nutritional Status in Cancer: What is its Impact and how it Affects Disease Progression and Prognosis? Nutr. Cancer 2017, 69, 1151–1176. [Google Scholar] [CrossRef]
- Shao, Y.; Wu, B.; Jia, W.; Zhang, Z.; Chen, Q.; Wang, D. Prognostic value of pretreatment neutrophil-to-lymphocyte ratio in renal cell carcinoma: A systematic review and meta-analysis. BMC Urol. 2020, 20, 90. [Google Scholar] [CrossRef]
- Semeniuk-Wojtaś, A.; Lubas, A.; Stec, R.; Syryło, T.; Niemczyk, S.; Szczylik, C. Neutrophil-to-lymphocyte Ratio, Platelet-to-lymphocyte Ratio, and C-reactive Protein as New and Simple Prognostic Factors in Patients with Metastatic Renal Cell Cancer Treated with Tyrosine Kinase Inhibitors: A Systemic Review and Meta-analysis. Clin. Genitourin. Cancer 2018, 16, e685–e693. [Google Scholar] [CrossRef]
- Lucca, I.; de Martino, M.; Hofbauer, S.L.; Zamani, N.; Shariat, S.F.; Klatte, T. Comparison of the prognostic value of pretreatment measurements of systemic inflammatory response in patients undergoing curative resection of clear cell renal cell carcinoma. World J. Urol. 2015, 33, 2045–2052. [Google Scholar] [CrossRef] [PubMed]
- Peng, D.; He, Z.S.; Li, X.S.; Tang, Q.; Zhang, L.; Yang, K.W.; Yu, X.T.; Zhang, C.J.; Zhou, L.Q. Prognostic Value of Inflammatory and Nutritional Scores in Renal Cell Carcinoma After Nephrectomy. Clin. Genitourin. Cancer 2017, 15, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.G.; Choi, D.K.; Sung, H.H.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Choi, H.Y.; Lee, H.M. Preoperative Prognostic Nutritional Index is a Significant Predictor of Survival in Renal Cell Carcinoma Patients Undergoing Nephrectomy. Ann. Surg. Oncol. 2016, 23, 321–327. [Google Scholar] [CrossRef]
- Peng, Q.; Liu, L.; Li, T.; Lei, C.; Wan, H. Prognostic impact of prognostic nutritional index on renal cell carcinoma: A meta-analysis of 7629 patients. PLoS ONE 2022, 17, e0265119. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.W.; Seo, S.P.; Kim, W.T.; Yun, S.J.; Lee, S.C.; Kim, W.J.; Hwang, E.C.; Kang, S.H.; Hong, S.H.; Chung, J.; et al. A Low Geriatric Nutritional Risk Index is Associated with Aggressive Pathologic Characteristics and Poor Survival after Nephrectomy in Clear Renal Cell Carcinoma: A Multicenter Retrospective Study. Nutr. Cancer 2020, 72, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef]
- Mao, C.; Xu, W.; Ma, W.; Wang, C.; Guo, Z.; Yan, J. Prognostic Value of Pretreatment Prognostic Nutritional Index in Patients with Renal Cell Carcinoma: A Meta-Analysis. Front. Oncol. 2021, 11, 719941. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Mjaess, G.; Chebel, R.; Karam, A.; Moussa, I.; Pretot, D.; Abi Tayeh, G.; Sarkis, J.; Semaan, A.; Peltier, A.; Aoun, F.; et al. Prognostic role of neutrophil-to-lymphocyte ratio (NLR) in urological tumors: An umbrella review of evidence from systematic reviews and meta-analyses. Acta Oncol. 2021, 60, 704–713. [Google Scholar] [CrossRef]
- Zhou, X.; Luo, G. A meta-analysis of the platelet-lymphocyte ratio: A notable prognostic factor in renal cell carcinoma. Int. J. Biol. Markers 2022, 37, 123–133. [Google Scholar] [CrossRef]
- Caliskan, S. Elevated neutrophil to lymphocyte and platelet to lymphocyte ratios predict high grade and advanced stage renal cell carcinoma. Int. J. Biol. Markers 2019, 34, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Nozawa, H.; Chiu, C.; Hanahan, D. Infiltrating neutrophils mediate the initial angiogenic switch in a mouse model of multistage carcinogenesis. Proc. Natl. Acad. Sci. USA 2006, 103, 12493–12498. [Google Scholar] [CrossRef] [PubMed]
- Gooden, M.J.; de Bock, G.H.; Leffers, N.; Daemen, T.; Nijman, H.W. The prognostic influence of tumour-infiltrating lymphocytes in cancer: A systematic review with meta-analysis. Br. J. Cancer 2011, 105, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Masucci, M.T.; Minopoli, M.; Carriero, M.V. Tumor Associated Neutrophils. Their Role in Tumorigenesis, Metastasis, Prognosis and Therapy. Front. Oncol. 2019, 9, 1146. [Google Scholar] [CrossRef]
- el-Hag, A.; Clark, R.A. Immunosuppression by activated human neutrophils. Dependence on the myeloperoxidase system. J. Immunol. 1987, 139, 2406–2413. [Google Scholar] [CrossRef]
- Wang, Z.; Peng, S.; Wang, A.; Xie, H.; Guo, L.; Jiang, N.; Niu, Y. Platelet-lymphocyte ratio acts as an independent predictor of prognosis in patients with renal cell carcinoma. Clin. Chim. Acta 2018, 480, 166–172. [Google Scholar] [CrossRef]
- Tsujino, T.; Komura, K.; Hashimoto, T.; Muraoka, R.; Satake, N.; Matsunaga, T.; Tsutsumi, T.; Yoshikawa, Y.; Takai, T.; Minami, K.; et al. C-reactive protein-albumin ratio as a prognostic factor in renal cell carcinoma—A data from multi-institutional study in Japan. Urol. Oncol. 2019, 37, 812.e1–812.e8. [Google Scholar] [CrossRef]
- Asegaonkar, S.B.; Asegaonkar, B.N.; Takalkar, U.V.; Advani, S.; Thorat, A.P. C-Reactive Protein and Breast Cancer: New Insights from Old Molecule. Int. J. Breast Cancer 2015, 2015, 145647. [Google Scholar] [CrossRef]
- Andus, T.; Geiger, T.; Hirano, T.; Northoff, H.; Ganter, U.; Bauer, J.; Kishimoto, T.; Heinrich, P.C. Recombinant human B cell stimulatory factor 2 (BSF-2/IFN-beta 2) regulates beta-fibrinogen and albumin mRNA levels in Fao-9 cells. FEBS Lett. 1987, 221, 18–22. [Google Scholar] [CrossRef]
- Caraceni, P.; Tufoni, M.; Bonavita, M.E. Clinical use of albumin. Blood Transfus. 2013, 11 (Suppl. 4), s18–s25. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Chen, S.; Xu, J.; Li, G.; He, Y. The prognostic significance of the prognostic nutritional index in cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Ruan, G.T.; Zhang, Q.; Zhang, X.; Tang, M.; Song, M.M.; Zhang, X.W.; Li, X.R.; Zhang, K.P.; Ge, Y.Z.; Yang, M.; et al. Geriatric Nutrition Risk Index: Prognostic factor related to inflammation in elderly patients with cancer cachexia. J. Cachexia Sarcopenia Muscle 2021, 12, 1969–1982. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.M.; Power, D.G.; Daly, L.; Cushen, S.J.; Ni Bhuachalla, E.; Prado, C.M. Cancer-associated malnutrition, cachexia and sarcopenia: The skeleton in the hospital closet 40 years later. Proc. Nutr. Soc. 2016, 75, 199–211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | n (%) | NLR, Median (IQR) | p-Value | PLR, Median (IQR) | p-Value | CAR, Median (IQR) | p-Value | PNI, Median (IQR) | p-Value | GNRI, Median (IQR) | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.008 | 0.685 | 0.154 | <0.001 | <0.001 | ||||||
| <65 | 113 (53.1) | 1.97 (1.40–2.78) | 139.2 (106.3–177.6) | 0.023 (0–0.047) | 52.0 (48.9–55.2) | 105.7 (101.7–109.1) | |||||
| ≥65 | 100 (46.9) | 2.43 (1.72–3.21) | 132.3 (105.6–179.9) | 0.025 (0.022–0.050) | 48.1 (44.0–51.6) | 101.3 (96.5–105.7) | |||||
| Gender | 0.484 | 0.001 | 0.231 | 0.036 | 0.026 | ||||||
| Male | 155 (72.8) | 2.17 (1.64–2.96) | 129.9 (98.3–172.5) | 0.024 (0.021–0.049) | 50.9 (46.9–54.6) | 104.2 (99.8–108.3) | |||||
| Female | 58 (27.2) | 1.91 (1.36–3.20) | 163.5 (121.7–214.3) | 0.024 (0–0.044) | 49.1 (44.6–53.0) | 102.8 (95.3–106.4) | |||||
| BMI | 0.681 | 0.213 | <0.001 | 0.215 | 0.022 | ||||||
| <25 | 139 (65.3) | 2.05 (1.62–3.05) | 140.0 (114.0–177.1) | 0.023 (0–0.029) | 50.5 (46.1–53.4) | 102.8 (96.8–106.8) | |||||
| ≥25 | 74 (34.7) | 2.26 (1.63–2.96) | 130.4 (92.6–182.6) | 0.032 (0.022–0.070) | 51.3 (46.5–55.0) | 105.7 (100.9–108.7) | |||||
| Tumor size | 0.393 | 0.557 | <0.001 | 0.397 | 0.150 | ||||||
| ≤4 cm | 157 (73.7) | 2.05 (1.60–2.97) | 136.0 (105.9–176.9) | 0.023 (0–0.036) | 50.8 (46.8–53.6) | 104.2 (99.7–107.2) | |||||
| >4 cm | 56 (26.3) | 2.23 (1.69–3.34) | 138.9 (106.1–214.2) | 0.044 (0.023–0.095) | 50.7 (43.6–54.1) | 102.8 (93.9–108.7) | |||||
| Pathological T stage | 0.015 | 0.126 | <0.001 | 0.227 | 0.233 | ||||||
| 1–2 | 167 (78.4) | 2.01 (1.55–2.88) | 135.1 (100.9–176.7) | 0.023 (0–0.044) | 51.0 (46.7–54.0) | 104.2 (99.6–108.0) | |||||
| 3–4 | 32 (15.0) | 2.56 (1.87–3.55) | 140.8 (116.0–244.6) | 0.064 (0.026–0.357) | 50.2 (42.0–53.7) | 100.9 (93.9–108.3) | |||||
| Unknown | 14 (6.6) | ||||||||||
| Histologic type | 0.158 | 0.594 | 0.865 | 0.939 | 0.211 | ||||||
| ccRCC | 172 (80.8) | 2.20 (1.61–3.06) | 139.7 (107.2–179.2) | 0.024 (0.021–0.047) | 50.9 (46.4–54.0) | 104.2 (99.7–108.0) | |||||
| Non-ccRCC | 33 (15.5) | 1.80 (1.63–2.55) | 136.0 (96.4–183.3) | 0.023 (0–0.100) | 51.3 (45.9–53.4) | 102.1 (95.5–107.2) | |||||
| Unknown | 8 (3.8) | ||||||||||
| Tumor grade | 0.003 | 0.003 | <0.001 | 0.001 | 0.007 | ||||||
| <3 | 160 (75.1) | 2.04 (1.56–2.88) | 132.6 (101.0–174.8) | 0.024 (0.005–0.043) | 51.1 (47.1–54.2) | 104.2 (99.8–108.0) | |||||
| ≥3 | 34 (16.0) | 2.58 (1.95–3.69) | 170.4 (125.1–253.3) | 0.050 (0.022–0.467) | 47.0 (40.0–51.6) | 101.0 (89.2–106.1) | |||||
| Unknown | 19 (8.9) | ||||||||||
| LVI | 0.424 | 0.215 | 0.163 | 0.858 | 0.799 | ||||||
| No | 109 (51.2) | 2.03 (1.56–2.83) | 135.1 (98.0–172.1) | 0.024 (0.021–0.036) | 50.9 (46.0–54.6) | 104.2 (98.3–108.3) | |||||
| Yes | 89 (41.8) | 2.26 (1.64–3.02) | 141.0 (109.6–184.9) | 0.025 (0–0.066) | 51.0 (47.1–53.9) | 104.2 (99.2–107.3) | |||||
| Unknown | 15 (7.0) |
| Variables | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | HR (95% CI) | ||
| Age | ≥65 vs. <65 | 0.164 | 0.57 (0.25–1.26) | ||
| Sex | Male vs. Female | 0.105 | 2.41 (0.83–6.97) | ||
| BMI | ≥25 vs. <25 | 0.654 | 1.20 (0.55–2.61) | ||
| Tumor size | >4 cm vs. ≤4 cm | <0.001 | 9.25 (3.91–21.90) | ||
| Pathological T-stage | 3–4 vs. 1–2 | <0.001 | 9.84 (4.49–21.57) | ||
| Histologic type | Non-ccRCC vs. ccRCC | 0.611 | 1.27 (0.51–3.14) | ||
| Grade | ≥3 vs. <3 | <0.001 | 10.39 (4.74–22.74) | ||
| LVI | Yes vs. no | <0.001 | 9.01 (3.09–26.24) | ||
| NLR | ≥2.18 vs. <2.18 | 0.013 | 2.77 (1.24–6.17) | 0.132 | 1.99 (0.81–4.87) |
| PLR | ≥153.7 vs. <153.7 | 0.027 | 4.24 (1.95–9.24) | 0.236 | 1.68 (0.71–3.95) |
| CAR | ≥0.025 vs. <0.025 | 0.003 | 3.63 (1.54–8.59) | 0.016 | 3.08 (1.24–7.67) |
| PNI | <48.4 vs. ≥48.4 | 0.056 | 2.09 (0.98–4.44) | 0.605 | 0.75 (0.24–2.27) |
| GNRI | ≤98 vs. >98 | 0.045 | 2.22 (1.02–4.85) | 0.439 | 1.54 (0.52–4.56) |
| Variables | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | HR (95% CI) | ||
| Age | ≥65 vs. <65 | 0.930 | 1.05 (0.35–3.14) | ||
| Sex | Male vs. Female | 0.266 | 2.36 (0.52–10.68) | ||
| BMI | ≥25 vs. <25 | 0.812 | 1.14 (0.38–3.43) | ||
| Tumor size | >4 cm vs. ≤4 cm | 0.261 | 1.84 (0.63–5.36) | ||
| Pathological T-stage | 3–4 vs. 1–2 | 0.247 | 2.03 (0.61–6.71) | ||
| Histologic type | Non-ccRCC vs. ccRCC | 0.820 | 1.16 (0.31–4.31) | ||
| Grade | ≥3 vs. <3 | 0.598 | 1.43 (0.38–5.42) | ||
| LVI | Yes vs. no | 0.054 | 2.96 (0.98–8.89) | ||
| NLR | ≥2.18 vs. <2.18 | 0.012 | 5.11 (1.42–18.36) | 0.049 | 3.96 (1.01–15.59) |
| PLR | ≥153.7 vs. <153.7 | 0.268 | 1.81 (0.63–5.19) | ||
| CAR | ≥0.025 vs. <0.025 | 0.144 | 2.41 (0.74–7.82) | ||
| PNI | <48.4 vs. ≥48.4 | 0.041 | 3.15 (1.05–9.43) | 0.303 | 1.86 (0.57–6.06) |
| GNRI | ≤98 vs. >98 | 0.124 | 2.32 (0.79–6.78) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makino, T.; Izumi, K.; Iwamoto, H.; Kadomoto, S.; Kadono, Y.; Mizokami, A. Comparison of the Prognostic Value of Inflammatory and Nutritional Indices in Nonmetastatic Renal Cell Carcinoma. Biomedicines 2023, 11, 533. https://doi.org/10.3390/biomedicines11020533
Makino T, Izumi K, Iwamoto H, Kadomoto S, Kadono Y, Mizokami A. Comparison of the Prognostic Value of Inflammatory and Nutritional Indices in Nonmetastatic Renal Cell Carcinoma. Biomedicines. 2023; 11(2):533. https://doi.org/10.3390/biomedicines11020533
Chicago/Turabian StyleMakino, Tomoyuki, Kouji Izumi, Hiroaki Iwamoto, Suguru Kadomoto, Yoshifumi Kadono, and Atsushi Mizokami. 2023. "Comparison of the Prognostic Value of Inflammatory and Nutritional Indices in Nonmetastatic Renal Cell Carcinoma" Biomedicines 11, no. 2: 533. https://doi.org/10.3390/biomedicines11020533