
Secreted Frizzled Related Protein 5 (SFRP5) Serum Levels Are Decreased in Critical Illness and Sepsis and Are Associated with Short-Term Mortality
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. SFRP5 Measurements
2.3. Statistical Analysis
3. Results
3.1. SFRP5 Levels Are Decreased in Critical Illness and Sepsis
3.2. SFRP5 Levels Are Dependent of Age and Comorbidities, but Independent of Sex and BMI in Critical Illness
3.3. SFRP5 Levels Correlate with Biomarkers of (Anti-)Inflammation as well as Hepatic and Lipid Metabolism
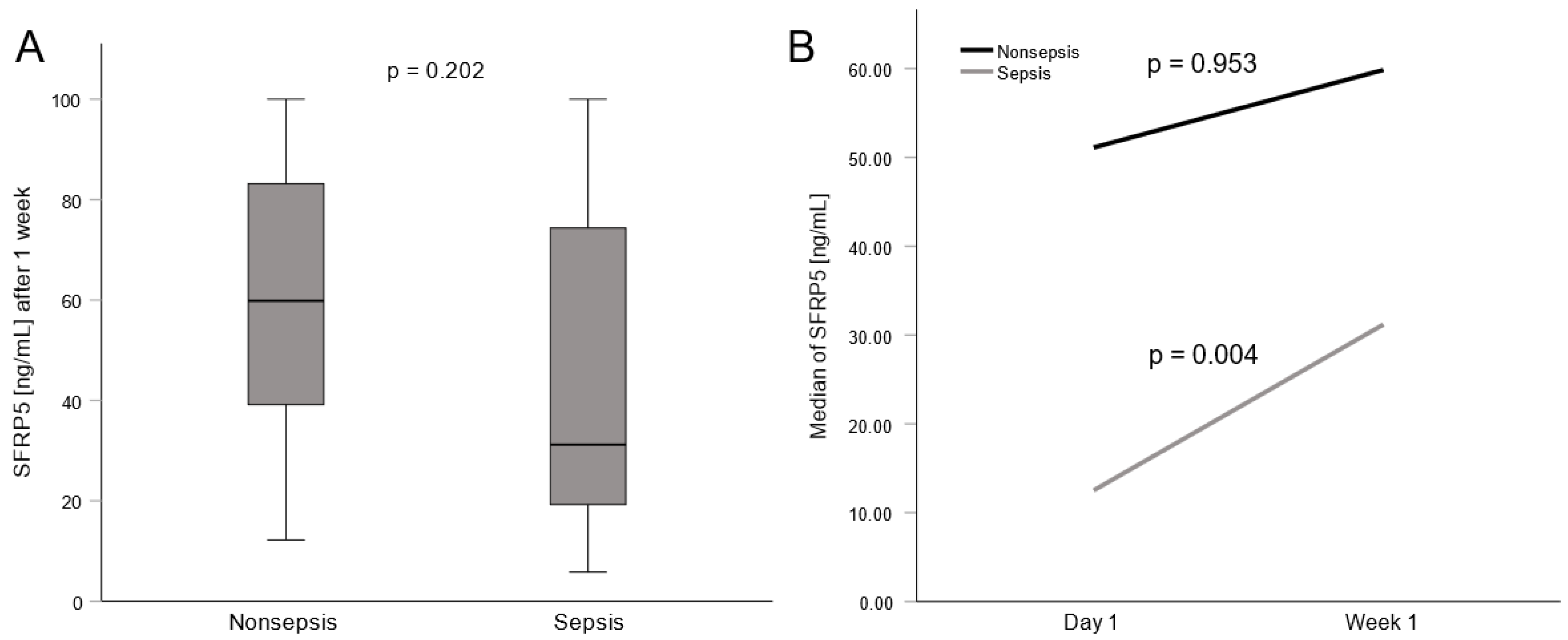
3.4. Septic Patients Recover Levels of SFRP5 after One Week of Intensive Care Treatment
3.5. SFRP5 Levels at Admission to the ICU Are Predictors of Short-Term Mortality in Critical Illness but Not Sepsis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleischmann-Struzek, C.; Mellhammar, L.; Rose, N.; Cassini, A.; Rudd, K.E.; Schlattmann, P.; Allegranzi, B.; Reinhart, K. Incidence and mortality of hospital- and ICU-treated sepsis: Results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Boomer, J.S.; Green, J.M.; Hotchkiss, R.S. The changing immune system in sepsis: Is individualized immuno-modulatory therapy the answer? Virulence 2014, 5, 45–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Ryan, T.; Coakley, J.D.; Martin-Loeches, I. Defects in innate and adaptive immunity in patients with sepsis and health care associated infection. Ann. Transl. Med. 2017, 5, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hohlstein, P.; Gussen, H.; Bartneck, M.; Warzecha, K.T.; Roderburg, C.; Buendgens, L.; Trautwein, C.; Koch, A.; Tacke, F. Prognostic Relevance of Altered Lymphocyte Subpopulations in Critical Illness and Sepsis. J. Clin. Med. 2019, 8, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loosen, S.H.; Koch, A.; Tacke, F.; Roderburg, C.; Luedde, T. The Role of Adipokines as Circulating Biomarkers in Critical Illness and Sepsis. Int. J. Mol. Sci. 2019, 20, 4820. [Google Scholar] [CrossRef] [Green Version]
- Shubin, N.J.; Monaghan, S.F.; Ayala, A. Anti-inflammatory mechanisms of sepsis. Contrib. Microbiol. 2011, 17, 108–124. [Google Scholar]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-induced immunosuppression: From cellular dysfunctions to immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutaki, D.; Michos, A.; Bacopoulou, F.; Charmandari, E. The Emerging Role of Sfrp5 and Wnt5a in the Pathogenesis of Obesity: Implications for a Healthy Diet and Lifestyle. Nutrients 2021, 13, 2459. [Google Scholar] [CrossRef]
- Bertran, L.; Portillo-Carrasquer, M.; Aguilar, C.; Porras, J.A.; Riesco, D.; Martinez, S.; Vives, M.; Sabench, F.; Gonzalez, E.; Del Castillo, D.; et al. Deregulation of Secreted Frizzled-Related Protein 5 in Nonalcoholic Fatty Liver Disease Associated with Obesity. Int. J. Mol. Sci. 2021, 22, 6895. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, J.; Kim, D.W.; Ha, Y.; Ihm, M.H.; Kim, H.; Song, K.; Lee, I. Wnt5a induces endothelial inflammation via beta-catenin-independent signaling. J. Immunol. 2010, 185, 1274–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, C.; Schaer, D.J.; Bachli, E.B.; Kurrer, M.O.; Schoedon, G. Wnt5A/CaMKII signaling contributes to the inflammatory response of macrophages and is a target for the antiinflammatory action of activated protein C and interleukin-10. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 504–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenthal, A.; Ehlers, S.; Lauber, J.; Buer, J.; Lange, C.; Goldmann, T.; Heine, H.; Brandt, E.; Reiling, N. The Wingless homolog WNT5A and its receptor Frizzled-5 regulate inflammatory responses of human mononuclear cells induced by microbial stimulation. Blood 2006, 108, 965–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergenfelz, C.; Medrek, C.; Ekstrom, E.; Jirstrom, K.; Janols, H.; Wullt, M.; Bredberg, A.; Leandersson, K. Wnt5a induces a tolerogenic phenotype of macrophages in sepsis and breast cancer patients. J. Immunol. 2012, 188, 5448–5458. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.B.; Chen, X.D.; Zhou, X.Y.; Zhu, Q. The Wnt antagonist and secreted frizzled-related protein 5: Implications on lipid metabolism, inflammation, and type 2 diabetes mellitus. Biosci. Rep. 2018, 38, BSR20180011. [Google Scholar] [CrossRef]
- Garcia-Tobilla, P.; Solorzano, S.R.; Salido-Guadarrama, I.; Gonzalez-Covarrubias, V.; Morales-Montor, G.; Diaz-Otanez, C.E.; Rodríguez-Dorantes, M. SFRP1 repression in prostate cancer is triggered by two different epigenetic mechanisms. Gene 2016, 593, 292–301. [Google Scholar] [CrossRef]
- Chatani, N.; Kamada, Y.; Kizu, T.; Ogura, S.; Furuta, K.; Egawa, M.; Hamano, M.; Ezaki, H.; Kiso, S.; Shimono, A.; et al. Secreted frizzled-related protein 5 (Sfrp5) decreases hepatic stellate cell activation and liver fibrosis. Liver Int. 2015, 35, 2017–2026. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Chen, L.; Shan, X.; Shan, X.; Tang, J.; Zhou, F.; Chen, Q.; Quan, H.; Nie, D.; Zhang, W.; et al. Epigenetic silencing of SFRP1 and SFRP5 by hepatitis B virus X protein enhances hepatoma cell tumorigenicity through Wnt signaling pathway. Int. J. Cancer 2014, 135, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, M.; Sheldahl, L.C.; Park, M.; Miller, J.R.; Moon, R.T. The Wnt/Ca2+ pathway: A new vertebrate Wnt signaling pathway takes shape. Trends Genet. 2000, 16, 279–283. [Google Scholar] [CrossRef]
- Chang, J.T.; Esumi, N.; Moore, K.; Li, Y.; Zhang, S.; Chew, C.; Goodman, B.; Rattner, A.; Moody, S.; Stetten, G.; et al. Cloning and characterization of a secreted frizzled-related protein that is expressed by the retinal pigment epithelium. Hum. Mol. Genet. 1999, 8, 575–583. [Google Scholar] [CrossRef]
- Chen, L.; Zhao, X.; Liang, G.; Sun, J.; Lin, Z.; Hu, R.; Chen, P.; Zhang, Z.; Zhou, L.; Li, Y. Recombinant SFRP5 protein significantly alleviated intrahepatic inflammation of nonalcoholic steatohepatitis. Nutr. Metab. 2017, 14, 56. [Google Scholar] [CrossRef] [Green Version]
- Ouchi, N.; Higuchi, A.; Ohashi, K.; Oshima, Y.; Gokce, N.; Shibata, R.; Akasaki, Y.; Shimono, A.; Walsh, K. Sfrp5 is an anti-inflammatory adipokine that modulates metabolic dysfunction in obesity. Science 2010, 329, 454–457. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Hoyos, M.; Cantalapiedra, D.; Arroyo, C.; Esteve, P.; Rodriguez, J.; Riveiro, R.; Trujillo, M.J.; Ramos, C.; Bovolenta, P.; Ayuso, C. Evaluation of SFRP1 as a candidate for human retinal dystrophies. Mol. Vis. 2004, 10, 426–431. [Google Scholar]
- Carstensen-Kirberg, M.; Kannenberg, J.M.; Huth, C.; Meisinger, C.; Koenig, W.; Heier, M.; Peters, A.; Rathmann, W.; Roden, M.; Herder, C.; et al. Inverse associations between serum levels of secreted frizzled-related protein-5 (SFRP5) and multiple cardiometabolic risk factors: KORA F4 study. Cardiovasc. Diabetol. 2017, 16, 109. [Google Scholar] [CrossRef] [Green Version]
- Carstensen, M.; Wiza, C.; Rohrig, K.; Fahlbusch, P.; Roden, M.; Herder, C.; Ouwens, D.M. Effect of Sfrp5 on cytokine release and insulin action in primary human adipocytes and skeletal muscle cells. PLoS ONE 2014, 9, e85906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Peng, Q.; Jiang, F.; Xue, L.; Li, J.; Fan, Z.; Chen, P.; Chen, G.; Cai, Y. Secreted frizzled-related protein 5 protects against oxidative stress-induced apoptosis in human aortic endothelial cells via downregulation of Bax. J. Biochem. Mol. Toxicol. 2017, 31, e21978. [Google Scholar] [CrossRef]
- Sun, M.; Wang, W.; Min, L.; Chen, C.; Li, Q.; Weng, W. Secreted frizzled-related protein 5 (SFRP5) protects ATDC5 cells against LPS-induced inflammation and apoptosis via inhibiting Wnt5a/JNK pathway. J. Orthop. Surg. Res. 2021, 16, 129. [Google Scholar] [CrossRef]
- Mori, H.; Prestwich, T.C.; Reid, M.A.; Longo, K.A.; Gerin, I.; Cawthorn, W.P.; Susulic, V.S.; Krishnan, V.; Greenfield, A.; Macdougald, O.A. Secreted frizzled-related protein 5 suppresses adipocyte mitochondrial metabolism through WNT inhibition. J. Clin. Investig. 2012, 122, 2405–2416. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Rankin, S.A.; Sinner, D.; Kenny, A.P.; Krieg, P.A.; Zorn, A.M. Sfrp5 coordinates foregut specification and morphogenesis by antagonizing both canonical and noncanonical Wnt11 signaling. Genes Dev. 2008, 22, 3050–3063. [Google Scholar] [CrossRef] [Green Version]
- Schulte, D.M.; Muller, N.; Neumann, K.; Oberhauser, F.; Faust, M.; Gudelhofer, H.; Brandt, B.; Krone, W.; Laudes, M. Pro-inflammatory wnt5a and anti-inflammatory sFRP5 are differentially regulated by nutritional factors in obese human subjects. PLoS ONE 2012, 7, e32437. [Google Scholar] [CrossRef]
- Marinou, K.; Christodoulides, C.; Antoniades, C.; Koutsilieris, M. Wnt signaling in cardiovascular physiology. Trends Endocrinol. Metab. 2012, 23, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Rydzewska, M.; Nikolajuk, A.; Matulewicz, N.; Stefanowicz, M.; Karczewska-Kupczewska, M. Serum secreted frizzled-related protein 5 in relation to insulin sensitivity and its regulation by insulin and free fatty acids. Endocrine 2021, 74, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.C.; Wang, C.P.; Hsu, C.C.; Chiu, C.A.; Yu, T.H.; Hung, W.C.; Lu, L.F.; Chung, F.M.; Tsai, I.T.; Lin, H.C.; et al. Circulating secreted frizzled-related protein 5 (Sfrp5) and wingless-type MMTV integration site family member 5a (Wnt5a) levels in patients with type 2 diabetes mellitus. Diabetes Metab. Res. Rev. 2013, 29, 551–556. [Google Scholar] [PubMed]
- Tong, S.; Ji, Q.; Du, Y.; Zhu, X.; Zhu, C.; Zhou, Y. Sfrp5/Wnt Pathway: A Protective Regulatory System in Atherosclerotic Cardiovascular Disease. J. Interferon. Cytokine Res. 2019, 39, 472–482. [Google Scholar] [CrossRef] [Green Version]
- An, Y.; Wang, Q.; Wang, H.; Zhang, N.; Zhang, F. Clinical significance of sFRP5, RBP-4 and NT-proBNP in patients with chronic heart failure. Am. J. Transl. Res. 2021, 13, 6305–6311. [Google Scholar]
- Schulte, D.M.; Kragelund, D.; Muller, N.; Hagen, I.; Elke, G.; Titz, A.; Schädler, D.; Schumacher, J.; Weiler, N.; Bewig, B.; et al. The wingless-related integration site-5a/secreted frizzled-related protein-5 system is dysregulated in human sepsis. Clin. Exp. Immunol. 2015, 180, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.Y.; Park, H.H.; Kim, H.; Kim, H.N.; Kim, I.; Jeon, S.; Kim, W.; Bae, J.S.; Lee, W. Wnt5a and Wnt11 as acute respiratory distress syndrome biomarkers for severe acute respiratory syndrome coronavirus 2 patients. Eur. Respir. J. 2020, 56, 2001531. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Voigt, S.; Kruschinski, C.; Sanson, E.; Duckers, H.; Horn, A.; Yagmur, E.; Zimmermann, H.; Trautwein, C.; Tacke, F. Circulating soluble urokinase plasminogen activator receptor is stably elevated during the first week of treatment in the intensive care unit and predicts mortality in critically ill patients. Crit. Care 2011, 15, R63. [Google Scholar] [CrossRef] [Green Version]
- Kurt, B.; Buendgens, L.; Wirtz, T.H.; Loosen, S.H.; Schulze-Hagen, M.; Truhn, D.; Brozat, J.F.; Abu Jhaisha, S.; Hohlstein, P.; Koek, G.; et al. Serum Perilipin 2 (PLIN2) Predicts Multiple Organ Dysfunction in Critically Ill Patients. BioMedicines 2021, 9, 1210. [Google Scholar] [CrossRef]
- Ward, P.A. New approaches to the study of sepsis. EMBO Mol. Med. 2012, 4, 1234–1243. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients | Sepsis | Nonsepsis | p-Value |
|---|---|---|---|---|
| Number n | 223 | 147 | 76 | |
| Sex (male/female) n | 134/89 | 87/60 | 47/29 | 0.701 |
| Age (years) | 63 (18–90) | 64 (20–90) | 61 (18–85) | 0.587 |
| APACHE II score | 18 (3–43) | 19 (3–43) | 15 (3–33) | 0.003 * |
| SOFA score | 10 (0–19) | 11 (3–19) | 8.5 (0–16) | 0.008 * |
| Charlson Comorbidity Index | 5 (0–12) | 5 (0–12) | 5 (0–11) | 0.433 |
| Mechanical ventilation n (%) | 166 (74.4) | 111 (75.5) | 55 (72.4) | 0.610 |
| Vasopressor demand n (%) | 152 (68.2) | 109 (74.1) | 43 (56.6) | 0.008 * |
| ICU days n | 9 (2–137) | 12 (2–137) | 7 (2–45) | 0.002 * |
| Death in ICU n (%) | 54 (24.2) | 38 (25.9) | 16 (21.1) | 0.428 |
| 30-day mortality n (%) | 61 (27.4) | 43 (29.3) | 18 (23.7) | 0.374 |
| 1-year mortality n (%) | 98 (43.9) | 74 (50.3) | 24 (31.6) | 0.015 * |
| SFRP5 (ng/mL) | 24.66 (0.06–100) | 19.21 (0.06–100) | 32.83 (0.10–100) | 0.031 * |
| Etiology of (non)Sepsis Critical Illness, n (%) | Sepsis n = 147 | Nonsepsis n = 76 |
|---|---|---|
| Pulmonary | 83 (56.5) | |
| Abdominal | 22 (15.0) | |
| Urogenital | 10 (6.8) | |
| Other | 32 (21.8) | |
| Cardiocirculatory disorder | 17 (22.4) | |
| Respiratory failure | 12 (15.8) | |
| Advanced liver disease | 17 (22.4) | |
| Other | 30 (39.5) |
| Parameters | r | p-Value |
|---|---|---|
| Demographics | ||
| Age | −0.138 | 0.040 * |
| Body mass index | 0.022 | 0.755 |
| Blood count and markers of inflammation | ||
| Leukocytes | 0.133 | 0.048 * |
| Hemoglobin | 0.140 | 0.036 * |
| Platelets | 0.034 | 0.616 |
| C-reactive Protein | −0.088 | 0.190 |
| Procalcitonin | −0.175 | 0.028 * |
| Interleukin 6 | −0.061 | 0.435 |
| Interleukin 10 | −0.302 | <0.001 * |
| Electrolytes and renal system | ||
| Sodium | 0.083 | 0.219 |
| Potassium | 0.084 | 0.212 |
| Urea | 0.047 | 0.489 |
| Uric acid | 0.053 | 0.480 |
| Creatinine | −0.004 | 0.953 |
| Cystatin C | 0.021 | 0.772 |
| Hepato-pancreatico-biliary system and coagulation | ||
| Protein, total | 0.238 | <0.001 * |
| Albumin | 0.228 | 0.008 * |
| INR | −0.030 | 0.662 |
| aPTT | −0.154 | 0.023 * |
| Bilirubin, total | 0.110 | 0.113 |
| Gamma-GT | 0.093 | 0.166 |
| AST | 0.095 | 0.172 |
| ALT | 0.117 | 0.084 |
| Lipase | 0.147 | 0.049 * |
| Cardiopulmonary system | ||
| NTproBNP | −0.003 | 0.978 |
| Norephinephrine demand at day 1 (µg/day) | −0.017 | 0.816 |
| Horovitz quotient (PaO2/FiO2) | 0.049 | 0.724 |
| Ventilatory FiO2 demand | 0.156 | 0.161 |
| Net fluid balance day 1 | −0.059 | 0.406 |
| Net fluid balance day 3 | −0.070 | 0.332 |
| Metabolism and endocrinology | ||
| Glucose | −0.039 | 0.564 |
| HbA1c | 0.116 | 0.242 |
| Insulin | 0.123 | 0.219 |
| C-Peptide | 0.004 | 0.966 |
| HOMA IR | 0.021 | 0.838 |
| Cholesterol | 0.173 | 0.019 * |
| HDL-cholesterol | 0.201 | 0.046 * |
| LDL-cholesterol | 0.265 | 0.008 * |
| Triglycerides | 0.058 | 0.436 |
| ICU parameters | ||
| Days on ICU | −0.155 | 0.021 * |
| SOFA day 1 | 0.027 | 0.803 |
| SOFA day 3 | −0.064 | 0.585 |
| APACHE-II day 1 | −0.034 | 0.661 |
| APACHE-II day 3 | −0.097 | 0.391 |
| Comorbidity | SFRP5 Concentration in ng/mL, Median (Range) | p-Value |
|---|---|---|
| Diabetes | 22.13 (0.06–100) | 0.972 |
| Liver disease | 47.77 (6.59–100) | 0.005 * |
| Coronary artery disease | 21.54 (0.06–100) | 0.063 |
| Hypertension | 25.44 (0.10–100) | 0.729 |
| Chronic alcohol abuse | 34.68 (3.28–100) | 0.077 |
| Chronic obstructive lung disease | 17.44 (1.94–100) | 0.497 |
| Active malignancy | 13.09 (0.06–100) | 0.056 |
| Adipokine | r | p-Value | n |
|---|---|---|---|
| Adiponectin | 0.169 | 0.109 | 91 |
| Ghrelin | 0.101 | 0.350 | 88 |
| Resistin | −0.288 | 0.006 * | 91 |
| Leptin | 0.069 | 0.517 | 91 |
| Leptin receptor | 0.178 | 0.093 | 90 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hohlstein, P.; Brozat, J.F.; Schuler, J.; Abu Jhaisha, S.; Pollmanns, M.R.; Bündgens, L.; Wirtz, T.H.; Yagmur, E.; Hamesch, K.; Weiskirchen, R.; et al. Secreted Frizzled Related Protein 5 (SFRP5) Serum Levels Are Decreased in Critical Illness and Sepsis and Are Associated with Short-Term Mortality. Biomedicines 2023, 11, 313. https://doi.org/10.3390/biomedicines11020313
Hohlstein P, Brozat JF, Schuler J, Abu Jhaisha S, Pollmanns MR, Bündgens L, Wirtz TH, Yagmur E, Hamesch K, Weiskirchen R, et al. Secreted Frizzled Related Protein 5 (SFRP5) Serum Levels Are Decreased in Critical Illness and Sepsis and Are Associated with Short-Term Mortality. Biomedicines. 2023; 11(2):313. https://doi.org/10.3390/biomedicines11020313
Chicago/Turabian StyleHohlstein, Philipp, Jonathan F. Brozat, Julia Schuler, Samira Abu Jhaisha, Maike R. Pollmanns, Lukas Bündgens, Theresa H. Wirtz, Eray Yagmur, Karim Hamesch, Ralf Weiskirchen, and et al. 2023. "Secreted Frizzled Related Protein 5 (SFRP5) Serum Levels Are Decreased in Critical Illness and Sepsis and Are Associated with Short-Term Mortality" Biomedicines 11, no. 2: 313. https://doi.org/10.3390/biomedicines11020313