
Prolonged Door-to-Balloon Time Leads to Endothelial Glycocalyx Damage and Endothelial Dysfunction in Patients with ST-Elevation Myocardial Infarction
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cell Isolation and Culture
2.3. Atomic Force Microscopy
2.4. Enzyme-Linked Immunosorbent Assay
2.5. Nitric Oxide Product Measurements
2.6. Statistical Analysis
3. Results
3.1. Characteristics of STEMI Group
3.2. STEMI Leads to eGC Damage and Endothelial Dysfunction
3.3. D2B Time > 60 Min Leads to eGC Damage and Prolonged Hospitalization
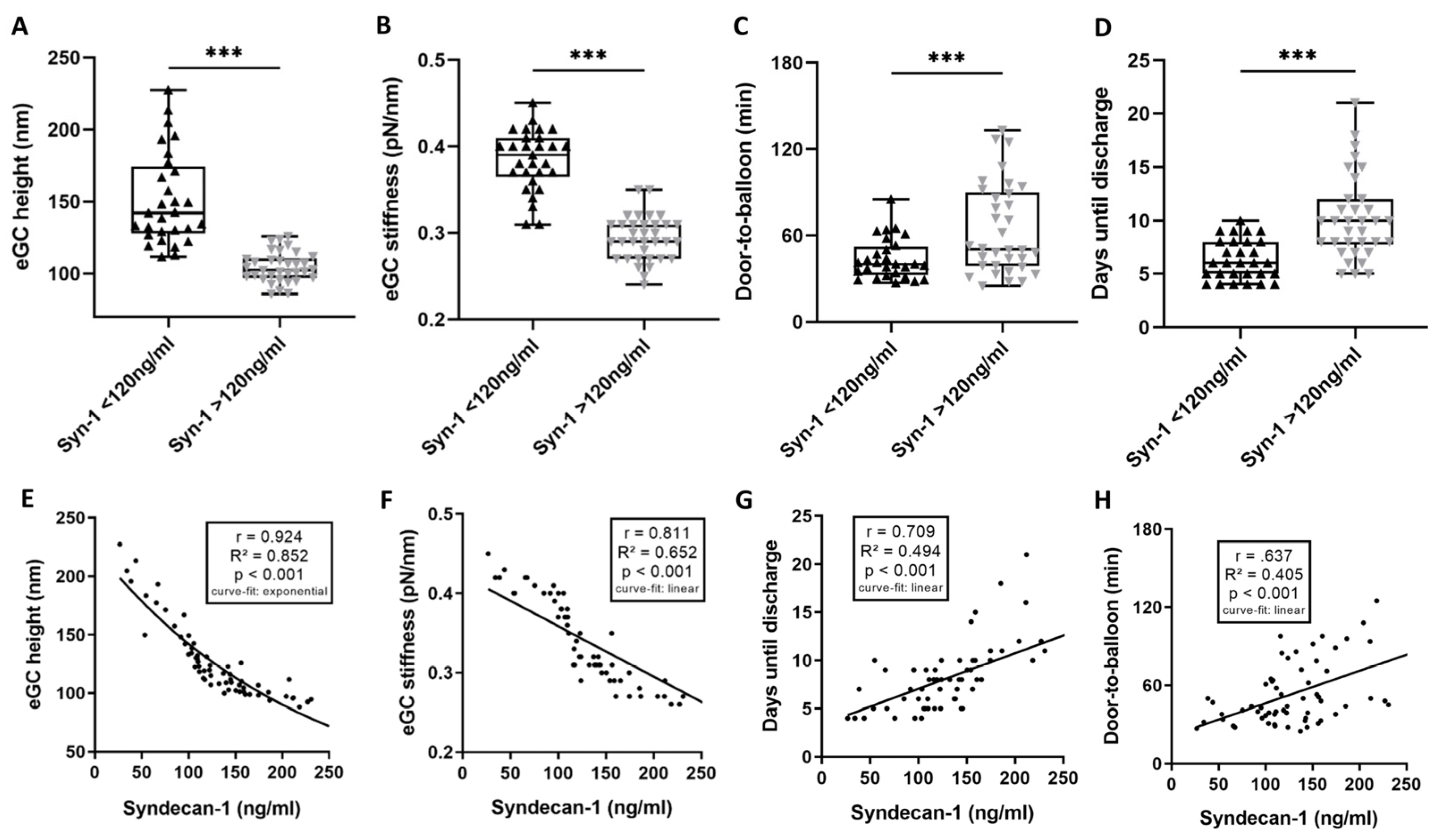
3.4. High Syndecan-1 Levels Are Associated with Unfavorable Outcomes for eGC and Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABOVE | group with a D2B time > 60 min |
| AFM | atomic force microscope |
| BELOW | group with a D2B time ≤ 60 min |
| BMI | body mass index |
| C3a | complement factor C3a |
| C5a | complement factor C5a |
| cGMP | cyclic guanosine monophosphate |
| CK | creatine kinase |
| CRP | c-reactive protein |
| CVRF | cardiovascular risk-factor |
| D2B | door-to-balloon time |
| ECLS | extracorporeal life support |
| ECMO | extracorporeal membrane oxygenation |
| eGC | endothelial glycocalyx |
| ELISA | enzyme-linked immunosorbent assay |
| ESC | European Society of Cardiology |
| FDC | force distance curve |
| HCl | hydrochloric acid |
| HIGH | group with syndecan-1 levels ≤ 120 ng/mL |
| HUVEC | human umbilical vein endothelial cells |
| I/R | ischemia-reperfusion |
| ICU | intensive care unit |
| IL | interleukin |
| IRI | ischemia-reperfusion injury |
| LDH | lactate dehydrogenase |
| LOW | group with syndecan-1 levels ≤ 120 ng/mL |
| LVEF | left ventricular ejection fraction |
| M | mean |
| MMP | matrix metalloproteinases |
| NO | nitric oxide |
| NOA-280i | Nitric Oxide Analyzer-280i |
| NOx | nitric oxide products |
| PCI | percutaneous coronary intervention |
| Pro-BNP II | pro-brain natriuretic peptide II |
| ROSC | return of spontaneous circulation |
| RR | Riva-Rocci, blood pressure |
| SD | standard deviation |
| STEMI | ST-elevation myocardial infarction |
| Syn-1 | syndecan-1 |
| TIMP | tissue inhibitor of matrix metalloproteinases |
| VSMC | vascular smooth muscle cells |
References
- Cosgun, Z.C.; Fels, B.; Kusche-Vihrog, K. Nanomechanics of the Endothelial Glycocalyx: From Structure to Function. Am. J. Pathol. 2020, 190, 732–741. [Google Scholar] [CrossRef]
- Abassi, Z.; Armaly, Z.; Heyman, S.N. Glycocalyx Degradation in Ischemia-Reperfusion Injury. Am. J. Pathol. 2020, 190, 752–767. [Google Scholar] [CrossRef] [PubMed]
- Ferdinandy, P.; Andreadou, I.; Baxter, G.F.; Bøtker, H.E.; Davidson, S.M.; Dobrev, D.; Gersh, B.J.; Heusch, G.; Lecour, S.; Ruiz-Meana, M.; et al. Interaction of Cardiovascular Nonmodifiable Risk Factors, Comorbidities and Comedications With Ischemia/Reperfusion Injury and Cardioprotection by Pharmacological Treatments and Ischemic Conditioning. Pharmacol. Rev. 2023, 75, 159–216. [Google Scholar] [CrossRef]
- Lee, S.-J.; Lee, C.-K.; Kang, S.; Park, I.; Kim, Y.H.; Kim, S.K.; Hong, S.P.; Bae, H.; He, Y.; Kubota, Y.; et al. Angiopoietin-2 exacerbates cardiac hypoxia and inflammation after myocardial infarction. J. Clin. Investig. 2018, 128, 5018–5033. [Google Scholar] [CrossRef] [PubMed]
- Rehm, M.; Bruegger, D.; Christ, F.; Conzen, P.; Thiel, M.; Jacob, M.; Chappell, D.; Stoeckelhuber, M.; Welsch, U.; Reichart, B.; et al. Shedding of the endothelial glycocalyx in patients undergoing major vascular surgery with global and regional ischemia. Circulation 2007, 116, 1896–1906. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, R.; Karkabi, B.; Goldenberg, I.; Shlomo, N.; Vorobeichik, D.; Zafrir, B.; Shiran, A.; Adawi, S.; Iakobishvili, Z.; Beigel, R.; et al. Avoidance of Coronary Angiography in High-Risk Patients With Acute Coronary Syndromes: The ACSIS Registry Findings. Cardiovasc. Revascularization. Med. Mol. Interv. 2020, 21, 1230–1236. [Google Scholar] [CrossRef]
- Pedersen, S.; Galatius, S.; Mogelvang, R.; Davidsen, U.; Galloe, A.; Abildstrom, S.Z.; Abildgaard, U.; Hansen, P.R.; Bech, J.; Iversen, A.; et al. Long-term prognosis in an ST-segment elevation myocardial infarction population treated with routine primary percutaneous coronary intervention: From clinical trial to real-life experience. Circ. Cardiovasc. Interv. 2009, 2, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Thiele, H.; Desch, S.; de Waha, S. Akuter Myokardinfarkt bei Patienten mit ST-Strecken-Hebungs-Infarkt. Herz 2017, 42, 728–738. [Google Scholar] [CrossRef]
- Konijnenberg, L.S.F.; Damman, P.; Duncker, D.J.; Kloner, R.A.; Nijveldt, R.; van Geuns, R.-J.M.; Berry, C.; Riksen, N.P.; Escaned, J.; van Royen, N. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc. Res. 2020, 116, 787–805. [Google Scholar] [CrossRef]
- Vahldieck, C.; Cianflone, E.; Fels, B.; Löning, S.; Depelmann, P.; Sabatino, J.; Salerno, N.; Karsten, C.M.; Torella, D.; Weil, J.; et al. Endothelial Glycocalyx and Cardiomyocyte Damage Is Prevented by Recombinant Syndecan-1 in Acute Myocardial Infarction. Am. J. Pathol. 2023, 193, 474–492. [Google Scholar] [CrossRef] [PubMed]
- Tkachenko, E.; Rhodes, J.M.; Simons, M. Syndecans: New kids on the signaling block. Circ. Res. 2005, 96, 488–500. [Google Scholar] [CrossRef] [PubMed]
- Wernly, B.; Fuernau, G.; Masyuk, M.; Muessig, J.M.; Pfeiler, S.; Bruno, R.R.; Desch, S.; Muench, P.; Lichtenauer, M.; Kelm, M.; et al. Syndecan-1 Predicts Outcome in Patients with ST-Segment Elevation Infarction Independent from Infarct-related Myocardial Injury. Sci. Rep. 2019, 9, 18367. [Google Scholar] [CrossRef]
- Rovas, A.; Sackarnd, J.; Rossaint, J.; Kampmeier, S.; Pavenstädt, H.; Vink, H.; Kümpers, P. Identification of novel sublingual parameters to analyze and diagnose microvascular dysfunction in sepsis: The NOSTRADAMUS study. Crit. Care Lond. Engl. 2021, 25, 112. [Google Scholar] [CrossRef] [PubMed]
- Fels, B.; Acharya, S.; Vahldieck, C.; Graf, T.; Käding, N.; Rupp, J.; Kusche-Vihrog, K. Mineralocorticoid receptor-antagonism prevents COVID-19-dependent glycocalyx damage. Pflug. Arch. 2022, 474, 1069–1076. [Google Scholar] [CrossRef]
- Killip, T.; Kimball, J.T. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am. J. Cardiol. 1967, 20, 457–464. [Google Scholar] [CrossRef]
- Wong, G.C.; Welsford, M.; Ainsworth, C.; Abuzeid, W.; Fordyce, C.B.; Greene, J.; Huynh, T.; Lambert, L.; Le May, M.; Lutchmedial, S.; et al. 2019 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Guidelines on the Acute Management of ST-Elevation Myocardial Infarction: Focused Update on Regionalization and Reperfusion. Can. J. Cardiol. 2019, 35, 107–132. [Google Scholar] [CrossRef]
- Bruegger, D.; Brettner, F.; Rossberg, I.; Nussbaum, C.; Kowalski, C.; Januszewska, K.; Becker, B.F.; Chappell, D. Acute degradation of the endothelial glycocalyx in infants undergoing cardiac surgical procedures. Ann. Thorac. Surg. 2015, 99, 926–931. [Google Scholar] [CrossRef]
- Lassus, J.; Tarvasmäki, T.; Tolppanen, H. Biomarkers in cardiogenic shock. Adv. Clin. Chem. 2022, 109, 31–73. [Google Scholar] [CrossRef]
- Seropian, I.M.; Sonnino, C.; Van Tassell, B.W.; Biasucci, L.M.; Abbate, A. Inflammatory markers in ST-elevation acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 382–395. [Google Scholar] [CrossRef]
- Wu, Y.; Pan, N.; An, Y.; Xu, M.; Tan, L.; Zhang, L. Diagnostic and Prognostic Biomarkers for Myocardial Infarction. Front. Cardiovasc. Med. 2021, 7, 617277. [Google Scholar] [CrossRef]
- Ostrowski, S.R.; Pedersen, S.H.; Jensen, J.S.; Mogelvang, R.; Johansson, P.I. Acute myocardial infarction is associated with endothelial glycocalyx and cell damage and a parallel increase in circulating catecholamines. Crit. Care Lond. Engl. 2013, 17, R32. [Google Scholar] [CrossRef] [PubMed]
- Pöss, J.; Fuernau, G.; Denks, D.; Desch, S.; Eitel, I.; de Waha, S.; Link, A.; Schuler, G.; Adams, V.; Böhm, M.; et al. Angiopoietin-2 in acute myocardial infarction complicated by cardiogenic shock--a biomarker substudy of the IABP-SHOCK II-Trial. Eur. J. Heart Fail. 2015, 17, 1152–1160. [Google Scholar] [CrossRef] [PubMed]
- Kusche-Vihrog, K.; Urbanova, K.; Blanqué, A.; Wilhelmi, M.; Schillers, H.; Kliche, K.; Pavenstädt, H.; Brand, E.; Oberleithner, H. C-reactive protein makes human endothelium stiff and tight. Hypertens. Dallas Tex 1979 2011, 57, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Prabhu, S.D.; Bansal, S.S. CD4+ T-lymphocytes exhibit biphasic kinetics post-myocardial infarction. Front. Cardiovasc. Med. 2022, 9, 992653. [Google Scholar] [CrossRef]
- Nordeng, J.; Schandiz, H.; Solheim, S.; Åkra, S.; Hoffman, P.; Roald, B.; Bendz, B.; Arnesen, H.; Helseth, R.; Seljeflot, I. TIMP-1 expression in coronary thrombi associate with myocardial injury in ST-elevation myocardial infarction patients. Coron. Artery Dis. 2022, 33, 446–455. [Google Scholar] [CrossRef]
- Bavia, L.; Lidani, K.C.F.; Andrade, F.A.; Sobrinho, M.I.A.H.; Nisihara, R.M.; de Messias-Reason, I.J. Complement activation in acute myocardial infarction: An early marker of inflammation and tissue injury? Immunol. Lett. 2018, 200, 18–25. [Google Scholar] [CrossRef]
- Fang, Z.; Li, X.; Liu, J.; Lee, H.; Salciccioli, L.; Lazar, J.; Zhang, M. The role of complement C3 in the outcome of regional myocardial infarction. Biochem. Biophys. Rep. 2023, 33, 101434. [Google Scholar] [CrossRef]
- Wolf, D.; Ley, K. Immunity and Inflammation in Atherosclerosis. Circ. Res. 2019, 124, 315–327. [Google Scholar] [CrossRef]
- Roy, P.; Orecchioni, M.; Ley, K. How the immune system shapes atherosclerosis: Roles of innate and adaptive immunity. Nat. Rev. Immunol. 2022, 22, 251–265. [Google Scholar] [CrossRef]
- Riehle, C.; Bauersachs, J. Key inflammatory mechanisms underlying heart failure. Herz 2019, 44, 96–106. [Google Scholar] [CrossRef]
- Tanindi, A.; Sahinarslan, A.; Elbeg, S.; Cemri, M. Relationship Between MMP-1, MMP-9, TIMP-1, IL-6 and Risk Factors, Clinical Presentation, Extent and Severity of Atherosclerotic Coronary Artery Disease. Open Cardiovasc. Med. J. 2011, 5, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Opstad, T.B.; Seljeflot, I.; Bøhmer, E.; Arnesen, H.; Halvorsen, S. MMP-9 and Its Regulators TIMP-1 and EMMPRIN in Patients with Acute ST-Elevation Myocardial Infarction: A NORDISTEMI Substudy. Cardiology 2018, 139, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Tiller, C.; Reindl, M.; Holzknecht, M.; Lechner, I.; Schwaiger, J.; Brenner, C.; Mayr, A.; Klug, G.; Bauer, A.; Metzler, B.; et al. Association of plasma interleukin-6 with infarct size, reperfusion injury, and adverse remodelling after ST-elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 113–123. [Google Scholar] [CrossRef]
- Cimmino, G.; Ragni, M.; Cirillo, P.; Petrillo, G.; Loffredo, F.; Chiariello, M.; Gresele, P.; Falcinelli, E.; Golino, P. C-reactive protein induces expression of matrix metalloproteinase-9: A possible link between inflammation and plaque rupture. Int. J. Cardiol. 2013, 168, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Fuernau, G.; Muench, P.; Desch, S.; Eitel, I.; Schuler, G.; Adams, V.; Figulla, H.R.; Thiele, H. Impairment of the endothelial glycocalyx in cardiogenic shock and its prognostic relevance. Shock Augusta Ga 2015, 43, 450–455. [Google Scholar] [CrossRef]
- Frydland, M.; Ostrowski, S.R.; Møller, J.E.; Hadziselimovic, E.; Holmvang, L.; Ravn, H.B.; Jensen, L.O.; Pettersson, A.S.; Kjaergaard, J.; Lindholm, M.G.; et al. Plasma Concentration of Biomarkers Reflecting Endothelial Cell- and Glycocalyx Damage are Increased in Patients With Suspected ST-Elevation Myocardial Infarction Complicated by Cardiogenic Shock. Shock Augusta Ga 2018, 50, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Serraino, G.F.; Jiritano, F.; Costa, D.; Ielapi, N.; Battaglia, D.; Bracale, U.M.; Mastroroberto, P.; Andreucci, M.; Serra, R. Metalloproteinases in Cardiac Surgery: A Systematic Review. Biomolecules 2023, 13, 113. [Google Scholar] [CrossRef]
- Fels, B.; Kusche-Vihrog, K. It takes more than two to tango: Mechanosignaling of the endothelial surface. Pflug. Arch. 2020, 472, 419–433. [Google Scholar] [CrossRef]
- Wang, Q.; Zuurbier, C.J.; Huhn, R.; Torregroza, C.; Hollmann, M.W.; Preckel, B.; Brom, C.E.v.D.; Weber, N.C. Pharmacological Cardioprotection against Ischemia Reperfusion Injury-The Search for a Clinical Effective Therapy. Cells 2023, 12, 1432. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma, C.; Vink, H.; van Haare, J.; Bekkers, S.C.; van Rooijen, B.D.; Backes, W.H.; Wildberger, J.E.; Crijns, H.J.; van Teeffelen, J.; Schalla, S. Non-invasive assessment of microvascular dysfunction in patients with microvascular angina. Int. J. Cardiol. 2017, 248, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Duranteau, J.; De Backer, D.; Donadello, K.; Shapiro, N.I.; Hutchings, S.D.; Rovas, A.; Legrand, M.; Harrois, A.; Ince, C. The future of intensive care: The study of the microcirculation will help to guide our therapies. Crit. Care Lond. Engl. 2023, 27, 190. [Google Scholar] [CrossRef] [PubMed]
- Rovas, A.; Lukasz, A.-H.; Vink, H.; Urban, M.; Sackarnd, J.; Pavenstädt, H.; Kümpers, P. Bedside analysis of the sublingual microvascular glycocalyx in the emergency room and intensive care unit—The GlycoNurse study. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 16. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | STEMI Group (n = 63) | |
|---|---|---|
| Age (years) | 64 (13) | |
| Hypertension (%) | 79.0 | |
| Diabetes (%) | 65.5 | |
| BMI (kg/m2) | 27.4 (4.5) | |
| Pos. family history (%) | 86.7 | |
| Hyperlipidemia (%) | 88.9 | |
| Smoking (%) | 62.3 | |
| Door-to-balloon time (min) | 55.5 (27.2) | |
| Puncture-to-balloon (min) | 11.7 (7.8) | |
| Door-to-needle (min) | 31.3 (16.3) | |
| Killip class (%) | I–II | 30.2 |
| III–IV | 69.9 | |
| LV EF (goups) | <40% | 15.6 |
| 40–50% | 44.4 | |
| >50% | 37.8 | |
| Days until discharge | 8.4 (3.7) | |
| Troponin max. (pg/mL) | [Ref.: 0–14] | 3053.0 (2653) |
| CK max. (U/L) | [Ref.: 20–200] | 1100.8 (1464) |
| LDH max. (U/L) | [Ref.: 135–225] | 446.6 (318.9) |
| Pro BNP II (pg/mL) | [Ref.: 0–121] | 1972.7 (2614) |
| Creatinine (mg/dL) | [Ref.: 0.7–1.2] | 2.19 (0.9) |
| Inflammatory markers | ||
| CRP max. (mg/L) | [Ref.: 0–5] | 45.4 (48.0) |
| Leukocytes (Gpt/L) | [Ref.: 4–9] | 17.41 (4.6) |
| eGC height (nm) | 125.9 (32.8) | |
| eGC stiffness (pN/nm) | 0.34 (0.05) | |
| Syndecan-1 (ng/mL) | 136.72 (69.3) | |
| Heparan sulfate (ng/mL) | 10.82 (8.6) | |
| Hyaluronic acid (µg/mL) | 182.9 (85.9) | |
| Nitric oxide (mM) | 6.39 (2.3) | |
| Angiopoetin-2 (ng/mL) | 18.5 (8.7) | |
| C3a (ng/mL) | 676.0 (343.4) | |
| C5a (ng/mL) | 36.2 (27.0) |
| Parameter | D2B ≤ 60 min (n = 42) | D2B > 60 min (n = 21) | p-Value | |
|---|---|---|---|---|
| Age (years) | 66 (11) | 63 (12) | 0.422 | |
| Door-to-balloon time (min) | 39.2 (21.7) | 88.0 (8.4) | <0.001 | |
| Puncture-to-balloon (min) | 9.8 (11.9) | 17.0 (4.6) | <0.01 | |
| Door-to-needle (min) | 25.1 (21.6) | 43.7 (7.4) | <0.001 | |
| Killip class | I–II | 31.0 | 28.6 | 0.066 |
| III–IV | 69.0 | 71.4 | ||
| Days until discharge | 7.9 (3.4) | 9.3 (3.8) | 0.162 | |
| Troponin max. (ng/mL) | 1.7 (2.2) | 3.5 (2.7) | <0.01 | |
| CK max. (U/L) | 800.5 (1350) | 1250.9 (1511) | 0.253 | |
| LDH max. (U/L) | 413.9 (275.4) | 462.5 (340.1) | 0.580 | |
| Pro BNP II (pg/mL) | 1752.7 (2993) | 2440.3 (1611) | 0.551 | |
| Creatinine (mg/dL) | 2.08 (1.4) | 2.39 (0.5) | 0.237 | |
| Inflammatory markers | ||||
| CRP max. (mg/L) | 40.9 (58.3) | 54.4 (42.1) | 0.296 | |
| Leukocytes (Gpt/L) | 11.54 (4.0) | 12.37 (5.7) | 0.634 | |
| eGC height (nm) | 124.9 (16.9) | 106.8 (34.9) | <0.001 | |
| eGC stiffness (pN/nm) | 0.35 (0.04) | 0.30 (0.05) | <0.001 | |
| Syndecan-1 (ng/mL) | 118.11 (88.1) | 173.95 (49.0) | 0.02 | |
| Heparan sulfate (ng/mL) | 7.99 (3.2) | 12.24 (10.1) | 0.065 | |
| Hyaluronic acid (µg/mL) | 174.9 (90.8) | 198.9 (83.3) | 0.300 | |
| Nitric oxide (mM) | 6.12 (3.6) | 4.88 (2.1) | <0.01 | |
| Angiopoetin-2 (ng/mL) | 17.7 (9.6) | 20.1 (8.3) | 0.302 | |
| C3a (ng/mL) | 643.0 (385.3) | 972.2 (262.5) | <0.001 | |
| C5a (ng/mL) | 38.3 (28.7) | 61.4 (22.7) | <0.001 | |
| Parameter | Syn-1 ≤ 120 ng/mL (n = 29) | Syn-1 > 120 ng/mL (n = 34) | p-Value | |
|---|---|---|---|---|
| Age (years) | 66 (13) | 63 (12) | 0.306 | |
| Door-to-balloon time (min) | 45.5 (17.1) | 63.9 (31.3) | <0.01 | |
| Puncture-to-balloon (min) | 9.5 (4.7) | 13.9 (9.7) | 0.033 | |
| Door-to-needle (min) | 30.2 (11.5) | 32.3 (19.6) | 0.627 | |
| Killip class | I–II | 31.0 | 29.4 | 0.290 |
| III–IV | 69.0 | 70.6 | ||
| Days until discharge | 6.3 | 10.2 | <0.001 | |
| Troponin max. (ng/mL) | 2.8 (3.0) | 3.3 (2.4) | 0.467 | |
| CK max. (U/L) | 239.0 (861.9) | 759.1 (1767) | <0.01 | |
| LDH max. (U/L) | 386.4 (265.1) | 497.7 (354.3) | 0.176 | |
| Pro BNP II (pg/mL) | 986.8 (1279) | 2882.9 (3210) | 0.069 | |
| Creatinine (mg/dL) | 2.43 (1.4) | 1.98 (0.2) | 0.067 | |
| Inflammatory markers | ||||
| CRP max. (mg/L) | 43.8 (39.7) | 46.8 (54.7) | 0.080 | |
| Leukocytes (Gpt/L) | 11.16 (3.7) | 12.24 (5.2) | 0.357 | |
| eGC height (nm) | 151.3 (32.0) | 104.4 (10.5) | <0.001 | |
| eGC stiffness (pN/nm) | 0.38 (0.03) | 0.29 (0.02) | <0.001 | |
| Syndecan-1 (ng/mL) | 88.93 (28.3) | 177.49 (67.9) | <0.001 | |
| Heparan sulfate (ng/mL) | 6.88 (10.8) | 11.67 (2.5) | <0.001 | |
| Hyaluronic acid (µg/mL) | 198.4 (107.2) | 169.7 (60.8) | 0.188 | |
| Nitric oxide (mM) | 6.14 (2.2) | 6.60 (2.3) | 0.468 | |
| Angiopoetin-2 (ng/mL) | 20.1 (9.1) | 17.2 (8.4) | 0.183 | |
| C3a (ng/mL) | 505.5 (144.6) | 963.6 (322.9) | <0.001 | |
| C5a (ng/mL) | 30.5 (11.6) | 59.1 (29.5) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vahldieck, C.; Fels, B.; Löning, S.; Nickel, L.; Weil, J.; Kusche-Vihrog, K. Prolonged Door-to-Balloon Time Leads to Endothelial Glycocalyx Damage and Endothelial Dysfunction in Patients with ST-Elevation Myocardial Infarction. Biomedicines 2023, 11, 2924. https://doi.org/10.3390/biomedicines11112924
Vahldieck C, Fels B, Löning S, Nickel L, Weil J, Kusche-Vihrog K. Prolonged Door-to-Balloon Time Leads to Endothelial Glycocalyx Damage and Endothelial Dysfunction in Patients with ST-Elevation Myocardial Infarction. Biomedicines. 2023; 11(11):2924. https://doi.org/10.3390/biomedicines11112924
Chicago/Turabian StyleVahldieck, Carl, Benedikt Fels, Samuel Löning, Laura Nickel, Joachim Weil, and Kristina Kusche-Vihrog. 2023. "Prolonged Door-to-Balloon Time Leads to Endothelial Glycocalyx Damage and Endothelial Dysfunction in Patients with ST-Elevation Myocardial Infarction" Biomedicines 11, no. 11: 2924. https://doi.org/10.3390/biomedicines11112924