
The Prognostic and Predictive Value of Genomic Assays in Guiding Adjuvant Breast Radiation Therapy
 ,
,
Abstract
:1. Breast Cancer and Breast Conservation Therapy
2. De-Escalation of Radiation Therapy Based on Clinical Factors in Breast Cancer
3. Genomic Profiling of Breast Cancers
4. Genome Expression Assays as Prognostic and Predictive Biomarkers for Adjuvant Systemic Therapy
5. Prognostic Genomic Assays and Adjuvant Radiation Therapy
6. The Potential for Predictive Genomic Assays to Guide Adjuvant Radiation Therapy
7. Summary and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Early Breast Cancer Trialists’ Collaborative, Group. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, M.; Collins, R.; Darby, S.; Davies, C.; Elphinstone, P.; Evans, V.; Godwin, J.; Gray, R.; Hicks, C.; James, S.; et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 366, 2087–2106. [Google Scholar] [PubMed]
- Blichert-Toft, M.; Nielsen, M.; Düring, M.; Møller, S.; Rank, F.; Overgaard, M.; Mouridsen, H.T. Long-term results of breast conserving surgery vs. mastectomy for early stage invasive breast cancer: 20-year follow-up of the Danish randomized DBCG-82TM protocol. Acta Oncol. 2008, 47, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.-H.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litière, S.; Werutsky, G.; Fentiman, I.S.; Rutgers, E.; Christiaens, M.-R.; Van Limbergen, E.; Baaijens, M.H.; Bogaerts, J.; Bartelink, H. Breast conserving therapy versus mastectomy for stage I–II breast cancer: 20 year follow-up of the EORTC 10801 phase 3 randomised trial. Lancet Oncol. 2012, 13, 412–419. [Google Scholar] [CrossRef]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [Green Version]
- Lingos, T.I.; Recht, A.; Vicini, F.; Abner, A.; Silver, B.; Harris, J.R. Radiation pneumonitis in breast cancer patients treated with conservative surgery and radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 355–360. [Google Scholar] [CrossRef]
- Back, M. Impact of radiation therapy on acute toxicity in breast conservation therapy for early breast cancer. Clin. Oncol. 2004, 16, 12–16. [Google Scholar] [CrossRef]
- Vicini, F.A.; Cecchini, R.S.; White, J.R.; Arthur, D.W.; Julian, T.B.; A Rabinovitch, R.; Kuske, R.R.; A Ganz, P.; Parda, D.S.; Scheier, M.F.; et al. Long-term primary results of accelerated partial breast irradiation after breast-conserving surgery for early-stage breast cancer: A randomised, phase 3, equivalence trial. Lancet 2019, 394, 2155–2164. [Google Scholar] [CrossRef]
- Meattini, I.; Marrazzo, L.; Saieva, C.; Desideri, I.; Scotti, V.; Simontacchi, G.; Bonomo, P.; Greto, D.; Mangoni, M.; Scoccianti, S.; et al. Accelerated Partial-Breast Irradiation Compared With Whole-Breast Irradiation for Early Breast Cancer: Long-Term Results of the Randomized Phase III APBI-IMRT-Florence. Trial. J. Clin. Oncol. 2020, 38, 4175–4183. [Google Scholar] [CrossRef] [PubMed]
- NSABP B-39, RTOG 0413: A Randomized Phase III Study of conventional whole breast irradiation versus partial breast irradiation for women with stage 0, I, or II breast cancer. Clin. Adv. Hematol. Oncol. 2006, 4, 719–721.
- Coles, C.E.; Griffin, C.L.; Kirby, A.M.; Titley, J.; Agrawal, R.K.; Alhasso, A.; Bhattacharya, I.S.; Brunt, A.M.; Ciurlionis, L.; Chan, C.; et al. Partial-breast radiotherapy after breast conservation surgery for patients with early breast cancer (UK IMPORT LOW trial): 5-year results from a multicentre, randomised, controlled, phase 3, non-inferiority trial. Lancet 2017, 390, 1048–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa, C.; Harris, E.E.; Leonardi, M.C.; Smith, B.D.; Taghian, A.G.; Thompson, A.M.; White, J.; Harris, J.R. Accelerated Partial Breast Irradiation: Executive summary for the update of an ASTRO Evidence-Based Consensus Statement. Pract. Radiat. Oncol. 2017, 7, 73–79. [Google Scholar] [CrossRef]
- Murray Brunt, A.; Haviland, J.S.; Wheatley, D.A.; Sydenham, M.A.; Alhasso, A.; Bloomfield, D.J.; Chan, C.; Churn, M.; Cleator, S.; Coles, C.E.; et al. Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial. Lancet 2020, 395, 1613–1626. [Google Scholar] [CrossRef]
- Brunt, A.M.; Haviland, J.; Sydenham, M.; Agrawal, R.K.; Algurafi, H.; Alhasso, A.; Barrett-Lee, P.; Bliss, P.; Bloomfield, D.; Bowen, J.; et al. Ten-Year Results of FAST: A Randomized Controlled Trial of 5-Fraction Whole-Breast Radiotherapy for Early Breast Cancer. J. Clin. Oncol. 2020, 38, 3261–3272. [Google Scholar] [CrossRef]
- Haque, W.; Verma, V.; Butler, E.B.; Teh, B.S. Omission of radiotherapy in elderly women with early stage metaplastic breast cancer. Breast 2018, 38, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Bazan, J.G.; Jhawar, S.R.; Stover, D.; Park, K.U.; Beyer, S.; Healy, E.; White, J.R. De-escalation of radiation therapy in patients with stage I, node-negative, HER2-positive breast cancer. NPJ Breast Cancer 2021, 7, 33. [Google Scholar] [CrossRef]
- Fisher, B.; Bryant, J.; Dignam, J.J.; Wickerham, D.L.; Mamounas, E.P.; Fisher, E.R.; Margolese, R.G.; Nesbitt, L.; Paik, S.; Pisansky, T.M.; et al. Tamoxifen, radiation therapy, or both for prevention of ipsilateral breast tumor recurrence after lumpectomy in women with invasive breast cancers of one centimeter or less. J. Clin. Oncol. 2002, 20, 4141–4149. [Google Scholar] [CrossRef]
- Pötter, R.; Gnant, M.; Kwasny, W.; Tausch, C.; Handl-Zeller, L.; Pakisch, B.; Taucher, S.; Hammer, J.; Luschin-Ebengreuth, G.; Schmid, M.; et al. Lumpectomy plus tamoxifen or anastrozole with or without whole breast irradiation in women with favorable early breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 334–340. [Google Scholar] [CrossRef]
- Malmström, P.; Holmberg, L.; Anderson, H.; Mattsson, J.; Jönsson, P.-E.; Tennvall-Nittby, L.; Balldin, G.; Lovén, L.; Svensson, J.-H.; Ingvar, C.; et al. Breast conservation surgery, with and without radiotherapy, in women with lymph node-negative breast cancer: A randomised clinical trial in a population with access to public mammography screening. Eur. J. Cancer 2003, 39, 1690–1697. [Google Scholar] [CrossRef] [PubMed]
- Killander, F.; Karlsson, P.; Anderson, H.; Mattsson, J.; Holmberg, E.; Lundstedt, D.; Malmström, P. No breast cancer subgroup can be spared postoperative radiotherapy after breast-conserving surgery. Fifteen-year results from the Swedish Breast Cancer Group randomised trial, SweBCG 91 RT. Eur. J. Cancer 2016, 67, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.R.; Anderson, S.; Tan-Chiu, E.; Fisher, B.; Eaton, L.; Wolmark, N. Fifteen-year prognostic discriminants for invasive breast carcinoma: National Surgical Adjuvant Breast and Bowel Project Protocol-06. Cancer 2001, 91, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.S.; Schnaper, L.A.; Bellon, J.R.; Cirrincione, C.T.; Berry, D.A.; Mc Cormick, B.; Muss, H.B.; Smith, B.L.; Hudis, C.A.; Winer, E.P.; et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: Long-term follow-up of CALGB 9343. J. Clin. Oncol. 2013, 31, 2382–2387. [Google Scholar] [CrossRef] [Green Version]
- Hughes, K.S.; Schnaper, L.A.; Berry, D.; Cirrincione, C.; McCormick, B.; Shank, B.; Wheeler, J.; Champion, L.A.; Smith, T.J.; Smith, B.L.; et al. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N. Engl. J. Med. 2004, 351, 971–977. [Google Scholar] [CrossRef] [Green Version]
- Kunkler, I.H.; Williams, L.J.; Jack, W.J.L.; A Cameron, D.; Dixon, J.M. Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME II): A randomised controlled trial. Lancet Oncol. 2015, 16, 266–273. [Google Scholar] [CrossRef]
- N.C.C.N Clinical Practice Guidelines in Oncology Breast Cancer. 2022. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419 (accessed on 7 November 2022).
- Fyles, A.; McCready, D.; Manchul, L.; Trudeau, M.; Merante, P.; Pintilie, M.; Weir, L.; Olivotto, I. A randomized trial of tamoxifen with or without breast radiation in women with early breast cancer 50 years of age and older. Radiother. Oncol. 2004, 73, S14. [Google Scholar]
- Liu, F.-F.; Shi, W.; Done, S.J.; Miller, N.; Pintilie, M.; Voduc, D.; Nielsen, T.O.; Nofech-Mozes, S.; Chang, M.C.; Whelan, T.J.; et al. Identification of a Low-Risk Luminal A Breast Cancer Cohort That May Not Benefit From Breast Radiotherapy. J. Clin. Oncol. 2015, 33, 2035–2040. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. A Prospective Cohort Study Evaluating Risk of Local Recurrence Following Breast Conserving Surgery and Endocrine Therapy in Low Risk Luminal A Breast Cancer (LUMINA). 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT01791829 (accessed on 10 November 2022).
- Whelan, T.J.; Smith, S.; Nielsen, T.O.; Parpia, S.; Fyles, A.W.; Bane, A.; Liu, F.-F.; Grimard, L.; Stevens, C.; Bowen, J.; et al. LUMINA: A prospective trial omitting radiotherapy (RT) following breast conserving surgery (BCS) in T1N0 luminal A breast cancer (BC). J. Clin. Oncol. 2022, 40, LBA501. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Sørlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Sørlie, T.; Tibshirani, R.; Parker, J.; Hastie, T.; Marron, J.S.; Nobel, A.; Deng, S.; Johnsen, H.; Pesich, R.; Geisler, S.; et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 2003, 100, 8418–8423. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, P.L.; Taghian, A.G.; Katz, M.S.; Niemierko, A.; Raad, R.F.A.; Boon, W.L.; Bellon, J.R.; Wong, J.S.; Smith, B.L.; Harris, J.R. Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. J. Clin. Oncol. 2008, 26, 2373–2378. [Google Scholar] [CrossRef] [PubMed]
- Arvold, N.D.; Taghian, A.G.; Niemierko, A.; Raad, R.F.A.; Sreedhara, M.; Nguyen, P.L.; Bellon, J.R.; Wong, J.S.; Smith, B.L.; Harris, J.R.; et al. Age, breast cancer subtype approximation, and local recurrence after breast-conserving therapy. J. Clin. Oncol. 2011, 29, 3885–3891. [Google Scholar] [CrossRef]
- Bane, A.L.; Whelan, T.; Pond, G.; Parpia, S.; Gohla, G.; Fyles, A.; Pignol, J.-P.; Pritchard, K.; Chambers, S.; Levine, M. Tumor factors predictive of response to hypofractionated radiotherapy in a randomized trial following breast conserving therapy. Ann. Oncol. 2014, 25, 992–998. [Google Scholar] [CrossRef]
- Voduc, K.D.; Cheang, M.C.U.; Tyldesley, S.; Gelmon, K.; Nielsen, T.O.; Kennecke, H. Breast cancer subtypes and the risk of local and regional relapse. J. Clin. Oncol. 2010, 28, 1684–1691. [Google Scholar] [CrossRef] [Green Version]
- Lowery, A.J.; Kell, M.R.; Glynn, R.W.; Kerin, M.J.; Sweeney, K.J. Locoregional recurrence after breast cancer surgery: A systematic review by receptor phenotype. Breast Cancer Res. Treat. 2012, 133, 831–841. [Google Scholar] [CrossRef]
- Carlson, J.J.; Roth, J.A. The impact of the Oncotype Dx breast cancer assay in clinical practice: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2013, 141, 13–22. [Google Scholar] [CrossRef]
- Harris, L.; Fritsche, H.; Mennel, R.; Norton, L.; Ravdin, P.; Taube, S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C. American society of clinical oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J. Clin. Oncol. 2007, 25, 5287–5312. [Google Scholar] [CrossRef] [Green Version]
- Harris, L.N.; Ismaila, N.; McShane, L.M.; Hayes, D.F. Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women With Early-Stage Invasive Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline Summary. J. Oncol. Pract. 2016, 12, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Raab, R.; Ismaila, N.; Andre, F.; Stearns, V.; Kalinsky, K. Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer: ASCO Guideline Update Q and A. Jco Oncol. Pract. 2022, 18, 646–648. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.; Ismaila, N.; Allison, K.H.; Barlow, W.E.; Collyar, D.E.; Damodaran, S.; Henry, N.L.; Jhaveri, K.; Kalinsky, K.; Kuderer, N.M.; et al. Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2022, 40, 1816–1837. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Paik, S. Development of the 21-gene assay and its application in clinical practice and clinical trials. J. Clin. Oncol. 2008, 26, 721–728. [Google Scholar] [CrossRef]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [Green Version]
- Paik, S.; Tang, G.; Shak, S.; Kim, C.; Baker, J.; Kim, W.; Cronin, M.; Baehner, F.L.; Watson, D.; Bryant, J.; et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor—positive breast cancer. J. Clin. Oncol. 2006, 24, 3726–3734. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Tang, G.; Fisher, B.; Paik, S.; Shak, S.; Costantino, J.P.; Watson, D.; Geyer, C.E.; Wickerham, D.L.; Wolmark, N. Association Between the 21-Gene Recurrence Score Assay and Risk of Locoregional Recurrence in Node-Negative, Estrogen Receptor—Positive Breast Cancer: Results From NSABP B-14 and NSABP B-20. J. Clin. Oncol. 2010, 28, 1677–1683. [Google Scholar] [CrossRef]
- Tang, G.; Shak, S.; Paik, S.; Anderson, S.; Costantino, J.P.; Geyer, C.E., Jr.; Mamounas, E.P.; Wickerham, D.L.; Wolmark, N. Comparison of the prognostic and predictive utilities of the 21-gene Recurrence Score assay and Adjuvant! for women with node-negative, ER-positive breast cancer: Results from NSABP B-14 and NSABP B-20. Breast Cancer Res. Treat. 2011, 127, 133–142. [Google Scholar] [CrossRef] [Green Version]
- Habel, L.A.; Shak, S.; Jacobs, M.K.; Capra, A.; Alexander, C.; Pho, M.; Baker, J.; Walker, M.; Watson, D.; Hackett, J.; et al. A population-based study of tumor gene expression and risk of breast cancer death among lymph node-negative patients. Breast Cancer Res. 2006, 8, R25. [Google Scholar] [CrossRef] [Green Version]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparano, J.A.; Gray, R.J.; Ravdin, P.M.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Goetz, M.P.; et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N. Engl. J. Med. 2019, 380, 2395–2405. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Barlow, W.E.; Shak, S.; Hortobagyi, G.N.; Livingston, R.B.; Yeh, I.-T.; Ravdin, P.; Bugarini, R.; Baehner, F.L.; Davidson, N.; et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: A retrospective analysis of a randomised trial. Lancet Oncol. 2010, 11, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albain, K.S.; Barlow, W.E.; Ravdin, P.M.; Farrar, W.B.; Burton, G.V.; Ketchel, S.J.; Cobau, C.D.; Levine, E.G.; Ingle, J.N.; Pritchard, K.I.; et al. Adjuvant chemotherapy and timing of tamoxifen in postmenopausal patients with endocrine-responsive, node-positive breast cancer: A phase 3, open-label, randomised controlled trial. Lancet 2009, 374, 2055–2063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalinsky, K.; Barlow, W.E.; Gralow, J.R.; Meric-Bernstam, F.; Albain, K.S.; Hayes, D.F.; Lin, N.U.; Perez, E.A.; Goldstein, L.J.; Chia, S.K.; et al. 21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer. N. Engl. J. Med. 2021, 385, 2336–2347. [Google Scholar] [CrossRef]
- Vijver, M.J.v.d.; He, Y.D.; Veer, L.J.v.; Dai, H.; Hart, A.A.M.; Voskuil, D.W.; Schreiber, G.J.; Peterse, J.L.; Roberts, C.; Marton, M.J.; et al. A gene-expression signature as a predictor of survival in breast cancer. N. Engl. J. Med. 2002, 347, 1999–2009. [Google Scholar] [CrossRef] [Green Version]
- Van’t Veer, L.J.; Dai, H.; Van De Vijver, M.J.; He, Y.D.; Hart, A.A.M.; Mao, M.; Peterse, H.L.; Van Der Kooy, K.; Marton, M.J.; Witteveen, A.T.; et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002, 415, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Buyse, M.; Loi, S.; Veer, L.V.; Viale, G.; Delorenzi, M.; Glas, A.; D’Assignies, M.S.; Bergh, J.; Lidereau, R.; Ellis, P.; et al. Validation and clinical utility of a 70-gene prognostic signature for women with node-negative breast cancer. J. Natl. Cancer Inst. 2006, 98, 1183–1192. [Google Scholar] [CrossRef] [Green Version]
- Piccart, M.; van’t Veer, L.J.; Poncet, C.; Cardozo, J.M.N.L.; Delaloge, S.; Pierga, J.-Y.; Vuylsteke, P.; Brain, E.; Vrijaldenhoven, S.; Neijenhuis, P.A.; et al. 70-gene signature as an aid for treatment decisions in early breast cancer: Updated results of the phase 3 randomised MINDACT trial with an exploratory analysis by age. Lancet Oncol. 2021, 22, 476–488. [Google Scholar]
- Cardoso, F.; van’t Veer, L.J.; Bogaerts, J.; Slaets, L.; Viale, G.; Delaloge, S.; Pierga, J.Y.; Brain, E.; Causeret, S.; Delorenzi, M.; et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. N. Engl. J. Med. 2016, 375, 717–729. [Google Scholar] [CrossRef] [Green Version]
- Cardozo, J.M.N.L.; Drukker, C.A.; Rutgers, E.J.T.; Schmidt, M.K.; Glas, A.M.; Witteveen, A.; Cardoso, F.; Piccart, M.; Esserman, L.J.; Poncet, C.; et al. Outcome of Patients With an Ultralow-Risk 70-Gene Signature in the MINDACT. Trial. J. Clin. Oncol. 2022, 40, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- Delahaye, L.J.M.J.; Drukker, C.A.; Dreezen, C.; Witteveen, A.; Chan, B.; Snel, M.; Beumer, I.J.; Bernards, R.; Audeh, M.W.; Veer, L.J.V.; et al. A breast cancer gene signature for indolent disease. Breast Cancer Res. Treat. 2017, 164, 461–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayasekera, J.; Schechter, C.B.; Sparano, J.A.; Jagsi, R.; White, J.; Chapman, J.-A.W.; Whelan, T.; Anderson, S.J.; Fyles, A.W.; Sauerbrei, W.; et al. Effects of Radiotherapy in Early-Stage, Low-Recurrence Risk, Hormone-Sensitive Breast Cancer. J. Natl. Cancer Inst. 2018, 110, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Woodward, W.A.; Barlow, W.E.; Jagsi, R.; Buchholz, T.; Shak, S.; Baehner, F.; Whelan, T.J.; Davidson, N.E.; Ingle, J.N.; King, T.A.; et al. Association Between 21-Gene Assay Recurrence Score and Locoregional Recurrence Rates in Patients With Node-Positive Breast Cancer. JAMA Oncol. 2020, 6, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Solin, L.J.; Gray, R.; Goldstein, L.J.; Recht, A.; Baehner, F.L.; Shak, S.; Badve, S.; Perez, E.A.; Shulman, L.N.; Martino, S.; et al. Prognostic value of biologic subtype and the 21-gene recurrence score relative to local recurrence after breast conservation treatment with radiation for early stage breast carcinoma: Results from the Eastern Cooperative Oncology Group E2197 study. Breast Cancer Res. Treat. 2012, 134, 683–692. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.H.; Horng, C.-F.; West, M.; Huang, E.; Pittman, J.; Tsou, M.-H.; Dressman, H.; Chen, C.-M.; Tsai, S.Y.; Jian, J.J.; et al. Genomic prediction of locoregional recurrence after mastectomy in breast cancer. J. Clin. Oncol. 2006, 24, 4594–4602. [Google Scholar] [CrossRef] [Green Version]
- Nuyten, D.S.A.; Kreike, B.; Hart, A.A.M.; Chi, J.-T.A.; Sneddon, J.B.; Wessels, L.F.A.; Peterse, H.J.; Bartelink, H.; Brown, P.O.; Chang, H.Y.; et al. Predicting a local recurrence after breast-conserving therapy by gene expression profiling. Breast Cancer Res. 2006, 8, R62. [Google Scholar] [CrossRef] [Green Version]
- Drukker, C.A.; Elias, S.G.L.; Nijenhuis, M.V.L.; Wesseling, J.; Bartelink, H.; Elkhuizen, P.; Fowble, B.; Whitworth, P.W.; Patel, R.R.; Snoo, F.A.d.; et al. Gene expression profiling to predict the risk of locoregional recurrence in breast cancer: A pooled analysis. Breast Cancer Res. Treat. 2015, 149, 599–613. [Google Scholar] [CrossRef] [Green Version]
- Mamounas, E.P.; Liu, Q.; Paik, S.; Baehner, F.L.; Tang, G.; Jeong, J.-H.; Kim, S.R.; Butler, S.M.; Jamshidian, F.; Cherbavaz, D.B.; et al. 21-Gene Recurrence Score and Locoregional Recurrence in Node-Positive/ER-Positive Breast Cancer Treated With Chemo-Endocrine Therapy. J. Natl. Cancer Inst. 2017, 109, djw259. [Google Scholar] [CrossRef]
- Fitzal, F.; Filipits, M.; Fesl, C.; Rudas, M.; Greil, R.; Balic, M.; Moinfar, F.; Herz, W.; Dubsky, P.; Bartsch, R.; et al. PAM-50 predicts local recurrence after breast cancer surgery in postmenopausal patients with ER+/HER2-disease: Results from 1204 patients in the randomized ABCSG-8 trial. Br. J. Surg. 2021, 108, 308–314. [Google Scholar] [CrossRef]
- Wallden, B.; Storhoff, J.; Nielsen, T.; Dowidar, N.; Schaper, C.; Ferree, S.; Liu, S.; Leung, S.; Geiss, G.; Snider, J.; et al. Development and verification of the PAM50-based Prosigna breast cancer gene signature assay. BMC Med. Genom. 2015, 8, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnant, M.; Filipits, M.; Greil, R.; Stoeger, H.; Rudas, M.; Bago-Horvath, Z.; Mlineritsch, B.; Kwasny, W.; Knauer, M.; Singer, C.; et al. Predicting distant recurrence in receptor-positive breast cancer patients with limited clinicopathological risk: Using the PAM50 Risk of Recurrence score in 1478 postmenopausal patients of the ABCSG-8 trial treated with adjuvant endocrine therapy alone. Ann. Oncol. 2014, 25, 339–345. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. The IDEA Study (Individualized Decisions for Endocrine Therapy Alone). 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT02400190 (accessed on 10 November 2022).
- ClinicalTrials.gov. The PRECISION Trial (Profiling Early Breast Cancer for Radiotherapy Omission): A Phase II Study of Breast-Conserving Surgery Without Adjuvant Radiotherapy for Favorable-Risk Breast Cancer. 2022. Available online: https://www.clinicaltrials.gov/ct2/show/NCT02653755 (accessed on 10 November 2022).
- ClinicalTrials.gov. De-Escalation of Breast Radiation Trial for Hormone Sensitive, HER-2 Negative, Oncotype Recurrence Score Less Than or Equal to 18 Breast Cancer (DEBRA). 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT04852887 (accessed on 10 November 2022).
- ClinicalTrials.gov. Regional Radiotherapy in Biomarker Low-Risk Node Positive and T3N0 Breast Cancer (TAILOR RT). 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT03488693 (accessed on 10 November 2022).
- ClinicalTrials.gov. EXamining PErsonalised Radiation Therapy for Low-Risk Early Breast Cancer. 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT02889874 (accessed on 10 November 2022).
- He, L.; Lv, Y.; Song, Y.; Zhang, B. The prognosis comparison of different molecular subtypes of breast tumors after radiotherapy and the intrinsic reasons for their distinct radiosensitivity. Cancer Manag. Res. 2019, 11, 5765–5775. [Google Scholar] [CrossRef] [PubMed]
- Tramm, T.; Kyndi, M.; Myhre, S.; Nord, S.; Alsner, J.; Sørensen, F.B.; Sørlie, T.; Overgaard, J. Relationship between the prognostic and predictive value of the intrinsic subtypes and a validated gene profile predictive of loco-regional control and benefit from post-mastectomy radiotherapy in patients with high-risk breast cancer. Acta Oncol. 2014, 53, 1337–1346. [Google Scholar] [CrossRef]
- Speers, C.; Zhao, S.; Liu, M.; Bartelink, H.; Pierce, L.J.; Feng, F.Y. Development and Validation of a Novel Radiosensitivity Signature in Human Breast Cancer. Clin. Cancer Res. 2015, 21, 3667–3677. [Google Scholar] [CrossRef] [Green Version]
- Niméus-Malmström, E.; Krogh, M.; Malmström, P.; Strand, C.; Fredriksson, I.; Karlsson, P.; Nordenskjöld, B.; Stål, O.; Östberg, G.; Peterson, C.; et al. Gene expression profiling in primary breast cancer distinguishes patients developing local recurrence after breast-conservation surgery, with or without postoperative radiotherapy. Breast Cancer Res. 2008, 10, R34. [Google Scholar] [CrossRef] [Green Version]
- Tramm, T.; Mohammed, H.; Myhre, S.; Kyndi, M.; Alsner, J.; Børresen-Dale, A.-L.; Sørlie, T.; Frigessi, A.; Overgaard, J. Development and Validation of a Gene Profile Predicting Benefit of Postmastectomy Radiotherapy in Patients with High-Risk Breast Cancer: A Study of Gene Expression in the DBCG82bc Cohort. Clin. Cancer Res. 2014, 20, 5272–5280. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, M.; Chang, S.L.; Fishbane, N.; Davicioni, E.; Zhao, S.G.; Hartman, L.; Holmberg, E.; Feng, F.Y.; Speers, C.W.; Pierce, L.J.; et al. Clinicogenomic Radiotherapy Classifier Predicting the Need for Intensified Locoregional Treatment After Breast-Conserving Surgery for Early-Stage Breast Cancer. J. Clin. Oncol. 2019, 37, 3340–3349. [Google Scholar] [CrossRef]
- Eschrich, S.A.; Fulp, W.J.; Pawitan, Y.; Foekens, J.A.; Smid, M.; Martens, J.W.; Echevarria, M.; Kamath, V.; Lee, J.-H.; Harris, E.E.; et al. Validation of a radiosensitivity molecular signature in breast cancer. Clin. Cancer Res. 2012, 18, 5134–5143. [Google Scholar] [CrossRef] [Green Version]
- Torres-Roca, J.F.; Eschrich, S.; Zhao, H.; Bloom, G.; Sung, J.; McCarthy, S.; Cantor, A.B.; Scuto, A.; Li, C.; Zhang, S.; et al. Prediction of radiation sensitivity using a gene expression classifier. Cancer Res. 2005, 65, 7169–7176. [Google Scholar] [CrossRef] [Green Version]
- Torres-Roca, J.F.; Fulp, W.J.; Caudell, J.J.; Servant, N.; Bollet, M.A.; van de Vijver, M.; Naghavi, A.O.; Harris, E.E.; Eschrich, S.A. Integration of a Radiosensitivity Molecular Signature Into the Assessment of Local Recurrence Risk in Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 631–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschrich, S.; Zhang, H.; Zhao, H.; Boulware, D.; Lee, J.-H.; Bloom, G.; Torres-Roca, J.F. Systems Biology Modeling of the Radiation Sensitivity Network: A Biomarker Discovery Platform. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 497–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschrich, S.A.; Pramana, J.; Zhang, H.; Zhao, H.; Boulware, D.; Lee, J.-H.; Bloom, G.; Rocha-Lima, C.; Kelley, S.; Calvin, D.P.; et al. A Gene Expression Model of Intrinsic Tumor Radiosensitivity: Prediction of Response and Prognosis after Chemoradiation. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.G.; Berglund, A.; Schell, M.J.; Mihaylov, I.; Fulp, W.J.; Yue, B.; Welsh, E.; Caudell, J.J.; Ahmed, K.; Strom, T.S.; et al. A genome-based model for adjusting radiotherapy dose (GARD): A retrospective, cohort-based study. Lancet Oncol. 2017, 18, 202–211. [Google Scholar] [CrossRef]
- Shen, J.; Yan, D.; Bai, L.; Geng, R.; Zhao, X.; Li, H.; Dong, Y.; Cao, J.; Tang, Z.; Liu, S.-B. An 11-Gene Signature Based on Treatment Responsiveness Predicts Radiation Therapy Survival Benefit Among Breast Cancer Patients. Front. Oncol. 2022, 11, 5565. [Google Scholar] [CrossRef]
- Cui, Y.; Li, B.; Pollom, E.L.; Horst, K.C.; Li, R. Integrating Radiosensitivity and Immune Gene Signatures for Predicting Benefit of Radiotherapy in Breast Cancer. Clin. Cancer Res. 2018, 24, 4754–4762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrieling, C.; Werkhoven, E.v.; Maingon, P.; Poortmans, P.; Weltens, C.; Fourquet, A.; Schinagl, D.; Oei, B.; Rodenhuis, C.C.; Horior, J.-C.; et al. Prognostic Factors for Local Control in Breast Cancer After Long-term Follow-up in the EORTC Boost vs No Boost Trial A Randomized Clinical Trial. JAMA Oncol. 2017, 3, 42–48. [Google Scholar] [CrossRef]


{kind=link}
| Microarray | Number of Genes | Genes | Classification | Reference |
|---|---|---|---|---|
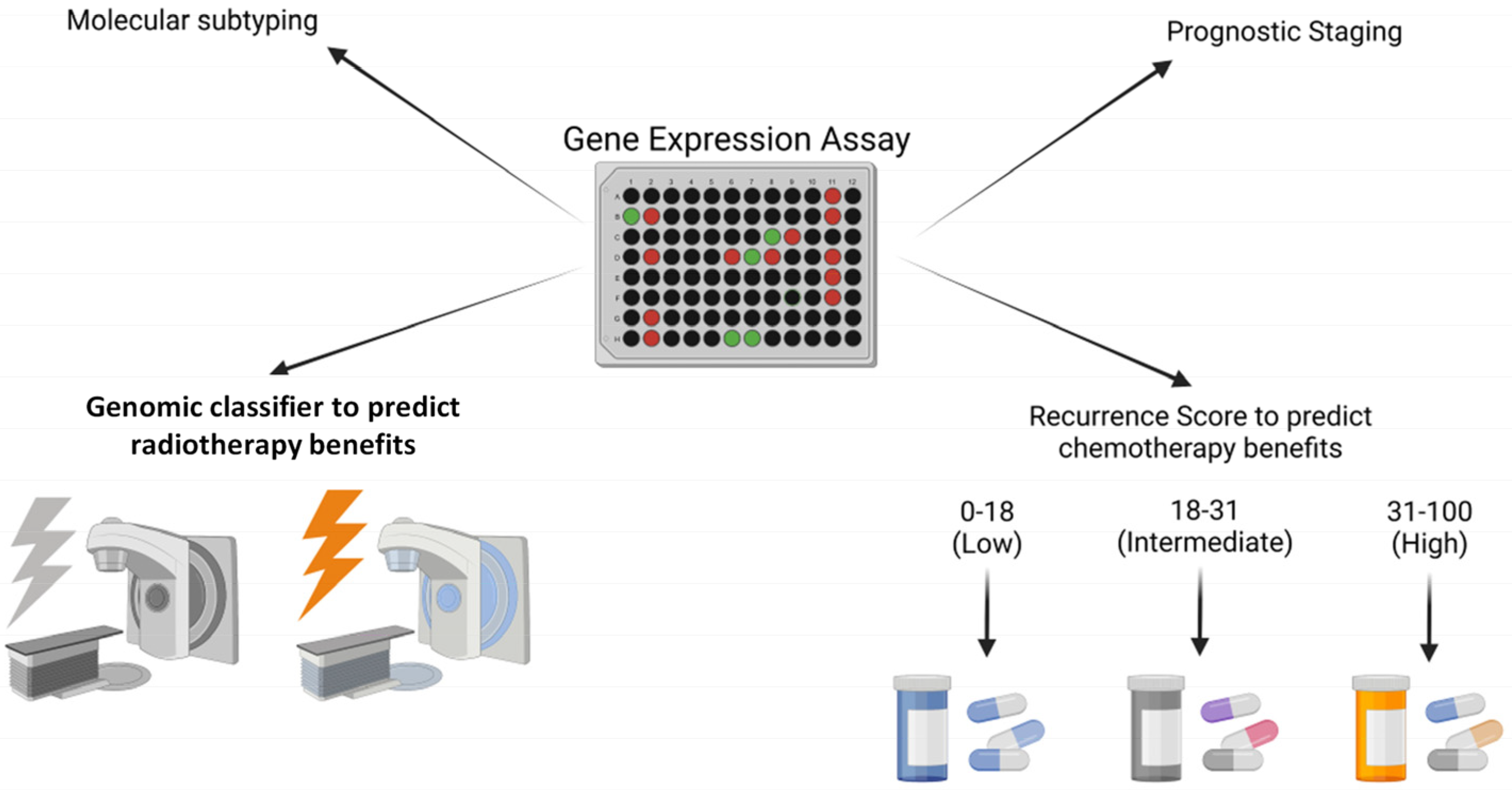
| OncotypeDx | 21 genes | 16 cancer-related genes associated with proliferation, invasion, and estrogen signaling as well as 5 reference genes | Generates “Recurrence Score” (RS), from 0–100 which stratifies patients into low (0–18), intermediate (18–31), and high (31–100) risk of distant reccurence. | [43] |
| Mammoprint | 70 genes | Genes associated with cell cycle, invasion, metastases and signal transduction | Classifies breast cancer patients into “poor prognosis” or “good prognosis”. Calculates MammaPrint Index (MPI) to stratify Low or High risk of reccurence. | [54,55] |
| PAM 50 | 50 genes | 50 discriminator genes + 8 controls. These genes identify the intrinsic breast cancer subtypes by indentifying the underlying biology associated with ER and HER2 pathways, and proliferation genes and markers of the basal phenotype. | Calculates a “risk-of-recurrence” (ROR) score, 0–100 which classifies low (0–40), intermediate (41–60), or high (61–100) risk for node-negative cancers. | [68,69,70] |
| Prospective Clinical Trials | Enrollment Criteria | Aims | Reference |
|---|---|---|---|
| LUMINA | Grade 1–2 invasive breast cancers of luminal A subtype (defined as: ER ≥ 1%, PR > 20%, HER2 negative and Ki67 ≤ 13.25%) in women > 55 yo | To evaluate patients who have low risk of local reccurence following breast conservation surgery and endocrine therapy alone who may be candidates for radiation omission. | [26,27] |
| IDEA | ER+ invasive breast cancers with RS ≤ 18 who plan to receive endocrine therapy in post-menopausal women | To evaluate locoregional recurrence rates in low risk women via considering tumor biology including OncotypeDx, in which radiation therapy can be omitted after breast conservation surgery. | [71] |
| PRECISION | ER+ early stage breast cancers < 2 cm with a low risk PAM-50-based ROR in women > 50 yo | To evaluate locoregional recurrence rates in patients omitting radiation treatment after lumpectomy. | [72] |
| DEBRA | ER+/Her-2 negative early stage breast cancers with RS ≤ 18 in women age 50–69 yo | To evaluate omission of breast radiation after breast conservation surgery and endocrine therapy. | [73] |
| EXPERT | ER+/Her-2 negative early stage breast cancers with PAM-50 ROR < 60 in women ≥ 50 yo | To evaluate the omission of breast radiation therapy compared to obseravation after breast conserving surgery and endocrine therapy. | [75] |
| TAILOR-RT | ER+/Her2-negative biomarker low risk breast cancers (defined as RS ≤ 25) with low lymph node burden (1–3+ lymph nodes) | To evaluate the effects on low risk breast cancer patients after ommission or treatment of regional nodal radiation. | [74] |
| Microarray | Number of Genes | Genes | Classification | Reference |
|---|---|---|---|---|
| Speers et al. | 51 genes | Enriched with genes associated with cell cycle arrest and DNA damage response | Identify women at an increased risk of local recurrence most likely to benefit from radiation | [78] |
| Danish Breast Cancer Cooperative Group (DBCG82bc) | 7 genes | HLA-DQA, RGS1, DNALI1, hCG2023290, IGKC, OR8G2, and ADH1B. Genes involving immune system, protein signalling, and metabolism enzymes | Identified patients with “high LRR risk” in which PMRT significantly reduced the risk of LR and “low LRR risk” group in which PMRT showed no additional reduction in LR rate and the response to radiation was independent of intrinsic molecular subtype | [77,80] |
| Adjuvant Radiotherapy Intensification Classifier (ARTIC) | 27 genes | Genes related to cell proliferation, cell cycle and kinase activity as well as patient age | A gene classifier for radiation sensitivity in patients with high-risk node negative early stage breast cancers was developed using three publicly available cohorts | [81] |
| RSI radiosensitivity index | 10 genes | Related to DNA damage response, histone deacetylation, cell cycle, apoptosis and proliferation | Predict clinical outcomes and benefit from radiation therapy among several cancer types, including breast cancer | [82,83,84,85,86] |
| Shen et al. | 11 genes | Genes that look at the tumor immune micro-environment | Stratify tumors based on response to radiation therapy and the tumor immune microenvironment | [88] |
| Cui et al | 33 radiation-related genes | Tumor microenvironment genes such as tumor-associated antigens on the major histocompatibility complex (MHC) molecules. | Stratification of patients by predicting benefits from radiotherapy. | [89] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beyer, S.J.; Tallman, M.; Jhawar, S.R.; White, J.R.; Bazan, J.G. The Prognostic and Predictive Value of Genomic Assays in Guiding Adjuvant Breast Radiation Therapy. Biomedicines 2023, 11, 98. https://doi.org/10.3390/biomedicines11010098
Beyer SJ, Tallman M, Jhawar SR, White JR, Bazan JG. The Prognostic and Predictive Value of Genomic Assays in Guiding Adjuvant Breast Radiation Therapy. Biomedicines. 2023; 11(1):98. https://doi.org/10.3390/biomedicines11010098
Chicago/Turabian StyleBeyer, Sasha J., Miranda Tallman, Sachin R. Jhawar, Julia R. White, and Jose G. Bazan. 2023. "The Prognostic and Predictive Value of Genomic Assays in Guiding Adjuvant Breast Radiation Therapy" Biomedicines 11, no. 1: 98. https://doi.org/10.3390/biomedicines11010098