
Association between Immunosuppressive Therapy Utilized in the Treatment of Autoimmune Disease or Transplant and Cancer Progression

Abstract
:1. Introduction
2. Autoimmunity and Cancer Correlation
3. Immunodeficiency and Cancer Correlation
4. Immunosuppression in Autoimmune Disease and Cancer Correlation
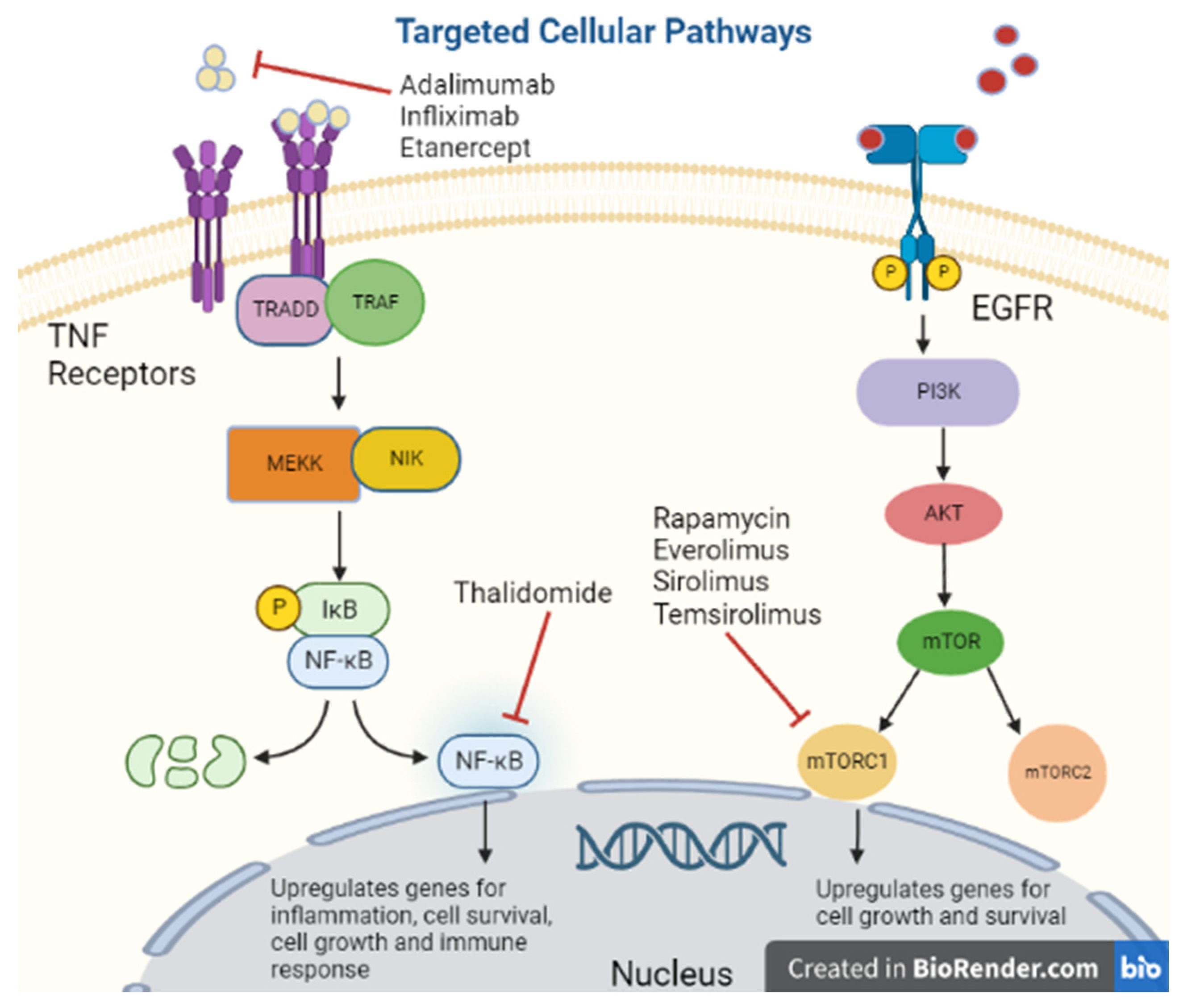
Tumor Necrosis Factor-Alpha Inhibitors
5. Transplant Immunosuppression and Cancer Correlation
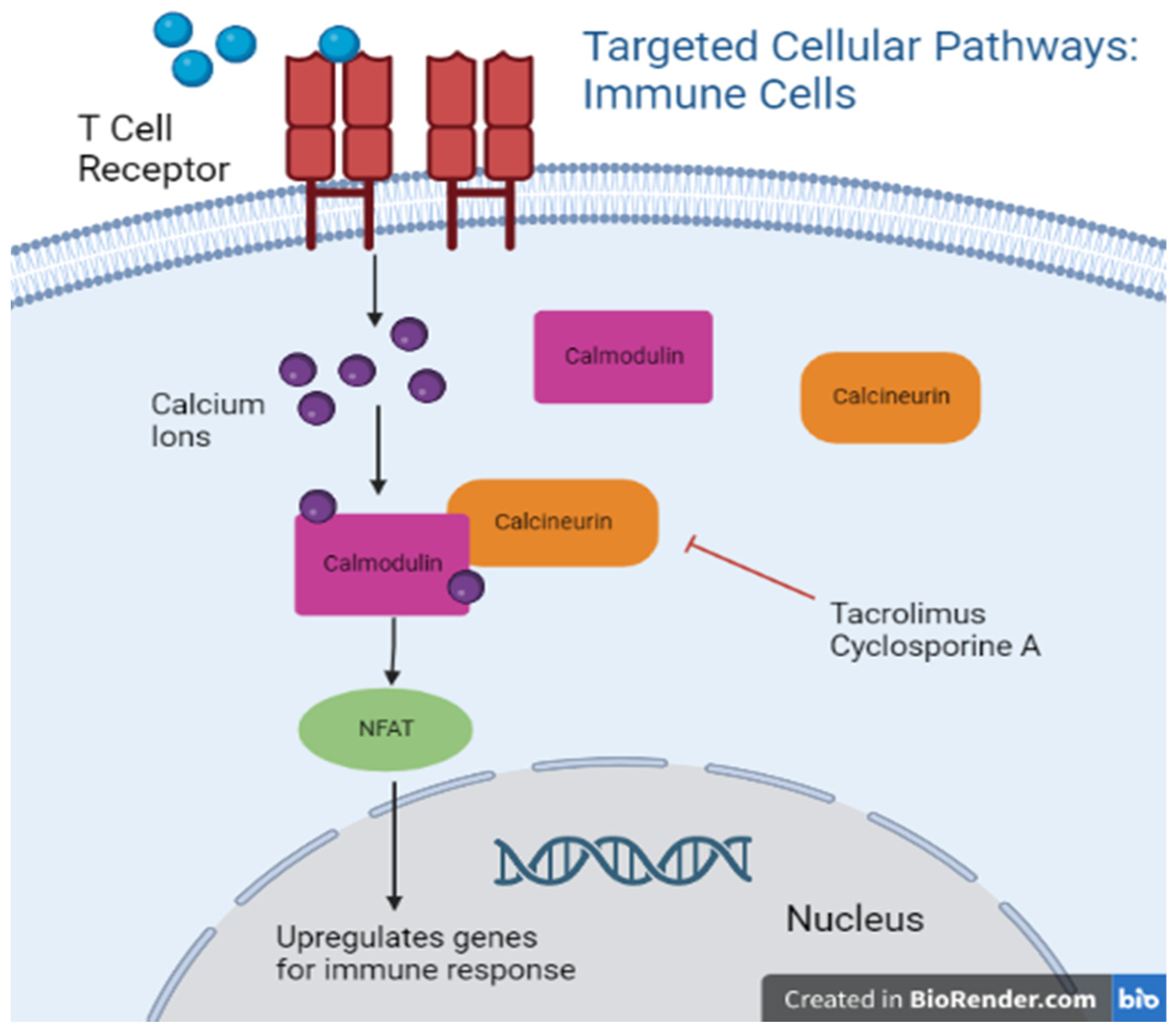
5.1. Calcineurin Inhibitors
5.2. mTOR Inhibitors
6. Immunosuppression in Both Autoimmune Disease/Transplant and Cancer Correlation
Purine Synthesis Antagonists
7. Immune Checkpoint Inhibitors in Transplant and Autoimmune Disease
8. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Burnet, F.M. The Concept of Immunological Surveillance. Prog. Tumor Res. 1970, 13, 1–27. [Google Scholar] [CrossRef]
- Thomas, L.; Lawrence, H. Cellular and Humoral Aspects of the Hypersensitive States; Hoeber-Harper: New York, NY, USA, 1959; pp. 529–532.
- Thomas, L. On immunosurveillance in human cancer. Yale J. Biol. Med. 1982, 55, 329. [Google Scholar]
- Nozawa, M.; Weil, R.; Mcintosh, R.; Reemtsma, K. Is immunological surveillance not a cell-mediated immune function? Transplantation 1974, 17, 135–139. [Google Scholar] [CrossRef]
- Stutman, O. Chemical carcinogenesis in nude mice: Comparison between nude mice from homozygous matings and heterozygous matings and effect of age and carcinogen dose. J. Natl. Cancer Inst. 1979, 62, 353–358. [Google Scholar] [PubMed]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The Immunobiology of Cancer Immunosurveillance and Immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankaran, V.; Ikeda, H.; Bruce, A.T.; White, J.M.; Swanson, P.E.; Old, L.J.; Schreiber, R.D. IFNγ and lymphocytes prevent primary tumour development and shape tumour immunogenicity. Nature 2001, 410, 1107–1111. [Google Scholar] [CrossRef]
- Li, C.; Chen, Z. Autoimmunity as an Etiological Factor of Cancer: The Transformative Potential of Chronic Type 2 Inflammation. Front. Cell Dev. Biol. 2021, 9, 664305. [Google Scholar] [CrossRef]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Anderson, W.F.; Rabkin, C.S.; Turner, N.; Fraumeni, J.F., Jr.; Rosenberg, P.S.; Camargo, M.C. The Changing Face of Noncardia Gastric Cancer Incidence Among US Non-Hispanic Whites. J. Natl. Cancer Inst. 2018, 110, 608–615. [Google Scholar] [CrossRef] [Green Version]
- Zityogel, L.; Perreault, C.; Finn, O.J. Beneficial autoimmunity improves cancer prognosis. Nat. Rev. Clin. Oncol. 2021, 18, 591–602. [Google Scholar] [CrossRef]
- Khan, S.; Pruitt, S.; Xuan, L. Prevalence of autoimmune disease among patients with lung cancer: Implications for immunotherapy treatment options. JAMA Oncol. 2016, 2, 1507–1508. [Google Scholar] [CrossRef]
- Jacob, S.; Rahbari, K.; Tegtmeyer, K. Lung Cancer Survival in Patients with Autoimmune Disease. JAMA Netw. Open 2020, 3, e2029917. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.; Ellershaw, J. Anti-Hu antibodies may indicate a positive response to chemotherapy in paraneoplastic syndrome secondary to small cell lung cancer. Palliat. Med. 2003, 17, 638–639. [Google Scholar] [CrossRef] [PubMed]
- Manley, G.T.; Smitt, P.S.; Dalmau, J.; Posner, J.B. Hu antigens: Reactivity with hu antibodies, tumor expression, and major immunogenic sites. Ann. Neurol. 1995, 38, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Marafini, I.; Monteleone, G.; Stolfi, C. Association Between Celiac Disease and Cancer. Int. J. Mol. Sci. 2020, 21, 4155. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.A.; Cooper, D.S.; Levy, E.G.; Ladenson, P.W.; Braverman, L.E.; Daniels, G.; Greenspan, F.S.; McDougall, I.R.; Nikolai, T.F. Treatment guidelines for patients with hyperthyroidism and hypothyroidism. JAMA 1995, 273, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Rotondi, M.; Groppelli, G.; Croce, L.; Latrofa, F.; Ancona, G.; Coperchini, F.; Pasquali, D.; Cappelli, C.; Fugazza, A.; Guazzoni, V.; et al. Patients with chronic autoimmune thyroiditis are not at higher risk for developing clinically overt thyroid cancer: A 10-year follow-up study. Eur. J. Endocrinol. 2020, 183, 317–323. [Google Scholar] [CrossRef]
- Chen, Y.K.; Lin, C.L.; Cheng, F.T.F.; Sung, F.C.; Kao, C.H. Cancer risk in patients with Hashimoto’s thyroiditis: A nationwide cohort study. Br. J. Cancer 2013, 109, 2496–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manger, B.; Schett, G. Paraneoplastic syndromes in rheumatology. Nat. Rev. Rheumatol. 2014, 10, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Soomro, Z.; Youssef, M.; Yust-Katz, S.; Jalali, A. Paraneoplastic Syndromes in Small Cell Lung Cancer. J. Thorac. Dis. 2020, 12, 6253. Available online: https://jtd.amegroups.com/article/view/38423 (accessed on 11 October 2022). [CrossRef]
- Mayor, P.C.; Eng, K.H.; Singel, K.L.; Abrams, S.I.; Odunsi, K.; Moysich, K.B.; Fuleihan, R.; Garabedian, E.; Lugar, P.; Ochs, H.D.; et al. Cancer in primary immunodeficiency diseases: Cancer incidence in the United States Immune Deficiency Network Registry. J. Allergy Clin. Immunol. 2018, 141, 1028–1035. [Google Scholar] [CrossRef]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grulich, A.E.; Van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekara, S. The treatment strategies of autoimmune disease may need a different approach from conventional protocol: A review. Indian J. Pharm. 2012, 44, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.; Diamond, B. Autoimmune Diseases. N. Engl. J. Med. 2001, 345, 340–350. [Google Scholar] [CrossRef]
- Marmont, A.M. New horizons in the treatment of autoimmune diseases: Immunoablation and stem cell transplantation. Annu. Rev. Med. 2000, 51, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Wallach, D.; Varfolomeev, E.E.; Malinin, N.L.; Goltsev, Y.V.; Kovalenko, A.V.; Boldin, M.P. Tumor necrosis factor receptor and Fas signaling mechanisms. Annu. Rev. Immunol. 1999, 17, 331–367. [Google Scholar] [CrossRef]
- Mocellin, S.; Riccardo Rossi, C.; Pilati, P.; Nitti, D. Tumor necrosis factor, cancer and anticancer therapy. Cytokine Growth Factor Rev. 2004, 16, 35–53. [Google Scholar] [CrossRef] [PubMed]
- Fajardo, L.; Kwan, H.; Kowalski, J.; Prionas, S. Dual role of tumor necrosis factor-alpha in angiogenesis. Am. J. Pathol. 1992, 140, 539–544. [Google Scholar]
- Overall, C.; Kleifeld, O. Tumour microenvironment-opinion: Validating matrix metalloproteinases as drug targets and antitargets for cancer therapy. Nat. Rev. Cancer 2006, 6, 227–239. [Google Scholar] [CrossRef]
- Kumar, S.; Witzig, T.E.; Rajkumar, S.V. Thalidomide as an anticancer agent. J. Cell. Mol. Med. 2022, 6, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.K. Properties of Thalidomide and its analogues: Implications for anticancer therapy. AAPS J. 2005, 7, E14–E15. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Mehta, J.; Desikan, R.; Ayers, D.; Roberson, P.; Eddlemon, P.; Munshi, N.; Anaissie, E.; Wilson, C.; Dhodapkar, M.; et al. Antitumor Activity of Thalidomide in Refractory Multiple Myeloma. N. Engl. J. Med. 1999, 341, 1565–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keystone, E. Advances in targeted therapy: Safety of biological agents. Ann. Rheum. Dis. 2003, 62 (Suppl. 2), ii34–ii36. [Google Scholar] [CrossRef] [Green Version]
- Askling, J.; Fored, C.M.; Baecklund, E.; Brandt, L.; Backlin, C.; Ekbom, A.; Sundström, C.; Bertilsson, L.; Cöster, L.; Geborek, P.; et al. Haematopoietic malignancies in rheumatoid arthritis: Lymphoma risk and characteristics after exposure to tumour necrosis factor antagonists. Ann. Rheum. Dis. 2005, 64, 1414. [Google Scholar] [CrossRef] [Green Version]
- Geborek, P.; Bladström, A.; Turesson, C.; Gulfe, A.; Petersson, I.F.; Saxne, T.; Olsson, H.; Jacobsson, L.T. Tumour necrosis factor blockers do not increase overall tumour risk in patients with rheumatoid arthritis, but may be associated with an increased risk of lymphomas. Ann. Rheum. Dis. 2005, 64, 699. [Google Scholar] [CrossRef] [Green Version]
- Solomon, D. The comparative safety and effectiveness of TNFalpha antagonists. J. Manag. Care Pharm. 2007, 13 (Suppl. 1), S7–S18. [Google Scholar] [CrossRef]
- Burmester, G.R.; Mease, P.; Dijkmans, B.A.; Gordon, K.; Lovell, D.; Panaccione, R.; Perez, J.; Pangan, A.L. Adalimumab safety and mortality rates from global clinical trials of six immune-mediated inflammatory diseases. Ann. Rheum. Dis. 2009, 68, 1863–1869. [Google Scholar] [CrossRef]
- Benson, J.M.; Peritt, D.; Scallon, B.J.; Heavner, G.A.; Shealy, D.J.; Giles-Komar, J.M.; Mascelli, M.A. Discovery and mechanism of ustekinumab: A human monoclonal antibody targeting interleukin-12 and interleukin-23 for treatment of immune-mediated disorders. mAbs 2011, 3, 535–545. [Google Scholar] [CrossRef] [Green Version]
- Wyant, T.; Fedyk, E.; Abhyankar, B. An Overview of the Mechanism of Action of the Monoclonal Antibody Vedolizumab. J. Crohn’s Colitis 2016, 10, 1437–1444. [Google Scholar] [CrossRef] [Green Version]
- Hasan, B.; Tandon, K.S.; Miret, R.; Khan, S.; Riaz, A.; Gonzalez, A.; Rahman, A.U.; Charles, R.; Narula, N.; Castro, F.J. Ustekinumab does not increase risk of new or recurrent cancer in inflammatory bowel disease patients with prior malignancy. J. Gastroenterol. Hepatol. 2022, 37, 1016–1021. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.J.; Zenger, C.; Pecoriello, J.; Pang, A.; Vallely, M.; Hudesman, D.P.; Chang, S.; E Axelrad, J. Ustekinumab and Vedolizumab Are Not Associated With Subsequent Cancer in IBD Patients with Prior Malignancy. Inflamm. Bowel Dis. 2022, 28, 1826–1832. [Google Scholar] [CrossRef]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of Cancer Risk Among US Solid Organ Transplant Recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef] [PubMed]
- Berastegui, C.; LaPorta, R.; López-Meseguer, M.; Romero, L.; Gómez-Ollés, S.; Riera, J.; Monforte, V.; Sáez, B.; Bravo, C.; Roman, A.; et al. Epidemiology and Risk Factors for Cancer After Lung Transplantation. Transplant. Proc. 2017, 49, 2285–2291. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S.; Ramsay, N.K.; Steinbuch, M.; Dusenbery, K.E.; Shapiro, R.S.; Weisdorf, D.J.; Robison, L.L.; Miller, J.S.; Neglia, J.P. Malignant Neoplasms Following Bone Marrow Transplantation. Blood 1996, 87, 3633–3639. [Google Scholar] [CrossRef] [Green Version]
- Saglam, K.; Sahin, T.T.; Ogut, Z.; Ince, V.; Usta, S.; Yilmaz, S. De Novo Malignancies After Liver Transplantation: Experience of a High-Volume Center. J. Gastrointest. Cancer 2021, 53, 1020–1027. [Google Scholar] [CrossRef]
- Caforio, A.; Fortina, A.; Piaserico, S.; Alaibac, M. Skin cancer in heart transplant recipients: Risk factor analysis and relevance of immunosuppressive therapy. Circulation 2000, 102, III222–III227. [Google Scholar] [CrossRef]
- Vajdic, C.; McDonald, S.; McCredie, M. Cancer incidence before and after kidney transplantation. JAMA 2006, 296, 2823–2831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enderby, C.; Keller, C.A. An overview of immunosuppression in solid organ transplantation. Am. J. Manag. Care 2015, 21 (Suppl. 1), S12–S23. [Google Scholar] [PubMed]
- Matser, Y.A.; Terpstra, M.L.; Nadalin, S.; Nossent, G.D.; de Boer, J.; van Bemmel, B.C.; van Eeden, S.; Budde, K.; Brakemeier, S.; Bemelman, F.J. Transmission of breast cancer by a single multiorgan donor to 4 transplant recipients. Am. J. Transplant. 2018, 18, 1810–1814. [Google Scholar] [CrossRef] [Green Version]
- Desai, R.; Collett, D.; Watson, C.J.; Johnson, P.; Evans, T.; Neuberger, J. Cancer Transmission From Organ Donors—Unavoidable But Low Risk. Transplantation 2012, 94, 1200–1207. Available online: https://journals.lww.com/transplantjournal/Fulltext/2012/12270/Cancer_Transmission_From_Organ_Donors_Unavoidable.5.aspx (accessed on 20 September 2022). [CrossRef] [PubMed]
- Eccher, A.; Girolami, I.; Motter, J.D.; Marletta, S.; Gambaro, G.; Momo, R.E.; Nacchia, F.; Donato, P.; Boschiero, L.; Boggi, U.; et al. Donor-transmitted cancer in kidney transplant recipients: A systematic review. J. Nephrol. 2020, 33, 1321–1332. [Google Scholar] [CrossRef]
- Borel, J.F.; Feurer, C.; Magnée, C.; Stähelin, H. Effects of the new anti-lymphocytic peptide cyclosporin A in animals. Immunology 1977, 32, 1017–1025. [Google Scholar]
- Ho, S.; Clipstone, N.; Timmermann, L.; Northrop, J.; Graef, I.; Fiorentino, D.; Nourse, J.; Crabtree, G.R. The mechanism of action of cyclosporin A and FK506. Clin. Immunol. Immunopathol. 1996, 80 Pt 2, S40–S45. [Google Scholar] [CrossRef] [PubMed]
- Tutschka, P.J.; Beschorner, W.E.; Allison, A.C.; Burns, W.H.; Santos, G.W. Use of cyclosporin A in allogeneic bone marrow transplantation in the rat. Nature 1979, 280, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.; Zhu, J.W.; Tadrous, M.; Drucker, A. Association Between Topical Calcineurin Inhibitor Use and Risk of Cancer, Including Lymphoma, Keratinocyte Carcinoma, and Melanoma: A Systematic Review and Meta-analysis. JAMA Dermatol. 2021, 157, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Dantal, J.; Soulillou, J.P. Immunosuppressive Drugs and the Risk of Cancer after Organ Transplantation. N. Engl. J. Med. 2005, 352, 1371–1373. [Google Scholar] [CrossRef] [PubMed]
- Stewart, T.; Tsai, S.C.; Grayson, H.; Henderson, R.; Opelz, G. Incidence of de-novo breast cancer in women chronically immunosuppressed after organ transplantation. Lancet 1995, 346, 796–798. [Google Scholar] [CrossRef]
- Stewart, T.; Henderson, R. Reduced incidence of rectal cancer, compared to gastric and colonic cancer, in a population of 73,076 men and women chronically immunosuppressed. Clin. Cancer Res. 1997, 3, 51–55. [Google Scholar] [PubMed]
- Miller, J.L. Sirolimus approved with renal transplant indication. Am. J. Health-Syst. Pharm. 1999, 56, 2177–2178. [Google Scholar] [CrossRef]
- Morice, W.; Brunn, G.J.; Wiederrecht, G.; Siekierka, J.; Abraham, R. Rapamycin-induced inhibition of p34cdc2 kinase activation is associated with G1/S-phase growth arrest in T lymphocytes. J. Biol. Chem. 1993, 268, 3734–3737. [Google Scholar] [CrossRef] [PubMed]
- Sabers, C.J.; Martin, M.M.; Brunn, G.J.; Williams, J.M.; Dumont, F.J.; Wiederrecht, G.; Abraham, R.T. Isolation of a Protein Target of the FKBP12-Rapamycin Complex in Mammalian Cells. J. Biol. Chem. 1995, 270, 815–8220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, J.D.; Lerner, C.G.; Schwartz, R.H. Inhibition of cell cycle progression by rapamycin induces T cell clonal anergy even in the presence of costimulation. J. Immunol. 1999, 162, 2775–2784. [Google Scholar] [PubMed]
- Vanasek, T.L.; Khoruts, A.; Zell, T.; Mueller, D.L. Antagonistic roles for CTLA-4 and the mammalian target of rapamycin in the regulation of clonal anergy: Enhanced cell cycle progression promotes recall antigen responsiveness. J. Immunol. 2001, 167, 5636–5644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luan, F.L.; Hojo, M.; Maluccio, M.; Yamaji, K.; Suthanthiran, M. Rapamycin blocks tumor progression: Unlinking immunosuppression from antitumor efficacy. Transplantation 2002, 73, 1565–1572. [Google Scholar] [CrossRef] [Green Version]
- Euvrard, S.; Ulrich, C.; Lefrancois, N. Immunosuppressants and Skin Cancer in Transplant Patients: Focus on Rapamycin. Dermatol. Surg. 2004, 30, 628–633. [Google Scholar] [CrossRef]
- Mathew, T.; Kreis, H.; Friend, P. Two-year incidence of malignancy in sirolimus-treated renal transplant recipients: Results from five multicenter studies. Clin. Transpl. 2004, 18, 446–449. [Google Scholar] [CrossRef]
- Kwitkowski, V.E.; Prowell, T.M.; Ibrahim, A.; Farrell, A.T.; Justice, R.; Mitchell, S.S.; Sridhara, R.; Pazdur, R. FDA Approval Summary: Temsirolimus as Treatment for Advanced Renal Cell Carcinoma. Oncologist 2010, 15, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Carew, J.S.; Kelly, K.R.; Nawrocki, S.T. Mechanisms of mTOR inhibitor resistance in cancer therapy. Target. Oncol. 2011, 6, 17–27. [Google Scholar] [CrossRef]
- Huang, S.; Bjornsti, M.A.; Houghton, P.J. Rapamycins: Mechanisms of Action and Cellular Resistance. Cancer Biol. Ther. 2003, 2, 222–232. [Google Scholar] [CrossRef] [Green Version]
- Farley, J.H.; Brady, W.E.; Fujiwara, K.; Nomura, H.; Yunokawa, M.; Tokunaga, H.; Saitou, M.; Gershenson, D.M. A phase II evaluation of temsirolimus in combination with carboplatin and paclitaxel followed by temsirolimus consolidation as first-line therapy in the treatment of stage III-IV clear cell carcinoma of the ovary. JCO 2016, 34, 5531. [Google Scholar] [CrossRef]
- McWilliams, R.R.; Allred, J.B.; Slostad, J.A.; Katipamula, R.; Dronca, R.S.; Rumilla, K.M.; Erickson, L.A.; Bryce, A.H.; Joseph, R.W.; Kottschade, L.A.; et al. NCCTG N0879 (Alliance): A randomized phase 2 cooperative group trial of carboplatin, paclitaxel, and bevacizumab ± everolimus for metastatic melanoma. Cancer 2018, 124, 537–545. [Google Scholar] [CrossRef]
- Baselga, J.; Campone, M.; Piccart, M.; Burris, I.I.I.H.A.; Rugo, H.S.; Sahmoud, T.; Noguchi, S.; Gnant, M.; Pritchard, K.I.; Lebrun, F.; et al. Everolimus in Postmenopausal Hormone-Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 366, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Pallet, N.; Legendre, C. Adverse events associated with mTOR inhibitors. Expert Opin. Drug Saf. 2013, 12, 177–186. [Google Scholar] [CrossRef]
- Pike, K.G.; Malagu, K.; Hummersone, M.G.; Menear, K.A.; Duggan, H.M.; Gomez, S.; Martin, N.M.; Ruston, L.; Pass, S.L.; Pass, M. Optimization of potent and selective dual mTORC1 and mTORC2 inhibitors: The discovery of AZD8055 and AZD2014. Bioorg. Med. Chem. Lett. 2013, 23, 1212–1216. [Google Scholar] [CrossRef] [PubMed]
- Carlo, M.I.; Molina, A.M.; Lakhman, Y.; Patil, S.; Woo, K.; DeLuca, J.; Lee, C.H.; Hsieh, J.J.; Feldman, D.R.; Motzer, R.J.; et al. A phase Ib study of BEZ235, a dual inhibitor of phosphatidylinositol 3-kinase (PI3K) and mammalian target of rapamycin (mTOR), in patients with advanced renal cell carcinoma. Oncologist 2016, 21, 787–788. [Google Scholar] [CrossRef] [Green Version]
- Powles, T.; Lackner, M.R.; Oudard, S.; Escudier, B.; Ralph, C.; Brown, J.E.; Hawkins, R.E.; Castellano, D.; Rini, B.I.; Staehler, M.D.; et al. Randomized open-label phase II trial of apitolisib (GDC-0980), a novel inhibitor of the PI3K/mammalian target of rapamycin pathway, versus everolimus in patients with metastatic renal cell carcinoma. J. Clin. Oncol. 2016, 34, 1660. [Google Scholar] [CrossRef]
- Jackson, R.C.; Weber, G.; Morris, H.P. IMP dehydrogenase, an enzyme linked with proliferation and malignancy. Nature 1975, 256, 331–333. [Google Scholar] [CrossRef]
- Allison, A.; Eugui, E. Immunosuppressive and other anti-rheumatic activities of mycophenolate mofetil. Agents Actions Suppl. 1993, 44, 165–188. [Google Scholar]
- Staatz, C.E.; Tett, S.E. Pharmacology and toxicology of mycophenolate in organ transplant recipients: An update. Arch. Toxicol. 2014, 88, 1351–1389. [Google Scholar] [CrossRef]
- Allison, A.C.; Eugui, E.M. The design and development of an immunosuppressive drug, mycophenolate mofetil. Springer Semin. Immunopathol. 1993, 14, 353–380. [Google Scholar] [CrossRef]
- Allison, A.C.; Eugui, E.M. Mycophenolate mofetil and its mechanisms of action. Immunopharmacology 2000, 47, 85–118. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kimura, T.; Ando, K.; Sawada, M.; Tamura, G. Antitumor activity of mycophenolic acid. J. Antibiot. 1969, 22, 297–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, R.H.; Lively, D.H.; DeLong, D.C.; Cline, J.C.; Sweeny, M.J. Mycophenolic acid: Antiviral and antitumor properties. J. Antibiot. 1968, 21, 463–464. [Google Scholar] [CrossRef]
- Tressler, R.J.; Garvin, L.J.; Slate, D.L. Anti-tumor activity of mycophenolate mofetil against human and mouse tumors in vivo. Int. J. Cancer 1994, 57, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Naffouje, R.; Grover, P.; Yu, H.; Sendilnathan, A.; Wolfe, K.; Majd, N.; Smith, E.P.; Takeuchi, K.; Senda, T.; Kofuji, S.; et al. Anti-Tumor Potential of IMP Dehydrogenase Inhibitors: A Century-Long Story. Cancers 2019, 11, 1346. [Google Scholar] [CrossRef] [Green Version]
- Takebe, N.; Cheng, X.; Wu, S.; Bauer, K.; Goloubeva, O.G.; Fenton, R.G.; Heyman, M.; Rapoport, A.P.; Badros, A.; Shaughnessy, J.; et al. Phase I Clinical Trial of the Inosine Monophosphate Dehydrogenase Inhibitor Mycophenolate Mofetil (Cellcept) in Advanced Multiple Myeloma Patients. Clin. Cancer Res. 2004, 10, 8301–8308. [Google Scholar] [CrossRef] [Green Version]
- Behrend, M. Adverse Gastrointestinal Effects of Mycophenolate Mofetil. Drug Saf. 2001, 24, 645–663. [Google Scholar] [CrossRef]
- Han, D.; Sasaki, M.; Yoshino, H.; Kofuji, S.; Sasaki, A.T.; Steckl, A.J. In-vitro evaluation of MPA-loaded electrospun coaxial fiber membranes for local treatment of glioblastoma tumor cells. J. Drug Deliv. Sci. Technol. 2017, 40, 45–50. [Google Scholar] [CrossRef]
- Valvezan, A.J.; McNamara, M.C.; Miller, S.K.; Torrence, M.E.; Asara, J.M.; Henske, E.P.; Manning, B.D. IMPDH inhibitors for antitumor therapy in tuberous sclerosis complex. JCI Insight 2020, 5, 135071. [Google Scholar] [CrossRef] [Green Version]
- Robson, R.; Cecka, J.M.; Opelz, G.; Budde, M.; Sacks, S. Prospective Registry-Based Observational Cohort Study of the Long-Term Risk of Malignancies in Renal Transplant Patients Treated with Mycophenolate Mofetil. Am. J. Transplant. 2005, 5, 2954–2960. [Google Scholar] [CrossRef] [PubMed]
- Cherikh, W.S.; Kauffman, H.M.; McBride, M.A.; Maghirang, J.; Swinnen, L.J.; Hanto, D.W. Association of the type of induction immunosuppression with posttransplant lymphoproliferative disorder, graft survival, and patient survival after primary kidney transplantation. Transplantation 2003, 76, 1289–1293. Available online: https://journals.lww.com/transplantjournal/Fulltext/2003/11150/Association_of_the_type_of_induction.4.aspx (accessed on 16 October 2022). [CrossRef] [PubMed]
- Allison, A. Mechanisms of action of mycophenolare mofetil. Lupus 2005, 14 (Suppl. 3), 2–8. [Google Scholar] [CrossRef]
- Murray, J.E.; Merrill, J.P.; Dammin, G.J.; Dealy, J.B., Jr.; Alexandre, G.W.; Harrison, J.H. Kidney transplantation in modified recipients. Ann. Surg. 1962, 156, 337. [Google Scholar] [CrossRef] [PubMed]
- Murray-Lyon, I.; Stern, R.; Williams, R. Controlled trial of prednisone and azathioprine in active chronic hepatitis. Lancet 1973, 301, 735–737. [Google Scholar] [CrossRef]
- Johnson, P.J.; McFarlane, I.G.; Williams, R. Azathioprine for Long-Term Maintenance of Remission in Autoimmune Hepatitis. N. Engl. J. Med. 1995, 333, 958–963. [Google Scholar] [CrossRef]
- Pasternak, B.; Svanström, H.; Schmiegelow, K.; Jess, T.; Hviid, A. Use of Azathioprine and the Risk of Cancer in Inflammatory Bowel Disease. Am. J. Epidemiol. 2013, 177, 1296–1305. [Google Scholar] [CrossRef]
- Setshedi, M.; Epstein, D.; Winter, T.A.; Myer, L.; Watermeyer, G.; Hift, R. Use of thiopurines in the treatment of inflammatory bowel disease is associated with an increased risk of non-melanoma skin cancer in an at-risk population: A cohort study. J. Gastroenterol. Hepatol. 2012, 27, 385–389. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, M.; Jiang, B.; Jin, T.; Shi, T.; Xu, B. Cancer occurrence following azathioprine treatment in myasthenia gravis patients: A systematic review and meta-analysis. J. Clin. Neurosci. 2021, 88, 70–74. [Google Scholar] [CrossRef]
- Burchenal, J.H.; Murphy, M.L.; Ellison, R.R.; Sykes, M.P.; Tan, T.C.; Leone, L.A.; Karnof-Sky, D.A.; Craver, L.F.; Dargeon, H.W.; Rhoads, C.P. Clinical Evaluation of a New Antimetabolite, 6-Mercaptopurine, in the Treatment of Leukemia and Allied Diseases. Blood 1953, 8, 965–999. [Google Scholar] [CrossRef] [Green Version]
- Korelitz, B.I.; Mirsky, F.J.; Fleisher, M.R.; Warman, J.I.; Wisch, N.; Gleim, G.W. Malignant neoplasms subsequent to treatment of inflammatory bowel disease with 6-mercaptopurine. Am. J. Gastroenterol. 1999, 94, 3248–3253. [Google Scholar] [CrossRef] [PubMed]
- Kandiel, A.; Fraser, A.G.; Korelitz, B.I.; Brensinger, C.; Lewis, J.D. Increased risk of lymphoma among inflammatory bowel disease patients treated with azathioprine and 6-mercaptopurine. Gut 2005, 54, 1121–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, L.C.; Bhatia, S.; Thompson, J.A.; Grivas, P. Preexisting autoimmune disease: Implications for immune checkpoint inhibitor therapy in solid tumors. J. Natl. Compr. Cancer Netw. 2019, 17, 750–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, H.; Weinmann, S.C.; Salama, A.K. Checkpoint Inhibitors in Melanoma Patients with Underlying Autoimmune Disease. Cancer Manag. Res. 2021, 13, 8199–8208. [Google Scholar] [CrossRef]
- Abdel-Wahab, N.; Shah, M.; Lopez-Olivo, M.A.; Suarez-Almazor, M.E. Use of Immune Checkpoint Inhibitors in the Treatment of Patients With Cancer and Preexisting Autoimmune Disease. Ann. Intern. Med. 2018, 168, 121–130. [Google Scholar] [CrossRef]
- Kehl, K.L.; Yang, S.; Awad, M.M.; Palmer, N.; Kohane, I.S.; Schrag, D. Pre-existing autoimmune disease and the risk of immune-related adverse events among patients receiving checkpoint inhibitors for cancer. Cancer Immunol. Immunother. 2019, 68, 917–926. [Google Scholar] [CrossRef]
- Tang, H.; Zhou, J.; Bai, C. The Efficacy and Safety of Immune Checkpoint Inhibitors in Patients With Cancer and Preexisting Autoimmune Disease. Front. Oncol. 2021, 11, 625872. [Google Scholar] [CrossRef]
- Frohne, C.C.; Llano, E.M.; Perkovic, A.; Cohen, R.D.; Luke, J.J. Complete response of metastatic melanoma in a patient with Crohn’s disease simultaneously receiving anti-α4β7 and anti-PD1 antibodies. J. ImmunoTherapy Cancer 2019, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.; Zeitouni, N.; Fan, W.; Samie, F.H. Immune checkpoint inhibitor therapy in solid organ transplant recipients: A patient-centered systematic review. J. Am. Acad. Derm. 2020, 82, 1490–1500. [Google Scholar] [CrossRef]
- Kumar, V.; Shinagare, A.B.; Rennke, H.G.; Ghai, S.; Lorch, J.H.; Ott, P.A.; Rahma, O.E. The Safety and Efficacy of Checkpoint Inhibitors in Transplant Recipients: A Case Series and Systematic Review of Literature. Oncologist 2020, 25, 505–514. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Organ Transplanted | Highest Cancer SIRs 1 | Most Common Suppression 4 |
|---|---|---|
| Kidney | NMSC 2, PTLD 3, Kidney | Tacro + MMF + steroids |
| Liver | NMSC 2, PTLD 3, Liver | Tacro + MMF + steroids |
| Lung | NMSC 2, PTLD 3, Lung | Tacro + MMF + steroids |
| Heart | NMSC 2, PTLD 3, Lung | Tacro + MMF + steroids |
| Pancreas | NMSC 2, PTLD 3, Pancreas | Tacro + MMF + steroids |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reyes, A.; Mohanty, A.; Pharaon, R.; Massarelli, E. Association between Immunosuppressive Therapy Utilized in the Treatment of Autoimmune Disease or Transplant and Cancer Progression. Biomedicines 2023, 11, 99. https://doi.org/10.3390/biomedicines11010099
Reyes A, Mohanty A, Pharaon R, Massarelli E. Association between Immunosuppressive Therapy Utilized in the Treatment of Autoimmune Disease or Transplant and Cancer Progression. Biomedicines. 2023; 11(1):99. https://doi.org/10.3390/biomedicines11010099
Chicago/Turabian StyleReyes, Amanda, Atish Mohanty, Rebecca Pharaon, and Erminia Massarelli. 2023. "Association between Immunosuppressive Therapy Utilized in the Treatment of Autoimmune Disease or Transplant and Cancer Progression" Biomedicines 11, no. 1: 99. https://doi.org/10.3390/biomedicines11010099