
Atherogenic Index of Plasma in Non-Alcoholic Fatty Liver Disease: Systematic Review and Meta-Analysis

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Risk of Bias Assessment in Individual Studies
2.4. Summary Measures and Synthesis of Results
3. Results
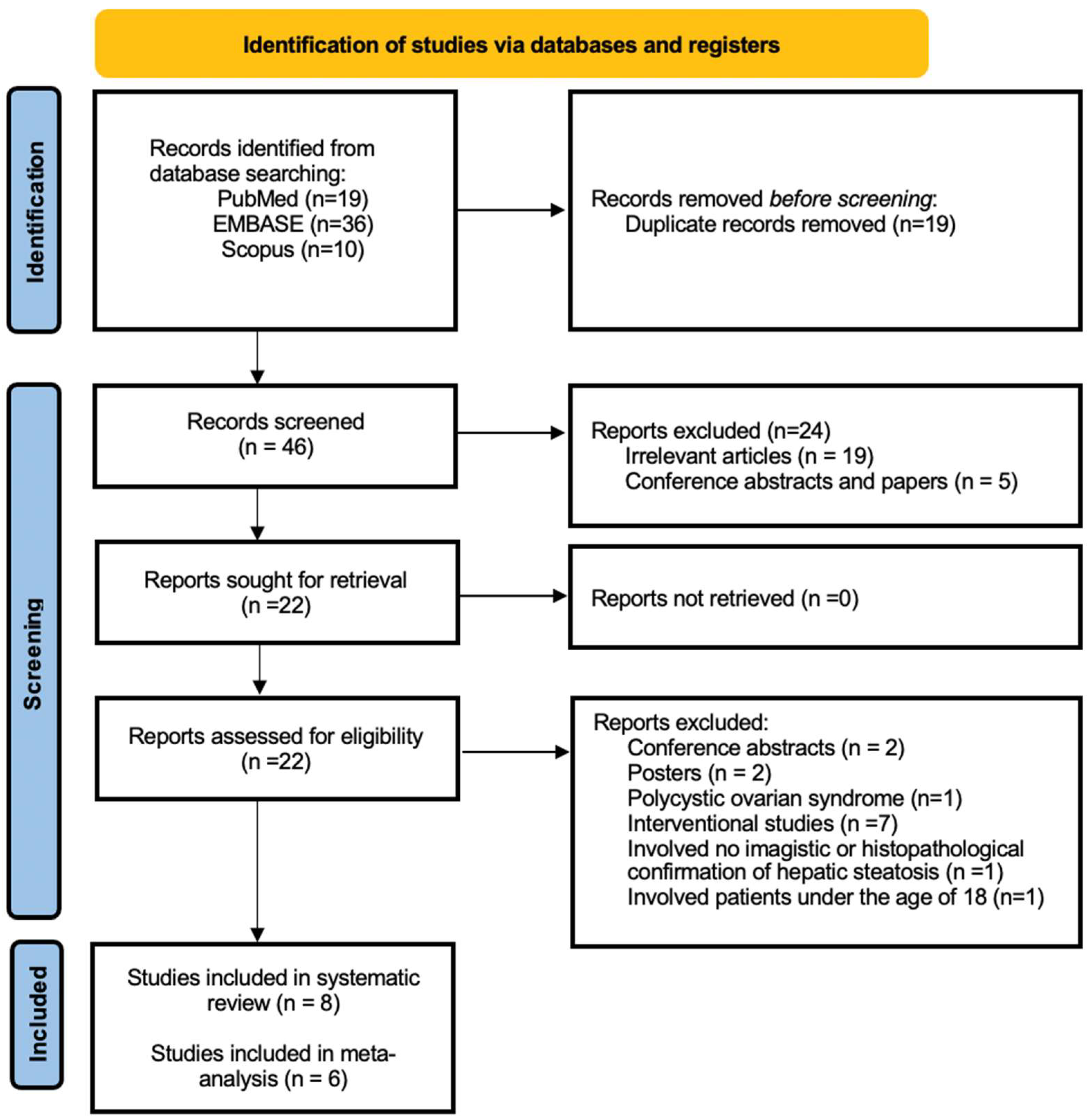
3.1. General Results
3.2. Study Characteristics
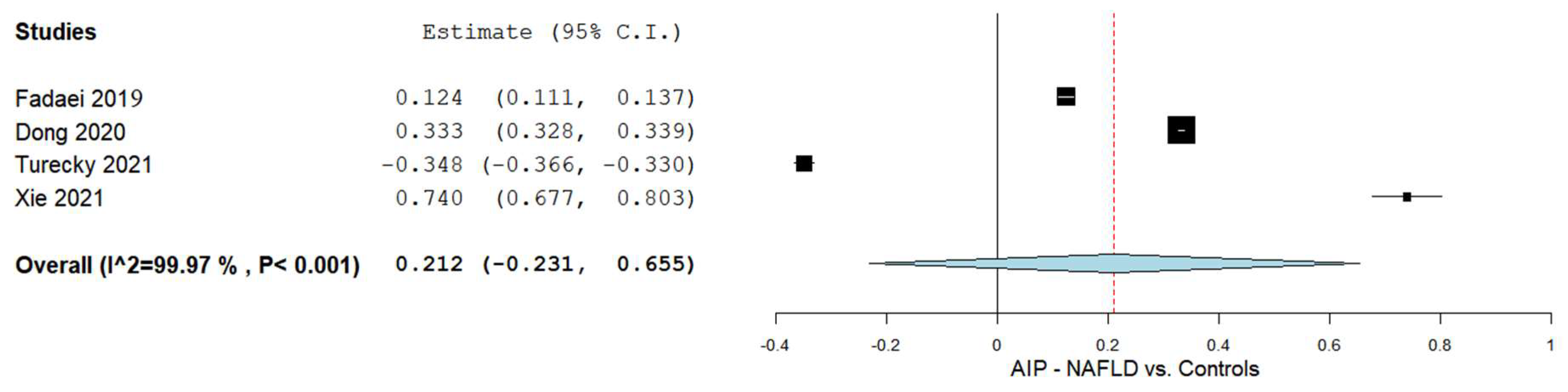
3.3. AIP and NAFLD
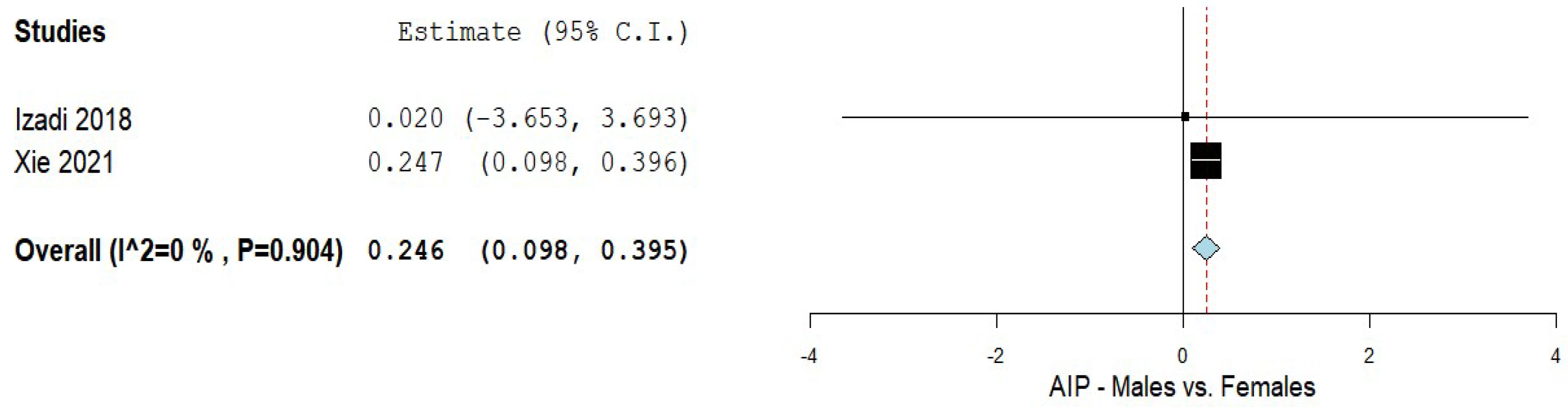
3.4. AIP and Males and Females
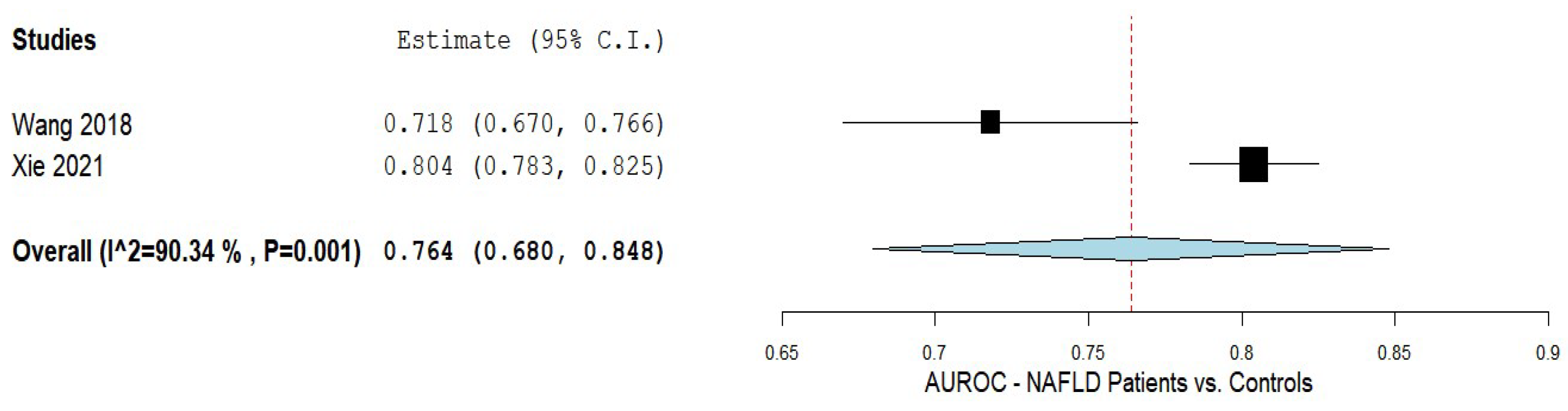
3.5. AIP in Predicting NAFLD
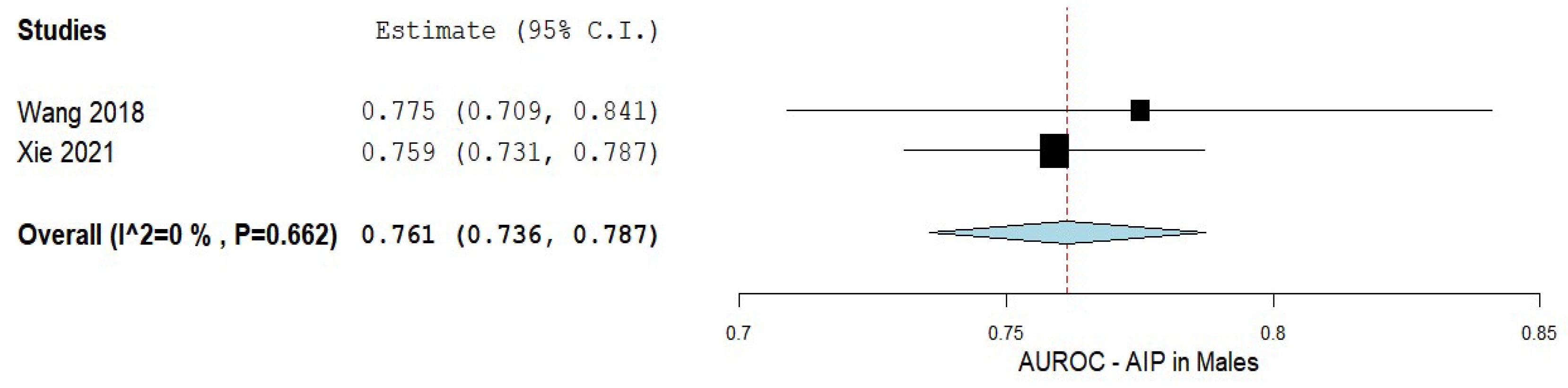
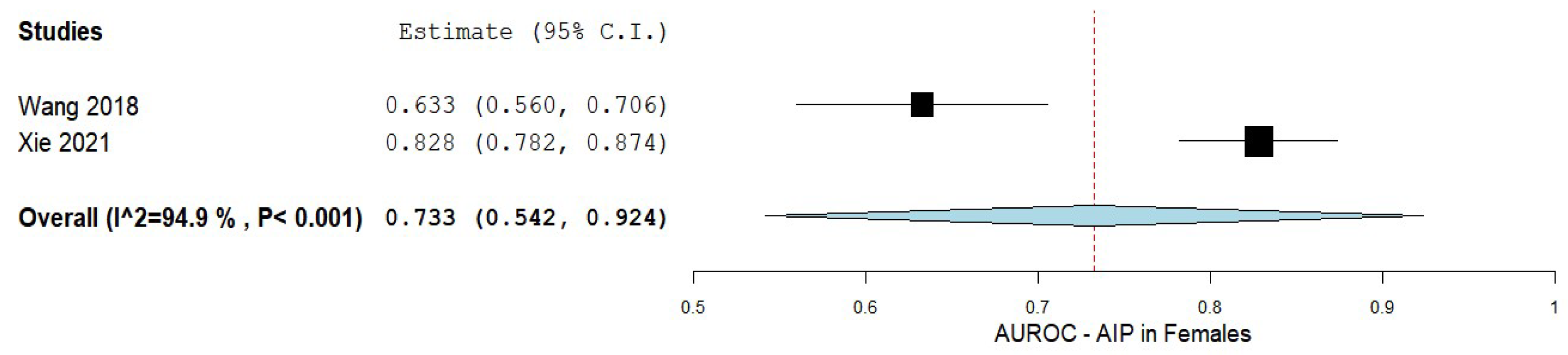
3.6. AIP in Predicting NAFLD Based on Sex
3.7. Bias Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ludwig, J.; Viggiano, T.R.; McGill, D.B.; Oh, B.J. Nonalcoholic Steatohepatitis: Mayo Clinic Experiences with a Hitherto Unnamed Disease. Mayo Clin. Proc. 1980, 55, 434–438. [Google Scholar] [PubMed]
- Yki-Järvinen, H. Non-Alcoholic Fatty Liver Disease as a Cause and a Consequence of Metabolic Syndrome. Lancet Diabetes Endocrinol. 2014, 2, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Fan, N.; Peng, L.; Xia, Z.; Zhang, L.; Song, Z.; Wang, Y.; Peng, Y. Triglycerides to High-Density Lipoprotein Cholesterol Ratio as a Surrogate for Nonalcoholic Fatty Liver Disease: A Cross-Sectional Study. Lipids Health Dis. 2019, 18, 39. [Google Scholar] [CrossRef] [PubMed]
- Fadaei, R.; Meshkani, R.; Poustchi, H.; Fallah, S.; Moradi, N.; Panahi, G.; Merat, S.; Golmohammadi, T. Association of Carotid Intima Media Thickness with Atherogenic Index of Plasma, Apo B/Apo A-I Ratio and Paraoxonase Activity in Patients with Non-Alcoholic Fatty Liver Disease. Arch. Physiol. Biochem. 2019, 125, 19–24. [Google Scholar] [CrossRef]
- Xie, F.; Pei, Y.; Zhou, Q.; Cao, D.; Wang, Y. Comparison of Obesity-Related Indices for Identifying Nonalcoholic Fatty Liver Disease: A Population-Based Cross-Sectional Study in China. Lipids Health Dis. 2021, 20, 132. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global Burden of NAFLD and NASH: Trends, Predictions, Risk Factors and Prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Sumida, Y.; Nakajima, A.; Itoh, Y. Limitations of Liver Biopsy and Non-Invasive Diagnostic Tests for the Diagnosis of Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis. World J. Gastroenterol. 2014, 20, 475–485. [Google Scholar] [CrossRef]
- Nassir, F. NAFLD: Mechanisms, Treatments, and Biomarkers. Biomolecules 2022, 12, 824. [Google Scholar]
- Ismaiel, A.; Leucuta, D.C.; Popa, S.L.; Dumitrascu, D.L. Serum Visfatin Levels in Nonalcoholic Fatty Liver Disease and Liver Fibrosis: Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3029. [Google Scholar] [CrossRef]
- Ismaiel, A.; Jaaouani, A.; Leucuta, D.-C.; Popa, S.-L.; Dumitrascu, D.L. The Visceral Adiposity Index in Non-Alcoholic Fatty Liver Disease and Liver Fibrosis-Systematic Review and Meta-Analysis. Biomedicines 2021, 9, 1890. [Google Scholar] [CrossRef] [PubMed]
- Sporea, I.; Popescu, A.; Dumitrașcu, D.; Brisc, C.; Nedelcu, L.; Trifan, A.; Gheorghe, L.; Braticevici, C.F. Nonalcoholic Fatty Liver Disease: Status Quo. J. Gastrointestin. Liver Dis. 2018, 27, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Alsharoh, H.; Ismaiel, A.; Leucuta, D.C.; Popa, S.L.; Dumitrascu, D.L. Plasminogen Activator Inhibitor-1 Levels in Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. J. Gastrointestin. Liver Dis. 2022, 31, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Fernando, D.H.; Forbes, J.M.; Angus, P.W.; Herath, C.B. Development and Progression of Non-Alcoholic Fatty Liver Disease: The Role of Advanced Glycation End Products. Int. J. Mol. Sci. 2019, 20, 5037. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; Sanyal, A.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef]
- Raff, E.J.; Kakati, D.; Bloomer, J.R.; Shoreibah, M.; Rasheed, K.; Singal, A.K. Diabetes Mellitus Predicts Occurrence of Cirrhosis and Hepatocellular Cancer in Alcoholic Liver and Non-Alcoholic Fatty Liver Diseases. J. Clin. Transl. Hepatol. 2015, 3, 9–16. [Google Scholar] [CrossRef]
- Samuel, V.T.; Shulman, G.I. Nonalcoholic Fatty Liver Disease as a Nexus of Metabolic and Hepatic Diseases. Cell Metab. 2018, 27, 22–41. [Google Scholar] [CrossRef]
- Zhang, Q.Q.; Lu, L.G. Nonalcoholic Fatty Liver Disease: Dyslipidemia, Risk for Cardiovascular Complications, and Treatment Strategy. J. Clin. Transl. Hepatol. 2015, 3, 78. [Google Scholar] [CrossRef]
- Targher, G.; Day, C.P.; Bonora, E. Risk of Cardiovascular Disease in Patients with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef]
- Nseir, W.; Shalata, A.; Marmor, A.; Assy, N. Mechanisms Linking Nonalcoholic Fatty Liver Disease with Coronary Artery Disease. Dig. Dis. Sci. 2011, 56, 3439–3449. [Google Scholar] [CrossRef]
- Ismaiel, A.; Colosi, H.A.; Rusu, F.; Dumitrașcu, D.L. Cardiac Arrhythmias and Electrocardiogram Modifications in Non-Alcoholic Fatty Liver Disease. A Systematic Review. J. Gastrointestin. Liver Dis. 2019, 28, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Ismaiel, A.; Dumitraşcu, D.L. Cardiovascular Risk in Fatty Liver Disease: The Liver-Heart Axis-Literature Review. Front. Med. 2019, 6, 202. [Google Scholar] [CrossRef] [PubMed]
- Ismaiel, A.; Spinu, M.; Budisan, L.; Leucuta, D.C.; Popa, S.L.; Chis, B.A.; Berindan-Neagoe, I.; Olinic, D.M.; Dumitrascu, D.L. Relationship between Adipokines and Cardiovascular Ultrasound Parameters in Metabolic-Dysfunction-Associated Fatty Liver Disease. J. Clin. Med. 2021, 10, 5194. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Yu, L.; Zhou, H.; Ma, Q.; Zhou, X.; Lei, T.; Hu, J.; Xu, W.; Yi, N.; Lei, S. Atherogenic Index of Plasma Is a Novel and Better Biomarker Associated with Obesity: A Population-Based Cross-Sectional Study in China. Lipids Health Dis. 2018, 17, 37. [Google Scholar] [CrossRef]
- Liu, H.; Liu, K.; Pei, L.; Li, S.; Zhao, J.; Zhang, K.; Zong, C.; Zhao, L.; Fang, H.; Wu, J.; et al. Atherogenic Index of Plasma Predicts Outcomes in Acute Ischemic Stroke. Front. Neurol. 2021, 12, 1728. [Google Scholar] [CrossRef] [PubMed]
- Niroumand, S.; Khajedaluee, M.; Khadem-Rezaiyan, M.; Abrishami, M.; Juya, M.; Khodaee, G.; Dadgarmoghaddam, M. Atherogenic Index of Plasma (AIP): A Marker of Cardiovascular Disease. Med. J. Islam. Repub. Iran 2015, 29, 240. [Google Scholar] [PubMed]
- Samimi, S.; Rajabzadeh, S.; Rabizadeh, S.; Nakhjavani, M.; Nakhaei, P.; Avanaki, F.A.; Esteghamati, A. Atherogenic Index of Plasma Is an Independent Predictor of Metabolic-Associated Fatty Liver Disease in Patients with Type 2 Diabetes. Eur. J. Med. Res. 2022, 27, 112. [Google Scholar] [CrossRef]
- Chang, Y.; Li, Y.; Guo, X.; Dai, D.; Sun, Y. The Association of Ideal Cardiovascular Health and Atherogenic Index of Plasma in Rural Population: A Cross-Sectional Study from Northeast China. Int. J. Environ. Res. Public Health 2016, 13, 1027. [Google Scholar] [CrossRef]
- Shen, S.; Lu, Y.; Qi, H.; Li, F.; Shen, Z.; Wu, L.; Yang, C.; Wang, L.; Shui, K.; Wang, Y.; et al. Association between Ideal Cardiovascular Health and the Atherogenic Index of Plasma. Medicine 2016, 95, e3866. [Google Scholar] [CrossRef]
- Von Delius, M.; Le, C.M.; Dong, V.M. Rhodium-Phosphoramidite Catalyzed Alkene Hydroacylation: Mechanism and Octaketide Natural Product Synthesis. J. Am. Chem. Soc. 2012, 134, 15022–15032. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Ismaiel, A.; Ciobanu, O.; Ismaiel, M.; Leucuta, D.C.; Popa, S.L.; David, L.; Ensar, D.; Al Srouji, N.; Dumitrascu, D. Atherogenic Index of Plasma in Non-Alchoholic Fatty Liver Disease: Systematic Review and Meta-Analysis. Inplasy Protocol 202280043. Int. Platf. Regist. Syst. Rev. Meta-Anal. Protoc. 2022, 43. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.T.A.D.; Green, S. (Eds.) 9.5.2 Identifying and Measuring Heterogeneity. Chapter 9 Sect. Analysing data and undertaking meta-analyses. In 9.5.2. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.0.2 (Updated September 2009); Cochrane Training: Cochrane, AB, Canada, 2009; Volume 100. [Google Scholar]
- Ampuero, J.; Aller, R.; Gallego-Durán, R.; Banales, J.; Crespo, J.; Mora-Cuadrado, N.; Garcia-Monzon, C.; Pareja, M.J.; Vilar-Gomez, E.; Jiménez-Agüero, R.; et al. Metabolically Unhealthy Status Impacts on the Risk of Significant Liver Injury in Biopsy-Proven NAFLD Patients beyond Obesity. J. Hepatol. 2018, 68, S832–S833. [Google Scholar] [CrossRef]
- Nassri, A.B.; Carranza, M.A.; Muftah, M.; Smotherman, C.; Malespin, M.; Ghali, P.M. Tu1574—Novel Noninvasive Inflammatory-Nutritional Biomarkers for Detecting Fibrosis in Non-Alcoholic Fatty Liver Disease. Gastroenterology 2019, 156, S-1364. [Google Scholar] [CrossRef]
- Li, H.-X.; Xu, M.-J.; Yuan, J.; Ding, Y.; Yang, L.; Wang, D.; Zhao, L.Y.G. The Change of Serum Asprosin Level in Patients with Type 2 Diabetes plus Non-Alcoholic Fatty Liver Disease and the Influencing Factors. J. Jiangsu Univ. Ed. 2019, 29, 62–66. [Google Scholar]
- Thomas, D.M.; Iqbal, A.N.; Singh, R.; Srijaya, S.; Prashant, K.S.; Premaletha, N.; Devadas, K. Do NAFLD Patients with Advanced Fibrosis Have an Adverse Cardiometabolic Profile: A Comparative Study Using Carotid Intimal Medial Thickness, Metabolic Syndrome, and Atherogenic Index of Plasma. J. Gastroenterol. Hepatol. 2021, 36, 270. [Google Scholar]
- Sangouni, A.A.; Sasanfar, B.; Ghadiri-Anari, A.; Hosseinzadeh, M. Effect of L-Carnitine Supplementation on Liver Fat Content and Cardiometabolic Indices in Overweight/Obese Women with Polycystic Ovary Syndrome: A Randomized Controlled Trial. Clin. Nutr. ESPEN 2021, 46, 54–59. [Google Scholar] [CrossRef]
- Hamed, N.; Soliman, A.; De Sanctis, V.; Alaaraj, N.; Alyafei, F.; Shaat, M.; Aljaffali, N.; Itani, M.; Jour, C. The Prevalence of the Different Components of the Metabolic Syndrome (MetS) in Obese Nondiabetic Children and Young Adolescents and Their Anthropometric Data in Relation to Parents. Acta Biomed. 2021, 92, e2021321. [Google Scholar] [CrossRef] [PubMed]
- Mahran, H.N.; Saber, L.M.; Alghaithy, A.A.; Elareefy, A.A. The Role of Elevated Alanine Aminotransferase (ALT), FasL and Atherogenic Dyslipidemia in Type II Diabetes Mellitus. J. Taibah Univ. Med. Sci. 2017, 12, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Gelli, C.; Tarocchi, M.; Abenavoli, L.; Di Renzo, L.; Galli, A.; De Lorenzo, A. Effect of a Counseling-Supported Treatment with the Mediterranean Diet and Physical Activity on the Severity of the Non-Alcoholic Fatty Liver Disease. World J. Gastroenterol. 2017, 23, 3150–3162. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, S.; Gargari, B.P.; Aliasghari, F.; Asjodi, F.; Izadi, A. Ramadan Fasting Improves Liver Function and Total Cholesterol in Patients with Nonalcoholic Fatty Liver Disease. Int. J. Vitam. Nutr. Res. Int. Z. Fur Vitam. Ernahrungsforschung. J. Int. Vitaminol. Nutr. 2020, 90, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Farzin, L.; Asghari, S.; Rafraf, M.; Asghari-Jafarabadi, M.; Shirmohammadi, M. No Beneficial Effects of Resveratrol Supplementation on Atherogenic Risk Factors in Patients with Nonalcoholic Fatty Liver Disease. Int. J. Vitam. Nutr. Res. Int. Z. Fur Vitam. Ernahrungsforschung. J. Int. Vitaminol. Nutr. 2020, 90, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Moradi, F.; Kooshki, F.; Nokhostin, F.; Khoshbaten, M.; Bazyar, H.; Pourghassem Gargari, B. A Pilot Study of the Effects of Chromium Picolinate Supplementation on Serum Fetuin-A, Metabolic and Inflammatory Factors in Patients with Nonalcoholic Fatty Liver Disease: A Double-Blind, Placebo-Controlled Trial. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. 2021, 63, 126659. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Orang, Z.; Mozaffari-Khosravi, H. Effect of Omega-3 Supplementation on Cardiometabolic Indices in Diabetic Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. BMC Nutr. 2021, 7, 86. [Google Scholar] [CrossRef]
- Naeini, F.; Namkhah, Z.; Tutunchi, H.; Rezayat, S.M.; Mansouri, S.; Yaseri, M.; Hosseinzadeh-Attar, M.J. Effects of Naringenin Supplementation on Cardiovascular Risk Factors in Overweight/Obese Patients with Nonalcoholic Fatty Liver Disease: A Pilot Double-Blind, Placebo-Controlled, Randomized Clinical Trial. Eur. J. Gastroenterol. Hepatol. 2022, 34, 345–353. [Google Scholar] [CrossRef]
- Sangouni, A.A.; Sangsefidi, Z.S.; Yarhosseini, F.; Hosseinzadeh, M.; Akhondi-Meybodi, M.; Ranjbar, A.; Madadizadeh, F.; Mozaffari-Khosravi, H. Effect of Cornus Mas L. Fruit Extract on Lipid Accumulation Product and Cardiovascular Indices in Patients with Non-Alcoholic Fatty Liver Disease: A Double-Blind Randomized Controlled Trial. Clin. Nutr. ESPEN 2022, 47, 51–57. [Google Scholar] [CrossRef]
- Izadi, A.; Gargari, B.P.; Aliasghari, F.; Ebrahimi, S. Adipokines and Visceral Adiposity Index in Relation to Clinical Findings of NAFLD Patients. Prog. Nutr. 2018, 20, 145–152. [Google Scholar] [CrossRef]
- Wang, Q.; Zheng, D.; Liu, J.; Fang, L.; Li, Q. Atherogenic Index of Plasma Is a Novel Predictor of Non-Alcoholic Fatty Liver Disease in Obese Participants: A Cross-Sectional Study. Lipids Health Dis. 2018, 17, 284. [Google Scholar] [CrossRef] [PubMed]
- Izadi, A.; Aliasghari, F.; Gargari, B.P.; Ebrahimi, S. Strong Association between Serum Vitamin D and Vaspin Levels, AIP, VAI and Liver Enzymes in NAFLD Patients. Int. J. Vitam. Nutr. Res. Int. Z. Vitam. Ernahrungsforschung. J. Int. Vitaminol. Nutr. 2020, 90, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.S.; Tang, M.J.; Xu, T.L.; Su, J.B.; Wang, X.Q.; Xu, F.; Zhang, D.M.; Zhu, Q.; Cao, J.; Wang, H. Association of Serum Fibroblast Growth Factor 19 Levels with Arteriosclerosis Parameters Assessed by Arterial Stiffness and Atherogenic Index of Plasma in Patients with Type 2 Diabetes. Diabetol. Metab. Syndr. 2020, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.-Y.; Mao, Y.-Q.; Li, Z.-Y.; Yu, F.-J. The Value of the Atherogenic Index of Plasma in Non-Obese People with Non-Alcoholic Fatty Liver Disease: A Secondary Analysis Based on a Cross-Sectional Study. Lipids Health Dis. 2020, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Turecký, L.; Kupčová, V.; Urfinová, M.; Repiský, M.; Uhlíková, E. Serum Butyrylcholinesterase/HDL-Cholesterol Ratio and Atherogenic Index of Plasma in Patients with Fatty Liver Disease. Vnitr. Lek. 2021, 67, 4–8. [Google Scholar] [CrossRef]
- Pan, J.J.; Fallon, M.B. Gender and Racial Differences in Nonalcoholic Fatty Liver Disease. World J. Hepatol. 2014, 6, 274–283. [Google Scholar] [CrossRef]
- Lonardo, A.; Trande, P. Are There Any Sex Differences in Fatty Liver? A Study of Glucose Metabolism and Body Fat Distribution. J. Gastroenterol. Hepatol. 2000, 15, 775–782. [Google Scholar] [CrossRef]
- Saponaro, C.; Sabatini, S.; Gaggini, M.; Carli, F.; Rosso, C.; Positano, V.; Armandi, A.; Caviglia, G.P.; Faletti, R.; Bugianesi, E.; et al. Adipose Tissue Dysfunction and Visceral Fat Are Associated to Hepatic Insulin Resistance and Severity of NASH Even in Lean Individuals. Liver Int. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Sumida, Y.; Yoneda, M.; Tokushige, K.; Kawanaka, M.; Fujii, H.; Yoneda, M.; Imajo, K.; Takahashi, H.; Eguchi, Y.; Ono, M.; et al. FIB-4 First in the Diagnostic Algorithm of Metabolic-Dysfunction-Associated Fatty Liver Disease in the Era of the Global Metabodemic. Life 2021, 11, 143. [Google Scholar] [CrossRef]
- Giannini, C.; Santoro, N.; Caprio, S.; Kim, G.; Lartaud, D.; Shaw, M.; Pierpont, B.; Weiss, R. The Triglyceride-to-HDL Cholesterol RatioAssociation with Insulin Resistance in Obese Youths of Different Ethnic Backgrounds. Diabetes Care 2011, 34, 1869–1874. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Adams, L.A.; de Lédinghen, V.; Wong, G.L.-H.; Sookoian, S. Noninvasive Biomarkers in NAFLD and NASH—Current Progress and Future Promise. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 461–478. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Jou, J.H. Nonalcoholic Fatty Liver Disease and Recent Guideline Updates. Clin. Liver Dis. 2021, 17, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Chalasani, N. Non-Invasive Assessment of Non-Alcoholic Fatty Liver Disease: Clinical Prediction Rules and Blood-Based Biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A New Definition for Metabolic Dysfunction-Associated Fatty Liver Disease: An International Expert Consensus Statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Longo, M.; Zatterale, F.; Naderi, J.; Parrillo, L.; Formisano, P.; Raciti, G.A.; Beguinot, F.; Miele, C. Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications. Int. J. Mol. Sci. 2019, 20, 2358. [Google Scholar] [CrossRef]
- She, Y.; Mangat, R.; Tsai, S.; Proctor, S.D.; Richard, C. The Interplay of Obesity, Dyslipidemia and Immune Dysfunction: A Brief Overview on Pathophysiology, Animal Models, and Nutritional Modulation. Front. Nutr. 2022, 9, 138. [Google Scholar] [CrossRef]
- Pei, K.; Gui, T.; Kan, D.; Feng, H.; Jin, Y.; Yang, Y.; Zhang, Q.; Du, Z.; Gai, Z.; Wu, J.; et al. An Overview of Lipid Metabolism and Nonalcoholic Fatty Liver Disease. Biomed Res. Int. 2020, 2020, 4020249. [Google Scholar] [CrossRef]
- Sumner, A.E.; Finley, K.B.; Genovese, D.J.; Criqui, M.H.; Boston, R.C. Fasting Triglyceride and the Triglyceride-HDL Cholesterol Ratio Are Not Markers of Insulin Resistance in African Americans. Arch. Intern. Med. 2005, 165, 1395–1400. [Google Scholar] [CrossRef]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef]
- Bugianesi, E.; Moscatiello, S.; Ciaravella, M.; Marchesini, G. Insulin resistance in nonalcoholic fatty liver disease. Curr. Pharm. Des. 2010, 16, 1941–1951. [Google Scholar] [CrossRef]
- Akhtar, D.H.; Iqbal, U.; Vazquez-Montesino, L.M.; Dennis, B.B.; Ahmed, A. Pathogenesis of Insulin Resistance and Atherogenic Dyslipidemia in Nonalcoholic Fatty Liver Disease. J Clin Transl Hepatol. 2019, 28, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Nevola, R.; Coppola, C.; Narciso, V.; Rinaldi, L.; Calvaruso, V.; Pafundi, P.C.; Lombardi, R.; et al. Reduced incidence of type 2 diabetes in patients with chronic hepatitis C virus infection cleared by direct-acting antiviral therapy: A prospective study. Diabetes Obes Metab. 2020, 22, 2408–2416. [Google Scholar] [CrossRef] [PubMed]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Original Research: Diagnostic Accuracy of Non-Invasive Tests for Advanced Fibrosis in Patients with NAFLD: An Individual Patient Data Meta-Analysis. Gut 2022, 71, 1006. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, A.; Ismaiel, A.; Procopio, A.C.; Luzza, F.; Abenavoli, L.; Dumitrascu, D.L. Non-invasive biochemical markers and surrogate scores in evaluating non-alcoholic steatohepatitis. A narrative review. Minerva Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Cianci, N.; Subhani, M.; Hill, T.; Khanna, A.; Zheng, D.; Sheth, A.; Crooks, C.; Aithal, G.P. Prognostic Non-Invasive Biomarkers for All-Cause Mortality in Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. World J. Hepatol. 2022, 14, 1025. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismaiel, A.; Ciobanu, O.S.; Ismaiel, M.; Leucuta, D.-C.; Popa, S.-L.; David, L.; Ensar, D.; Al Srouji, N.; Dumitrascu, D.L. Atherogenic Index of Plasma in Non-Alcoholic Fatty Liver Disease: Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 2101. https://doi.org/10.3390/biomedicines10092101
Ismaiel A, Ciobanu OS, Ismaiel M, Leucuta D-C, Popa S-L, David L, Ensar D, Al Srouji N, Dumitrascu DL. Atherogenic Index of Plasma in Non-Alcoholic Fatty Liver Disease: Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(9):2101. https://doi.org/10.3390/biomedicines10092101
Chicago/Turabian StyleIsmaiel, Abdulrahman, Oana Sabina Ciobanu, Mohamed Ismaiel, Daniel-Corneliu Leucuta, Stefan-Lucian Popa, Liliana David, Dilara Ensar, Nahlah Al Srouji, and Dan L. Dumitrascu. 2022. "Atherogenic Index of Plasma in Non-Alcoholic Fatty Liver Disease: Systematic Review and Meta-Analysis" Biomedicines 10, no. 9: 2101. https://doi.org/10.3390/biomedicines10092101