

Systematic Review and Meta-Analysis of the Usefulness of Epicardial Fat Thickness as a Non-Invasive Marker of the Presence and Severity of Nonalcoholic Fatty Liver Disease

Abstract
:1. Introduction
2. Method
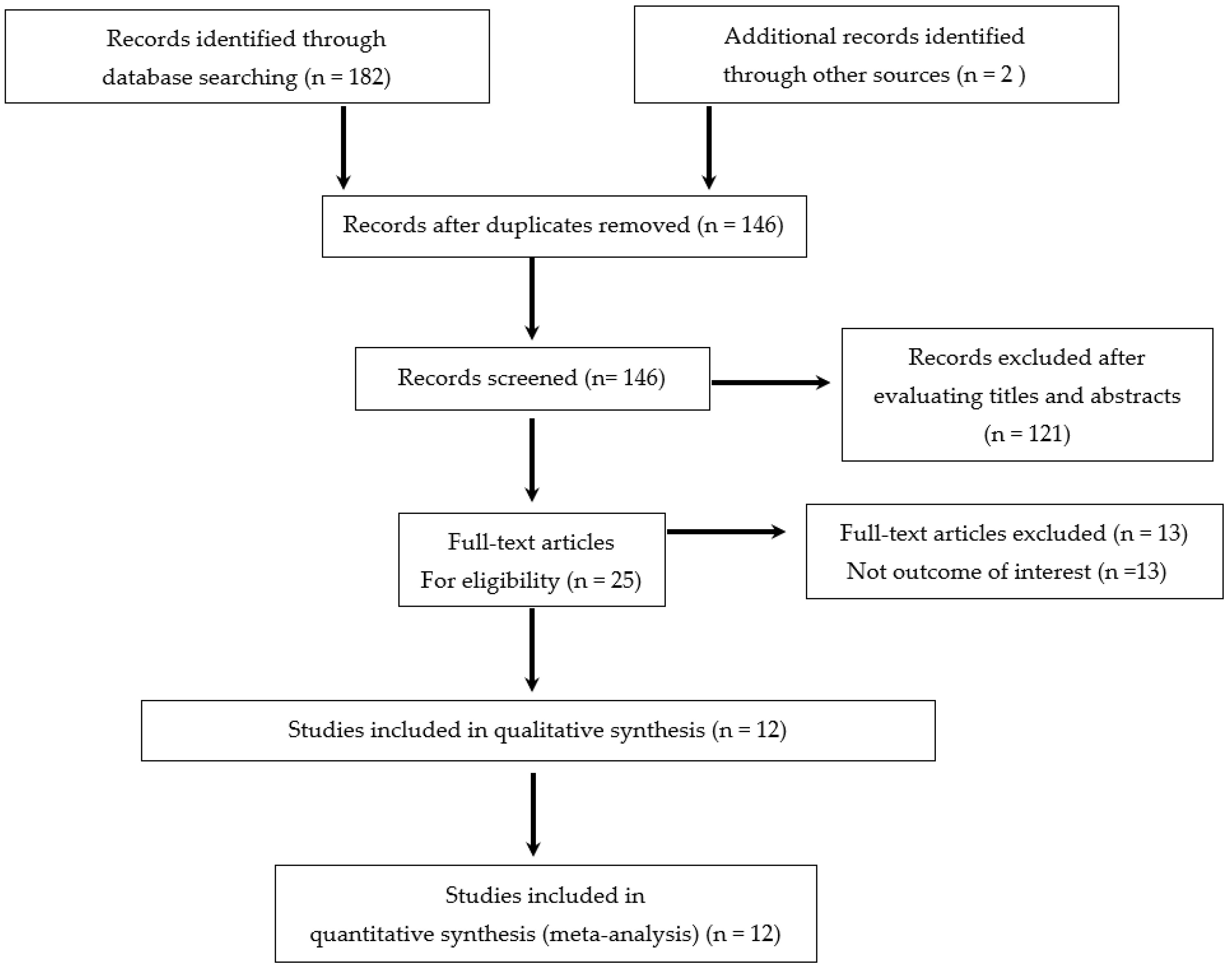
2.1. Data Sources and Searches
2.2. Data Extraction and Methodological Quality Rating
2.3. Data Synthesis and Analysis
3. Results
3.1. Characteristics of Included Studies, Methodological Quality
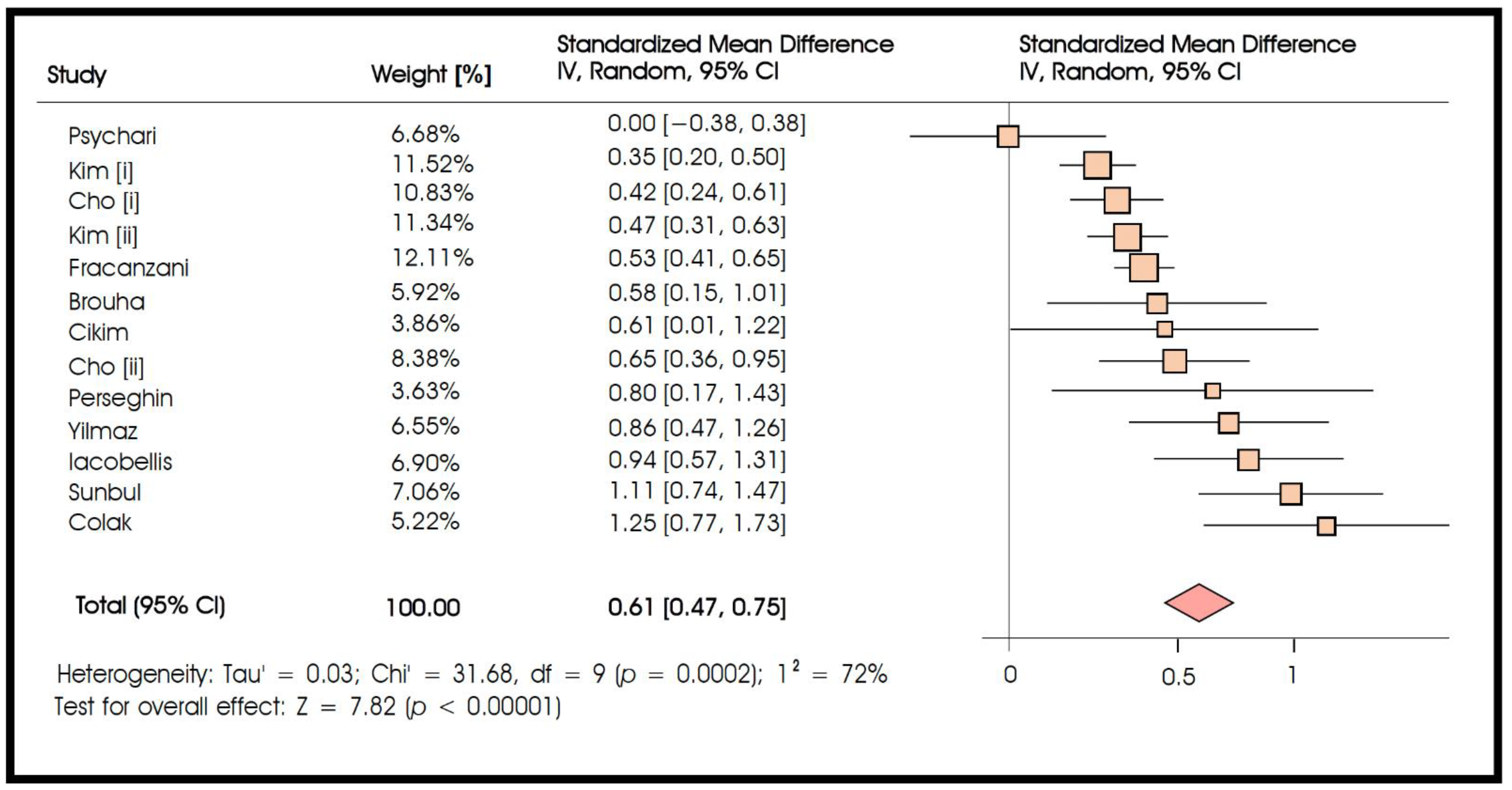
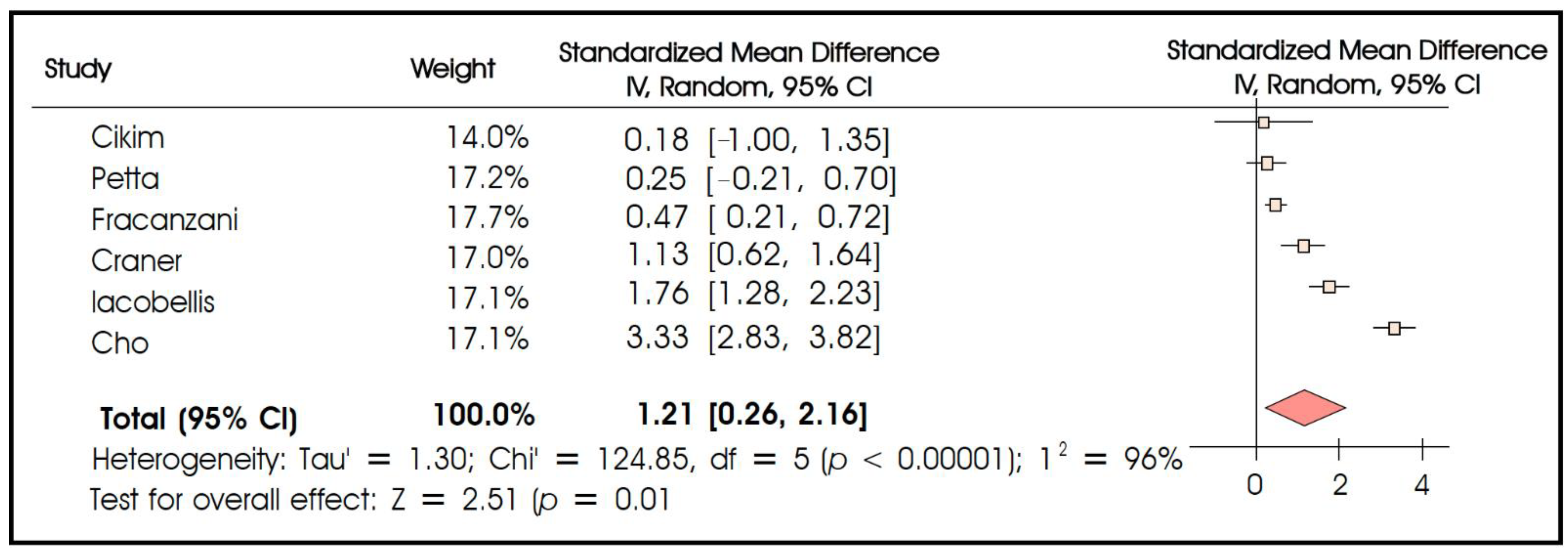
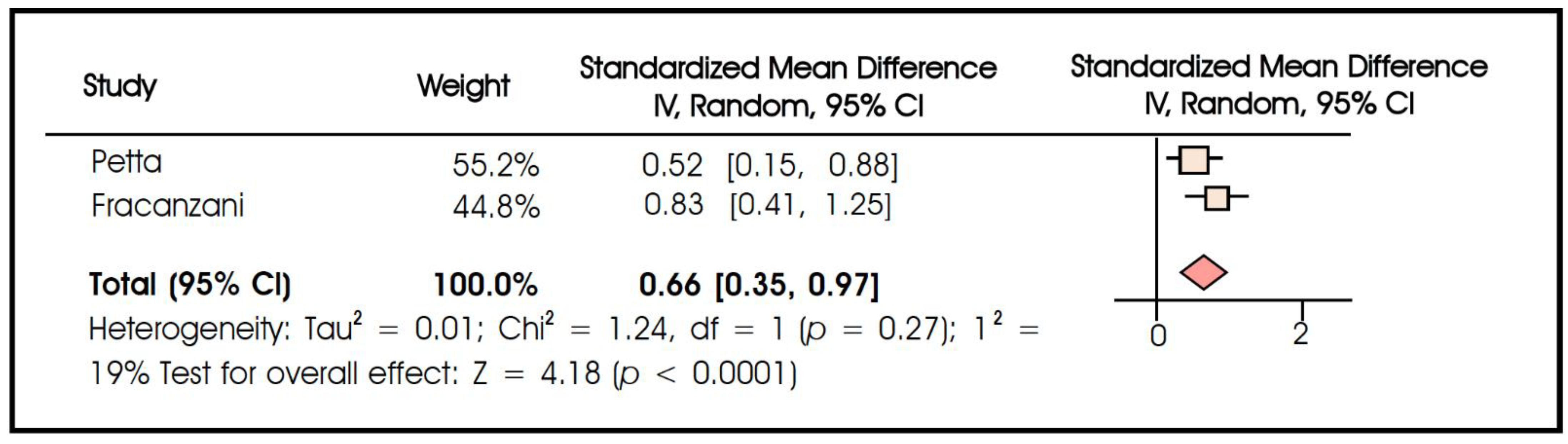
3.2. Quantitative Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rabkin, S.W. Epicardial fat: Properties, function and relationship to obesity. Obes. Rev. 2007, 8, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Salazar, J.; Luzardo, E.; Mejias, J.C.; Rojas, J.; Ferreira, A.; Rivas-Rios, J.R.; Bermudez, V. Epicardial Fat: Physiological, Pathological, and Therapeutic Implications. Cardiol. Res. Pract. 2016, 2016, 1291537. [Google Scholar] [CrossRef] [PubMed]
- Villasante Fricke, A.C.; Iacobellis, G. Epicardial Adipose Tissue: Clinical Biomarker of Cardio-Metabolic Risk. Int. J. Mol. Sci. 2019, 20, 5989. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Bianco, A.C. Epicardial adipose tissue: Emerging physiological, pathophysiological and clinical features. Trends Endocrinol. Metab. 2011, 22, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Perseghin, G.; Lattuada, G.; De Cobelli, F.; Esposito, A.; Belloni, E.; Ntali, G.; Ragogna, F.; Canu, T.; Scifo, P.; Del Maschio, A.; et al. Increased mediastinal fat and impaired left ventricular energy metabolism in young men with newly found fatty liver. Hepatology 2008, 47, 51–58. [Google Scholar] [CrossRef]
- Granér, M.; Nyman, K.; Siren, R.; Pentikäinen, M.O.; Lundbom, J.; Hakkarainen, A.; Lauerma, K.; Lundbom, N.; Nieminen, M.S.; Taskinen, M.R. Ectopic fat depots and left ventricular function in nondiabetic men with nonalcoholic fatty liver disease. Circulation. Cardiovasc. Imaging 2015, 8, e001979. [Google Scholar] [CrossRef]
- Wong, C.X.; Ganesan, A.N.; Selvanayagam, J.B. Epicardial fat and atrial fibrillation: Current evidence, potential mechanisms, clinical implications, and future directions. Eur. Heart J. 2017, 38, 1294–1302. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Gariani, K.; Jornayvaz, F.R. Pathophysiology of NASH in endocrine diseases. Endocr. Connect. 2021, 10, R52–R65. [Google Scholar] [CrossRef]
- Bhatia, L.S.; Curzen, N.P.; Calder, P.C.; Byrne, C.D. Non-alcoholic fatty liver disease: A new and important cardiovascular risk factor? Eur. Heart J. 2012, 33, 1190–1200. [Google Scholar] [CrossRef] [Green Version]
- Tana, C.; Ballestri, S.; Ricci, F.; Di Vincenzo, A.; Ticinesi, A.; Gallina, S.; Giamberardino, M.A.; Cipollone, F.; Sutton, R.; Vettor, R.; et al. Cardiovascular Risk in Non-Alcoholic Fatty Liver Disease: Mechanisms and Therapeutic Implications. Int. J. Environ. Res. Public Health 2019, 16, 3104. [Google Scholar] [CrossRef]
- Adams, L.A.; Anstee, Q.M.; Tilg, H.; Targher, G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66, 1138–1153. [Google Scholar] [CrossRef] [PubMed]
- Seeff, L.B.; Everson, G.T.; Morgan, T.R.; Curto, T.M.; Lee, W.M.; Ghany, M.G.; Shiffman, M.L.; Fontana, R.J.; Di Bisceglie, A.M.; Bonkovsky, H.L.; et al. Complication rate of percutaneous liver biopsies among persons with advanced chronic liver disease in the HALT-C trial. Clin. Gastroenterol. Hepatol. 2010, 8, 877–883. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Vali, Y.; Boursier, J.; Spijker, R.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H. Prognostic accuracy of FIB-4, NAFLD fibrosis score and APRI for NAFLD-related events: A systematic review. Liver Int. 2021, 41, 261–270. [Google Scholar] [CrossRef]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef]
- Cotter, T.G.; Rinella, M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology 2020, 158, 1851–1864. [Google Scholar] [CrossRef] [PubMed]
- Fracanzani, A.L.; Pisano, G.; Consonni, D.; Tiraboschi, S.; Baragetti, A.; Bertelli, C.; Norata, G.D.; Dongiovanni, P.; Valenti, L.; Grigore, L.; et al. Epicardial Adipose Tissue (EAT) Thickness Is Associated with Cardiovascular and Liver Damage in Nonalcoholic Fatty Liver Disease. PLoS ONE 2016, 11, e0162473. [Google Scholar] [CrossRef]
- Colak, Y.; Karabay, C.Y.; Tuncer, I.; Kocabay, G.; Kalayci, A.; Senates, E.; Ozturk, O.; Doganay, H.L.; Enc, F.Y.; Ulasoglu, C.; et al. Relation of epicardial adipose tissue and carotid intima-media thickness in patients with nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2012, 24, 613–618. [Google Scholar] [CrossRef]
- Iacobellis, G.; Barbarini, G.; Letizia, C.; Barbaro, G. Epicardial fat thickness and nonalcoholic fatty liver disease in obese subjects. Obesity 2014, 22, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.S.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonran-Domized Studies on Meta-Analysis. 2009. Available online: http://www.evidencebasedpublichealth.de/download/Newcastle_Ottowa_Scale_Pope_Bruce.pdf (accessed on 31 August 2022).
- Petta, S.; Argano, C.; Colomba, D.; Cammà, C.; Di Marco, V.; Cabibi, D.; Tuttolomondo, A.; Marchesini, G.; Pinto, A.; Licata, G.; et al. Epicardial fat, cardiac geometry and cardiac function in patients with non-alcoholic fatty liver disease: Association with the severity of liver disease. J. Hepatol. 2015, 62, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Cikim, A.S.; Topal, E.; Harputluoglu, M.; Keskin, L.; Zengin, Z.; Cikim, K.; Ozdemir, R.; Aladag, M.; Yologlu, S. Epicardial adipose tissue, hepatic steatosis and obesity. J. Endocrinol. Invest. 2007, 30, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.I.; Jo, E.A.; Cho, S.H.; Kim, B.H. The Influence of Epicardial Fat and Nonalcoholic Fatty Liver Disease on Heart Rate Recovery in Metabolic Syndrome. Metab. Syndr. Relat. Disord. 2017, 15, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Psychari, S.N.; Rekleiti, N.; Papaioannou, N.; Varhalama, E.; Drakoulis, C.; Apostolou, T.S.; Iliodromitis, E.K. Epicardial Fat in Nonalcoholic Fatty Liver Disease: Properties and Relationships With Metabolic Factors, Cardiac Structure, and Cardiac Function. Angiology 2016, 67, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700–711. [Google Scholar]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. Ascertaining the minimal clinically important difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral-Sciences; Erlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Priest, C.; Tontonoz, P. Inter-organ cross-talk in metabolic syndrome. Nat. Metab. 2019, 1, 1177–1188. [Google Scholar] [CrossRef]
- Oishi, Y.; Manabe, I. Organ System Crosstalk in Cardiometabolic Disease in the Age of Multimorbidity. Front. Cardiovasc. Med. 2020, 7, 64. [Google Scholar] [CrossRef]
- Britton, K.A.; Fox, C.S. Ectopic fat depots and cardiovascular disease. Circulation 2011, 124, e837–e841. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Nasu, K.; Terashima, M.; Ehara, M.; Kinoshita, Y.; Ito, T.; Kimura, M.; Tanaka, N.; Habara, M.; Tsuchikane, E.; et al. The impact of epicardial fat volume on coronary plaque vulnerability: Insight from optical coherence tomography analysis. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Yerramasu, A.; Dey, D.; Venuraju, S.; Anand, D.V.; Atwal, S.; Corder, R.; Berman, D.S.; Lahiri, A. Increased volume of epicardial fat is an independent risk factor for accelerated progression of sub-clinical coronary atherosclerosis. Atherosclerosis 2012, 220, 223–230. [Google Scholar] [CrossRef] [PubMed]
- van der Poorten, D.; Milner, K.L.; Hui, J.; Hodge, A.; Trenell, M.I.; Kench, J.G.; London, R.; Peduto, T.; Chisholm, D.J.; George, J. Visceral fat: A key mediator of steatohepatitis in metabolic liver disease. Hepatology 2008, 48, 449–457. [Google Scholar] [CrossRef]
- Cheung, O.; Kapoor, A.; Puri, P.; Sistrun, S.; Luketic, V.A.; Sargeant, C.C.; Contos, M.J.; Shiffman, M.L.; Stravitz, R.T.; Sterling, R.K.; et al. The impact of fat distribution on the severity of nonalcoholic fatty liver disease and metabolic syndrome. Hepatology 2007, 46, 1091–1100. [Google Scholar] [CrossRef]
- Yamashita, K.; Yamamoto, M.H.; Ebara, S.; Okabe, T.; Saito, S.; Hoshimoto, K.; Yakushiji, T.; Isomura, N.; Araki, H.; Obara, C.; et al. Association between increased epicardial adipose tissue volume and coronary plaque composition. Heart Vessel. 2014, 29, 569–577. [Google Scholar] [CrossRef]
- Saco-Ledo, G.; Valenzuela, P.L.; Castillo-Garcia, A.; Arenas, J.; Leon-Sanz, M.; Ruilope, L.M.; Lucia, A. Physical exercise and epicardial adipose tissue: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2021, 22, e13103. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Villasante Fricke, A.C. Effects of Semaglutide Versus Dulaglutide on Epicardial Fat Thickness in Subjects with Type 2 Diabetes and Obesity. J. Endocr. Soc. 2020, 4, 42. [Google Scholar] [CrossRef]
- Requena-Ibáñez, J.A.; Santos-Gallego, C.G.; Rodriguez-Cordero, A.; Vargas-Delgado, A.P.; Mancini, D.; Sartori, S.; Atallah-Lajam, F.; Giannarelli, C.; Macaluso, F.; Lala, A.; et al. Mechanistic Insights of Empagliflozin in Nondiabetic Patients With HFrEF: From the EMPA-TROPISM Study. JACC Heart Fail. 2021, 9, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, S.W.; Campbell, H. Comparison of reducing epicardial fat by exercise, diet or bariatric surgery weight loss strategies: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 406–415. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef]
- Elming, M.B.; Lonborg, J.; Rasmussen, T.; Kuhl, J.T.; Engstrom, T.; Vejlstrup, N.; Kober, L.; Kofoed, K.F. Measurements of pericardial adipose tissue using contrast enhanced cardiac multidetector computed tomography--comparison with cardiac magnetic resonance imaging. Int. J. Cardiovasc. Imaging 2013, 29, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Gulgun, M.; Genc, F.A. Measurement of Epicardial Fat Thickness by Echocardiography Presents Challenges. Arq. Bras. Cardiol. 2016, 107, 497–498. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Design | Country | NAFLD (n) | Control (n) | Age (yr) NAFLD | Age (yr) Control | Male NAFLD (%) | Male Control (%) | Method for NAFLD Diagnosis and/or Intrahepatic Lipid Measurement | Liver Biopsy Performed for NAFLD Severity Assessment | Method for Epicardial Fat Thickness Measurement | NOS Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Brouha, 2017 | Cross-sectional | USA | 62 | 33 | 57.4 ± 11.1 | 62.6 ± 10.3 | 51.6 | 57.6 | MRI-PDFF | N | CT | 6 |
| Cho, 2017 | Case-control | South Korea | 309 | 463 | 51.9 | 52.6 | 88.0% | 71.1 | Ultrasound | N | TTE | 7 |
| Cikim, 2007 | Cross-sectional | Turkey | 49 | 14 | - | - | 0 | 0 | Ultrasound | N | TTE | 7 |
| Colak, 2012 | Case-control | Turkey | 57 | 30 | 44.2 ± 9.4 | 42.7 ± 14.5 | 83.9 | 87.5 | Ultrasound and liver biopsy | Y | TTE | 7 |
| Fracanzani, 2016 | Cross-sectional | Italy | 512 | 0 | 61 ± 13 | - | 61.3 | - | Ultrasound and liver biopsy | Y | TTE | 7 |
| Iacobellis, 2014 | Prospective cohort study | Italy | 62 | 62 | 43.9 ± 9.3 | 44 ± 8.5 | 67.8 | 72.6 | Ultrasound | N | TTE | 9 |
| Kim, 2016 | Case-control | South Korea | 676 | 796 | 44.0 ± 8.0 | 44.3 ± 9.1 | 94.0 | 76.1 | Ultrasound | N | CT | 7 |
| Oguz, 2016 | Case-control | Turkey | 41 | 37 | 37.9 ± 8.9 | 34.5 ± 8.6 | 65.9 | 46.0 | Ultrasound | N | TTE | 7 |
| Perseghi, 2007 | Case-control | Italy | 21 | 21 | 35 ± 7 | 36 ± 7 | 100 | 100 | 1H-MRS | N | MRI | 7 |
| Psychari, 2016 | Cross-sectional | Greece | 57 | 48 | 50 ± 13 | 50 ± 15 | 61 | 56 | Ultrasound | N | TTE | 7 |
| Sunbul, 2014 | Case-control | Turkey | 100 | 50 | 44.8 ± 9.8 | 45.1 ± 6.3 | 59 | 68 | Ultrasound and liver biopsy | Y | TTE | 7 |
| Yilmaz, 2011 | Case-control | Turkey | 54 | 56 | 47 ± 10 | 46 ± 11 | 48.1 | 48.2 | Liver biopsy | Y | TTE | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orci, L.A.; Jornayvaz, F.R.; Toso, C.; Gariani, K. Systematic Review and Meta-Analysis of the Usefulness of Epicardial Fat Thickness as a Non-Invasive Marker of the Presence and Severity of Nonalcoholic Fatty Liver Disease. Biomedicines 2022, 10, 2204. https://doi.org/10.3390/biomedicines10092204
Orci LA, Jornayvaz FR, Toso C, Gariani K. Systematic Review and Meta-Analysis of the Usefulness of Epicardial Fat Thickness as a Non-Invasive Marker of the Presence and Severity of Nonalcoholic Fatty Liver Disease. Biomedicines. 2022; 10(9):2204. https://doi.org/10.3390/biomedicines10092204
Chicago/Turabian StyleOrci, Lorenzo A., François R. Jornayvaz, Christian Toso, and Karim Gariani. 2022. "Systematic Review and Meta-Analysis of the Usefulness of Epicardial Fat Thickness as a Non-Invasive Marker of the Presence and Severity of Nonalcoholic Fatty Liver Disease" Biomedicines 10, no. 9: 2204. https://doi.org/10.3390/biomedicines10092204