
Serum Iron Level and 10-Year Survival after Melanoma
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurement of Iron Level
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Vanella, V.; Festino, L.; Vitale, M.G.; Alfano, B.; Ascierto, P.A. Emerging PD-1/PD-L1 antagonists for the treatment of malignant melanoma. Expert Opin. Emerg. Drugs 2021, 26, 79–92. [Google Scholar] [CrossRef]
- Lou-Qian, Z.; Rong, Y.; Ming, L.; Xin, Y.; Feng, J.; Lin, X. The prognostic value of epigenetic silencing of p16 gene in NSCLC patients: A systematic review and meta-analysis. PLoS ONE 2013, 8, e54970. [Google Scholar] [CrossRef]
- Datz, C.; Müller, E.; Aigner, E. Iron overload and non-alcoholic fatty liver disease. Minerva Endocrinol. 2017, 42, 173–183. [Google Scholar] [CrossRef]
- Toyokuni, S. Role of iron in carcinogenesis: Cancer as a ferrotoxic disease. Cancer Sci. 2009, 100, 9–16. [Google Scholar] [CrossRef]
- Klaunig, J.E.; Kamendulis, L.M. The role of oxidative stress in carcinogenesis. Annu. Rev. Pharmacol. Toxicol. 2004, 44, 239–267. [Google Scholar] [CrossRef]
- Le Gal, K.; Ibrahim, M.X.; Wiel, C.; Sayin, V.I.; Akula, M.K.; Karlsson, C.; Dalin, M.G.; Akyürek, L.M.; Lindahl, P.; Nilsson, J.; et al. Antioxidants can increase melanoma metastasis in mice. Sci. Transl. Med. 2015, 7, 308re8. [Google Scholar] [CrossRef]
- Lee, C.K.; Jeong, S.H.; Jang, C.; Bae, H.; Kim, Y.H.; Park, I.; Kim, S.K.; Koh, G.Y. Tumor metastasis to lymph nodes requires YAP-dependent metabolic adaptation. Science 2019, 363, 644–649. [Google Scholar] [CrossRef] [Green Version]
- Piskounova, E.; Agathocleous, M.; Murphy, M.M.; Hu, Z.; Huddlestun, S.E.; Zhao, Z.; Leitch, A.M.; Johnson, T.M.; DeBerardinis, R.J.; Morrison, S.J. Oxidative stress inhibits distant metastasis by human melanoma cells. Nature 2015, 527, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Dixon, S.J.; Lemberg, K.M.; Lamprecht, M.R.; Skouta, R.; Zaitsev, E.M.; Gleason, C.E.; Patel, D.N.; Bauer, A.J.; Cantley, A.M.; Yang, W.S.; et al. Ferroptosis: An iron-dependent form of nonapoptotic cell death. Cell 2012, 149, 1060–1072. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Chen, X.B.; Ying, M.D.; He, Q.J.; Cao, J.; Yang, B. The Role of Ferroptosis in Cancer Development and Treatment Response. Front. Pharmacol. 2018, 8, 992. [Google Scholar] [CrossRef]
- Talty, R.; Bosenberg, M. The role of ferroptosis in melanoma. Pigment Cell Melanoma Res. 2022, 35, 18–25. [Google Scholar] [CrossRef]
- Cosialls, E.; El Hage, R.; Dos Santos, L.; Gong, C.; Mehrpour, M.; Hamaï, A. Ferroptosis: Cancer Stem Cells Rely on Iron until “to Die for” It. Cells 2021, 10, 2981. [Google Scholar] [CrossRef]
- Quintana Pacheco, D.A.; Sookthai, D.; Graf, M.E.; Schübel, R.; Johnson, T.; Katzke, V.A.; Kaaks, R.; Kühn, T. Iron status in relation to cancer risk and mortality: Findings from a population-based prospective study. Int. J. Cancer 2018, 143, 561–569. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, H.; Müldür, E.; Endler, G.; Hübl, W. Prevalence of iron deficiency across different tumors and its association with poor performance status, disease status and anemia. Ann. Oncol. 2013, 24, 1886–1892. [Google Scholar] [CrossRef]
- Li, Y.; Xu, W.; Chen, P.; Liao, M.; Qin, W.; Liao, W.; Huang, Z. Correlation Analysis Between Preoperative Serum Iron Level and Prognosis as Well as Recurrence of HCC After Radical Resection. Cancer Manag. Res. 2020, 12, 31–41. [Google Scholar] [CrossRef] [Green Version]
- Sukiennicki, G.M.; Marciniak, W.; Muszyńska, M.; Baszuk, P.; Gupta, S.; Białkowska, K.; Ja-worska-Bieniek, K.; Durda, K.; Lener, M.; Pietrzak, S.; et al. Iron levels, genes involved in iron metabolism and antioxidative processes and lung cancer incidence. PLoS ONE 2019, 14, e0208610. [Google Scholar] [CrossRef]
- Lin, Y.; Bao, X.; Li, J.; Pan, C.; Qian, J.; Lin, L.; Qiu, Y.; Shi, B.; Liu, F.; Chen, F.; et al. Correlation between serum iron level and overall survival of oral cancer. J. Hyg. Res. 2021, 50, 756–762. (In Chinese) [Google Scholar] [CrossRef]
- Sawayama, H.; Miyamoto, Y.; Mima, K.; Kato, R.; Ogawa, K.; Hiyoshi, Y.; Shimokawa, M.; Aki-yama, T.; Kiyozumi, Y.; Iwagami, S.; et al. Preoperative iron status is a prognosis factor for stage II and III colorectal cancer. Int. J. Clin. Oncol. 2021, 26, 2037–2045. [Google Scholar] [CrossRef]
- Wen, C.P.; Lee, J.H.; Tai, Y.P.; Wen, C.; Wu, S.B.; Tsai, M.K.; Hsieh, D.P.; Chiang, H.C.; Hsiung, C.A.; Hsu, C.Y.; et al. High serum iron is associated with increased cancer risk. Cancer Res. 2014, 74, 6589–6597. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Sempos, C.T.; Freudenheim, J.L.; Muti, P.; Smit, E. Serum iron, copper and zinc concentrations and risk of cancer mortality in US adults. Ann. Epidemiol. 2004, 14, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Chua, A.C.; Knuiman, M.W.; Trinder, D.; Divitini, M.L.; Olynyk, J.K. Higher concentrations of serum iron and transferrin saturation but not serum ferritin are associated with cancer out-comes. Am. J. Clin. Nutr. 2016, 104, 736–742. [Google Scholar] [CrossRef] [Green Version]
- Bergomi, M.; Pellacani, G.; Vinceti, M.; Bassissi, S.; Malagoli, C.; Alber, D.; Sieri, S.; Vescovi, L.; Seidenari, S.; Vivoli, R. Trace elements and melanoma. J. Trace Elem. Med. Biol. 2005, 19, 69–73. [Google Scholar] [CrossRef]
- Liu, Y.; Shou, Y.; Zhu, R.; Qiu, Z.; Zhang, Q.; Xu, J. Construction and Validation of a Ferroptosis-Related Prognostic Signature for Melanoma Based on Single-Cell RNA Sequencing. Front. Cell Dev. Biol. 2022, 10, 818457. [Google Scholar] [CrossRef]
- Liu, C.; Liu, Y.; Yu, Y.; Zhao, Y.; Yu, A. Comprehensive analysis of ferroptosis-related genes and prognosis of cutaneous melanoma. BMC Med. Genom. 2022, 15, 39. [Google Scholar] [CrossRef]
- Zeng, H.; You, C.; Zhao, L.; Wang, J.; Ye, X.; Yang, T.; Wan, C.; Deng, L. Ferroptosis-Associated Classifier and Indicator for Prognostic Prediction in Cutaneous Melanoma. J. Oncol. 2021, 2021, 3658196. [Google Scholar] [CrossRef]


{kind=link}
| Frequency | Univariable Cox Regression | Multivariable Cox Regression | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Overall, 1 n = 375 | Alive, 1 n = 344 | Deceased, 1 n = 31 | HR 2 | 95% CI 2 | p | HR | 95% CI | p |
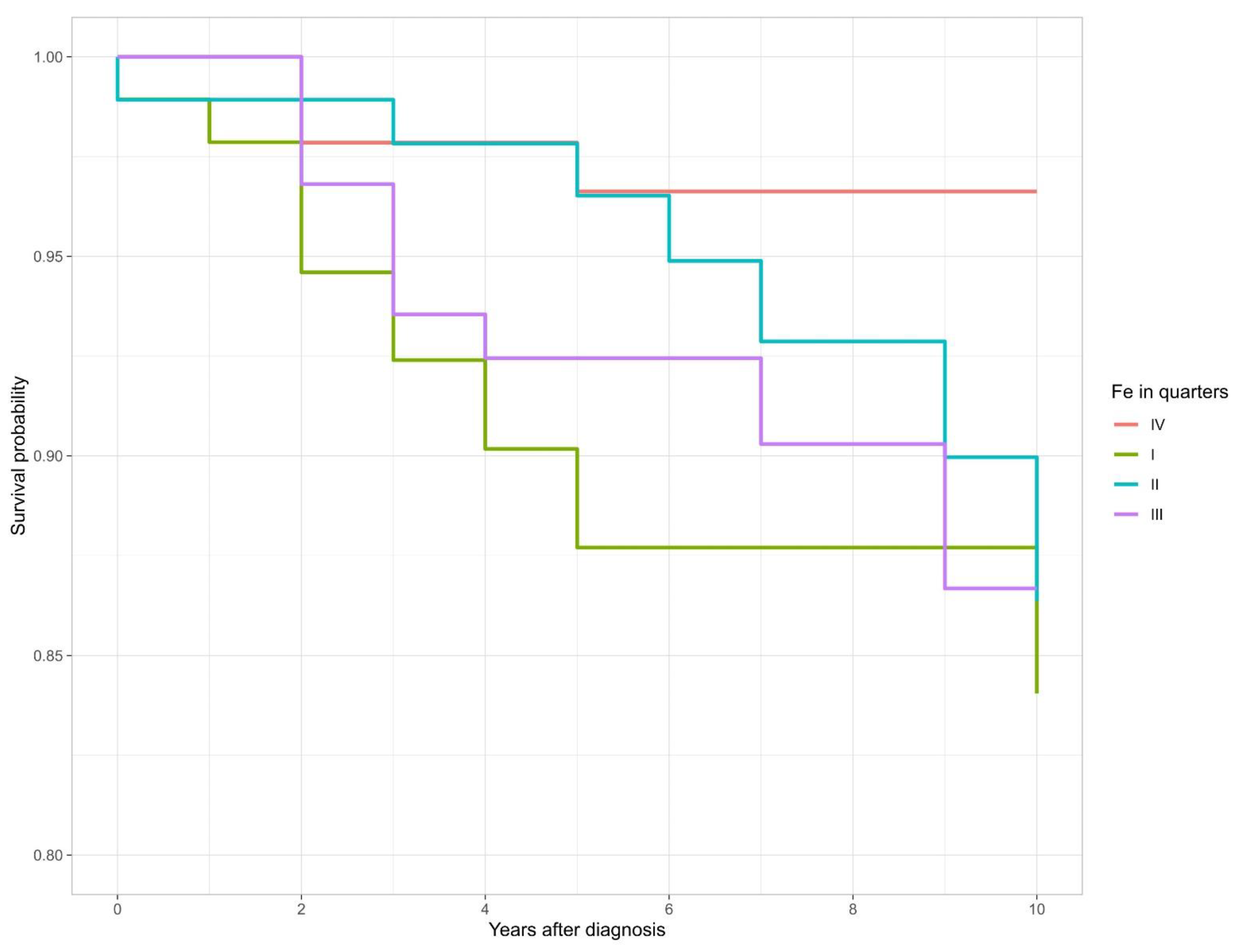
| Fe level in quarters (µg/L) | |||||||||
| I (162.15–893.05) | 94 (25%) | 82 (24%) | 12 (39%) | 4.12 | 1.16, 14.6 | 0.028 | 4.66 | 1.28, 16.9 | 0.019 |
| II (895.69–1095.88) | 93 (25%) | 86 (25%) | 7 (23%) | 2.35 | 0.61, 9.10 | 0.2 | 3.40 | 0.85, 13.6 | 0.083 |
| III (1105.49–1346.75) | 94 (25%) | 85 (25%) | 9 (29%) | 3.12 | 0.84, 11.5 | 0.088 | 3.71 | 0.99, 13.9 | 0.052 |
| IV (1348.63–2815.78) | 94 (25%) | 91 (26%) | 3 (9.7%) | — | — | — | — | ||
| Sex | |||||||||
| Female | 231 (62%) | 217 (63%) | 14 (45%) | — | — | — | — | ||
| Male | 144 (38%) | 127 (37%) | 17 (55%) | 2.09 | 1.03, 4.24 | 0.042 | 1.88 | 0.90, 3.92 | 0.092 |
| Age | 21.00–90.00 (54.63) | 21.00– 90.00 (53.76) | 38.00 – 86.00 (64.26) | 1.06 | 1.03, 1.09 | <0.001 | 1.05 | 1.02, 1.09 | <0.001 |
| Breslow (mm) * | 0.20–16.80 (1.80) | 0.20–16.80 (1.71) | 0.50–11.00 (3.22) | 1.16 | 1.04, 1.29 | 0.008 | 1.11 | 0.96, 1.28 | 0.2 |
| Clark | |||||||||
| II | 71 (19%) | 70 (20%) | 1 (3.2%) | — | — | — | — | ||
| III | 157 (42%) | 145 (42%) | 12 (39%) | 5.47 | 0.71, 42.1 | 0.10 | 4.35 | 0.56, 33.7 | 0.2 |
| IV/V | 147 (39%) | 129 (38%) | 18 (58%) | 8.76 | 1.17, 65.7 | 0.035 | 6.84 | 0.91, 51.7 | 0.062 |
| Subgroup | n | Mean | SD | Median | Min | Max | Range | IQR | |
|---|---|---|---|---|---|---|---|---|---|
| Sex | |||||||||
| Female | 231 | 1069.14 | 292.19 | 1044.88 | 162.15 | 1792.36 | 1630.21 | 395.5 | |
| Male | 144 | 1236.93 | 398.84 | 1234.28 | 369.67 | 2815.78 | 2446.11 | 526.49 | |
| Clark | |||||||||
| II | 71 | 1149.54 | 317.63 | 1156.85 | 460.85 | 2067.22 | 1606.37 | 451.18 | |
| III | 157 | 1107.69 | 318.32 | 1090.98 | 162.15 | 1934.12 | 1771.97 | 411.51 | |
| IV/V | 147 | 1153.5 | 386.68 | 1136.38 | 412.76 | 2815.78 | 2403.02 | 484.64 | |
| Fe level in quarters (µg/L) | |||||||||
| I (162.15–893.05) | 94 | 725.16 | 145.7 | 762.68 | 162.15 | 893.05 | 730.9 | 199.85 | |
| II (895.69–1095.88) | 93 | 999.41 | 59.49 | 998.63 | 895.69 | 1095.88 | 200.19 | 102.3 | |
| III (1105.49–1346.75) | 94 | 1228.17 | 68.56 | 1232.03 | 1105.49 | 1346.75 | 241.26 | 122.53 | |
| IV (1348.63–2815.78) | 94 | 1580.12 | 236.59 | 1529.21 | 1348.63 | 2815.78 | 1467.15 | 217.96 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowińska, K.; Baszuk, P.; Rogoża-Janiszewska, E.; Deptuła, J.; Marciniak, W.; Derkacz, R.; Lener, M.; Cybulski, C.; Kiedrowicz, M.; Boer, M.; et al. Serum Iron Level and 10-Year Survival after Melanoma. Biomedicines 2022, 10, 3018. https://doi.org/10.3390/biomedicines10123018
Rowińska K, Baszuk P, Rogoża-Janiszewska E, Deptuła J, Marciniak W, Derkacz R, Lener M, Cybulski C, Kiedrowicz M, Boer M, et al. Serum Iron Level and 10-Year Survival after Melanoma. Biomedicines. 2022; 10(12):3018. https://doi.org/10.3390/biomedicines10123018
Chicago/Turabian StyleRowińska, Karolina, Piotr Baszuk, Emilia Rogoża-Janiszewska, Jakub Deptuła, Wojciech Marciniak, Róża Derkacz, Marcin Lener, Cezary Cybulski, Magdalena Kiedrowicz, Magdalena Boer, and et al. 2022. "Serum Iron Level and 10-Year Survival after Melanoma" Biomedicines 10, no. 12: 3018. https://doi.org/10.3390/biomedicines10123018