
Comparison of Three Video Laryngoscopes and Direct Laryngoscopy for Emergency Endotracheal Intubation While Wearing PPE-AGP: A Randomized, Crossover, Simulation Trial
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
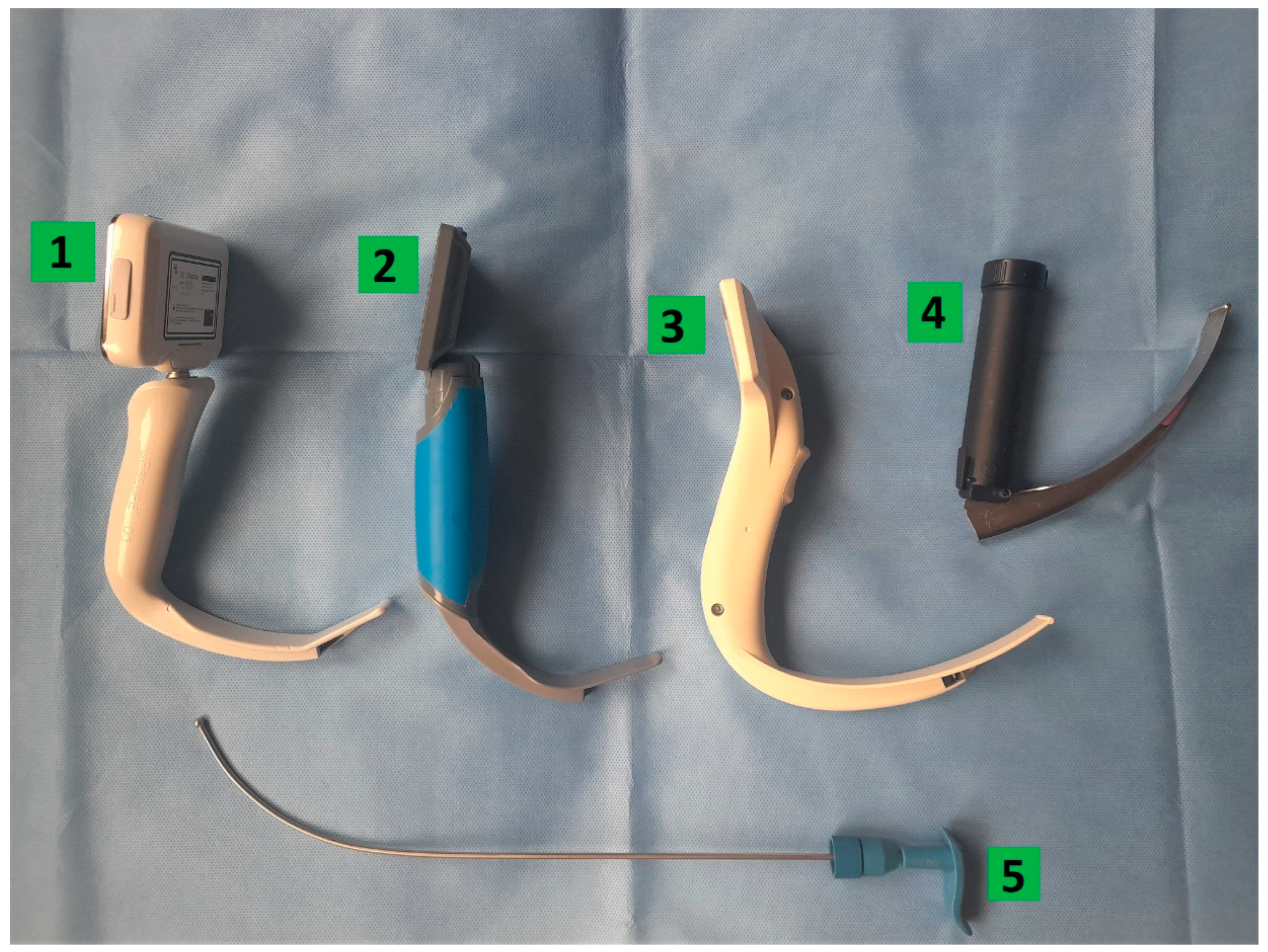
2.1. Direct Laryngoscopy
2.2. I-ViewTM Video Laryngoscope
2.3. ProVu® Video Laryngoscope
2.4. UESCOPE® Video Laryngoscope
2.5. Statistical Methods
2.6. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Technical Guidance: Infection Prevention and Control. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/infection-prevention-and-control (accessed on 26 June 2022).
- Schumacher, J.; Carvalho, C.; Greig, P.; Ragbourne, S.; Ahmad, I. Influence of respiratory protective equipment on simulated advanced airway skills by specialist tracheal intubation teams during the COVID-19 pandemic. Trends Anaesth. Crit. Care 2021, 39, 21–27. [Google Scholar] [CrossRef]
- Wei, H.; Jiang, B.; Behringer, E.C.; Hofmeyr, R.; Myatra, S.N.; Wong, D.T.; Sullivan, E.P.O.; Hagberg, C.A.; McGuire, B.; Baker, P.A.; et al. Controversies in airway management of COVID-19 patients: Updated information and international expert consensus recommendations. Br. J. Anaesth. 2021, 126, 361–366. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Weaver, K.R.; Barr, G.C., Jr.; Long, K.R.; Diaz, L., Jr.; Ratner, A.S.; Reboul, J.P.; Sturm, D.A.; Greenberg, M.R.; Dusza, S.W.; Glenn-Porter, B.; et al. Comparison of airway intubation devices when using a biohazard suit: A feasibility study. Am. J. Emerg. Med. 2015, 33, 810–814. [Google Scholar] [CrossRef]
- Zhang, J.; Sun, M.; Li, N.; Suo, X.; Xia, Z.; Zuo, M.; Liu, R. Acquired infection after intubating patients with COVID-19: A retrospective pilot study. J. Clin. Anesth. 2020, 67, 110006. [Google Scholar] [CrossRef]
- El-Boghdadly, K.; Wong, D.J.N.; Owen, R.; Neuman, M.D.; Pocock, S.; Carlisle, J.B.; Johnstone, C.; Andruszkiewicz, P.; Baker, P.A.; Biccard, B.M.; et al. Risks to healthcare workers following tracheal intubation of patients with COVID-19: A prospective international multicentre cohort study. Anaesthesia 2020, 75, 1437–1447. [Google Scholar] [CrossRef]
- Schumacher, J.; Arlidge, J.; Garnham, F.; Ahmad, I. A randomised crossover simulation study comparing the impact of chemical, biological, radiological or nuclear substance personal protection equipment on the performance of advanced life support in-terventions. Anaesthesia 2017, 72, 592–597. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, J.; Arlidge, J.; Dudley, D.; Sicinski, M.; Ahmad, I. The impact of respiratory protective equipment on difficult airway management: A randomised, crossover, simulation study. Anaesthesia 2020, 75, 1301–1306. [Google Scholar] [CrossRef]
- Castle, N.; Pillay, Y.; Spencer, N. Insertion of six different supraglottic airway devices whilst wearing chemical, biological, radiation, nuclear-personal protective equipment: A manikin study. Anaesthesia 2011, 66, 983–988. [Google Scholar] [CrossRef]
- Fullerton, J.N.; Roberts, K.J.; Wyse, M. Can experienced paramedics perform tracheal intubation at cardiac arrests? Five years experience of a regional air ambulance service in the UK. Resuscitation 2009, 80, 1342–1345. [Google Scholar] [CrossRef]
- Raatiniemi, L.; Länkimäki, S.; Martikainen, M. Pre-hospital airway management by non-physicians in Northern Finland-a cross-sectional survey. Acta Anaesthesiol. Scand. 2013, 57, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Ludwin, K.; Bialka, S.; Czyzewski, L.; Smereka, J.; Dabrowski, M.; Dabrowska, A.; Ladny, J.R.; Ruetzler, K.; Szarpak, L. Video laryngoscopy for endotracheal intubation of adult patients with suspected/ confirmed COVID-19. A systematic review and meta-analysis of randomized controlled trials. Disaster Emerg. Med. J. 2020, 5, 85–97. [Google Scholar] [CrossRef]
- Benoit, J.L.; Gerecht, R.B.; Steuerwald, M.T.; McMullan, J. Endotracheal intubation versus supraglottic airway placement in out-of-hospital cardiac arrest: A meta-analysis. Resuscitation 2015, 93, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.E.; Schmicker, R.H.; Daya, M.R.; Stephens, S.W.; Idris, A.H.; Carlson, J.N.; Colella, M.R.; Herren, H.; Hansen, M.; Richmond, N.J.; et al. Effect of a Strategy of Initial Laryngeal Tube Insertion vs. Endotracheal Intubation on 72-Hour Survival in Adults with Out-of-Hospital Cardiac Arrest A Randomized Clinical Trial. JAMA 2018, 320, 769–778. [Google Scholar] [CrossRef] [Green Version]
- McMullan, J.; Gerecht, R.; Bonomo, J.; Robb, R.; McNally, B.; Donnelly, J.; Wang, H.E. Airway management and out-of-hospital cardiac arrest outcome in the CARES registry. Resuscitation 2014, 85, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Behrens, N.H.; Fischer, M.; Krieger, T.; Monaco, K.; Wnent, J.; Seewald, S.; Grasner, J.T.; Bernhard, M. Effect of airway man-agement strategies during resuscitation from out-of-hospital cardiac arrest on clinical outcome: A registry-based analysis. Re-suscitation 2020, 152, 157–164. [Google Scholar]
- Ahmad, I.; Onwochei, D.N.; Muldoon, S.; Keane, O.; El-Boghdadly, K. Airway management research: A systematic review. Anaesthesia 2019, 74, 225–236. [Google Scholar] [CrossRef] [Green Version]
- Gadek, L.; Szarpak, L.; Konge, L.; Dabrowski, M.; Telecka-Gadek, D.; Maslanka, M.; Drela, W.L.; Jachowicz, M.; Iskrzycki, L.; Bialka, S.; et al. Direct vs. Video-Laryngoscopy for Intubation by Paramedics of Simulated COVID-19 Patients under Cardio-pulmonary Resuscitation: A Randomized Crossover Trial. J. Clin. Med. 2021, 10, 5740. [Google Scholar] [CrossRef]
- Shin, D.H.; Choi, P.C.; Na, J.U.; Cho, J.H.; Han, S.K. Utility of the Pentax-AWS in performing tracheal intubation while wearing chemical, biological, radiation and nuclear personal protective equipment: A randomised crossover trial using a manikin. Emerg. Med. J. 2013, 30, 527–531. [Google Scholar] [CrossRef]
- Pantazopoulos, I.; Kolonia, K.; Laou, E.; Mermiri, M.; Tsolaki, V.; Koutsovasilis, A.; Zakynthinos, G.; Gourgoulianis, K.; Arnaoutoglou, E.; Chalkias, A. Video Laryngoscopy Improves Intubation Times with Level C Personal Protective Equipment in Novice Physicians: A Randomized Cross-Over Manikin Study. J. Emerg. Med. 2021, 60, 764–771. [Google Scholar] [CrossRef]
- Kim, D.S.; Jeong, D.; Park, J.E.; Lee, G.T.; Shin, T.G.; Chang, H.; Kim, T.; Lee, S.U.; Yoon, H.; Cha, W.C.; et al. Endotracheal Intubation Using C-MAC Video Laryngoscope vs. Direct Laryngoscope While Wearing Personal Protective Equipment. J. Pers. Med. 2022, 12, 1720. [Google Scholar] [CrossRef] [PubMed]
- Yousif, S.; Machan, J.T.; Alaska, Y.; Suner, S. Airway Management in Disaster Response: A Manikin Study Comparing Direct and Video Laryngoscopy for Endotracheal Intubation by Prehospital Providers in Level C Personal Protective Equipment. Prehospital Disaster Med. 2017, 32, 352–356. [Google Scholar] [CrossRef]
- Sule, H.; Kulkarni, M.; Sugalski, G.; Murano, T. Maintenance of Skill Proficiency for Emergency Skills with and without Adjuncts despite the Use of Level C Personal Protective Equipment. Cureus 2020, 12, 7433. [Google Scholar] [CrossRef] [Green Version]
- Goh, Q.; Lie, S.; Tan, Z.; Tan, P.; Ng, S.; Abdullah, H. Time to intubation with McGrath™ videolaryngoscope versus direct laryngoscope in powered air-purifying respirator: A randomised controlled trial. Singap. Med. J. 2021. [Google Scholar] [CrossRef]
- Pieters, B.M.A.; Wilbers, N.E.R.; Huijzer, M.; Winkens, B.; Van Zundert, A.A.J. Comparison of seven videolaryngoscopes with the Macintosh laryngoscope in manikins by experienced and novice personnel. Anaesthesia 2016, 71, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maassen, R.; van Zundert, A. Comparison of the C-MAC® vidolaryngoscope with the Macintosh, Glidescope® and Airtraq® laryngoscopes in easy and difficult laryngoscopy scenarios in manikins. Anaesthesia 2010, 65, 955–956. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
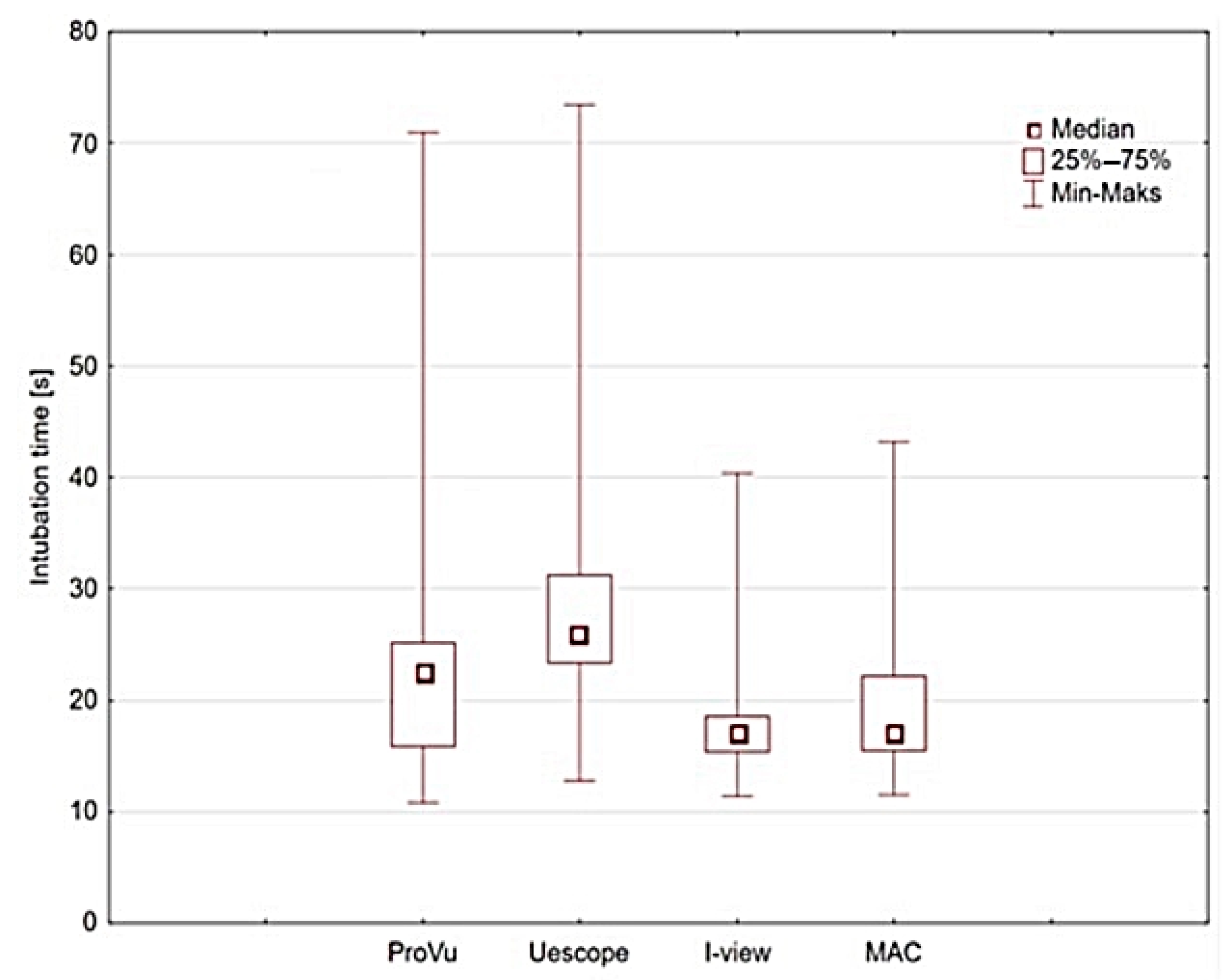
| Video Laryngoscope Type | Median | Mean | Minimum | Maximum | Lower Quartile | Upper Quartile | Standard Deviation |
|---|---|---|---|---|---|---|---|
| ProVu® | 27.7 | 28.8 | 11.8 | 70.5 | 19.7 | 29.8 | 9.2 |
| UESCOPE® | 29.4 | 28.1 | 12.8 | 73.4 | 22.3 | 33.9 | 10.1 |
| I-view | 17.4 | 16.0 | 10.3 | 40.8 | 14.3 | 17.5 | 4.6 |
| MAC | 17.9 | 16.1 | 10.5 | 43.2 | 14.4 | 22.2 | 5.2 |
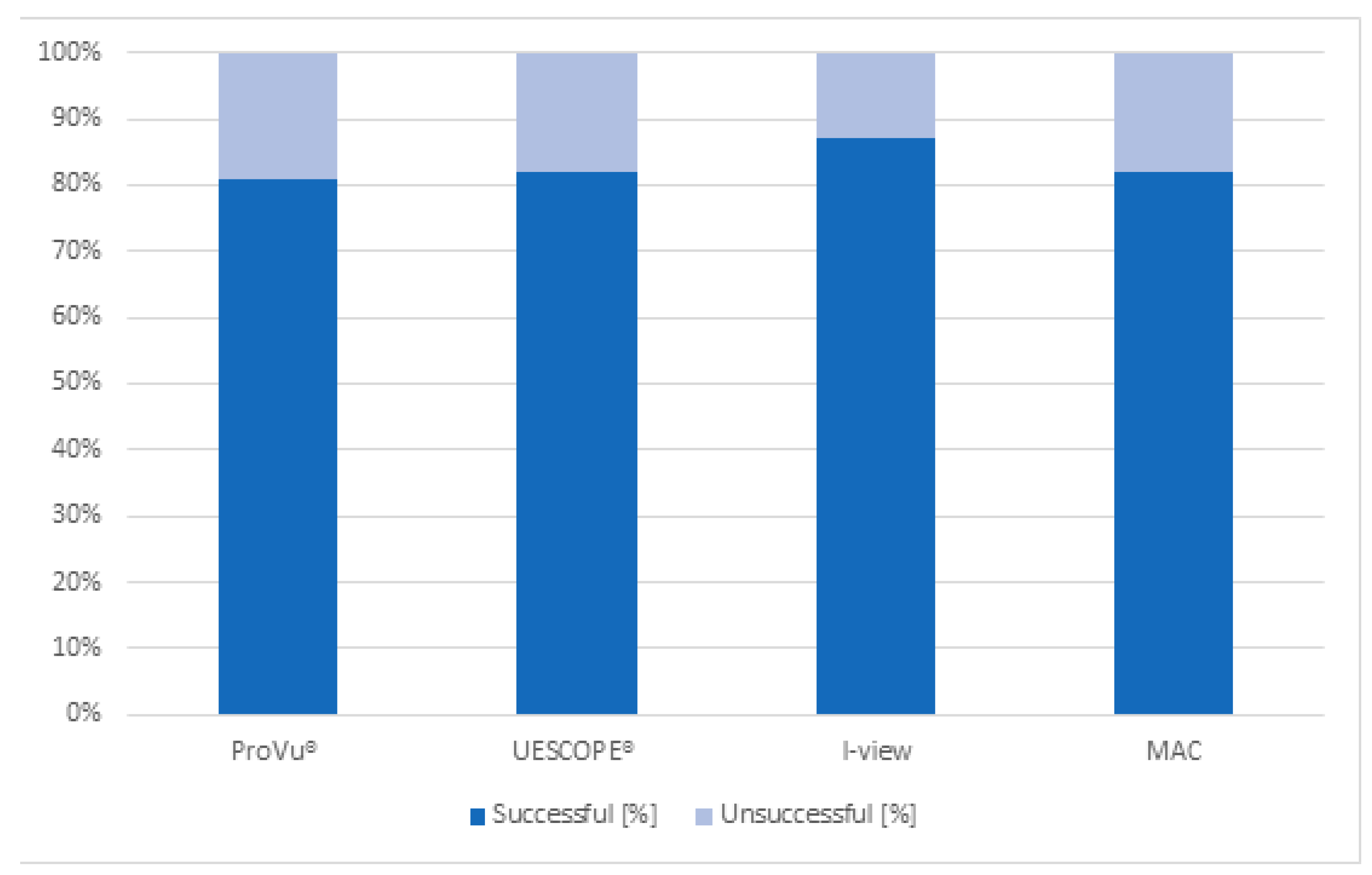
| Video Laryngoscope Type | Successful | Unsuccessful | ||
|---|---|---|---|---|
| Number | Percentage | Number | Percentage | |
| ProVu® | 43 | 81.1% | 10 | 18.9% |
| UESCOPE® | 44 | 83.0% | 9 | 17.0% |
| I-view | 47 | 88.6% | 6 | 11.4% |
| MAC | 45 | 84.9% | 7 | 15.1% |
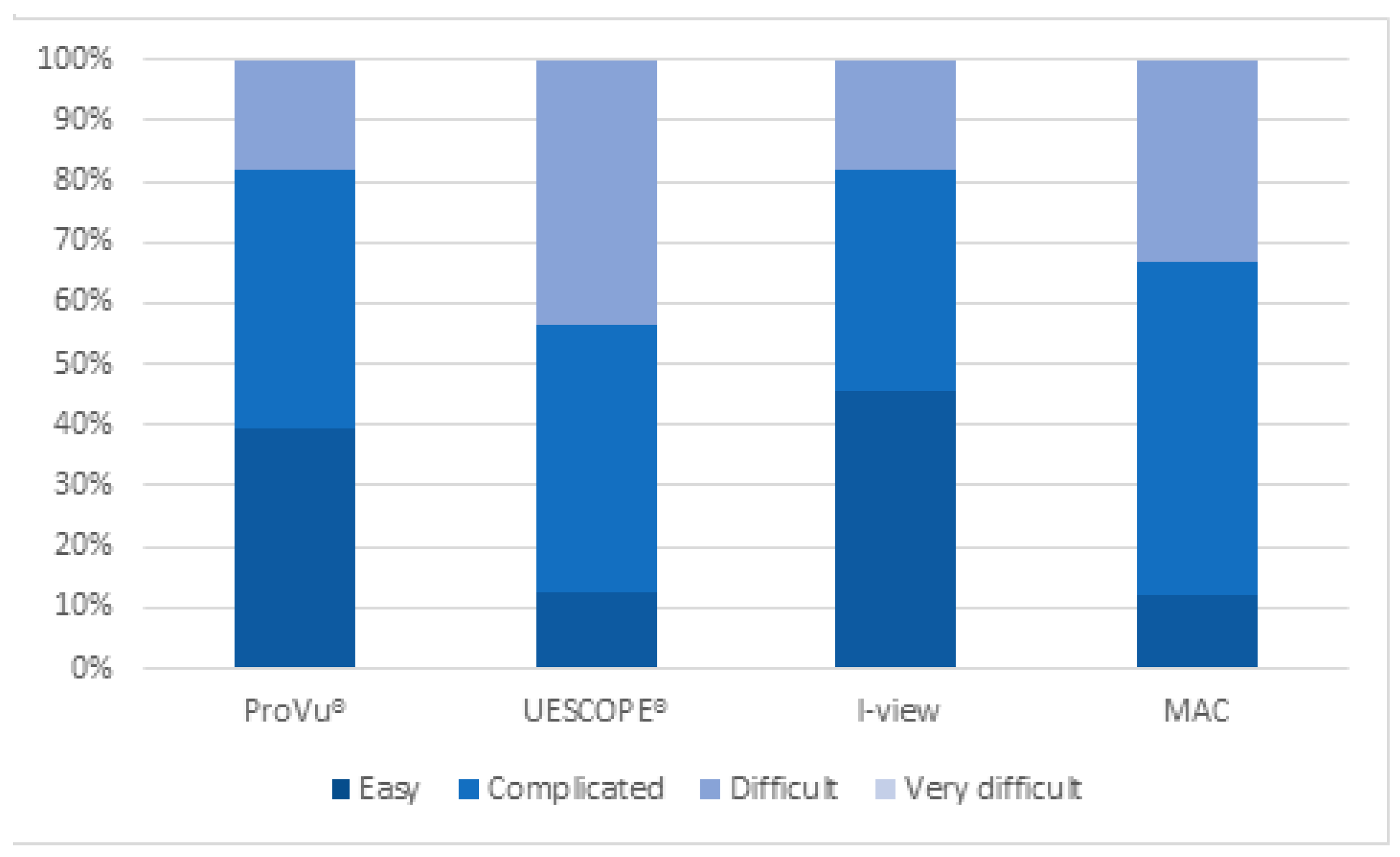
| Video Laryngoscope Type | Difficulty Level | |||||||
|---|---|---|---|---|---|---|---|---|
| Easy | Complicated | Difficult | Very Difficult | |||||
| Number | Percentage | Number | Percentage | Number | Percentage | Number | Percentage | |
| ProVu® | 21 | 39.6% | 22 | 41.6% | 10 | 18.8% | 0 | 0% |
| UESCOPE® | 7 | 13.2% | 22 | 41.6% | 24 | 45.2% | 0 | 0% |
| I-view | 24 | 45.2% | 20 | 37.9% | 9 | 16.9% | 0 | 0% |
| MAC | 6 | 11.3% | 29 | 54.7% | 18 | 34.0% | 0 | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kluj, P.; Fedorczak, A.; Fedorczak, M.; Gaszyński, T.; Kułak, C.; Wasilewski, M.; Znyk, M.; Bartczak, M.; Ratajczyk, P. Comparison of Three Video Laryngoscopes and Direct Laryngoscopy for Emergency Endotracheal Intubation While Wearing PPE-AGP: A Randomized, Crossover, Simulation Trial. Healthcare 2023, 11, 884. https://doi.org/10.3390/healthcare11060884
Kluj P, Fedorczak A, Fedorczak M, Gaszyński T, Kułak C, Wasilewski M, Znyk M, Bartczak M, Ratajczyk P. Comparison of Three Video Laryngoscopes and Direct Laryngoscopy for Emergency Endotracheal Intubation While Wearing PPE-AGP: A Randomized, Crossover, Simulation Trial. Healthcare. 2023; 11(6):884. https://doi.org/10.3390/healthcare11060884
Chicago/Turabian StyleKluj, Przemysław, Anna Fedorczak, Michał Fedorczak, Tomasz Gaszyński, Cezary Kułak, Mikołaj Wasilewski, Mateusz Znyk, Maria Bartczak, and Paweł Ratajczyk. 2023. "Comparison of Three Video Laryngoscopes and Direct Laryngoscopy for Emergency Endotracheal Intubation While Wearing PPE-AGP: A Randomized, Crossover, Simulation Trial" Healthcare 11, no. 6: 884. https://doi.org/10.3390/healthcare11060884