
Clinically Preferred Videolaryngoscopes in Airway Management: An Updated Systematic Review

Abstract
:1. Introduction
- Higher first-pass success: VLs increased the chance of first-pass success (successful intubation on first attempt) when compared to DLs.
- Fewer failed intubations: VLs resulted in fewer failed intubations when compared to DLs, even in anticipated difficult airways.
- Fewer hypoxemic events: VLs showed a reduction in hypoxemic events when compared to DLs.
- Increased glottic views: certain VLs provided an improved visualisation of the glottis in accordance with the Cormack–Lehane grade, which can reduce the likelihood of adverse events such as failed intubation or airway trauma.
- Less sore throat: there was a lower incidence of patient-reported sore throat post-intubation using VLs, hence possibly reducing patient anxiety with intubation.
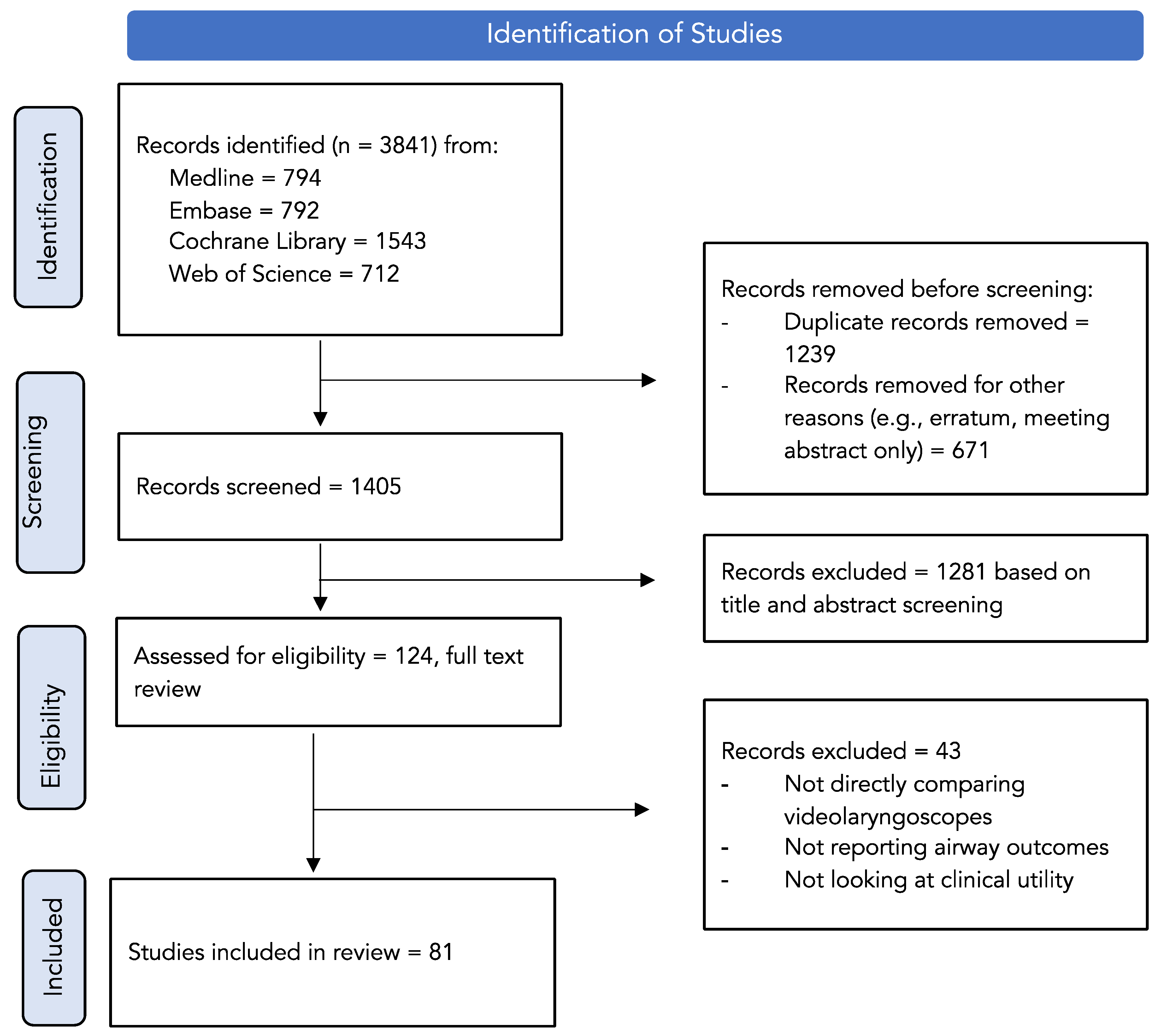
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, J.M.; Ma, E.L.; Wu, Q.P.; Tian, M.; Sun, Y.Y.; Lin, J.; Peng, L.; Xu, Q.; Wei, W.; Tan, H.; et al. Effectiveness and Safety of a Novel Approach for Management of Patients with Potential Difficult Mask Ventilation and Tracheal Intubation: A Multi-center Randomized Trial. Chin. Med. J. 2018, 131, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Landefeld, K.R.; Koike, S.; Ran, R.; Semler, M.W.; Barnes, C.; Stempek, S.B.; Janz, D.R.; Rice, T.W.; Russell, D.W.; Self, W.H.; et al. Effect of Laryngoscope Blade Size on First Pass Success of Tracheal Intubation in Critically Ill Adults. Crit. Care Explor. 2023, 5, e0855. [Google Scholar] [CrossRef] [PubMed]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst. Rev. 2022, 4, CD011136. [Google Scholar] [CrossRef] [PubMed]
- McClelland, G.; Smith, M.B. Just a routine operation: A critical discussion. J. Perioper. Pract. 2016, 26, 114–117. [Google Scholar] [CrossRef]
- Detsky, M.E.; Jivraj, N.; Adhikari, N.K.; Friedrich, J.O.; Pinto, R.; Simel, D.L.; Wijeysundera, D.N.; Scales, D.C. Will This Patient Be Difficult to Intubate?: The Rational Clinical Examination Systematic Review. JAMA 2019, 321, 493–503. [Google Scholar] [CrossRef]
- Norskov, A.K.; Wetterslev, J.; Rosenstock, C.V.; Afshari, A.; Astrup, G.; Jakobsen, J.C.; Thomsen, J.L.; Bottger, M.; Ellekvist, M.; Schousboe, B.M.; et al. Effects of using the simplified airway risk index vs usual airway assessment on unanticipated difficult tracheal intubation—A cluster randomized trial with 64,273 participants. Br. J. Anaesth. 2016, 116, 680–689. [Google Scholar] [CrossRef]
- van Zundert, A.; Town, C.; Dagleish, L.; Reynolds, H. Which Videolaryngoscope Should We Use in Airway Management? J. Anesth. Perioper. Med. 2016, 3, 247–257. [Google Scholar] [CrossRef]
- Al-Ghamdi, A.A.; El Tahan, M.R.; Khidr, A.M. Comparison of the Macintosh, GlideScope R, Airtraq R, and King VisionTM laryngoscopes in routine airway management. Minerva Anestesiol. 2016, 82, 1278–1287. [Google Scholar]
- Alvis, B.D.; Hester, D.; Watson, D.; Higgins, M.; St Jacques, P. Randomized controlled trial comparing the McGrath MAC video laryngoscope with the King Vision video laryngoscope in adult patients. Minerva Anestesiol. 2016, 82, 30–35. [Google Scholar]
- Wan, L.; Liao, M.; Li, L.; Qian, W.; Hu, R.; Chen, K.; Zhang, C.; Yao, W. McGrath Series 5 videolaryngoscope vs Airtraq DL videolaryngoscope for double-lumen tube intubation: A randomized trial. Medicine 2016, 95, e5739. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Doley, K.; Athar, M.; Raza, N.; Siddiqi, O.A.; Ali, S. Comparison of endotracheal intubation time in neutral position between C-Mac® and Airtraq® laryngoscopes: A prospective randomised study. Indian J. 2017, 61, 338–343. [Google Scholar] [CrossRef]
- Belze, O.; Lepage, E.; Bazin, Y.; Kerourin, P.; Fusciardi, J.; Remerand, F.; Espitalier, F. Glidescope versus Airtraq DL for double-lumen tracheal tube insertion in patients with a predicted or known difficult airway: A randomised study. Eur. J. Anaesthesiol. 2017, 34, 456–463. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Buttenberg, M.; Greif, R.; Nabecker, S.; Theiler, L. Evaluation of three unchannelled videolaryngoscopes and the Macintosh laryngoscope in patients with a simulated difficult airway: A randomised, controlled trial. Anaesthesia 2017, 72, 370–378. [Google Scholar] [CrossRef]
- Lee, J.; Kwak, H.J.; Lee, J.Y.; Chang, M.Y.; Lee, S.Y.; Kim, J.Y. Comparison of the Pentax AirwayScope and McGrath MAC videolaryngoscope for endotracheal intubation in patients with a normal airway. Medicine 2017, 96, e8713. [Google Scholar] [CrossRef] [PubMed]
- Raza, N.; Hasan, M.; Ahmed, S.M.; Bano, S.; Athar, M. A comparative study of McGrath and Airtraq videolaryngoscopes for tracheal intubation. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Sato Boku, A.; Sobue, K.; Kako, E.; Tachi, N.; Okumura, Y.; Kanazawa, M.; Hashimoto, M.; Harada, J. The usefulness of the McGrath MAC laryngoscope in comparison with Airwayscope and Macintosh laryngoscope during routine nasotracheal intubation: A randomaized controlled trial. BMC Anesthesiol. 2017, 17, 160. [Google Scholar] [CrossRef]
- Shravanalakshmi, D.; Bidkar, P.U.; Narmadalakshmi, K.; Lata, S.; Mishra, S.K.; Adinarayanan, S. Comparison of intubation success and glottic visualization using King Vision and C-MAC videolaryngoscopes in patients with cervical spine injuries with cervical immobilization: A randomized clinical trial. Surg. Neurol. Int. 2017, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Kumar, N.; Jain, A. A randomised trial to compare Truview PCD®, C-MAC® and Macintosh laryngoscopes in paediatric airway management. Asian J. Anesthesiol. 2017, 55, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Tseng, K.Y.; Lu, I.C.; Shen, Y.C.; Lin, C.H.; Chen, P.N.; Cheng, K.I. A comparison of the video laryngoscopes with Macintosh laryngoscope for nasotracheal intubation. Asian J. Anesthesiol. 2017, 55, 17–21. [Google Scholar] [CrossRef]
- Vadi, M.G.; Roddy, K.J.; Ghazal, E.A.; Um, M.; Neiheisel, A.J.; Applegate, R.L., 2nd. Comparison of the GlideScope Cobalt R and Storz DCI R Video Laryngoscopes in Children Younger Than 2 Years of Age During Manual In-Line Stabilization: A Randomized Trainee Evaluation Study. Pediatr. Emerg. Care 2017, 33, 467–473. [Google Scholar] [CrossRef]
- Vargas, M.; Pastore, A.; Aloj, F.; Laffey, J.G.; Servillo, G. A comparison of videolaryngoscopes for tracheal intubation in predicted difficult airway: A feasibility study. BMC Anesthesiol. 2017, 17, 25. [Google Scholar] [CrossRef] [PubMed]
- Abdelgalel, E.F.; Mowafy, S.M.S. Comparison between Glidescope, Airtraq and Macintosh laryngoscopy for emergency endotracheal intubation in intensive care unit: Randomized controlled trial. Egypt. J. Anaesth. 2018, 34, 123–128. [Google Scholar] [CrossRef]
- Ajimi, J.; Nishiyama, J.; Masuda, R.; Shibata, T.; Suzuki, T. Airtraq DL and AWS-200 for Double-lumen Endotracheal Tube Intubation: A Prospective Randomized Clinical Trial. Tokai J. Exp. Clin. Med. 2018, 43, 161–167. [Google Scholar] [PubMed]
- Cavus, E.; Janssen, S.; Reifferscheid, F.; Caliebe, A.; Callies, A.; von der Heyden, M.; Knacke, P.G.; Doerges, V. Videolaryngoscopy for Physician-Based, Prehospital Emergency Intubation: A Prospective, Randomized, Multicenter Comparison of Different Blade Types Using A.P. Advance, C-MAC System, and KingVision. Anesth. Analg. 2018, 126, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Chanchayanon, T.; Saewong, L. Comparison of glidescope and McGrath video laryngoscope for intubation and adverse events by anesthetic residents. J. Med. Assoc. Thail. 2018, 101, 803–807. [Google Scholar]
- El-Tahan, M.R.; Khidr, A.M.; Gaarour, I.S.; Alshadwi, S.A.; Alghamdi, T.M.; Al’ghamdi, A. A Comparison of 3 Videolaryngoscopes for Double-Lumen Tube Intubation in Humans by Users With Mixed Experience: A Randomized Controlled Study. J. Cardiothorac. Vasc. Anesth. 2018, 32, 277–286. [Google Scholar] [CrossRef]
- Gupta, A.; Kamal, G.; Gupta, A.; Sehgal, N.; Bhatla, S.; Kumar, R. Comparative evaluation of CMAC and Truview picture capture device for endotracheal intubation in neonates and infants undergoing elective surgeries: A prospective randomized control trial. Paediatr. Anaesth. 2018, 28, 1148–1153. [Google Scholar] [CrossRef]
- Mendonca, C.; Ungureanu, N.; Nowicka, A.; Kumar, P. A randomised clinical trial comparing the ‘sniffing’ and neutral position using channelled (KingVision®) and non-channelled (C-MAC®) videolaryngoscopes. Anaesthesia 2018, 73, 847–855. [Google Scholar] [CrossRef]
- Mishra, G.; Philip, V.M.; Kumar, V.R.H.; Sivashanmugam, T. Suitability of Nasotracheal Intubation using King Vision and TruviewPCD Video Laryngoscopes: A Randomized Clinical Trial. Anesth. Essays Res. 2018, 12, 581–585. [Google Scholar] [CrossRef]
- Yoo, J.Y.; Chae, Y.J.; Lee, Y.B.; Kim, S.; Lee, J.; Kim, D.H. A comparison of the Macintosh laryngoscope, McGrath video laryngoscope, and Pentax Airway Scope in paediatric nasotracheal intubation. Sci. Rep. 2018, 8, 17365. [Google Scholar] [CrossRef]
- Akbas, S.; Ozkan, A.S.; Karaaslan, E. A Comparison of McGrath MAC Versus C-MAC Videolaryngoscopes in Morbidly Obese Patients Undergoing Bariatric Surgery: A Randomized, Controlled Clinical Trial. Bariatr. Surg. Pract. Patient Care 2019, 14, 25–33. [Google Scholar] [CrossRef]
- Blajic, I.; Hodzovic, I.; Lucovnik, M.; Mekis, D.; Novak-Jankovic, V.; Stopar Pintaric, T. A randomised comparison of C-MACTM and King Vision R videolaryngoscopes with direct laryngoscopy in 180 obstetric patients. Int. J. Obstet. Anesth. 2019, 39, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Chae, Y.J.; Kim, D.H.; Park, E.J.; Oh, J.; Yi, I.K. A comparison of McGrath MAC, Pentax AWS, and Macintosh direct laryngoscopes for nasotracheal intubation: A randomized controlled trial. Ther. Clin. Risk Manag. 2019, 15, 1121–1128. [Google Scholar] [CrossRef]
- Markham, T.H.; Nwokolo, O.O.; Guzman-Reyes, S.; Medina-Rivera, G.; Gumbert, S.D.; Cai, C.; Burnett, T.; Syed, T.A.; Hagberg, C.A. A comparison of the king vision® and glidescope® video intubation systems in patients at risk for difficult intubation. Trends Anaesth. Crit. Care 2019, 28, 27–35. [Google Scholar] [CrossRef]
- Roh, G.U.; Kwak, H.J.; Lee, K.C.; Lee, S.Y.; Kim, J.Y. Randomized comparison of McGrath MAC videolaryngoscope, Pentax Airway Scope, and Macintosh direct laryngoscope for nasotracheal intubation in patients with manual in-line stabilization. Can. J. Anaesth. 2019, 66, 1213–1220. [Google Scholar] [CrossRef]
- Sahajanandan, R.; Dhanyee, A.S.; Gautam, A.K. A comparison of King vision video laryngoscope with CMAC D-blade in obese patients with anticipated difficult airway in tertiary hospital in India—Randomized control study. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Kusunoki, S.; Tanigawa, K.; Shime, N. Comparison of three video laryngoscopes and direct laryngoscopy for emergency endotracheal intubation: A retrospective cohort study. BMJ Open 2019, 9, e024927. [Google Scholar] [CrossRef]
- Zhu, H.; Liu, J.; Suo, L.; Zhou, C.; Sun, Y.; Jiang, H. A randomized controlled comparison of non-channeled king vision, McGrath MAC video laryngoscope and Macintosh direct laryngoscope for nasotracheal intubation in patients with predicted difficult intubations. BMC Anesthesiol. 2019, 19, 166. [Google Scholar] [CrossRef]
- Brozek, T.; Bruthans, J.; Porizka, M.; Blaha, J.; Ulrichova, J.; Michalek, P. A Randomized Comparison of Non-Channeled GlidescopeTM Titanium Versus Channeled KingVisionTM Videolaryngoscope for Orotracheal Intubation in Obese Patients with BMI > 35 kg.m−2. Diagnostics 2020, 10, 1024. [Google Scholar] [CrossRef]
- Huang, P.; Zhou, R.; Lu, Z.; Hang, Y.; Wang, S.; Huang, Z. GlideScope R versus C-MAC R(D) videolaryngoscope versus Macintosh laryngoscope for double lumen endotracheal intubation in patients with predicted normal airways: A randomized, controlled, prospective trial. BMC Anesthesiol. 2020, 20, 119. [Google Scholar] [CrossRef]
- Kaur, G.; Gupta, S.; Mehta, N.; Dhingra, J.S. Comparative Evaluation of McGrath MAC, Truview Video Laryngoscopes and Macintosh Laryngoscope for Endotracheal Intubation in Patients Undergoing Surgery under General Anaesthesia. Anesth. Essays Res. 2020, 14, 20–24. [Google Scholar] [CrossRef]
- Pappu, A.; Sharma, B.; Jain, R.; Dua, N.; Sood, J. A randomised comparative study of “videoendoscope” with the Truview EVO2, C-MAC D blade videolaryngoscope and the Macintosh laryngoscope. Indian J. Anaesth. 2020, 64, S186–S192. [Google Scholar] [CrossRef]
- Sen, R.; Mallepally, A.R.; Sakrikar, G.; Marathe, N.; Rathod, T. Comparison of TruView and King Vision video laryngoscopes in subaxial cervical spine injury: A randomized controlled trial. Surg. Neurol. Int. 2020, 11, 375. [Google Scholar] [CrossRef]
- Chandrashekaraiah, M.M.; Sahitya, V.A.; Narayan, P.; Adeel, S. Simulated difficult airway: Cmac d blade or glidescope? Sri Lankan J. Anaesthesiol. 2021, 29, 7–12. [Google Scholar] [CrossRef]
- Chandy, J.; Pillai, R.; Mathew, A.; Philip, A.V.; George, S.P.; Sahajanandan, R. A randomized clinical trial comparing the King Vision (channeled blade) and the CMAC (D blade) videolaryngoscopes in patients with cervical spine immobilization. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Singh, P.; Gupta, N.; Kumar Malhotra, R.; Girdhar, K.K. Comparative efficacy of C-MACR Miller videolaryngoscope versus McGrathR MAC size “1” videolaryngoscope in neonates and infants undergoing surgical procedures under general anesthesia: A prospective randomized controlled trial. Paediatr. Anaesth. 2021, 31, 1089–1096. [Google Scholar] [CrossRef]
- Mani, N.; Palanisamy, N.; Zachariah, M.; George, S.K.; Dsilva, A.A.; Johns, J.R. C-MAC D-blade vs airtraq for intubation with manual inline axial stabilisation—A randomised clinical trial. J. Clin. Diagn. Res. 2021, 15, UC01–UC04. [Google Scholar] [CrossRef]
- Sepmiko, J.; Senapathi, T.G.A.; Wiryana, M.; Kurniyanta, I.P.; Widnyana, I.M.G.; Sutawan, I.B.K.J. The efficacy of O-Mac®, patent video laryngoscope, and conventional laryngoscope for intubation in the operating room. Open Access Maced. J. Med. Sci. 2021, 9, 646–650. [Google Scholar] [CrossRef]
- Sultana, F.; Nikhar, S.A.; Durga, P. Comparison of Macintosh laryngoscope, non- channelled (C-MAC video-laryngoscope) and channelled laryngoscope (Airtraq) for intubation in lateral position—A prospective randomized controlled study. Trends Anaesth. Crit. Care 2021, 40, 30–34. [Google Scholar] [CrossRef]
- Teo, R.; Mian, N.; Masri, S.N.N.S.; Mahdi, S.N.M.; Nie, Y.C.; Nor, N.M. Glidescope® versus c-mac® video laryngoscopy in pediatric intubation. Does time matter? Iran. J. Pediatr. 2021, 31, e108316. [Google Scholar] [CrossRef]
- Gupta, N.; Sarma, R.; Vig, S.; Kumar, V.; Gupta, A.; Mishra, S. Comparison of C-MAC and McGrathMAC Videolaryngoscopes for Intubation in Patients with Normal Airway by Donned Anaesthesiologists Using an Intubation Box During COVID-19 Pandemic: A Prospective, Randomized Study. Turk. J. Anaesthesiol. Reanim. 2022, 50, 255–260. [Google Scholar] [CrossRef]
- Haldar, R.; Kannaujia, A.K.; Shamim, R.; Mishra, P. A comparison of endotracheal intubation characteristics between Macintosh, CMAC, and Smart Trach Video laryngoscope: A randomized prospective clinical trial. Expert Rev. Med. Devices 2022, 19, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Jayadi, J.; Veterini, A.S.; Kusuma, E.; Waloejo, C.S.; Airlangga, P.S.; Semedi, B.P. Comparison of Effectiveness between Wycope Video Laryngoscope, C-MAC Video Laryngoscope, and Direct Laryngoscope in Intubation of Elective Surgery Patients. Acta Med. 2022, 51, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Karadag Erkoc, S.; Yildirim Guclu, C.; Buyuk, S.; Bermede, O.; Erkent, F.D.; Yilmaz, A.A. Comparison of C-MAC vs. McGrath video laryngoscopes on glottic exposure and endotracheal intubation success with stylet usage in obese patients. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5763–5773. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Taluja, A.; Saxena, B.; Dwivedi, P. A Comparative Evaluation of 2 Videolaryngoscopes as an Intubation Aid in a Simulated Difficult Airway: A Prospective Randomised Study. Turk. J. Anaesthesiol. Reanim. 2022, 50, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Suryatheja, R.; Sinha, R.; Kumar, K.R.; Ranjan Ray, B.; Chowhan, M.G.; Pandey, R.K.; Darlong, V.; Punj, J. Comparison of time to intubate and intubation conditions with CMAC Miller blade size 1 and CMAC Macintosh blade size 2 in pediatric patients-A prospective randomized controlled study. Trends Anaesth. Crit. Care 2022, 45, 46–51. [Google Scholar] [CrossRef]
- Zhang, J.; Tan, L.Z.; Toh, H.; Foo, C.W.; Wijeratne, S.; Hu, H.; Seet, E. Comparing the first-attempt tracheal intubation success of the hyperangulated McGrath R X-blade vs the Macintosh-type CMAC videolaryngoscope in patients with cervical immobilization: A two-centre randomized controlled trial. J. Clin. Monit. Comput. 2022, 36, 1139–1145. [Google Scholar] [CrossRef]
- Altun, D.; Ozkan-Seyhan, T.; Orhan-Sungur, M.; Sivrikoz, N.; Camci, E. Comparison of 4 Laryngoscopes in 2 Difficult Airway Scenarios: A Randomized Crossover Simulation-Based Study. Simul. Healthc. 2016, 11, 304–308. [Google Scholar] [CrossRef]
- Arslan, Z.I.; Turna, C.; Gumus, N.E.; Toker, K.; Solak, M. Intubation of a Paediatric Manikin in Tongue Oedema and Face-to-Face Simulations by Novice Personnel: A Comparison of Glidescope, Airtraq and Direct Laryngoscopy. Turk. J. Anaesthesiol. Reanim. 2016, 44, 71–75. [Google Scholar] [CrossRef]
- El-Tahan, M.R.; Al’ghamdi, A.A.; Khidr, A.M.; Gaarour, I.S. Comparison of three videolaryngoscopes for double-lumen tubes intubation in simulated easy and difficult airways: A randomized trial. Minerva Anestesiol. 2016, 82, 1050–1058. [Google Scholar] [CrossRef]
- Hippard, H.K.; Kalyani, G.; Olutoye, O.A.; Mann, D.G.; Watcha, M.F. A comparison of the Truview PCD and the GlideScope Cobalt AVL video-laryngoscopes to the Miller blade for successfully intubating manikins simulating normal and difficult pediatric airways. Paediatr. Anesth. 2016, 26, 613–620. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, K.R.; Hong, D.Y.; Baek, K.J.; Lee, Y.H.; Park, S.O. Efficacy of various types of laryngoscope (direct, Pentax Airway Scope and GlideScope) for endotracheal intubation in various cervical immobilisation scenarios: A randomised cross-over simulation study. BMJ Open 2016, 6, e011089. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Lee, Y.; Kim, C.; Lim, T.H.; Oh, J.; Kang, H.; Lee, S. Comparison of the Pentax Airwayscope, Glidescope Video Laryngoscope, and Macintosh Laryngoscope during Chest Compression According to Bed Height. Medicine 2016, 95, e2631. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, T.; Shiga, T.; Homma, Y.; Koyama, Y.; Goto, T. Comparison of the force applied on oral structures during intubation attempts by novice physicians between the Macintosh direct laryngoscope, Airway Scope and C-MAC PM: A high-fidelity simulator-based study. BMJ Open 2016, 6, e011039. [Google Scholar] [CrossRef] [PubMed]
- Schroder, H.; Zoremba, N.; Rossaint, R.; Deusser, K.; Stoppe, C.; Coburn, M.; Rieg, A.; Schalte, G. Intubation performance using different laryngoscopes while wearing chemical protective equipment: A manikin study. BMJ Open 2016, 6, e010250. [Google Scholar] [CrossRef]
- Shin, M.; Bai, S.J.; Lee, K.Y.; Oh, E.; Kim, H.J. Comparing McGRATH R MAC, C-MAC R, and Macintosh Laryngoscopes Operated by Medical Students: A Randomized, Crossover, Manikin Study. Biomed. Res. Int. 2016, 2016, 8943931. [Google Scholar] [CrossRef]
- Hodnick, R.; Zitek, T.; Galster, K.; Johnson, S.; Bledsoe, B.; Ebbs, D. A Comparison of Paramedic First Pass Endotracheal Intubation Success Rate of the VividTrac VT-A 100, GlideScope Ranger, and Direct Laryngoscopy Under Simulated Prehospital Cervical Spinal Immobilization Conditions in a Cadaveric Model. Prehospital Disaster Med. 2017, 32, 621–624. [Google Scholar] [CrossRef]
- Lee, S.; Kang, H.; Oh, J.; Lim, T.H.; Lee, Y.; Kim, C. Comparison of pentax-AWS®, Glidescope®, and King Vision® for diff icult-airway intubation in manikins model by paramedics. Hong Kong J. Emerg. Med. 2017, 24, 237–243. [Google Scholar] [CrossRef]
- Owada, G.; Mihara, T.; Inagawa, G.; Asakura, A.; Goto, T.; Ka, K. A comparison of the Airtraq R, McGrath R, and Macintosh laryngoscopes for difficult paediatric intubation: A manikin study. PLoS ONE 2017, 12, e0171889. [Google Scholar] [CrossRef]
- Kriege, M.; Pirlich, N.; Ott, T.; Wittenmeier, E.; Dette, F. A comparison of two hyperangulated video laryngoscope blades to direct laryngoscopy in a simulated infant airway: A bicentric, comparative, randomized manikin study. BMC Anesthesiol. 2018, 18, 119. [Google Scholar] [CrossRef]
- Oshika, H.; Koyama, Y.; Taguri, M.; Maruyama, K.; Hirabayashi, G.; Yamada, S.M.; Kohno, M.; Andoh, T. Supraglottic airway device versus a channeled or non-channeled blade-type videolaryngoscope for accidental extubation in the prone position: A randomized crossover manikin study. Medicine 2018, 97, e11190. [Google Scholar] [CrossRef] [PubMed]
- Chew, S.H.; Lim, J.Z.M.; Chin, B.Z.B.; Chan, J.X.; Siew, R.C.H. Intubation with channeled versus non-channeled video laryngoscopes in simulated difficult airway by junior doctors in an out-of-hospital setting: A crossover manikin study. PLoS ONE 2019, 14, e0224017. [Google Scholar] [CrossRef]
- Desai, N.; Johnson, M.; Priddis, K.; Ray, S.; Chigaru, L. Comparative evaluation of AirtraqTM and GlideScope® videolaryngoscopes for difficult pediatric intubation in a Pierre Robin manikin. Eur. J. Pediatr. 2019, 178, 1105–1111. [Google Scholar] [CrossRef]
- Raimann, F.J.; Tepperis, D.M.; Meininger, D.; Zacharowski, K.; Schalk, R.; Byhahn, C.; Weber, C.F.; Mutlak, H. Comparing Four Video Laryngoscopes and One Optical Laryngoscope with a Standard Macintosh Blade in a Simulated Trapped Car Accident Victim. Emerg. Med. Int. 2019, 2019, 9690839. [Google Scholar] [CrossRef] [PubMed]
- Gaszynski, T.M. A Comparison of a Standard Macintosh Blade Laryngoscope, Pentax-AWS Videolaryngoscope and Intubrite Videolaryngoscope for Tracheal Intubation in Manikins in Sitting and Prone Positions: A Randomized Cross-Over Study. Diagnostics 2020, 10, 603. [Google Scholar] [CrossRef] [PubMed]
- Moritz, A.; Leonhardt, V.; Prottengeier, J.; Birkholz, T.; Schmidt, J.; Irouschek, A. Comparison of Glidescope® GoTM, King VisionTM, Dahlhausen VL, I-ViewTM and Macintosh laryngoscope use during difficult airway management simulation by experienced and inexperienced emergency medical staff: A randomized crossover manikin study. PLoS ONE 2020, 15, e0236474. [Google Scholar] [CrossRef]
- Romito, J.W.; Riccio, C.A.; Bagley, C.A.; Minhajuddin, A.; Barden, C.B.; Michael, M.M.; Bhoja, R.; Mootz, B.L.; Skrivanek, G.D.; Klein, K.W.; et al. Cervical Spine Movement in a Cadaveric Model of Severe Spinal Instability: A Study Comparing Tracheal Intubation with 4 Different Laryngoscopes. J. Neurosurg. Anesthesiol 2020, 32, 57–62. [Google Scholar] [CrossRef]
- Votruba, J.; Brozek, T.; Blaha, J.; Henlin, T.; Vymazal, T.; Donaldson, W.; Michalek, P. Video Laryngoscopic Intubation Using the King VisionTM Laryngoscope in a Simulated Cervical Spine Trauma: A Comparison Between Non-Channeled and Channeled Disposable Blades. Diagnostics 2020, 10, 139. [Google Scholar] [CrossRef] [PubMed]
- Yi, I.K.; Kwak, H.J.; Lee, K.C.; Lee, J.H.; Min, S.K.; Kim, J.Y. Comparison of McGrath, Pentax, and Macintosh laryngoscope in normal and cervical immobilized manikin by novices: A randomized crossover trial. Eur. J. Med. Res. 2020, 25, 35. [Google Scholar] [CrossRef]
- Ataman, A.K.; Altıntas, E. Comparison of a commercial 3D fabricated laryngoscope (Airangel®) with a widely-used video laryngoscope (Glidescope®): Randomized controlled cross-over study. Trends Anaesth. Crit. Care 2021, 40, 35–40. [Google Scholar] [CrossRef]
- Decamps, P.; Grillot, N.; Le Thuaut, A.; Brule, N.; Lejus-Bourdeau, C.; Reignier, J.; Lascarrou, J.B. Comparison of four channelled videolaryngoscopes to Macintosh laryngoscope for simulated intubation of critically ill patients: The randomized MACMAN2 trial. Ann. Intensive Care 2021, 11, 126. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Trikha, A.; Ayub, A.; Bhattacharjee, S.; Aravindan, A.; Gupta, N.; Prakash, K.; Aggarwal, R.; Ganesh, V.; Soni, K.D.; et al. Comparison of KingVision videolaryngoscope channelled blade with Tuoren videolaryngoscope non-channelled blade in a simulated COVID-19 intubation scenario by non-anaesthesiologists and experienced anaesthesiologists: A prospective randomised crossover mannequin study. Trends Anaesth. Crit. Care 2021, 38, 42–48. [Google Scholar] [CrossRef]
- Moritz, A.; Holzhauser, L.; Fuchte, T.; Kremer, S.; Schmidt, J.; Irouschek, A. Comparison of Glidescope Core, C-MAC Miller and conventional Miller laryngoscope for difficult airway management by anesthetists with limited and extensive experience in a simulated Pierre Robin sequence: A randomized crossover manikin study. PLoS ONE 2021, 16, e0250369. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.H.; Wagner, E.M.; Hu, J.S.; Tobin, M.R.; Cronin, A.J.; Couperus, K.S.; April, M.D.; Schauer, S.G.; Naylor, J.F. New Versus Old, The i-View Video Laryngoscope Versus the GlideScope: A Prospective, Randomized, Crossover Trial. Med. J. 2021, 81–89. Available online: https://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med19&AN=34449866 (accessed on 20 August 2023).
- Vig, S.; Bhan, S.; Gupta, N.; Meena, J.; Bhatnagar, S. Comparison of Mc Grath-MAC and C-MAC video laryngoscopes for intubation in a COVID simulated mannequin by novice users wearing face protective gear: A randomized crossover trial. Saudi J. Anaesth. 2021, 15, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Kabra, P.; Mandal, S.; Gupta, A.; Sarma, R.; Malhotra, R.K. Comparative evaluation of King Vision videolaryngoscope channeled and non-channeled blades with direct laryngoscope for intubation performance and skill retention by medical students: A randomized cross over two period study. J. Clin. Monit. Comput. 2022, 18, 18. [Google Scholar] [CrossRef]
- Er, A.; Caglar, A.; Citlenbik, H.; Akgul, F.; Ulusoy, E.; Oren, H.; Yiotalmaz, D.; Duman, M. Which Device Is Favorable for Intubation Attempts of Pediatric Residents on Four Different Pediatric Airway Simulations? Pediatr. Emerg. Care 2022, 38, e272–e277. [Google Scholar] [CrossRef]
- Kumar, B.; Ratre, B.K.; Garg, R.; Meena, J.K.; Singh, R.; Bhatnagar, S. Comparison between C-MAC and King Vision video laryngoscope (channelled blade) for tracheal intubation in aerosol-prevention intubation box for COVID-19 patients: A manikin-based study. Indian J. 2022, 66, 187–192. [Google Scholar] [CrossRef]
- Karalapillai, D.; Darvall, J.; Mandeville, J.; Ellard, L.; Graham, J.; Weinberg, L. A review of video laryngoscopes relevant to the intensive care unit. Indian J. Crit. Care Med. 2014, 18, 442–452. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Manufacturer | Address | Videolaryngoscope | Blade Type |
|---|---|---|---|
| AirAngelBlade.org, AirAngel Project Online 3D-Printed Videolaryngoscopes | USA | AirAngel blade 3D-printed | Non-channelled, Acute-angled |
| Airlangga university | Surbaya, Indonesia | Wycope | Non-channelled, Acute-angled |
| Dahlhausen | Köln, Germany | Dahlhausen | Non-channelled, Macintosh |
| Industry Design Registration of Indonesia: HKI. KI.05.01.02.P00202101656 and A00202100589 | Indonesia | O-Mac | Non-channelled, Macintosh |
| Intersurgical | Berkshire, United Kingdom | I-view | Non-Channelled, Macintosh |
| Karl Storz | Tuttlingen, Germany | DCI; C-MAC; C-MAC D-blade; C-MAC Pocket Monitor; CMAC Miller blade | Non-channelled, Macintosh, Miller and Acute-angled |
| King Systems Ambu, A/S | Ballerup, Denmark | King Vision VL channelled; non-channelled; aBlade channelled; aBLade non-channelled; Paediatric aBlade | Channelled/Non-channelled, Acute-angled |
| Medtronic Operational Headquarters | Minneaopolis, USA | McGrath Mac, McGrath Mac X-Blade | Non-channelled, Macintosh and acute-angulated |
| Pentax-AWS, Hoya Corporation | Tokyo, Japan | Pentax Airway Scope | Channelled |
| Prodol Meditec S.A. | Vizcaya, Spain | Airtraq; Airtraq double lumen | Channelled |
| Salter Labs | California, USA | Intubrite | Non-channelled, Macintosh |
| Smart Trach Medicare | Lucknow, India | Smart Trach | Non-channelled, Acute-angled |
| Soma Technology International | Bloomfield, USA | McGRATH Series 5 | Non-channelled, Acute-angled |
| Truphatek International ltd. | Netanya, Israel | TruView; Truview EVO2; Truview PCD | Non-channelled, Acute-angled |
| Tuoren Medical | Henan, China | TUORen | Non-channelled, Macintosh |
| Venner Medical | Kiel, Germany | Venner APA channelled; non-channelled | Channelled/Non-channelled, Macintosh and Acute-angled |
| Verathon Medical | Bothell, WA, USA | GlideScope; GlideScope Cobalt; Glidescope Advanced Video Laryngoscope | Non-channelled, Acute-angled |
| Vivid Medical | Palo Alto, CA, USA | VividTrac VT-A100 | Channelled |
| Year | First Author | No. of Patients | Setting | Intubator | Number and Types of Videolaryngoscopes Used | Outcomes Based On: A: Improved Glottis View B: Faster Time to Successful Intubation C: Higher First Attempt Intubation Success D: Less Use of Manoeuvres or Adjuncts E: Other | Clinically Preferred Videolaryngoscope | Blade Type of Most-Preferred VL |
|---|---|---|---|---|---|---|---|---|
| 2016 | Al-Ghamdi [8] | 86 | Surgical | Anaesthetists | 3: GS, AT, KV-C | A: Equal B: GS > KV-C > AT C: Equal D: Equal E: Less sore throat in AT and KV-C than GS | GS for primary outcomes | Non-channelled, Acute-angled |
| 2016 | Alvis [9] | 64 | Surgical | Anaesthetic Staff | 2: McGrath Mac, KV-C | A: Equal B: McGrath Mac C: McGrath Mac D: Equal | McGrath Mac | Non-channelled, Macintosh |
| 2016 | Wan [10] | 90 | Double Lumen Tube Surgical | Anaesthetists | 2: McGrath Series 5 (Acute), AT-DL | A: Equal B: AT C: Equal D: Equal | AT | Channelled |
| 2017 | Ahmed [11] | 60 | Surgical Difficult patients in Neutral Position | Anaesthetists | 2: CMAC, AT | A: Equal B: CMAC C: Equal D: Equal E: Less haemodynamic changes in CMAC | CMAC | Non-channelled, Macintosh |
| 2017 | Belze [12] | 72 | Double Lumen Tube Surgical with difficult airway | Anaesthetists | 2: GS, AT | A: Equal B: Equal C: Equal D: Equal | GS = AT | GS = Non-channelled, Acute-angled AT = Channelled |
| 2017 | Kleine-Brueggeney [13] | 480 | Surgical | Anaesthetists | 3: KV-NC, AT, APA | A: KV-NC > AT > APA B: AT > KV-NC > APA C: KV-NC > AT > APA D: - | KV-NC | Non-channelled, Acute-angled |
| 2017 | Lee [14] | 140 | Surgical | Anaesthetists | 2: McGrath Mac, AWS | A: AWS B: Equal C: Equal D: Equal | AWS | Channelled |
| 2017 | Raza [15] | 60 | Surgical | Anaesthetists | 2: AT, McGrath | A: Equal B: AT C: Equal D: - | AT | Channelled |
| 2017 | Sato Boku [16] | 60 | Surgical Nasotracheal Intubation | Anaesthetists | 2: McGrath Mac, AWS | A: Equal B: McGrath Mac C: Equal D: Equal | McGrath Mac | Non-channelled, Macintosh |
| 2017 | Shravanalakshmi [17] | 135 | Surgical with Cervical Spine Immobilisation | Anaesthetists | 3: CMAC, CMAC-D, KV-NC | A: KV-NC > CMAC-D B: CMAC > CMAC-D C: Equal D: Equal E: Ease of Laryngoscope insertion CMAC > KV-NC > CMAC-D | CMAC | Non-channelled, Macintosh |
| 2017 | Singh [18] | 150 | Paediatric Surgical | Anaesthetists | 2: CMAC, TV-PCD | A: TV-PCD B: CMAC C: Equal D: TV-PCD | TV-PCD | Non-channelled, Acute-angled |
| 2017 | Tseng [19] | 105 | Surgical Nasotracheal Intubation | Anaesthetists | 2: GS, AWS | A: Equal B: Equal C: Equal D: Equal | GS = AWS | GS = Non-channelled, Acute-angled AWS = Channelled |
| 2017 | Vadi [20] | 93 | Paediatric Surgical with Cervical Spine Immobilisation | Anaesthetic Trainees | 2: GS-Cobalt, DCI | A: Equal B: Equal C: Equal D: - | GS-Cobalt = DCI | GS = Non-channelled, Acute-angled DCI = Non-channelled, Macintosh |
| 2017 | Vargas [21] | 42 | Surgical Difficult Airway | Anaesthetists | 2: Imago-V-C, GS | A: Equal B: Equal C: Equal D: Imago-V E: Less force required with Imago-V-C | Imago-V-C | Channelled |
| 2018 | Abdelgalel [22] | 120 | Intensive Care Unit | ICU Physicians | 2: GS, AT | A: Equal B: Equal C: Equal D: - | GS = AT | GS = Non-channelled, Acute-angled AT = Channelled |
| 2018 | Ajimi [23] | 60 | Double Lumen Tube Surgical | Anaesthetists | 2: AT, AWS | A: Equal B: AT C: Equal D: - | AT | Channelled |
| 2018 | Cavus [24] | 168 | Pre-hospital | Emergency Physicians | 3: CMAC-PM, KV-C, APA | A: Equal B: Equal C: CMAC-PM + APA > KV-C D: - E: Handling concerns with KV-C | CMAC-PM + APA | CMAC-PM = Non-channelled, Acute-angled APA = Non-channelled, Macintosh |
| 2018 | Chanchayanon [25] | 40 | Surgical | Anaesthetic Residents | 2: GS, McGrath Series 5 (Acute) | A: Equal B: GS C: Equal D:- | GS | Non-channelled, Acute-angled |
| 2018 | El-Tahan [26] | 133 | Double Lumen Tube Surgical | Anaesthetists | 3: GS, AT, KV-C | A: Equal B: AT > GS C: Equal D: AT > GS | AT | Channelled |
| 2018 | Gupta [27] | 80 | Surgical Neonates and Infants | Anaesthetists | 2: CMAC-Miller, TV-PCD | A: Equal B: CMAC-Miller C: CMAC-Miller D: AT > GS | CMAC-Miller | Non-channelled, Miller |
| 2018 | Mendonca [28] | 200 | Surgical Neutral and ‘Sniffing’ | Anaesthetists | 2: KV-C, CMAC-D | A: KV-C > CMAC-D in Neutral B: Equal C: Equal D: - E: Modified Difficult Intubation Score Equal | KV-C | Channelled |
| 2018 | Mishra [29] | 80 | Nasotracheal Intubation Surgical | Anaesthetists | 2: KV-NC, TV-PCD | A: Equal B: Equal C: Equal D: Equal | KV-NC = TV-PCD | KV-NC = Non-channelled, Acute-angled TV-PCD = Non-channelled, Acute-angled |
| 2018 | Yoo [30] | 106 | Paediatric Nasotracheal Intubation | Anaesthetists | 2: AWS, McGrath Mac | A: Equal B: Equal C: Equal D: Equal | AWS = McGrath Mac | AWS = Channelled McGrath Mac = Non-channelled Macintosh |
| 2019 | Akbas [31] | 80 | Morbidly Obese Surgical | Anaesthetists | 2: McGrath Mac, CMAC | A: Equal B: CMAC C: Equal D: Equal E: Better Haemodynamic Response in CMAC | CMAC | Non-channelled, Macintosh |
| 2019 | Blajic [32] | 180 | Obstetric Caesareans | Anaesthetists | 2: CMAC, KV-C | A: KV-C B: Equal C: Equal D: CMAC E: Easier to use | CMAC | Non-channelled, Macintosh |
| 2019 | Chae [33] | 123 | Nasotracheal Intubation Surgical | Anaesthetists | 2: AWS, McGrath Mac | A: McGrath Mac B: Equal C: Equal D: Equal | McGrath Mac | Non-channelled, Macintosh |
| 2019 | Markham [34] | 225 | Anticipated Difficult Airway Surgical | Anaesthetic Residents | 3: GS-AVL, KV-C, KV-NC | A: Equal B: Equal C: GS-AVL + KV-NC > KV-C D: Equal | GS-AVL + KV-NC | GS-AVL = Non-channelled, Acute-angled KV-NC = Non-channelled, Acute-angled |
| 2019 | Roh [35] | 120 | Nasotracheal Intubation with Manual In-line Stabilisation Surgical | Anaesthetists | 2: AWS, McGrath Mac | A: Equal B: McGrath Mac C: Equal D: Equal E: Less Bleeding McGrath Mac | McGrath Mac | Non-channelled, Macintosh |
| 2019 | Sahajanandan [36] | 63 | Anticipated Difficult Airway in Obese Patients Surgical | Anaesthetists | 2: KV-C, CMAC-D | A: Equal B: Equal C: CMAC-D D: - | CMAC-D | Non-channelled, Acute-angled |
| 2019 | Suzuki [37] | 287 | Emergency Intubation Emergency Department and Intensive Care Unit | Emergency Physicians, Intensive Care Physicians, Anaesthetists and Residents | 3: KV-C, AWS, McGrath Mac | A: - B: Equal C: AWS + McGrath Mac > KV-C D: - | AWS + McGrath Mac | AWS = Channelled McGrath Mac = Non-channelled, Macintosh |
| 2019 | Zhu [38] | 94 | Nasotracheal Intubation Anticipated Difficult Airway | Anaesthetists | 2: KV-NC, McGrath Mac (acute) | A: Equal B: Equal C: Equal D: Equal | KV-NC = McGrath Mac | Non-channelled, Acute-angled McGrath Mac = Non-channelled, Macintosh |
| 2020 | Brozek [39] | 110 | Obese Patients Surgical | Anaesthetists | 2: KV-C, GS | A: Equal B: Equal C: GS D: Equal | GS | Non-channelled, Acute-angled |
| 2020 | Huang [40] | 89 | Double Lumen Tube Surgical | Anaesthetists | 2: GS, CMAC-D | A: CMAC-D B: CMAC-D C: Equal D: CMAC-D | CMAC-D | Non-channelled, Acute-angled |
| 2020 | Kaur [41] | 120 | Surgical | Anaesthetists | 2: McGrath Mac, TV | A: Equal B: Equal C: Equal D: Equal | McGrath Mac = TV | McGrath Mac = Non-channelled, Macintosh TV = Non-channelled, Acute-angled |
| 2020 | Pappu [42] | 120 | Surgical Difficult Airway | Anaesthetists | 2: TV-EVO2, CMAC-D | A: Equal B: CMAC-D C: - D: CMAC-D | CMAC-D | Non-channelled, Acute-angled |
| 2020 | Sen [43] | 60 | Surgical with Cervical Spine Immobilisation | Anaesthetists | 2: TV, KV-NC | A: Equal B: KV-NC C: Equal D:- E: Easier Intubation with KV-NC | KV-NC | Non-channelled, Acute-angled |
| 2021 | Chandrashekaraiah [44] | 60 | Surgical | Anaesthetists | 2: GS, CMAC-D | A: Equal B: GS C: Equal D: - | GS | Non-channelled, Acute-angled |
| 2021 | Chandy [45] | 100 | Surgical with Cervical Spine Immobilisation | Anaesthetists | 2: KV-C, CMAC-D | A: - B: Equal C: Equal D: KV-C E: KV-C Easier | KV-C | Channelled |
| 2021 | Gupta [46] | 140 | Neonates and Infants Surgical | Anaesthetists | 2: CMAC-Miller, McGrath Mac | A: CMAC-Miller B: Equal C: Equal D: - | CMAC-Miller | Non-channelled, Miller |
| 2021 | Mani [47] | 116 | Surgical with Manual In-line Stabilisation | Anaesthetists | 2: CMAC-D, AT | A: Equal B: Equal C: Equal D: CMAC-D | CMAC-D | Non-channelled, Acute-angled |
| 2021 | Sepmiko [48] | 270 | Surgical | Anaesthetists | 2: O-Mac, McGrath Mac | A: Equal B: O-Mac C: O-Mac D: O-Mac | O-Mac | Non-channelled, Macintosh |
| 2021 | Sultana [49] | 120 | Surgical in Lateral Position | Anaesthetists | 2: CMAC, AT | A: Equal B: CMAC C: Equal D: Equal | CMAC | Non-channelled, Macintosh |
| 2021 | Teo [50] | 65 | Surgical | Anaesthetists | 2: CMAC, GS | A: Equal B: CMAC > GS C: Equal D: Equal | CMAC | Non-channelled, Macintosh |
| 2022 | Gupta [51] | 60 | Surgical | Anaesthetists (COVID PPE) | 2: CMAC, McGrath Mac | A: Equal B: Equal C: Equal D: Equal | CMAC = McGrath Mac | CMAC = Non-channelled, Macintosh McGrath Mac = Non-channelled, Macintosh |
| 2022 | Haldar [52] | 375 | Surgical | Anaesthetists | 2: CMAC, ST | A: - B: CMAC > ST C: Equal D: Equal E: CMAC > ST Lifting force | CMAC | Non-channelled, Macintosh |
| 2022 | Jayadi [53] | 63 | Surgical | Anaesthetic residents | 2: CMAC, Wycope | A: - B: Equal C: - D: Equal | CMAC = Wycope | CMAC = Non-channelled, Macintosh Wycope = Non-channelled, Acute-angled |
| 2022 | Karadag [54] | 100 | Surgical | Anaesthetists | 2: McGrath (acute), CMAC | A: Equal B: Equal C: Equal D: Equal | McGrath = CMAC | CMAC = Non-channelled, Macintosh McGrath Mac = Non-channelled, Acute-angled |
| 2022 | Kumar [55] | 140 | Surgical | Anaesthetists | 2: McGrath Mac, KV-C | A: Equal B: McGrath Mac > KV C: Equal D: Equal | McGrath Mac | Non-channelled, Macintosh |
| 2022 | Suryatheja [56] | 160 | Surgical | Anaesthetic Residents | 2: CMAC Miller blade size 1, CMAC Macintosh Blade size 2 | A: Equal B: Equal C: Equal D: CMAC Mac > CMAC Mil | CMAC Mac | Non-channelled, Macintosh |
| 2022 | Zhang [57] | 210 | Surgical | Anaesthetists | 2: McGrath Mac-X, CMAC | A: McGrath Mac-X > CMAC B: CMAC > McGrath Mac-X C: Equal D: Equal | McGrath Mac-X = CMAC | McGrath Mac-X = Non-Channelled, Acute-angled CMAC = Non-channelled, Macintosh |
| Year | First Author | No. of Providers | Simulation Setting | Intubator | Number and Types of Videolaryngoscopes Used | Outcomes Based On: A: Improved Glottis View B: Faster Time to Successful Intubation C: Higher First Attempt Intubation Success D: Less Use of Manoeuvres or Adjuncts E: Other | Clinically Preferred Videolaryngoscope | Blade of Most-Preferred VL |
|---|---|---|---|---|---|---|---|---|
| 2016 | Altun [58] | 41 | Difficult Manikin | Anaesthetic Residents | 2: McGrath Mac (acute), CMAC | A: CMAC B: CMAC C: CMAC D: CMAC | CMAC | Non-channelled, Macintosh |
| 2016 | Arslan [59] | 36 | Difficult Paediatric Manikin | Medical Students | 2: GS, AT | A: - B: - C: GS D: GS | GS | Non-channelled, Acute-angled |
| 2016 | El-Tahan [60] | 21 | Double Lumen Tube Manikin | Anaesthetists | 3: GS, AT, KV-NC | A: Equal B: Equal C: Equal D: GS > KV-NC E: GS Preferred over AT and KV-NC | GS | Non-channelled, Acute-angled |
| 2016 | Hippard [61] | 30 | Paediatric Manikin | Anaesthetists | 2: TV-PCD, GS-Cobalt | A: - B: Equal C: Equal D: - | TV-PCD = GS-Cobalt | TV-PCD = Non-channelled, Acute-angled GS-Cobalt = Non-channelled, Acute-angled |
| 2016 | Kim [62] | 35 | Manikin | Physicians | 3: AWS, GS | A: GS B: Equal C: GS D: - | GS | Non-channelled, Acute-angled |
| 2016 | Kim [63] | 21 | Manikin | Physicians | 2: AWS, GS | A: Equal B: AWS C: Equal D: - | AWS | Channelled |
| 2016 | Nakanishi [64] | 35 | Manikin | Physicians | 2: AWS, CMAC | A: Equal B: AWS C: Equal D: - E: Higher Force on Incisors with CMAC than AWS | AWS | Channelled |
| 2016 | Schröder [65] | 42 | Manikin wearing chemical protective gear | Anaesthetists | 3: AT, GS, AP Advance | A: AP Advance > AT and GS B: AP Advance > AT and GS C: - D: - E: Preferred AP Advance > GS > AT | AP Advance | Channelled |
| 2016 | Shin [66] | 39 | Manikin | Novice Medical Students | 2: McGrath Mac, CMAC | A: Equal B: Equal C: Equal D: Equal E: Preferred McGrath Mac | McGrath Mac | Non-channelled, Macintosh |
| 2017 | Hodnick [67] | 5 | Cadaver | Paramedics | 2: GS, VT | A: Equal B: Equal C: Equal D: Equal | GS = VT | GS = Non-channelled, Acute-angled VT = Channelled |
| 2017 | Lee [68] | 18 | Manikin with Normal and Difficult Airway | Paramedics | 4: GS, AWS, KV-NC, KV-C | A: Equal B: AWS C: Equal D: - E: Preferred AWS | AWS | Channelled |
| 2017 | Owada [69] | 20 | Paediatric Manikin with Difficult Airway | Anaesthetists | 2: AT, McGrath Mac | A: AT B: Equal C: AT D: - E: AT Preferred and less dental trauma | AT | Channelled |
| 2018 | Kriege [70] | 80 | Infant Manikin Normal and Difficult Airway | Anaesthetic Staff and Paediatric Critical Care Medicine Staff | 2: KV-Paeds aBlade, CMAC-D | A: KV-Paeds aBlade B: KV-Paeds aBlade C: KV-Paeds aBlade D: - | KV-Paeds aBlade | Non-Channelled, Acute-angled |
| 2018 | Oshika [71] | 21 | Prone Manikin | Anaesthetists | 2: AWS, McGrath Mac | A: - B: AWS C: AWS D: - | AWS | Channelled |
| 2019 | Chew [72] | 105 | Difficult Airway Manikin | Junior Doctors | 3: KV-aBlade-C, KV-aBlade-NC, Mcgrath Mac | A: - B: KV-aBlade-C + McGrath Mac > KV-aBlade-NC C: KV-aBlade-C + McGrath Mac > KV-aBlade-NC D: - | KV-aBlade-C + McGrath Mac | KV-aBlade-C = Channelled McGrath Mac = Non-channelled, Macintosh |
| 2019 | Desai [73] | 26 | Paediatric Pierre Robin Sequence Manikin | Paediatric Intensive Care Physicians | 2: AT, GS | A: Equal B: AT C: AT D: - | AT | Channelled |
| 2019 | Raimann [74] | 42 | Trapped Car Crash Manikin | Anaesthetic Staff and Emergency Physicians | 4: CMAC-D, TV-PCD, CMAC, CMAC-PM | A: CMAC-D > TV-PCD B: CMAC > TV-PCD + CMAC-D, CMAC-PM > TV-PCD C: CMAC + CMAC-PM > TV-PCD D: - E: CMAC Preferred | CMAC | Non-channelled, Macintosh |
| 2020 | Gaszyński [75] | 11 | Prone and Sitting Manikin | Anaesthetists | 2: AWS, IB | A: Equal B: AWS C: Equal D: - E: Lower pressure with AWS | AWS | Channelled |
| 2020 | Moritz [76] | 112 | Difficult Airway Manikin | Anaesthetist and Paramedics | 4: I-View, KV-NC, GS, Dahlhausen | A: KV-NC, GS, Dahlhausen > I-View B: KV-NC, GS, Dahlhausen > I-View C: KV-NC, GS, Dahlhausen > I-View D: - E: Preferred GS | GS | Non-channelled, Acute-angled |
| 2020 | Romito [77] | 8 | Cadaver with Cervical Spine Instability | Anaesthetists | 3: CMAC-D, GS, McGrath Mac-X | A: Equal B: - C: Equal D: - | CMAC-D = GS = McGrath Mac-X | CMAC-D = Non-channelled, Acute-angled GS = Non-channelled, Acute-angled McGrath Mac-X = Non-channelled, Acute-angled |
| 2020 | Votruba [78] | 58 | Manikin with Cervical Spine Immbolisation | Anaesthetists | 2: KV-C, KV-NC | A: Equal B: KV-C C: KV-C D:- E: Easier with KV-C | KV-C | Channelled |
| 2020 | Yi [79] | 35 | Manikin with Normal Neck and with Cervical Spine Instability | Anaesthetic Nurses | 2: McGrath Mac, AWS | A: Equal B: Equal C: Equal D: - | McGrath Mac = AWS | MGrath Mac = Non-channelled, Macintosh AWS = Channelled |
| 2021 | Ataman [80] | 23 | Manikin with Normal and Difficult Airway | Emergency Physicians and Emergency Residents | 2: GS, AirAngel 3D-Printed | A: - B: GS C: GS D: - | GS | Non-channelled, Acute-angled |
| 2021 | Decamps [81] | 79 | Critical Illness Manikin | Residents | 4: KV-C, AWS, AT, VT | A: KV-C + AWS > VT B: AWS > VT C: Equal D: Equal E: Ease of use with KV-C + AWS + AT > VT | AWS | Channelled |
| 2021 | Gupta [82] | 50 | COVID Simulation Manikin | Anaesthetist and Non-Anaesthetic Physicians | 2: KV-C, Tuoren | A: KV-C B: KV-C C: KV-C D: KV-C E: Easier and less complications with KV-C | KV-C | Channelled |
| 2021 | Moritz [83] | 86 | Paediatric Pierre Robin Sequence Manikin | Anaesthetists | 2: GS-Core, CMAC-Miller | A: GS B: CMAC-Miller C: Equal D: CMAC-Miller E: CMAC-Miller preferred by both anaesthetist with experience and with limited experience | CMAC-Miller | Non-channelled, Miller |
| 2021 | Taylor [84] | 33 | Manikin | Military emergency providers | 2: I-view, GS | A: GS > I-view B: GS > I-view C: Equal D: - | GS | Non-channelled, Acute-angled |
| 2021 | Vig [85] | 30 | Manikin | Medical Professionals (no intubation experience) | 2: McGrath Mac, CMAC | A: CMAC > McGrath B: Equal C: Equal D: Equal | CMAC | Non-channelled, Macintosh |
| 2022 | Gupta [86] | 100 | Manikin | Medical Students | 2: KV-C, KV-NC | A: Equal B: KV-C > KVNC C: KV-C > KVNC D:- E: KV-C > KVNC ease of intubation | KV-C | Channelled |
| 2022 | Er [87] | 50 | Manikin | Paediatric Residents | 2: McGrath Mac, CMAC PM | A: CMAC PM > McGrath Mac B: CMAC PM > McGrath Mac C: CMAC PM > McGrath D:- | CMAC | Non-channelled, Macintosh |
| 2022 | Kumar [88] | 61 | Manikin | Healthcare Staff with COVID PPE | 2: CMAC, KV-C | A: Equal B: Equal C: Equal D: Equal E: CMAC > KV-C—easier insertion of laryngoscope blade | CMAC | Non-channelled, Macintosh |
| Surgical | Simulation | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| VLS | Surgical Studies | Favoured Studies | % of Studies Favoured | Total Number of Patients in Studies | Simulation Studies | Favoured Studies | % of Studies Favoured | Total Number of Participants in Studies | Total Studies | Favoured | % Favoured |
| CMAC | 25 | 19 | 76% | 2894 | 12 | 7 | 58% | 472 | 37 | 26 | 70% |
| McGrath | 19 | 12 | 63% | 2304 | 9 | 4 | 44% | 349 | 28 | 16 | 57% |
| GS | 13 | 9 | 69% | 1240 | 14 | 9 | 64% | 496 | 27 | 18 | 67% |
| KV-NC | 6 | 5 | 83% | 1074 | 7 | 1 | 14% | 494 | 13 | 6 | 46% |
| AWS | 8 | 4 | 50% | 1001 | 8 | 7 | 88% | 255 | 16 | 11 | 69% |
| AT | 11 | 6 | 54% | 1397 | 6 | 2 | 33% | 224 | 17 | 8 | 47% |
| KV-C | 12 | 2 | 17% | 1756 | 7 | 4 | 57% | 471 | 19 | 6 | 32% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nedunchezhian, V.; Nedunchezhian, I.; Van Zundert, A. Clinically Preferred Videolaryngoscopes in Airway Management: An Updated Systematic Review. Healthcare 2023, 11, 2383. https://doi.org/10.3390/healthcare11172383
Nedunchezhian V, Nedunchezhian I, Van Zundert A. Clinically Preferred Videolaryngoscopes in Airway Management: An Updated Systematic Review. Healthcare. 2023; 11(17):2383. https://doi.org/10.3390/healthcare11172383
Chicago/Turabian StyleNedunchezhian, Vikram, Ishvar Nedunchezhian, and André Van Zundert. 2023. "Clinically Preferred Videolaryngoscopes in Airway Management: An Updated Systematic Review" Healthcare 11, no. 17: 2383. https://doi.org/10.3390/healthcare11172383