
Assessment of the Possibility of Using the Laryngoscopes Macintosh, McCoy, Miller, Intubrite, VieScope and I-View for Intubation in Simulated Out-of-Hospital Conditions by People without Clinical Experience: A Randomized Crossover Manikin Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
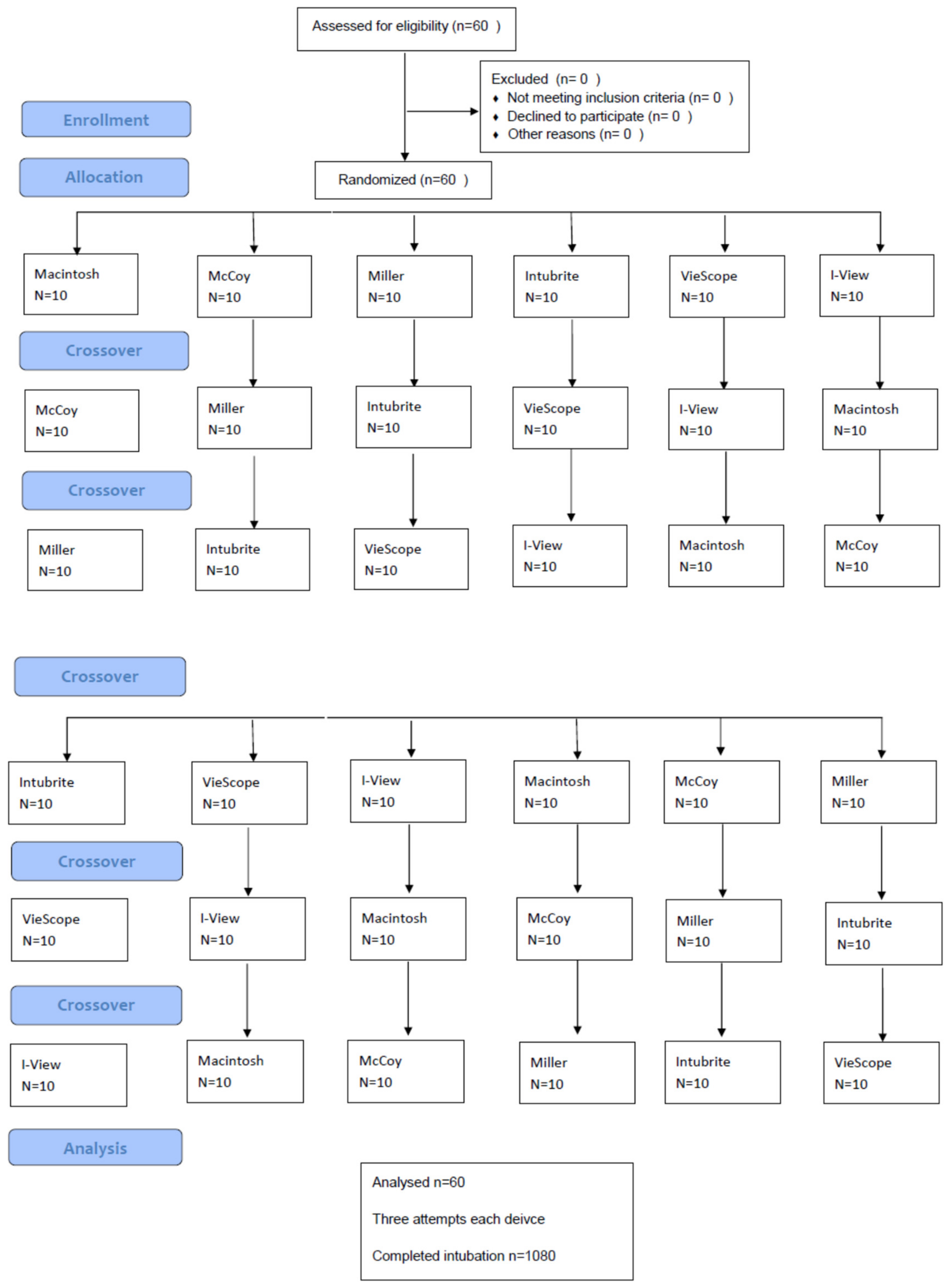
2.2. Study Design
2.3. Study Protocol
- Sex
- Age
- Experience level: the number of dummy intubations performed so far by the subject and which laryngoscopes were used for previous intubations.
- Success of intubation, position of the tube: tracheal vs. esophageal (primary endpoint);
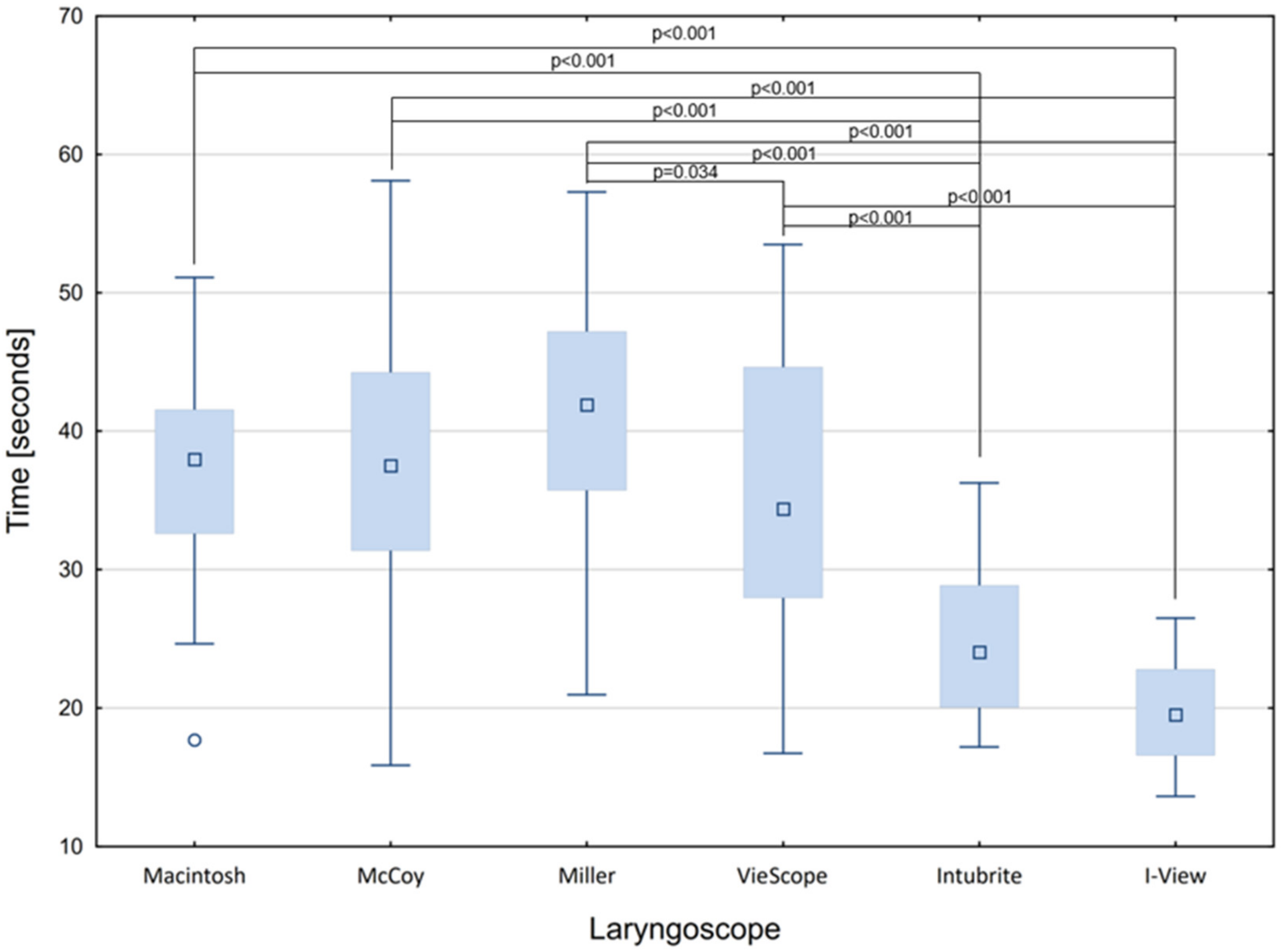
- Comparison of times to ventilation in the first, second, and third intubation attempts (secondary endpoint);
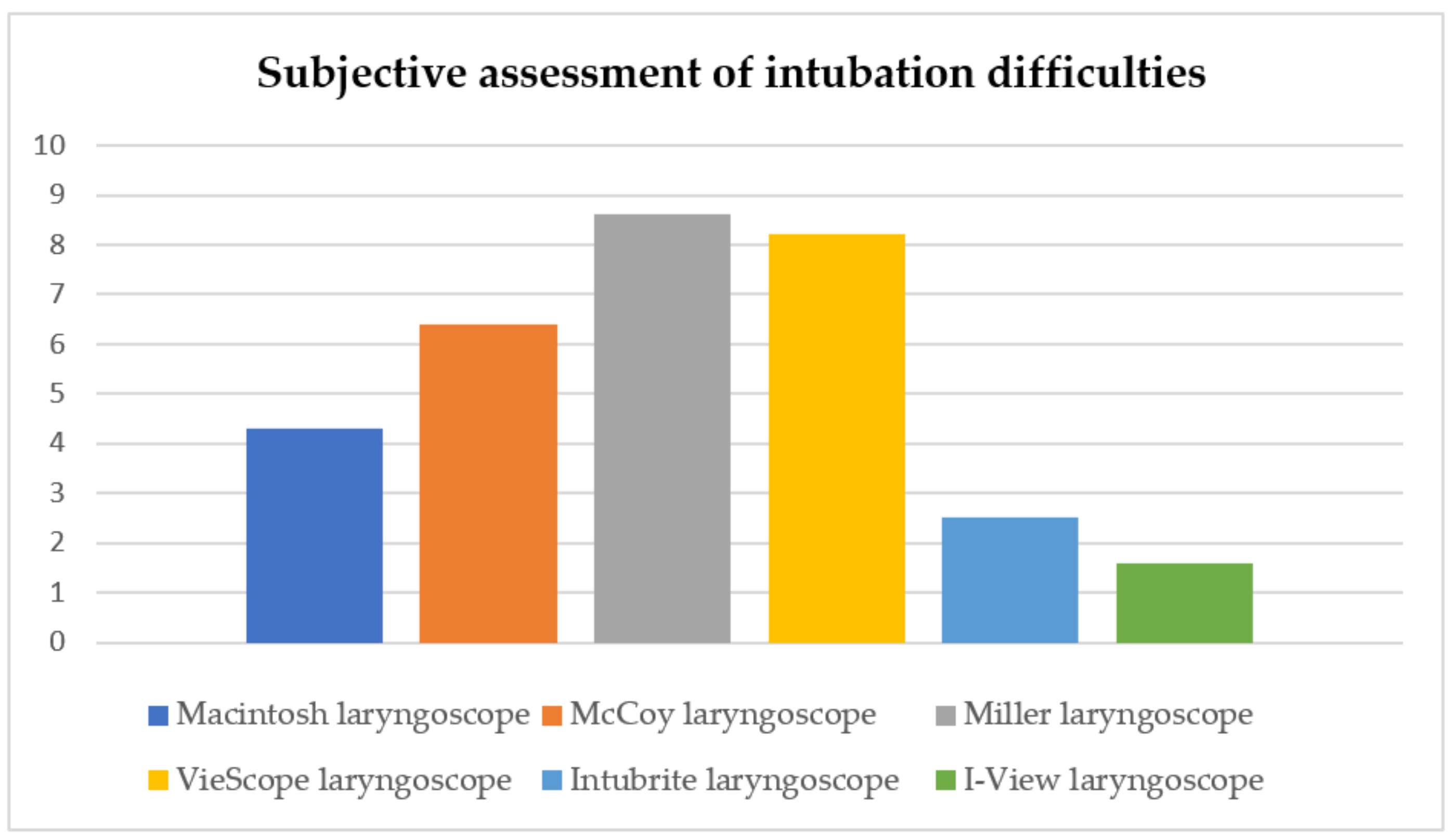
- Feelings of subjects (secondary endpoint).
2.4. Statistical Analysis
3. Results
3.1. Demographic and Contextual Data
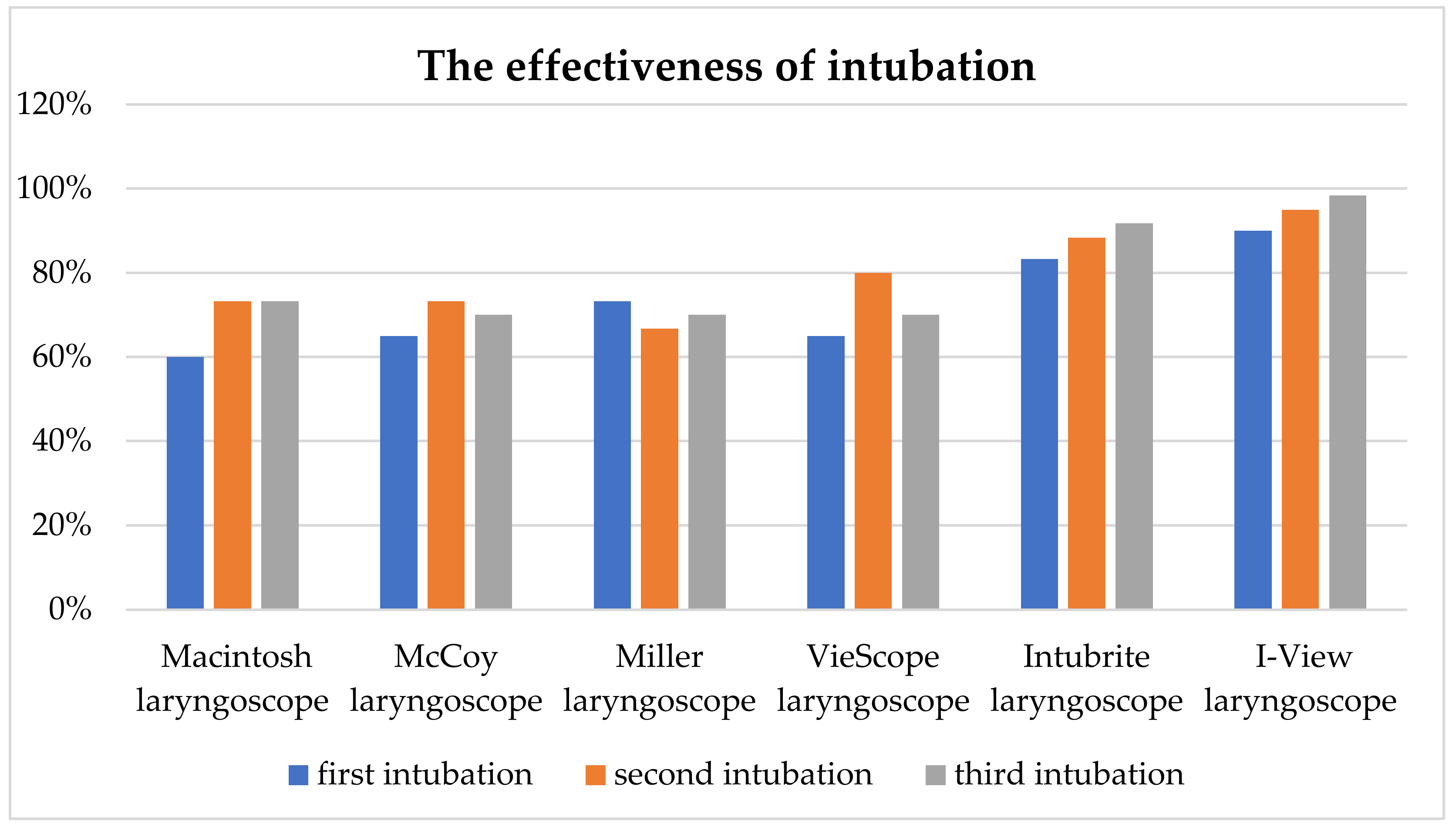
3.2. Primary Endpoint
3.3. Secondary Endpoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lewis, S.R.; Butler, A.R.; Parker, J.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst. Rev. 2016, 2022, CD011136. [Google Scholar] [CrossRef]
- Pierre, M.S.; Krischke, F.; Luetcke, B.; Schmidt, J. The influence of different patient positions during rapid induction with severe regurgitation on the volume of aspirate and time to intubation: A prospective randomised manikin simulation study. BMC Anesthesiol. 2019, 19, 16. [Google Scholar] [CrossRef] [PubMed]
- Gaszyński, T.M.; Jakubiak, J. Muscle activity during intubation using 4 laryngoscopes: Macintosh laryngoscope, Intubrite, TrueView Evo2 and KingVision—A comparative study. Med. Pr. 2016, 57, 155–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tesler, J.; Rucker, J.; Sommer, D. Rescuer position for tracheal intubation on the ground. Resuscitation 2003, 56, 83–89. [Google Scholar] [CrossRef]
- Attila, K.; Ludwin, K.; Evrin, T.; Katipoglu, B.; Torlinski, T.; Pruc, M.; Szarpak, L. The impact of COVID-19 on airway management in prehospital resuscitation. Disaster Emerg. Med. J. 2020, 5, 216–217. [Google Scholar] [CrossRef]
- Szarpak, L.; Drozd, A.; Smereka, J. Airway management and ventilation principles in COVID-19 patients. J. Clin. Anesth. 2020, 65, 109877. [Google Scholar] [CrossRef]
- Link, M.S.; Berkow, L.C.; Kudenchuk, P.J.; Halperin, H.R.; Hess, E.P.; Moitra, V.K.; Neumar, R.W.; O’Neil, B.J.; Paxton, J.H.; Silvers, S.M.; et al. Part 7: Adult advanced cardiovascular life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132 (Suppl. 2), S444–S464, Correction in Circulation 2015, 132, e385. [Google Scholar] [CrossRef]
- Ludwin, K.; Bialka, S.; Czyzewski, L.; Smereka, J.; Dabrowski, M.; Dabrowska, A.; Ladny, J.R.; Ruetzler, K.; Szarpak, L. Video laryngoscopy for endotracheal intubation of adult patients with suspected/confirmed COVID-19. A systematic review and meta-analysis of randomized controlled trials. Disaster Emerg. Med. J. 2020, 5, 85–97. [Google Scholar] [CrossRef]
- Ducharme, S.; Kramer, B.; Gelbart, D.; Colleran, C.; Risavi, B.; Carlson, J.N. A pilot, prospective, randomized trial of video versus direct laryngoscopy for paramedic endotracheal intubation. Resuscitation 2017, 114, 121–126. [Google Scholar] [CrossRef]
- Moritz, A.; Leonhardt, V.; Prottengeier, J.; Birkholz, T.; Schmidt, J.; Irouschek, A. Comparison of Glidescope® Go™, King Vision™, Dahlhausen VL, I-View™ and Macintosh laryngoscope use during difficult airway management simulation by experienced and inexperienced emergency medical staff: A randomized crossover manikin study. PLoS ONE 2020, 15, e0236474. [Google Scholar] [CrossRef]
- Nakanishi, T.T.; Sento, Y.; Kamimura, Y.; Sobue, K. Macintosh laryngoscope and i-view™ and C-MAC® video laryngoscopes for tracheal intubation with an aerosol box: A randomized crossover manikin study. JA Clin. Rep. 2021, 7, 52. [Google Scholar] [CrossRef]
- Wakabayashi, R.; Ishida, T.; Yamada, T.; Kawamata, M. Effect of an aerosol box on tracheal intubation difficulty. J. Anesth. 2020, 34, 790–793. [Google Scholar] [CrossRef]
- Taylor, D.H.; Wagner, E.M.; Hu, J.S.; Tobin, M.R.; Cronin, A.J.; Couperus, K.S.; April, M.D.; Schauer, S.G.; Naylor, J.F. New Versus Old, The i-View Video Laryngoscope Versus the GlideScope: A Prospective, Randomized, Crossover Trial. Med. J. 2021, 81–89. [Google Scholar]
- Bogdański, Ł.; Truszewski, Z.; Kurowski, A.; Czyżewski, Ł.; Zaśko, P.; Adamczyk, P.; Szarpak, Ł. Simulated endotracheal intubation of a patient with cervical spine immobilization during resuscitation: A randomized comparison of the Pentax AWS, the Airtraq, and the McCoy Laryngoscopes. Am. J. Emerg. Med. 2015, 33, 1814–1817. [Google Scholar] [CrossRef]
- Gawel, W.B.; Kaminska, H.; Wieczorek, W. The efficacy of endotracheal intubation utilizing INTUBRITE laryngoscope during cardiopulmonary resuscitation. Am. J. Emerg. Med. 2018, 36, 1895–1896. [Google Scholar] [CrossRef]
- Sierzantowicz, R.; Dabrowska, A.; Dabrowski, M.; Drozd, A.; Wojewodzka-Zelezniakowicz, M. ETView® video-tube versus Intubrite® laryngoscope for endotracheal intubation during CPR. Am. J. Emerg. Med. 2017, 35, 1367–1368. [Google Scholar] [CrossRef]
- Szarpak, L.; Smereka, J.; Ladny, J. Comparison of Macintosh and Intubrite laryngoscopes for intubation performed by novice physicians in a difficult airway scenario. Am. J. Emerg. Med. 2017, 35, 796–797. [Google Scholar] [CrossRef]
- Higashizawa, T.; Bioto, H.; Nishiyama, T.; Sakai, T.; Konishi, A. Assessment of practice of endotracheal intubation by levering Laryngoscope in teaching of undergraduate medical students. Masui 1997, 46, 1255–1258. [Google Scholar]
- Gaszyński, T. A comparison of a Standard Macintosh Blade Laryngoscope, Pentax-AWS Videolaryngoscope and Intubrite Videolaryngoscope for Tracheal Intubation in Manikins in Sitting and Prone Positions: A Randomized Cross-Over Study. Diagnostics 2020, 10, 603. [Google Scholar] [CrossRef]
- Yildirim, A.; Kiraz, H.A.; Ağaoğlu, I.; Akdur, O. Comparison of Macintosh, McCoy and C-MAC D-Blade video laryngoscope intubation by prehospital emergency health workers: A simulation study. Intern. Emerg. Med. 2017, 12, 91–97. [Google Scholar] [CrossRef]
- Sethuraman, D.; Darshane, S.; Guha, A.; Charters, P.; Charters, S. A randomised, crossover study of the Dorges, McCoy and Macintosh laryngoscope blades in simulated difficult intubation scenario. Anaesthesia 2006, 61, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Hikawa, Y.; Saito, Y.; Yasuda, K. The McCoy levering laryngoscope in patients with limited neck extension. Can. J. Anaesth. 1997, 44, 674–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altun, D.; Ozkan-Seyhan, T.; Orhan-Sungur, M.; Sivrikoz, N.; Camci, E. Comparison of 4 Laryngoscopes in 2 Difficult Airway Scenarios: A Randomized Crossover Simulation-Based Study. Simul. Healthc. 2016, 11, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Gabbott, D.A. Laryngoscopy using the McCoy laryngoscope after application of a cervical collar. Anaesthesia 1996, 51, 812–814. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, C.H.; McDonnell, J.G.; Harte, B.H.; Laffey, J.G. A comparison of direct and indirect laryngoscopes and the ILMA in novice users: A manikin study. Anaesthesia 2007, 62, 1161–1166. [Google Scholar] [CrossRef]
- Nandakumar, K.P.; Bhalla, A.P.; Pandey, R.K.; Baidya, D.K.; Subramaniam, R.; Kashyap, L. Comparison of Macintosh, McCoy, and Glidescope video laryngoscope for intubation in morbidly obese patients: Randomized controlled trial. Saudi J. Anaesth. 2018, 12, 433–439. [Google Scholar] [CrossRef]
- Akbarzadeh, S.R.; Gillani, M.T.; Tabari, M.; Morovatdar, N. Comparison analysis of the Usefulness of the GlideScope®, Macintosh, and McCoy Laryngoscopes for Endotracheal Intubation in Patients with Obesity: A Randomized, Clinical Trial. Anesthesiol. Pain Med. 2017, 7, e57913. [Google Scholar] [CrossRef] [Green Version]
- Harioka, T.; Nomura, K.; Mukaida, K.; Hosoi, S.; Nakao, S. The McCoy laryngoscope, external laryngeal pressure, and their combined use. Anaesth. Intensive Care 2000, 28, 537–539. [Google Scholar] [CrossRef] [Green Version]
- Cook, T.M.; Tuckey, J.P. A comparison between the Macintosh and the McCoy laryngoscope blades. Anaesthesia 1996, 51, 977–980. [Google Scholar] [CrossRef]
- Chisholm, D.G.; Calder, I. Experience with the McCoy laryngoscope in difficult laryngoscopy. Anaesthesia 1997, 52, 906–908. [Google Scholar] [CrossRef]
- Vidhya, S.; Prakash, N.; Swain, A.; Kumar, S.; Shukla, R. An Inquiry on Airway Management by McCoy Blade with Elevated Tip and Miller Straight Blade with Paraglossal Technique: Relevance for difficult airway Management in Current Infectious Times. Anesth. Essays Res. 2021, 15, 401–407. [Google Scholar] [CrossRef]
- Achen, B.; Terblanche, O.C.; Finucane, B.T. View of the larynx obtained using the Miller blade and paraglossal approach compared to that with the Macintosh blade. Anaesth. Intensive Care 2008, 36, 717–721. [Google Scholar] [CrossRef] [Green Version]
- Arino, J.J.; Velasco, J.M.; Gasco, C.; Lopez-Timoneda, F. Straight blades improve visualization of the larynx while curved blades increase ease of intubation: A comparison of Macintosh, Miller, McCoy, Belscope and Lee-Fiberview blades. Can. J. Anaesth. 2003, 50, 501–506. [Google Scholar] [CrossRef]
- Landry, W.B., 3rd; Nossaman, B.D. Airway risk factors for the Miller laryngoscope blade. J. Clin. Anesth. 2016, 33, 62–67. [Google Scholar] [CrossRef]
- Yadav, P.; Kundu, S.B.; Bhattacharjee, D.P. Comparison between Macintosh and McCoy larynbgoscope blade size 2 in paediatric patients—A randomised conteolled trial. Indian J. Anaesth. 2019, 63, 15–20. [Google Scholar] [CrossRef]
- Iohom, G.; Franklin, R.; Casey, W.; Lyons, B. The McCoy straight blade does not improve laryngoscopy and intubation in normal infants. Can. J. Anaesth. 2004, 51, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Maslanka, M.; Smereka, J.; Czyzewski, L.; Ladny, J.; Dabrowski, M.; Szarpak, L. VieScope® laryngoscope versus Macintosh laryngoscope during difficult intubation performed by paramedics: A randomized cross-over manikin trial. Disaster Emerg. Med. J. 2020, 5, 134–141. [Google Scholar] [CrossRef]
- Wieczorek, P.; Szarpak, L.; Dabrowska, A.; Pruc, M.; Navolokina, A.; Raczyński, A.; Smereka, J. A Comparison of the bébé VieScope™ and Direct Laryngoscope for Use While Wearing PPE-AGP: Randomized Crossover Simulation Trial. Children 2022, 9, 1774. [Google Scholar] [CrossRef]
- Szarpak, L.; Peacock, F.W.; Rafique, Z.; Ladny, J.R.; Nadolny, K.; Malysz, M.; Dabrowski, M.; Chirico, F.; Smereka, J. Comparison of VieScope® and Macintosh laryngoscopes for intubation during resuscitation by paramedics wearing personal equipment. Am. J. Emerg. Med. 2022, 53, 122–126. [Google Scholar] [CrossRef]
- Ecker, H.; Stranz, S.; Kolvenbach, S.; Herff, H.; Hellmich, M.; Wetsch, W.A. Airway Management during Massive Gastric Regurgitation Using VieScope or Macintosh Laryngoscope—A Randomized, Controlled Simulation Trial. J. Clin. Med. 2022, 11, 5363. [Google Scholar] [CrossRef]
- Ecker, H.; Kolvenbach, S.; Herff, H.; Wetsch, W.A. Intubation using VieScope vs. Video laryngoscopy in full personal protective equipment—A randomized, controlled simulation trial. BMC Anesthesiol. 2021, 21, 288. [Google Scholar] [CrossRef] [PubMed]
- Petzoldt, M.; Engels, Y.; Popal, Z.; Tariparast, P.A.; Sasu, P.B.; Brockmann, A.; Punke, M.A.; Grensemann, J. Elective Tracheal Intubation With the VieScope-A Prospective Randomized Non-inferiority Pilot Study (VieScope-Trial). Front. Med. 2022, 9, 820847. [Google Scholar] [CrossRef] [PubMed]
- Pieters, B.M.; Wilbers, N.E.; Huijzer, M.; Winkens, B.; Van Zundert, A.A. Comparison of seven videolaryngoscopes with the Macintosh laryngoscope in manikins by experienced and novice personnel. Anaesthesia 2016, 71, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Zundert, A.A.; Pieters, B.M. Videolaryngoscopy offers us more than classic direct laryngoscopy. Minerva Anestesiol. 2015, 81, 933–934. [Google Scholar]
- Van Zundert, A.; Pieters, B.; Doerges, V.; Gatt, S. Videolaryngoscopy allows a better view of the pharynx and larynx than classic laryngoscopy. Br. J. Anaesth. 2012, 109, 1014–1015. [Google Scholar] [CrossRef] [Green Version]
- Van Zundert, A.; Pieters, B.; van Zundert, T.; Gatt, S. Avoiding palatopharyngeal trauma during videolaryngoscopy: Do not forget the ‘blind spots’. Acta Anaesthesiol. Scand. 2012, 56, 532–534. [Google Scholar] [CrossRef]
- Pieters, B.M.A.; Maas, E.H.A.; Knape, J.T.A.; Van Zundert, A.A.J. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: A systematic review and meta-analysis. Anaesthesia 2017, 72, 1532–1541. [Google Scholar] [CrossRef] [Green Version]
- Smereka, J.; Ladny, J.R.; Szarpak, L. Comparison of the Intubrite and Macintosh laryngoscopes in a difficult airway scenario. Am. J. Emerg. Med. 2017, 35, 925. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laryngoscope | Attempt Number | Unsuccessful: Esophageal Position or Intubation > 60 s | Successful: Tracheal Position | p-Value |
|---|---|---|---|---|
| Macintosh laryngoscope | 1 | 24 (40%) | 36 (60%) | >0.05 |
| 2 | 16 (26.7%) | 44 (73.3%) | ||
| 3 | 16 (26.67%) | 44 (73.33%) | ||
| McCoy laryngoscope | 1 | 21 (35%) | 39 (65%) | >0.05 |
| 2 | 16 (26.7%) | 44 (73.3%) | ||
| 3 | 18 (30%) | 42 (70%) | ||
| Miller laryngoscope | 1 | 16 (26.67%) | 44 (73.33%) | >0.05 |
| 2 | 20 (33.3%) | 40 (66.7%) | ||
| 3 | 18 (30%) | 42 (70%) | ||
| VieScope laryngoscope | 1 | 21 (35%) | 39 (65%) | >0.05 |
| 2 | 12 (20%) | 48 (80%) | ||
| 3 | 18 (30%) | 42 (70%) | ||
| Intubrite laryngoscope | 1 | 10 (16.67%) | 50 (83.33%) | >0.05 |
| 2 | 7 (11.7%) | 53 (88.3%) | ||
| 3 | 5 (8.3%) | 55 (91.67%) | ||
| I-View laryngoscope | 1 | 6 (10%) | 54 (90%) | >0.05 |
| 2 | 3 (5%) | 57 (95%) | ||
| 3 | 1 (1.67%) | 59 (98.33%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratajczyk, P.; Kluj, P.; Dolder, P.; Szmyd, B.; Gaszyński, T. Assessment of the Possibility of Using the Laryngoscopes Macintosh, McCoy, Miller, Intubrite, VieScope and I-View for Intubation in Simulated Out-of-Hospital Conditions by People without Clinical Experience: A Randomized Crossover Manikin Study. Healthcare 2023, 11, 661. https://doi.org/10.3390/healthcare11050661
Ratajczyk P, Kluj P, Dolder P, Szmyd B, Gaszyński T. Assessment of the Possibility of Using the Laryngoscopes Macintosh, McCoy, Miller, Intubrite, VieScope and I-View for Intubation in Simulated Out-of-Hospital Conditions by People without Clinical Experience: A Randomized Crossover Manikin Study. Healthcare. 2023; 11(5):661. https://doi.org/10.3390/healthcare11050661
Chicago/Turabian StyleRatajczyk, Paweł, Przemysław Kluj, Przemysław Dolder, Bartosz Szmyd, and Tomasz Gaszyński. 2023. "Assessment of the Possibility of Using the Laryngoscopes Macintosh, McCoy, Miller, Intubrite, VieScope and I-View for Intubation in Simulated Out-of-Hospital Conditions by People without Clinical Experience: A Randomized Crossover Manikin Study" Healthcare 11, no. 5: 661. https://doi.org/10.3390/healthcare11050661