
On the Implementation of a Post-Pandemic Deep Learning Algorithm Based on a Hybrid CT-Scan/X-ray Images Classification Applied to Pneumonia Categories

 ,
,
Abstract
:1. Introduction
- Using preprocessing techniques to enhance the quality of images;
- Training DL model to distinguish between common pneumonia, coronavirus pneumonia and normal cases;
- Performing classification on two different modalities including chest X-ray and chest CT scan.
2. Related Work
2.1. X-ray-Based Approaches
2.2. CT-Scan Based Approaches
3. Materials and Methods
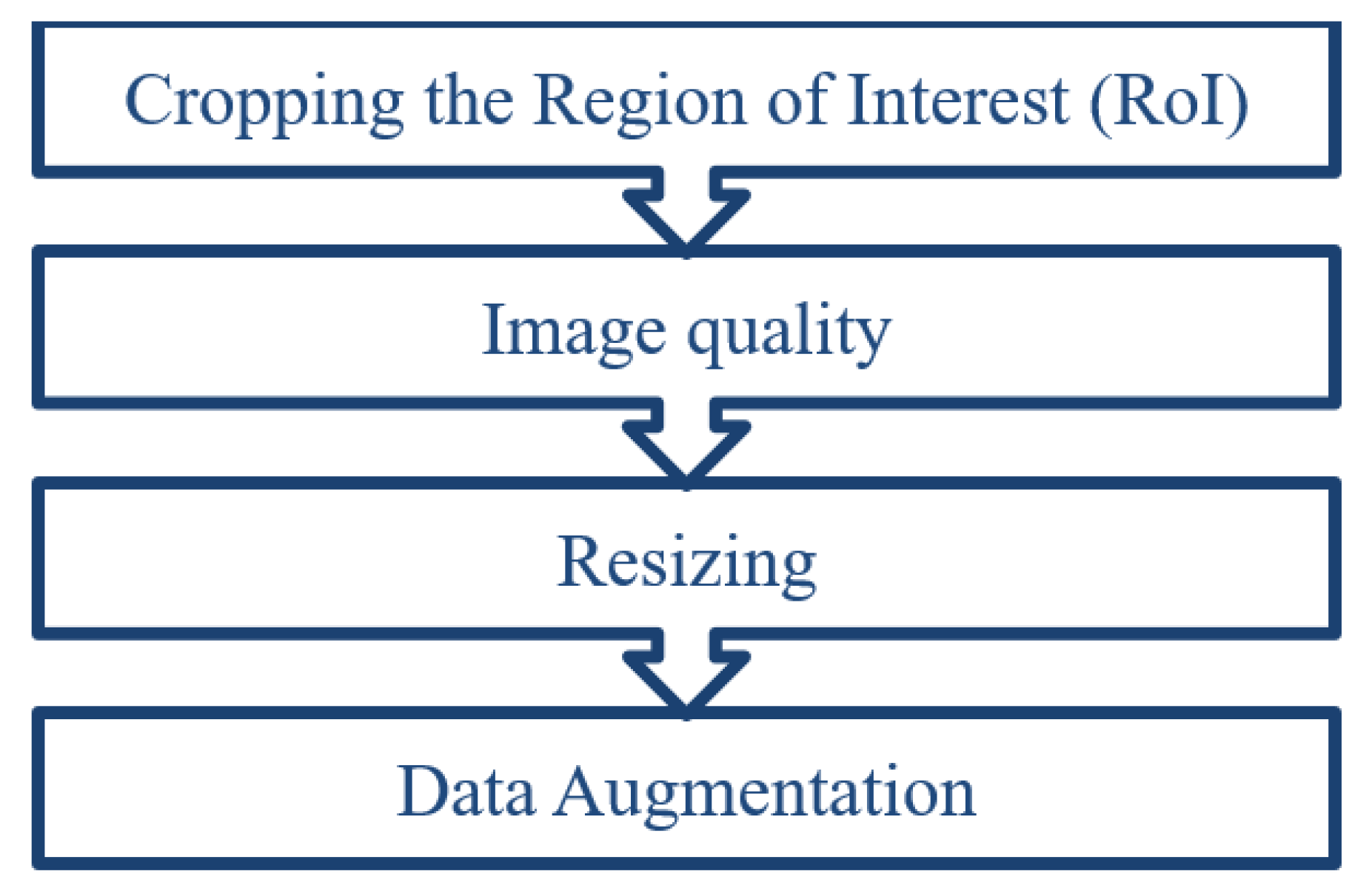
3.1. Image Preprocessing
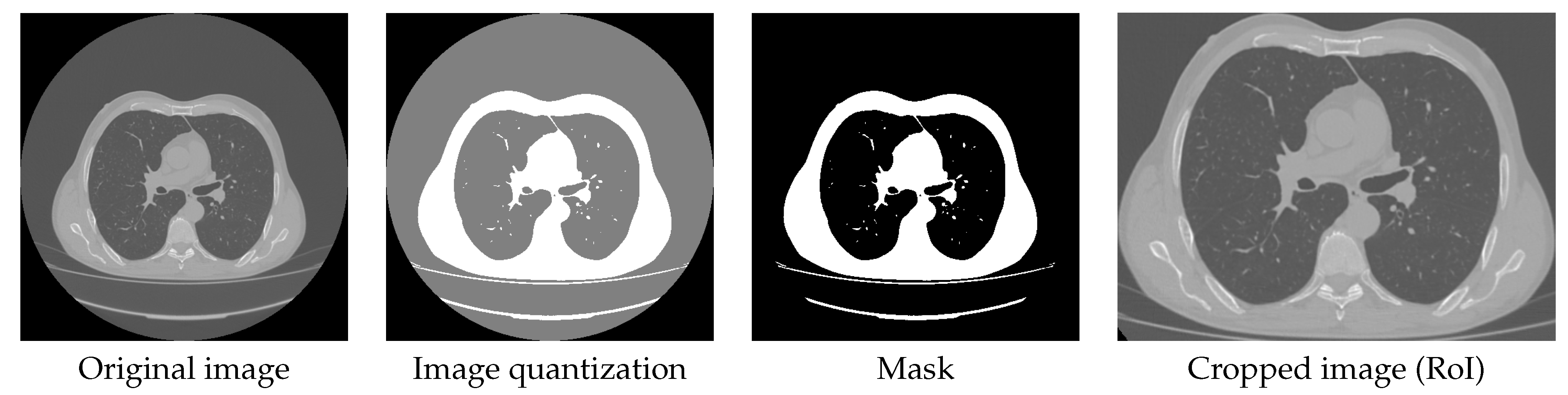
3.1.1. Cropping the Region of Interest (RoI)
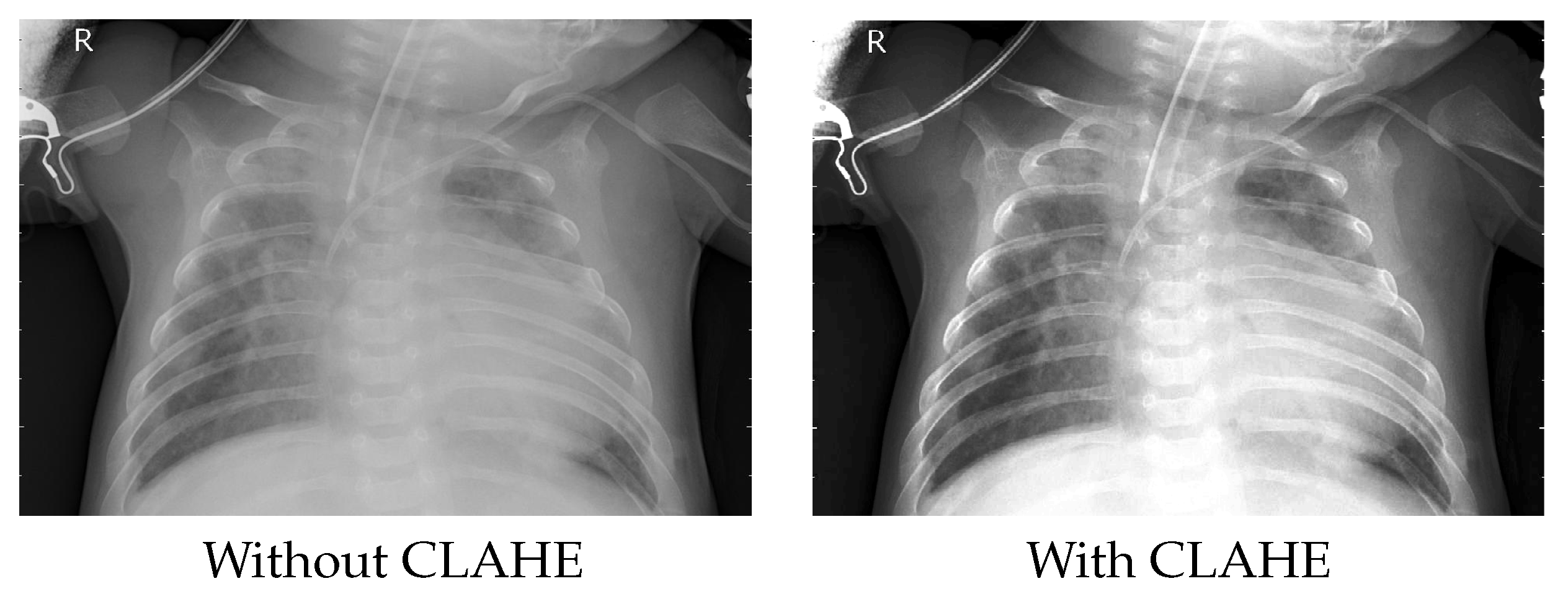
3.1.2. Improving the Image Quality
3.1.3. Image Resizing
3.1.4. Data Augmentation
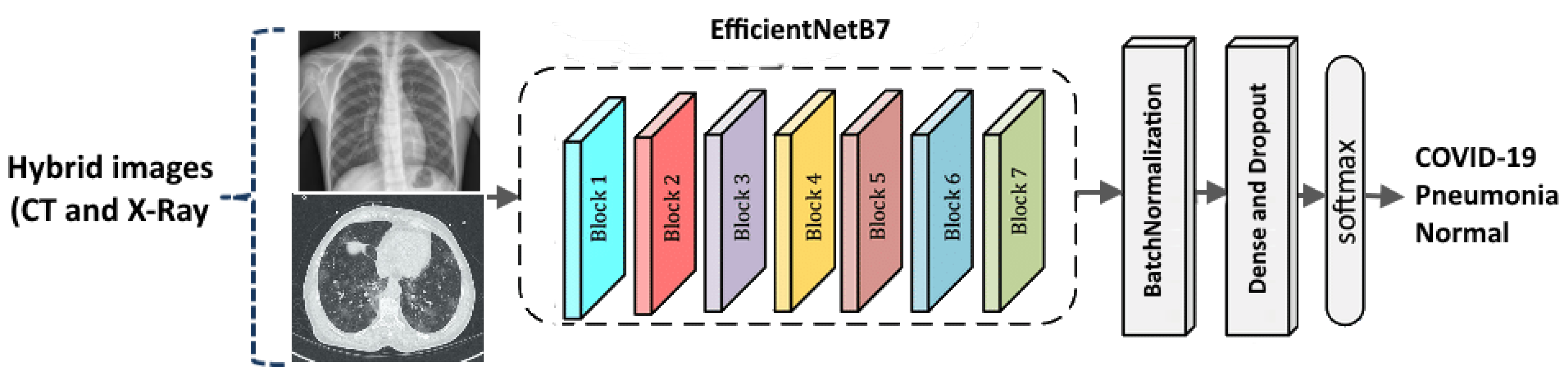
3.2. Classification Network Architecture
3.3. Used Datasets
3.3.1. X-ray Dataset
3.3.2. CT Scan Dataset
3.3.3. Cheikh Zaid Data
3.4. Experimental Settings
4. Experimental Results
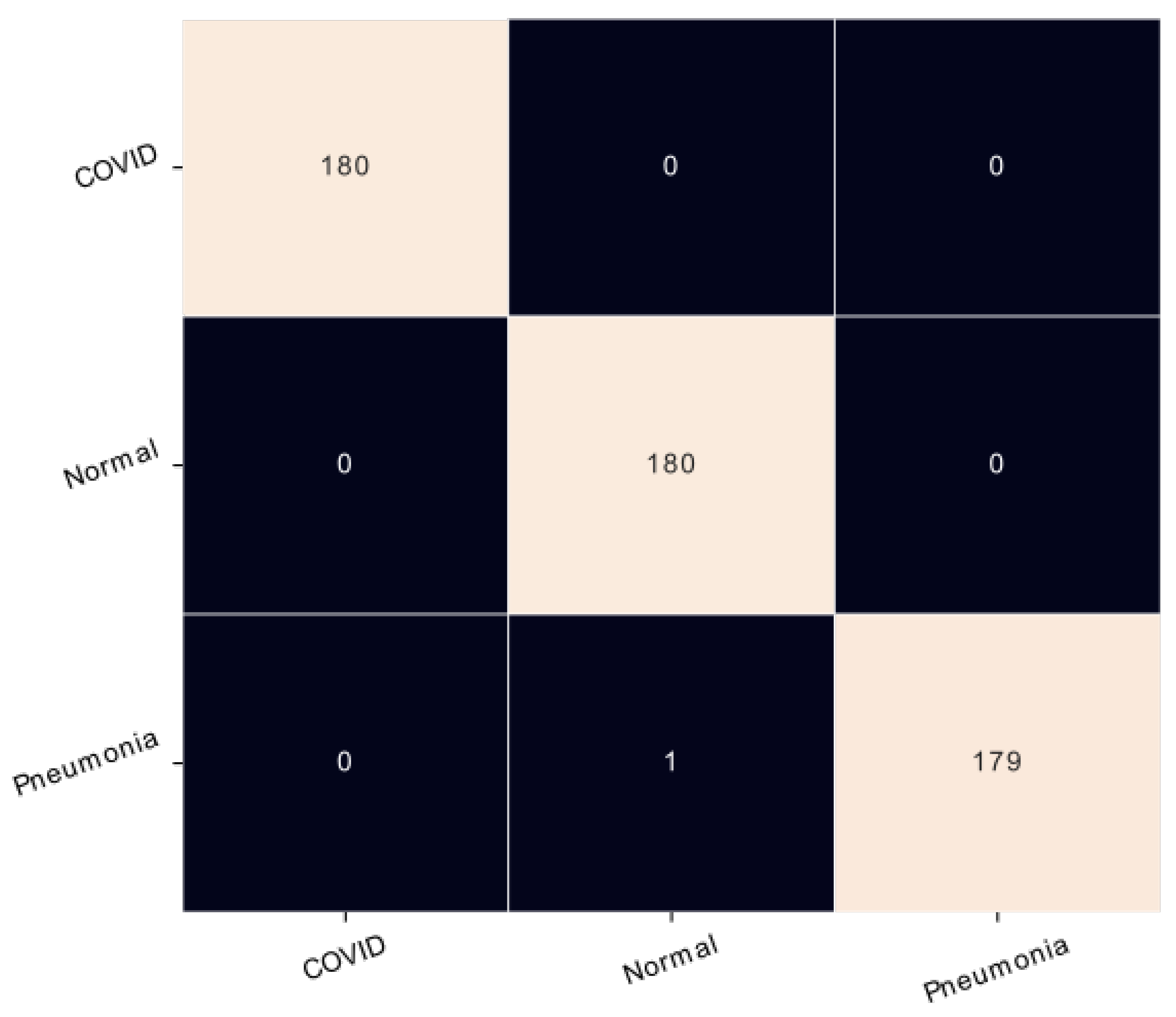
4.1. Results on X-ray Modality
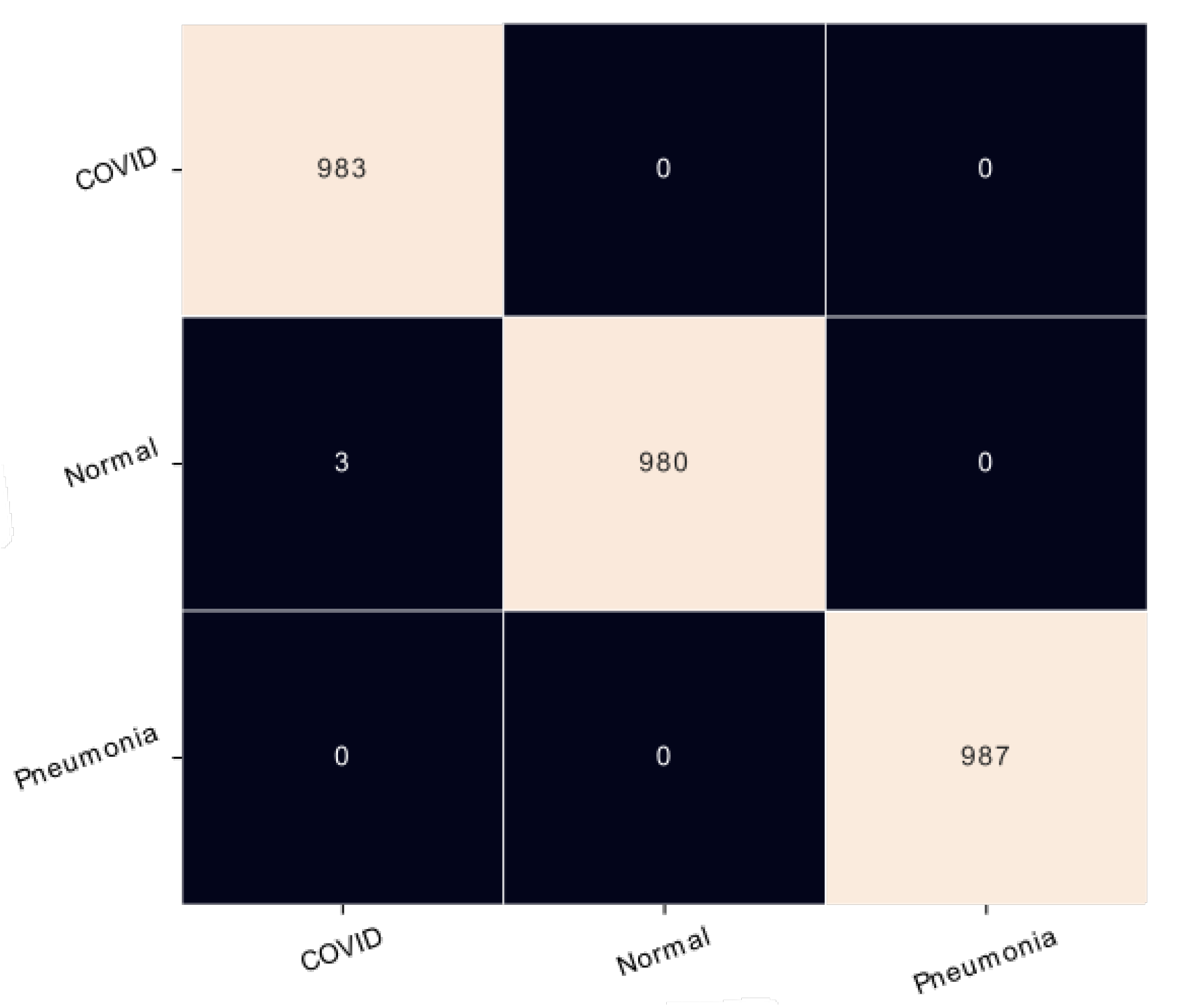
4.2. Results on CT Scan Modality
4.3. Results on Cheikh Zaid Data
4.4. Comparison with the State-of-the-Art
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus disease 2019–COVID-19. Clin. Microbiol. Rev. 2020, 33, e00028-20. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Chavez, S.; Carius, B.M.; Liang, S.Y.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Clinical update on COVID-19 for the emergency and critical care clinician: Medical management. Am. J. Emerg. Med. 2022, 56, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Leroux, S. Coronavirus Disease (COVID-19) Weekly Epidemiological Updates and Monthly Operational Updates. 2022. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 21 August 2022).
- Wuyam, B.; Baillieul, S.; Doutreleau, S.; Vergès, S. Adaptation à l’altitude dans les maladies respiratoires. Rev. Mal. Respir. 2022. [Google Scholar] [CrossRef] [PubMed]
- Asif, S.; Wenhui, Y.; Jin, H.; Jinhai, S. Classification of COVID-19 from chest X-ray images using deep convolutional neural network. In Proceedings of the 2020 IEEE 6th International Conference on Computer and Communications (ICCC), Chengdu, China, 11–14 December 2020; pp. 426–433. [Google Scholar]
- World Health Organization. Episode# 14-COVID-19-Tests; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/media-resources/science-in-5/episode-14—COVID-19—tests (accessed on 21 August 2022).
- Jawerth, N. Comment la RT-PCR en temps réel permet-elle de détecter le virus de la COVID-19. IAEA L’Agence Int. De L’énergie Atomique. Mal. Infect. 2020, 61, 2. [Google Scholar]
- World Health Organization. Use of Chest Imaging in COVID-19: A Rapid Advice Guide, 11 June 2020; Technical Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Farahat, Z.; Souissi, N.; Belmekki, M.; Megdiche, K.; Benamar, S.; Bennani, Y.; Bencherif, S.; Ngote, N. Diabetic Retinopathy: New Perspectives with Artificial Intelligence. In Proceedings of the 2021 Fifth International Conference On Intelligent Computing in Data Sciences (ICDS), Fez, Morocco, 20–22 October 2021; pp. 1–7. [Google Scholar]
- Eaton, S.L.; Roche, S.L.; Llavero Hurtado, M.; Oldknow, K.J.; Farquharson, C.; Gillingwater, T.H.; Wishart, T.M. Total protein analysis as a reliable loading control for quantitative fluorescent Western blotting. PLoS ONE 2013, 8, e72457. [Google Scholar] [CrossRef]
- Gargeya, R.; Leng, T. Automated identification of diabetic retinopathy using deep learning. Ophthalmology 2017, 124, 962–969. [Google Scholar] [CrossRef]
- Weng, S.F.; Reps, J.; Kai, J.; Garibaldi, J.M.; Qureshi, N. Can machine-learning improve cardiovascular risk prediction using routine clinical data? PLoS ONE 2017, 12, e0174944. [Google Scholar] [CrossRef] [Green Version]
- Soule, H.L. Les Enjeux Politique et Bioethique de L’Usage de L’Intelligence Artificielle Dans la Gestion du Coronavirus. Available online: https://revues.acaref.net/wp-content/uploads/sites/3/2021/12/Hayatou-Lay-SOULE.pdf (accessed on 21 August 2022).
- Munusamy, H.; Muthukumar, K.J.; Gnanaprakasam, S.; Shanmugakani, T.R.; Sekar, A. FractalCovNet architecture for COVID-19 chest X-ray image classification and CT-scan image segmentation. Biocybern. Biomed. Eng. 2021, 41, 1025–1038. [Google Scholar] [CrossRef]
- Nishio, M.; Noguchi, S.; Matsuo, H.; Murakami, T. Automatic classification between COVID-19 pneumonia, non-COVID-19 pneumonia, and the healthy on chest X-ray image: Combination of data augmentation methods. Sci. Rep. 2020, 10, 17532. [Google Scholar] [CrossRef]
- Ucar, F.; Korkmaz, D. COVIDiagnosis-Net: Deep Bayes-SqueezeNet based diagnosis of the coronavirus disease 2019 (COVID-19) from X-ray images. Med. Hypotheses 2020, 140, 109761. [Google Scholar] [CrossRef]
- Maftouni, M.; Law, A.C.C.; Shen, B.; Grado, Z.J.K.; Zhou, Y.; Yazdi, N.A. A robust ensemble-deep learning model for COVID-19 diagnosis based on an integrated CT scan images database. In Proceedings of the IIE Annual Conference. Proceedings. Institute of Industrial and Systems Engineers (IISE), Online, 22–25 May 2021; pp. 632–637. [Google Scholar]
- Tripathi, S.; Shetty, S.; Jain, S.; Sharma, V. Lung disease detection using deep learning. Int. J. Innov. Technol. Explor. Eng. 2021, 10, 8. [Google Scholar]
- Zhang, J.; Xie, Y.; Pang, G.; Liao, Z.; Verjans, J.; Li, W.; Sun, Z.; He, J.; Li, Y.; Shen, C.; et al. Viral pneumonia screening on chest X-rays using confidence-aware anomaly detection. IEEE Trans. Med. Imaging 2020, 40, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Sarki, R.; Ahmed, K.; Wang, H.; Zhang, Y.; Wang, K. Automated detection of COVID-19 through convolutional neural network using chest x-ray images. PLoS ONE 2022, 17, e0262052. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, T.; Ozyurt, F.; Dogan, S.; Subasi, A. A novel Covid-19 and pneumonia classification method based on F-transform. Chemom. Intell. Lab. Syst. 2021, 210, 104256. [Google Scholar] [CrossRef]
- Shelke, A.; Inamdar, M.; Shah, V.; Tiwari, A.; Hussain, A.; Chafekar, T.; Mehendale, N. Chest X-ray classification using deep learning for automated COVID-19 screening. SN Comput. Sci. 2021, 2, 300. [Google Scholar] [CrossRef] [PubMed]
- ElAraby, M.E.; Elzeki, O.M.; Shams, M.Y.; Mahmoud, A.; Salem, H. A novel Gray-Scale spatial exploitation learning Net for COVID-19 by crawling Internet resources. Biomed. Signal Process. Control 2022, 73, 103441. [Google Scholar] [CrossRef]
- Saba, L.; Agarwal, M.; Patrick, A.; Puvvula, A.; Gupta, S.K.; Carriero, A.; Laird, J.R.; Kitas, G.D.; Johri, A.M.; Balestrieri, A.; et al. Six artificial intelligence paradigms for tissue characterisation and classification of non-COVID-19 pneumonia against COVID-19 pneumonia in computed tomography lungs. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 423–434. [Google Scholar] [CrossRef]
- Shi, F.; Xia, L.; Shan, F.; Song, B.; Wu, D.; Wei, Y.; Yuan, H.; Jiang, H.; He, Y.; Gao, Y.; et al. Large-scale screening to distinguish between COVID-19 and community-acquired pneumonia using infection size-aware classification. Phys. Med. Biol. 2021, 66, 065031. [Google Scholar] [CrossRef]
- Nguyen, D.; Kay, F.; Tan, J.; Yan, Y.; Ng, Y.S.; Iyengar, P.; Peshock, R.; Jiang, S. Deep learning–based COVID-19 pneumonia classification using chest CT images: Model generalizability. Front. Artif. Intell. 2021, 4, 694875. [Google Scholar] [CrossRef]
- Pathan, S.; Siddalingaswamy, P.; Kumar, P.; MM, M.P.; Ali, T.; Acharya, U.R. Novel ensemble of optimized CNN and dynamic selection techniques for accurate Covid-19 screening using chest CT images. Comput. Biol. Med. 2021, 137, 104835. [Google Scholar] [CrossRef] [PubMed]
- Zuiderveld, K., VIII. Contrast limited adaptive histogram equalization. Graph. Gems 1994, 474–485. Available online: https://cir.nii.ac.jp/crid/1570009751230513024 (accessed on 21 August 2022).
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Beach, CA, USA, 10–15 June 2019; pp. 6105–6114. [Google Scholar]
- Shams, M.; Elzeki, O.; Abd Elfattah, M.; Hassanien, A. Chest X-ray Images with Three Classes: COVID-19, Normal, and Pneumonia. Mendeley Data 2020. [Google Scholar] [CrossRef]
- Morozov, S.P.; Andreychenko, A.; Pavlov, N.; Vladzymyrskyy, A.; Ledikhova, N.; Gombolevskiy, V.; Blokhin, I.A.; Gelezhe, P.; Gonchar, A.; Chernina, V.Y. Mosmeddata: Chest ct scans with covid-19 related findings dataset. arXiv 2020, arXiv:2005.06465. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Computer Vision—ECCV 2016: 14th European Conference, Amsterdam, The Netherlands, 11–14 October 2016; Proceedings Part IV 14; Springer: Cham, Switzerland, 2016; pp. 630–645. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Dataset | Architecture | Methods | Classes | Accuracy |
|---|---|---|---|---|---|
| Tripathi et al. [19] | Chest X-Ray 14 | CNN+VGG+STN | DL | 3 | 89.77% |
| Zhang et al. [20] | CXR dataset | Deep CNN | DL | 2 | 95.2% |
| Sarki et al. [21] | CIDC | VGG16 | TL | 2 | 100% |
| 3 | 87.5% | ||||
| Proposed CNN | DL | 2 | 97.67% | ||
| 3 | 93.75% | ||||
| Tuncer et al. [22] | Undefined | F-transform, MKLBP and SVM | F-transform and MKLBP | 3 | 97.01% |
| Nishio et al. [16] | Public datasets | VGG16 | DL and TL | 3 | 83.6% |
| Proposed CNN | Less than 80% | ||||
| Asif et al. [5] | COVID-chest Xray-dataset | Inception-v3 | TL | 3 | More than 98% |
| Shelke et al. [23] | India Images | VGG16 | DL | 3 | 95.9% |
| denseNet161 | 2 | 98.9% | |||
| ResNet-18 | 3 | 76% | |||
| Ucar and Korkmaz [17] | Public dataset named COVIDx | COVIDiagnosis-Net, based on SqueezeNet | D L | 3 | 98.3% |
| ElAraby et al. [24] | CXR | GSEN | DL + Crawler 2 | 2 | 95.60% |
| 3 | 92.76% |
| Article | Dataset | Architecture | Methods | Classes | Accuracy (%) |
|---|---|---|---|---|---|
| Saba et al. [25] | Covid dataset | iCNN & CNN | DL | 2 | 99.30% & 99.53% |
| VGG19 & IV3 | TL | 2 | 99.53% & 94.84% | ||
| k-NN & RF | ML | 2 | 96.84% & 74.58% | ||
| Shi et al. [26] | large-scale dataset CT scans | Proposed-CNN LR, SVM, NN | DL & ML | Groups with different ranges of infected lesion sizes | 87.9% |
| Maftouni et al. [18] | Covid-CT dataset | DenseNet-121 | DL | 3 | 94.42% |
| Residual Attention92 | 3 | 90.47% | |||
| proposed with FC | 3 | 98.32% | |||
| proposed with FC+VM | 3 | 97.93% | |||
| Nguyen et al. [27] | CC-CCII Dataset-China | CNN | DL | 2 (Covid+ & Covid-) | 87%/82.6% (UTSW) |
| Covid-CTset-Iran | 97%/98.8% (CC-CCCI) | ||||
| MosMedData-Russa | 86%/87.3% Covid-CTset) | ||||
| Pathan et al. [28] | Various sources | Proposed CNN: ResNet-50, AlexNet, VGG19, Densenet & Inception V3 | TL | 2(Covid+ & Covid-) | 96% |
| Non-Coronavirus Pneumonia (n = 47) | Coronavirus Pneumonia (n = 51) | Pneumonia (n = 29) | |
|---|---|---|---|
| Age (year): | |||
| <20 | 4 (8.51%) | 7 (13.73%) | 3 (10.34%) |
| 20-39 | 16 (34.04%) | 19 (37.25%) | 11 (37.93%) |
| 40-59 | 19 (40.43%) | 17 (33.33%) | 09 (31.04%) |
| ≥60 | 08 (17.02%) | 08 (15.69%) | 06 (20.69%) |
| Sex: | |||
| Male | 26 (55.32%) | 23 (45.10%) | 18 (62.07%) |
| Female | 21 (44.68%) | 28 (54.90%) | 11 (37.93%) |
| Presence of Fever: | |||
| Fever | 34 (72.34%) | 46 (90.19%) | 23 (79.31%) |
| No fever | 13 (27.66%) | 5 (9.81%) | 6 (20.69%) |
| White blood cell Count: | |||
| Normal | 11 (23.41%) | 3 (5.88%) | 5 (17.24%) |
| Elevated | 36 (76.59%) | 48 (94.12%) | 24 (82.76%) |
| Lymphocyte count: | |||
| Normal | 39 (82.97%) | 9 (17.65%) | 11 (37.93%) |
| Decreased | 8 (17.03%) | 42 (82.35%) | 18 (62.07%) |
| Comorbidities: | |||
| Cardiovascular Disease | 3 (6.38%) | 9 (17.64%) | 6 (20.69%) |
| Hypertension | 8 (17.02%) | 13 (25.49%) | 11 (37.93%) |
| COPD | 6 (12.76%) | 7 (13.72%) | 4 (13.79%) |
| Diabetes | 5 (10.64%) | 12 (23.53%) | 8 (27.59%) |
| Chronic liver Disease | 1 (2.13%) | 0 (0%) | 0 (0%) |
| Chronic kidney Disease | 0 (0%) | 1 (1.96%) | 0 (0%) |
| Malignant tumor | 0 (0%) | 2 (3.92%) | 0 (0%) |
| HIV | 0 (0%) | 0 (0%) | 0 (0%) |
| Severity: | |||
| Mild | - | 29 (57.7%) | - |
| Medium | - | 16 (15.5%) | - |
| Severe | - | 4 (16.3%) | - |
| Critical | - | 2 (10%) | - |
| Parameter | Value |
|---|---|
| Input size | |
| Batch size | 8 |
| Learning rate | |
| Optimizer | Adam |
| Epochs | 100 |
| Loss function | Categorical Crossentropy |
| Kernel initializer | Orthogonal |
| Classes | Precision | Recall | F1-Score |
|---|---|---|---|
| COVID-19 | 100% | 100% | 100% |
| Normal | 99% | 100% | 100% |
| Pneumonia | 100% | 99% | 100% |
| Architecture | Accuracy | Training Time (in s) | Inference Time (in s) |
|---|---|---|---|
| DenseNet121 | 97.73% | 1229.04 | 2.44 |
| ResNet152V2 | 95.18% | 1647.44 | 5.48 |
| EfficientNetB7 | 99.81% | 1366.84 | 2.51 |
| Classes | Precision | Recall | F1-Score |
|---|---|---|---|
| COVID-19 | 99% | 100% | 100% |
| Normal | 100% | 99% | 100% |
| Pneumonia | 100% | 100% | 100% |
| Architecture | Accuracy | Training Time (in s) | Inference Time (in s) |
|---|---|---|---|
| DenseNet121 | 92.63% | 20,330.95 | 40.76 |
| ResNet152V2 | 97.83% | 15,897.32 | 30.87 |
| EfficientNetB7 | 99.88% | 21,960.07 | 41.50 |
| Classes | Precision | Recall | F1-Score |
|---|---|---|---|
| Pneumonia | 95% | 93% | 93% |
| COVID-19 | 94% | 95% | 94% |
| Normal | 96% | 97% | 97% |
| Approach | CT Scan Modality | X-ray Modality |
|---|---|---|
| Tripathi et al. [19] | – | 89.77% |
| Sarki et al. [21] | – | 93.75% |
| Tuncer et al. [22] | – | 97.01% |
| Nishio et al. [16] | – | 83.6% |
| Asif et al. [5] | – | 98% |
| Shelke et al. [23] | – | 95.9% |
| Ucar and Korkmaz [17] | – | 98.3% |
| ElAraby et al. [24] | – | 92.76% |
| Maftouni et al. [18] | 98.32% | – |
| Our proposed approach | 99.88% | 99.81% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moussaid, A.; Zrira, N.; Benmiloud, I.; Farahat, Z.; Karmoun, Y.; Benzidia, Y.; Mouline, S.; El Abdi, B.; Bourkadi, J.E.; Ngote, N. On the Implementation of a Post-Pandemic Deep Learning Algorithm Based on a Hybrid CT-Scan/X-ray Images Classification Applied to Pneumonia Categories. Healthcare 2023, 11, 662. https://doi.org/10.3390/healthcare11050662
Moussaid A, Zrira N, Benmiloud I, Farahat Z, Karmoun Y, Benzidia Y, Mouline S, El Abdi B, Bourkadi JE, Ngote N. On the Implementation of a Post-Pandemic Deep Learning Algorithm Based on a Hybrid CT-Scan/X-ray Images Classification Applied to Pneumonia Categories. Healthcare. 2023; 11(5):662. https://doi.org/10.3390/healthcare11050662
Chicago/Turabian StyleMoussaid, Abdelghani, Nabila Zrira, Ibtissam Benmiloud, Zineb Farahat, Youssef Karmoun, Yasmine Benzidia, Soumaya Mouline, Bahia El Abdi, Jamal Eddine Bourkadi, and Nabil Ngote. 2023. "On the Implementation of a Post-Pandemic Deep Learning Algorithm Based on a Hybrid CT-Scan/X-ray Images Classification Applied to Pneumonia Categories" Healthcare 11, no. 5: 662. https://doi.org/10.3390/healthcare11050662