
Occupational Exposure to Inhalational Anesthetics and Teratogenic Effects: A Systematic Review
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies
2.2. Search Strategies and Data Resources
2.3. Data Extraction
2.4. Quality Assessment
2.5. Collecting, Summarizing and Reporting Results
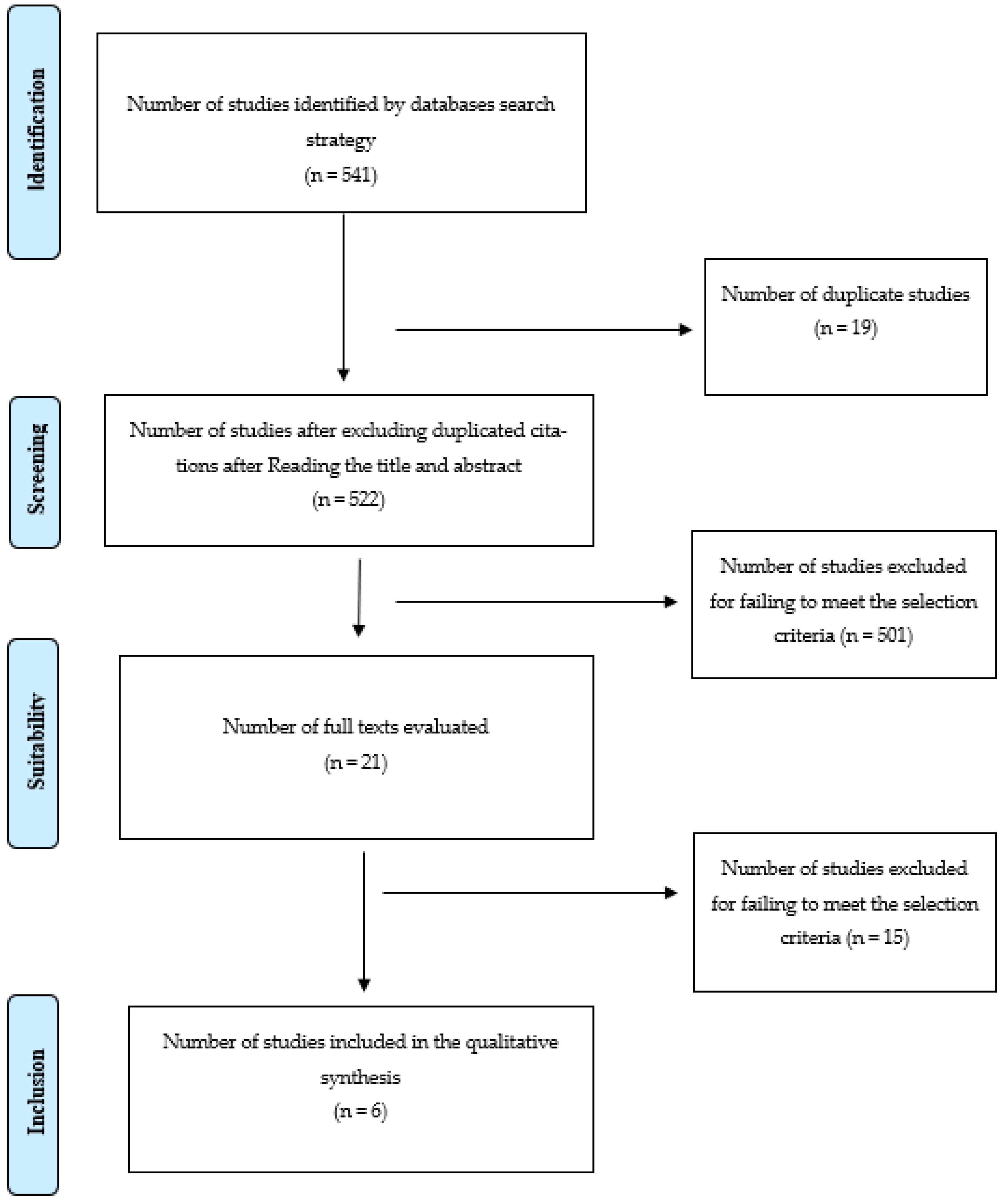
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saleh, M.A.; Wali, M.H.; Hassan, O.M.; Bayomy, H.; Nabil, N. Occupational Hazards Risk Assessment of Nurses Working in Operating Roms. Egypt. J. Occup. Med. 2020, 44, 793–808. [Google Scholar]
- da Costa, M.G.; Kalmar, A.; Struys, M. Inhaled Anesthetics: Environmental Role, Occupational Risk, and Clinical Use. J. Clin. Med. 2021, 10, 1306. [Google Scholar] [CrossRef] [PubMed]
- Vaĭsman, A.I. Usloviia truda v operatisionnykh i ikh vliianie na zdorov’e anesteziologov Working conditions in the operating room and their effect on the health of anesthetists. Eksperimental’naia Khirurgiia I Anesteziol. 1967, 12, 44–49. [Google Scholar]
- Boivin, J.F. Risk of spontaneous abortion in women occupationally exposed to anaesthetic gases: A meta-analysis. Occup. Environ. Med. 1997, 54, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Warembourg, C.; Cordier, S.; Garlantézec, R. An update systematic review of fetal death, congenital anomalies, and fertility disorders among health care workers. Am. J. Ind. Med. 2017, 60, 578–590. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Xu, Y.; Yin, H.; Wang, J.; Chen, K.; Li, Y. Developmental toxicity research of ginsenoside Rb1 using a whole mouse embryo culture model. Birth Defects Res. Part B Dev. Reprod. Toxicol. 2005, 74, 207–209. [Google Scholar] [CrossRef]
- Cui, Y.; Liu, J.; Zhu, Y.; Xie, K.; Yu, J.; Yu, L.; Wang, Y. Effects of sevoflurane on reproductive function of male rats and its main mechanism of action. Inhal. Toxicol. 2019, 31, 392–398. [Google Scholar] [CrossRef]
- Wen, J.; Xu, J.; Mathena, R.P.; Choi, J.H.; Mintz, C.D. Early Isoflurane Exposure Impairs Synaptic Development in Fmr1 KO Mice via the mTOR Pathway. Neurochem. Res. 2021, 46, 1577–1588. [Google Scholar] [CrossRef]
- Menon, J.M.; van Luijk, J.A.; Swinkels, J.; Lukas, E.; Ritskes-Hoitinga, M.; Roeleveld, N.; Schlünssen, V.; Mandrioli, D.; Hoffmann, S.; Popa, M.; et al. A health-based recommended occupational exposure limit for nitrous oxide using experimental animal data based on a systematic review and dose-response analysis. Environ. Res. 2021, 201, 111575. [Google Scholar] [CrossRef]
- Çakmak, G.; Eraydın, D.; Berkkan, A.; Yağar, S.; Burgaz, S. Genetic damage of operating and recovery room personnel occupationally exposed to waste anaesthetic gases. Hum. Exp. Toxicol. 2019, 38, 3–10. [Google Scholar] [CrossRef]
- Lucio, L.M.C.; Braz, M.G.; do Nascimento Junior, P.; Braz, J.R.C.; Braz, L.G. Occupational hazards, DNA damage, and oxidative stress on exposure to waste anesthetic gases. Braz. J. Anesthesiol. 2018, 68, 33–41. [Google Scholar] [CrossRef]
- Tompa, A.; Bíró, A.; Jakab, M. Cytogenetic, DNA-repair and Apoptosis Studies in Hospital Nurses’ Peripheral Blood Lymphocytes Occupationally Exposed to Volatile Anesthetic Gases. Int. J. Nurs. Clin. Pract. 2018, 5, 274. [Google Scholar] [CrossRef] [Green Version]
- Szyfter, K.; Stachecki, I.; Kostrzewska-Poczekaj, M.; Szaumkessel, M.; Szyfter-Harris, J.; Sobczyński, P. Exposure to volatile anaesthetics is not followed by a massive induction of single-strand DNA breaks in operation theatre personnel. J. Appl. Genet. 2016, 57, 343–348. [Google Scholar] [CrossRef] [Green Version]
- El-Ebiary, A.; Abuelfadl, A.; Sarhan, N.; Othman, M. Assessment of genotoxicity risk in operation room personnel by the alkaline comet assay. Hum. Exp. Toxicol. 2013, 32, 563–570. [Google Scholar] [CrossRef]
- Schifilliti, D.; Mondello, S.; D’Arrigo, M.G.; Chillè, G.; Fodale, V. Genotoxic effects of anesthetic agents: An update. Expert Opin. Drug Saf. 2011, 10, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Lawson, C.C.; Rocheleau, C.M.; Whelan, E.A.; Lividoti Hibert, E.N.; Grajewski, B.; Spiegelman, D.; Rich-Edwards, J.W. Occupational exposures among nurses and risk of spontaneous abortion. Am. J. Obstet. Gynecol. 2012, 206, 327.e1–327.e8. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Kang, M.-Y.; Kim, D.; Park, J.; Eom, H.; Kim, E.-A. Adverse pregnancy outcomes in healthcare workers: A Korean nationwide population-based study. Int. Arch. Occup. Environ. Health 2017, 90, 501–506. [Google Scholar] [CrossRef]
- Shirangi, A.; Fritschi, L.; Holman, C.D.J. Maternal occupational exposures and risk of spontaneous abortion in veterinary practice. Occup. Environ. Med. 2008, 65, 719–725. [Google Scholar] [CrossRef]
- Teschke, K.; Abanto, Z.; Arbour, L.; Beking, K.; Chow, Y.; Ma, R.P.G.; Jong, B.; Le, N.D.; Ratner, P.; Spinelli, J.J.; et al. Exposure to anesthetic gases and congenital anomalies in offspring of female registered nurses. Am. J. Ind. Med. 2011, 54, 118–127. [Google Scholar] [CrossRef]
- Buhre, W.; Disma, N.; Hendrickx, J.; DeHert, S.; Hollmann, M.W.; Huhn, R.; Jakobsson, J.; Nagele, P.; Peyton, P.; Vutskits, L. European Society of Anaesthesiology Task Force on Nitrous Oxide: A narrative review of its role in clinical practice. Br. J. Anaesth. 2019, 122, 587–604. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.M.; Ayora, A.; Barbara, A.; Gascó, A.; Medina, J.A.; Sol, J.; Sol, M.H. Occupational exposure to volatile anaesthetics: A systematic review. Occup. Med. 2016, 66, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Tulandi, T.; Al-Fozan, H. Definition and etiology of recurrent pregnancy loss. In This Topic Last Updated: 11 January 2017; Lockwood, C., Ed.; UpToDate: Waltham, MA, USA, 2017. [Google Scholar]
- Anderson, M.; Goldman, R.H. Occupational Reproductive Hazards for Female Surgeons in the Operating Room: A Review. JAMA Surg. 2020, 155, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.A.; El Dib, R.P.; Figueiredo, D.B.S.; Braz, L.G.; Braz, M.G. Spontaneous abortion in women occupationally exposed to inhalational anesthetics: A critical systematic review. Environ. Sci. Pollut. Res. 2021, 28, 10436–10449. [Google Scholar] [CrossRef]
- Ayoğlu, H.; Ayoğlu, F.N. Occupational Risks for Anaesthesiologists and Precautions. Turk. J. Anaesthesiol. Reanim. 2021, 49, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Mangla, M. Occupational risks to pregnant obstetrics and gynaecology trainees and physicians: Is it time to think about this? J. Mother Child 2022, 26, 111–117. [Google Scholar]
- Quansah, R.; Jaakkola, J.J. Occupational Exposures and Adverse Pregnancy Outcomes Among Nurses: A Systematic Review and Meta-Analysis. J. Women’s Health 2010, 19, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Molnár, L.; Tankó, B.; Fülesdi, B.; Molnár, C. Occupational Hazards of Halogenated Volatile Anesthetics and their Prevention: Review of the Literature. J. Addict. Res. Ther. 2014, 5, 1000426. [Google Scholar] [CrossRef] [Green Version]
- Scheftel, J.M.; Elchos, B.L.; Rubin, C.S.; Decker, J.A. Review of hazards to female reproductive health in veterinary practice. J. Am. Vet. Med. Assoc. 2017, 250, 862–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Lowe, G.; Twaddle, S. The Scottish Intercollegiate Guidelines Network (Sign): An Update. Scott. Med. J. 2005, 50, 51–52. [Google Scholar] [CrossRef] [PubMed]
- Allweiler, S.I.; Kogan, L.R. Inhalation anesthetics and the reproductive risk associated with occupational exposure among women working in veterinary anesthesia. Vet. Anaesth. Analg. 2013, 40, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Nagella, A.B.; Ravishankar, M.; Hemanth-Kumar, V.R. Anaesthesia practice and reproductive outcomes: Facts unveiled. Indian J. Anaesth. 2015, 59, 706–714. [Google Scholar] [CrossRef]
- Eftimova, B.; Sholjakova, M.; Mirakovski, D.; Hadzi-Nikolova, M. Health Effects Associated With Exposure to Anesthetic Gas Nitrous Oxide-N2O in Clinical Hospital—Shtip Personel. Open Access Maced. J. Med. Sci. 2017, 5, 800–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borayek, G.E.; El-Magd, S.A.; El-Gohary, S.S.; El-Naggar, A.M.; Hammouda, M.A. Occupational genotoxic effects among a group of nurses exposed ato anesthetic gases in operating rooms at zagazic university hospitals. Egypt. J. Occup. Med. 2018, 42, 105–122. [Google Scholar]
- Olika, M.K.; Dessalegn, Z.M.; Mekonin, G.T.; Aboye, M.B.; Wedajo, M.B.; Ilala, T.T.; Abebe, D.M.; Demissie, W.R. Effect of Inhalational Anesthetics Exposure on Reproductive Outcomes and Its Predictors Among Healthcare Personnel in Jimma Zone Public Hospitals: A Comparative Cross-Sectional Study. Int. J. Women’s Health 2022, 14, 1555–1568. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Casey, I. Waste Anesthetic Gases and the Incidence of Miscarriage. Int. J. Nurs. Health Sci. 2021, 1, 2021–2035. [Google Scholar]
- Hays, S.R. Inhalation anesthetic agents: Clinical effects and uses. In This Topic Last Updated: 8 February 2019; Joshi, G.P., UpToDate Inc., Eds.; UpToDate Inc.: Waltham, MA, USA, 2020; Available online: http://www.uptodate.com (accessed on 12 November 2022).


{kind=link}
| Study | Type of Study | Study Population | Data Collection Method | Type of Inhalational Anesthetic | Results | SIGN Evidence/Recommendation |
|---|---|---|---|---|---|---|
| Lawson et al. [16] | Retrospective cohorts | 7842 nurses exposed: working with inhalational anesthetics more than 1 h per day | Questionnaire on work history and occurrence of spontaneous abortions | Halothane, isoflurane, enflurane and nitrous oxide | No increased risk of spontaneous abortion in exposed nurses | 2+/C |
| Allweiler et al. [33] | Retrospective cohorts | Female veterinarians 295 exposed: working in anesthesia 86 non-exposed: working in intensive care | Questionnaire on work history and occurrence of spontaneous abortion or congenital malformations | Not specified | No increased risk of spontaneous abortion or congenital malformations in exposed veterinary females | 2+/C |
| Nagella et al. [34] | Retrospective cohorts | 345 female anesthesiologists exposed: working in the operating room during the first trimester of gestation Not exposed: working outside the operating room during the first trimester of gestation. | Questionnaire on work history and occurrence of spontaneous abortion or congenital malformations | Isoflurane, halothane, desflurane, sevoflurane and nitrous oxide | Increased risk of spontaneous abortions in exposed women Association between time worked and congenital malformations No association between type of inhalational anesthetics and spontaneous abortions or congenital malformations | 2-/ No recommendation |
| Eftimova et al. [35] | Retrospective cohorts | 23 exposed workers: working in operating room 20 non-exposed workers: working in intensive care | Questionnaire on work history and the occurrence of spontaneous abortion Measurement of nitrous oxide concentration in the operating room | Nitrous oxide | No increased risk of spontaneous abortions in exposed women No association between nitrous oxide concentrations and spontaneous abortions | 2++/B |
| Borayek et al. [36] | Retrospective cohorts | 32 exposed nurses: working in the operating room more than 6 h per day for 6 days per week 32 non-exposed nurses: working in hospital outpatient clinics | Questionnaire on work history and the occurrence of miscarriages or congenital malformations Measurement of isoflurane concentration in urine Evaluation of chromosomal alterations | Isoflurane | Longer working time in exposed women Higher risk of spontaneous abortions, congenital malformations and chromosomal alterations in exposed women No association between isoflurane in urine and spontaneous abortions, congenital malformations or chromosomal alterations Association between time worked and chromosomal alterations | 2-/ No recommendation |
| Olika et al. [37] | Retrospective cohorts | 146 exposed health professionals: working in the operating room 146 non-exposed health professionals: hospital outpatient clinics | Questionnaire on work history and occurrence of spontaneous abortion or congenital malformations | Not specified | Longer working time in exposed women Increased risk of spontaneous abortions and congenital malformations in exposed women Association between time worked and spontaneous abortion or congenital malformations | 2-/ No recommendation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Álvarez, J.M.; Escribano-Sánchez, G.; Osuna, E.; Molina-Rodríguez, A.; Díaz-Agea, J.L.; García-Sánchez, A. Occupational Exposure to Inhalational Anesthetics and Teratogenic Effects: A Systematic Review. Healthcare 2023, 11, 883. https://doi.org/10.3390/healthcare11060883
García-Álvarez JM, Escribano-Sánchez G, Osuna E, Molina-Rodríguez A, Díaz-Agea JL, García-Sánchez A. Occupational Exposure to Inhalational Anesthetics and Teratogenic Effects: A Systematic Review. Healthcare. 2023; 11(6):883. https://doi.org/10.3390/healthcare11060883
Chicago/Turabian StyleGarcía-Álvarez, José Manuel, Guillermo Escribano-Sánchez, Eduardo Osuna, Alonso Molina-Rodríguez, José Luis Díaz-Agea, and Alfonso García-Sánchez. 2023. "Occupational Exposure to Inhalational Anesthetics and Teratogenic Effects: A Systematic Review" Healthcare 11, no. 6: 883. https://doi.org/10.3390/healthcare11060883