Effect of Three Weeks of High-Intensity, Long-Term Preoperative Rehabilitation for Esophageal Cancer Patients with Stroke Sequelae Who Were Considered Unfit for Surgery Due to Low Activity: A Case Report

 ,
,
Abstract
:1. Introduction
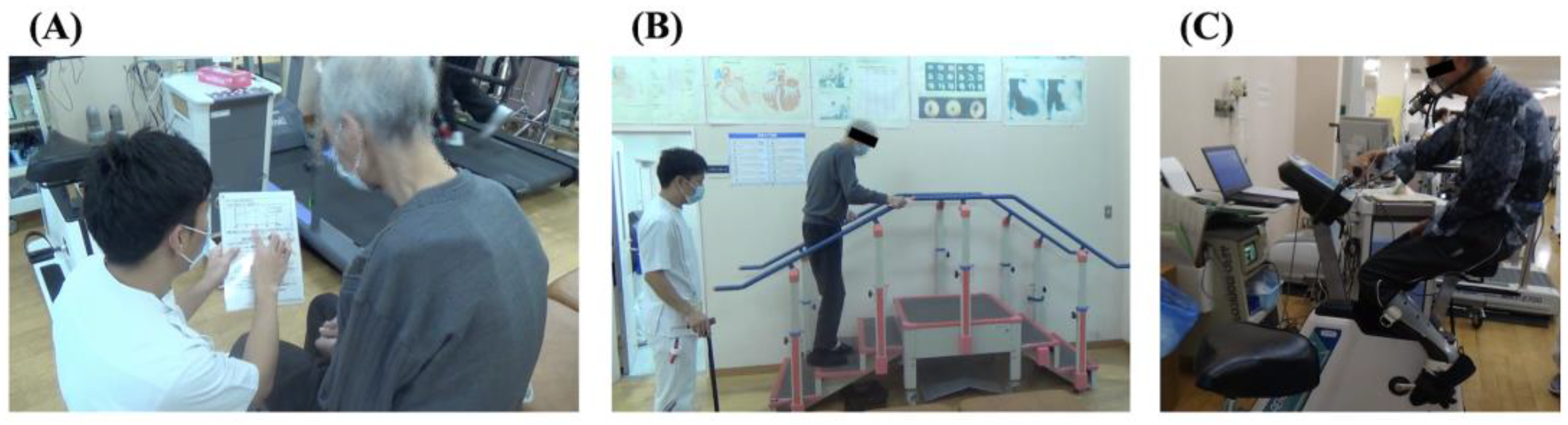
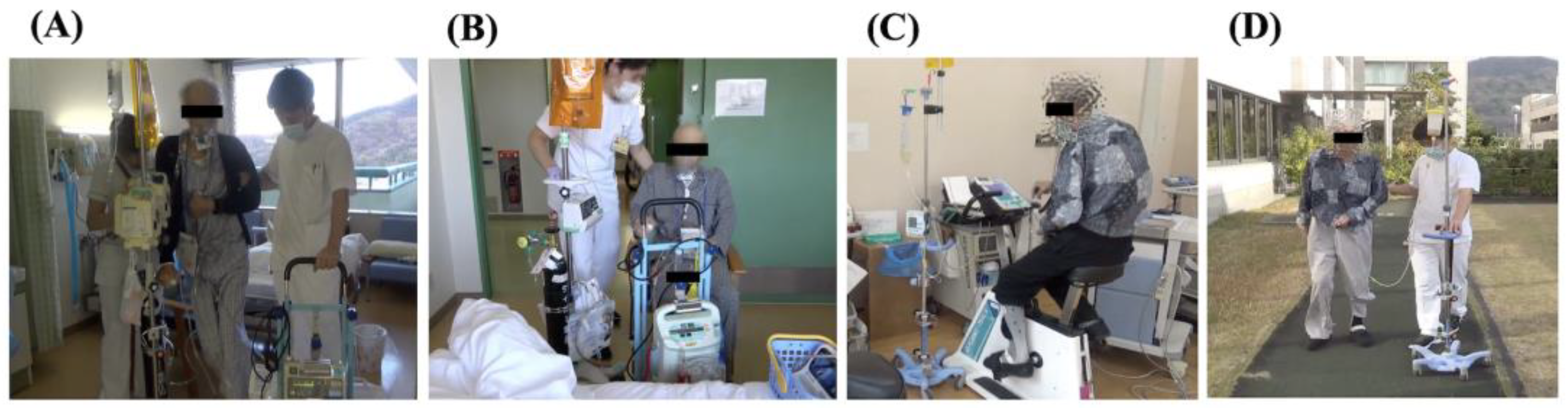
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Japan Esophageal Society. Guidelines for Diagnosis and Treatment of Carcinoma of the Esophagus 2022; Kanehara Syuppann: Tokyo, Japan, 2022; Volume 28. (In Japanese) [Google Scholar]
- The Japan Esophageal Society. Guidelines for Diagnosis and Treatment of Carcinoma of the Esophagus 2012; Kanehara Syuppann: Tokyo, Japan, 2012; Volume 9. (In Japanese) [Google Scholar]
- Zingg, U.; Smithers, B.M.; Gotley, D.C.; Smith, G.; Aly, A.; Clough, A.; Esterman, A.J.; Jamieson, G.G.; Watson, D.I. Factors Associated with Postoperative Pulmonary Morbidity After Esophagectomy for Cancer. Ann. Surg. Oncol. 2011, 18, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Kuppusamy, M.K.; Alderson, D.; Cecconello, I.; Chang, A.; Darling, G.; Davies, A.; D’Journo, X.B.; Gisbertz, S.S.; Griffin, S.M.; et al. Benchmarking Complications Associated with Esophagectomy. Ann. Surg. 2019, 269, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, K.E.; Goldman, L.; Young, B.; Lee, T.H. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: Outcomes and effects on length of stay. Am. J. Med. 2003, 115, 515–520. [Google Scholar] [CrossRef]
- Yamana, I.; Takeno, S.; Hashimoto, T.; Maki, K.; Shibata, R.; Shiwaku, H.; Shimaoka, H.; Shiota, E.; Yamashita, Y. Randomized Controlled Study to Evaluate the Efficacy of a Preoperative Respiratory Rehabilitation Program to Prevent Postoperative Pulmonary Complications after Esophagectomy. Dig. Surg. 2015, 32, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Inoue, J.; Ono, R.; Makiura, D.; Kashiwa-Motoyama, M.; Miura, Y.; Usami, M.; Nakamura, T.; Imanishi, T.; Kuroda, D. Prevention of postoperative pulmonary complications through intensive preoperative respiratory rehabilitation in patients with esophageal cancer. Dis. Esophagus 2013, 26, 68–74. [Google Scholar] [CrossRef]
- Halliday, L.J.; Doganay, E.; Wynter-Blyth, V.A.; Hanna, G.B.; Moorthy, K. The Impact of Prehabilitation on Post-operative Outcomes in Oesophageal Cancer Surgery: A Propensity Score Matched Comparison. J. Gastrointest. Surg. 2021, 25, 2733–2741. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, Y.; Sasaki, A.; Fujii, Y.; Fujisawa, R.; Sasaki, N.; Nikai, H.; Endo, F.; Baba, S.; Hasegawa, Y.; Kimura, T.; et al. Efficacy of enhanced prehabilitation for patients with esophageal cancer undergoing esophagectomy. Esophagus 2021, 18, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Tukanova, K.H.; Chidambaram, S.; Guidozzi, N.; Hanna, G.B.; McGregor, A.H.; Markar, S.R. Physiotherapy Regimens in Esophagectomy and Gastrectomy: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2022, 29, 3148–3167. [Google Scholar] [CrossRef]
- Pandey, S.; Tater, P. Post-stroke Movement Disorders: Clinical Spectrum, Pathogenesis, and Management. Neurol. India 2021, 69, 272–283. [Google Scholar] [CrossRef]
- Miller, E.L.; Murray, L.; Richards, L.; Zorowitz, R.D.; Bakas, T.; Clark, P.; Billinger, S.A. Comprehensive Overview of Nursing and Interdisciplinary Rehabilitation Care of the Stroke Patient: A scientific statement from the American Heart Association. Stroke 2010, 41, 2402–2448. [Google Scholar] [CrossRef] [Green Version]
- Teasdale, G.; Murray, G.; Parker, L.; Jennett, B. Adding up the Glasgow Coma Score. Acta Neurochir. Suppl. (Wien) 1979, 28, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Maas, A.; Lecky, F.; Manley, G.; Stocchetti, N.; Murray, G. The Glasgow Coma Scale at 40 years: Standing the test of time. Lancet Neurol. 2014, 13, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Brott, T.; Adams, H.P., Jr.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [Green Version]
- StatPearls. Muscle Strength Grading. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK436008/ (accessed on 30 December 2022).
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The reliability of the functional independence measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1985, 60, 2020–2027. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Iwata, M.; Kondo, I.; Sato, Y.; Satoh, K.; Soma, M.; Tsushima, E. An ankle-foot orthosis with inhibitor bar: Effect on hemiplegic gait. Arch. Phys. Med. Rehabil. 2003, 84, 924–927. [Google Scholar] [CrossRef]
- González-Rosalén, J.; Benítez-Martínez, J.C.; Medina-Mirapeix, F.; Cuerda-Del Pino, A.; Cervelló, A.; Martín-San Agustín, R. Intra- and Inter-Rater Reliability of Strength Measurements Using a Pull Hand-Held Dynamometer Fixed to the Examiner’s Body and Comparison with Push Dynamometry. Diagnostics 2021, 11, 1230. [Google Scholar] [CrossRef]
- Kinoshita, T.; Nishimura, Y.; Nakamura, T.; Hashizaki, T.; Kojima, D.; Kawanishi, M.; Uenishi, H.; Arakawa, H.; Ogawa, T.; Kamijo, Y.-I.; et al. Effects of physiatrist and registered therapist operating acute rehabilitation (PROr) in patients with stroke. PLoS ONE 2017, 12, e0187099. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, T.; Yoshikawa, T.; Nishimura, Y.; Kamijo, Y.-I.; Arakawa, H.; Nakamura, T.; Hashizaki, T.; Hoekstra, S.P.; Tajima, F. Mobilization within 24 hours of new-onset stroke enhances the rate of home discharge at 6-months follow-up: A prospective cohort study. Int. J. Neurosci. 2021, 131, 1097–1106. [Google Scholar] [CrossRef]
- Nakamura, R.; Watanabe, S.; Handa, T.; Morohashi, I. The relationship between walking speed and muscle strength for knee extension in hemiparetic stroke patients: A follow-up study. Tohoku J. Exp. Med. 1988, 154, 111–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, M.Y.C.; Eng, J.J.; Dawson, A.S.; McKay, H.A.; Harris, J.E. A Community-Based Fitness and Mobility Exercise Program for Older Adults with Chronic Stroke: A Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2005, 53, 1667–1674. [Google Scholar] [CrossRef] [Green Version]
- Pang, M.Y.C.; Eng, J.J.; Dawson, A.S.; Gylfadóttir, S. The use of aerobic exercise training in improving aerobic capacity in individuals with stroke: A meta-analysis. Clin. Rehabil. 2006, 20, 97–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaiki, R.; Kamijo, Y.-I.; Moriki, T.; Umemoto, Y.; Mukai, Y.; Mikami, Y.; Kouda, K.; Ogawa, T.; Nishimura, Y.; Tajima, F. Dose-response Rehabilitation Organized By Pror In Out-patients With Chronic Cerebrovascular Disorder: A single-center retrospective cohort study. J. Stroke Cerebrovasc. Dis. 2022, 31, 106375. [Google Scholar] [CrossRef] [PubMed]
- Guinan, E.M.; Dowds, J.; Donohoe, C.; Reynolds, J.V.; Hussey, J. The physiotherapist and the esophageal cancer patient: From prehabilitation to rehabilitation. Dis. Esophagus 2017, 30, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Haines, K.; Skinner, E.; Berney, S.; Austin Health POST Study Investigators. Association of postoperative pulmonary complications with delayed mobilisation following major abdominal surgery: An observational cohort study. Physiotherapy 2013, 99, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Whibley, J.; Peters, C.J.; Halliday, L.J.; Chaudry, A.M.; Allum, W.H. Poor performance in incremental shuttle walk and cardiopulmonary exercise testing predicts poor overall survival for patients undergoing esophago-gastric resection. Eur. J. Surg. Oncol. 2018, 44, 594–599. [Google Scholar] [CrossRef]
- Steffens, D.; Ismail, H.; Denehy, L.; Beckenkamp, P.R.; Solomon, M.; Koh, C.; Bartyn, J.; Pillinger, N. Preoperative Cardiopulmonary Exercise Test Associated with Postoperative Outcomes in Patients Undergoing Cancer Surgery: A Systematic Review and Meta-Analyses. Ann. Surg. Oncol. 2021, 28, 7120–7146. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Score | Description |
|---|---|
| 0 | Fully active, able to carry on all pre-disease performance without restriction. |
| 1 | Restricted in physically strenuous activity, but ambulatory and capable of performing a light or sedentary work (e.g., light housework or office work). |
| 2 | Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about more than 50% of waking hours. |
| 3 | Capable of only limited selfcare, confined to a bed or a chair for more than 50% of their waking hours. |
| 4 | Completely disabled. Cannot carry out any selfcare. Totally confined to a bed or a chair. |
| On Admission | Day before Surgery | At Discharge | |
|---|---|---|---|
| PS | 3 | 2 | 2 |
| Total FIM | 97 | 117 | 117 |
| Motor subscale | 62 | 82 | 82 |
| Cognition subscale | 35 | 35 | 35 |
| Body weight (kg) | 58.0 | 57.5 | 55.0 |
| CPET | |||
| VO2 max (mL/min) | 821.0 | 959.0 | 980.0 |
| VO2 max (mL/Kg/min) | 14.1 | 16.6 | 17.8 |
| 6 MWT (m) | 105.0 | 125.0 | 128.0 |
| 10 MWT (s) | 33.2 | 30.9 | 26.0 |
| HHD | |||
| Right (N) | 80.0 | 120.0 | 120.0 |
| Left (N) | 42.0 | 82.0 | 82.0 |
| On Admission | Day before Surgery | At Discharge | |
|---|---|---|---|
| FIM of the total | 97 | 117 | 117 |
| Motor subscale | 62 | 82.0 | 82.0 |
| Eating | 6 | 7 | 7 |
| Grooming | 5 | 7 | 7 |
| Bathing | 5 | 6 | 6 |
| Upper body dressing | 5 | 6 | 6 |
| Lower body dressing | 4 | 6 | 6 |
| Toileting | 4 | 6 | 6 |
| Bladder management | 7 | 7 | 7 |
| Bowel management | 7 | 7 | 7 |
| Bed to chair transfer | 4 | 6 | 6 |
| Toilet transfer | 4 | 6 | 6 |
| Shower transfer | 4 | 6 | 6 |
| Locomotion (ambulatory or wheelchair level) | 4 | 6 | 6 |
| Stairs | 3 | 6 | 6 |
| Cognition subscale | 35 | 35 | 35 |
| Cognitive comprehension | 7 | 7 | 7 |
| Expression | 7 | 7 | 7 |
| Social interaction | 7 | 7 | 7 |
| Problem solving | 7 | 7 | 7 |
| Memory | 7 | 7 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinoshita, T.; Nishimura, Y.; Zaiki, R.; Yasuoka, Y.; Umemoto, Y.; Koike, Y.; Kawanishi, M.; Tajima, F. Effect of Three Weeks of High-Intensity, Long-Term Preoperative Rehabilitation for Esophageal Cancer Patients with Stroke Sequelae Who Were Considered Unfit for Surgery Due to Low Activity: A Case Report. Healthcare 2023, 11, 665. https://doi.org/10.3390/healthcare11050665
Kinoshita T, Nishimura Y, Zaiki R, Yasuoka Y, Umemoto Y, Koike Y, Kawanishi M, Tajima F. Effect of Three Weeks of High-Intensity, Long-Term Preoperative Rehabilitation for Esophageal Cancer Patients with Stroke Sequelae Who Were Considered Unfit for Surgery Due to Low Activity: A Case Report. Healthcare. 2023; 11(5):665. https://doi.org/10.3390/healthcare11050665
Chicago/Turabian StyleKinoshita, Tokio, Yukihide Nishimura, Rikito Zaiki, Yoshinori Yasuoka, Yasunori Umemoto, Yumi Koike, Makoto Kawanishi, and Fumihiro Tajima. 2023. "Effect of Three Weeks of High-Intensity, Long-Term Preoperative Rehabilitation for Esophageal Cancer Patients with Stroke Sequelae Who Were Considered Unfit for Surgery Due to Low Activity: A Case Report" Healthcare 11, no. 5: 665. https://doi.org/10.3390/healthcare11050665