
Periodontal Healing after Lower Third Molars Extraction: A Clinical Evaluation of Different Flap Designs

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
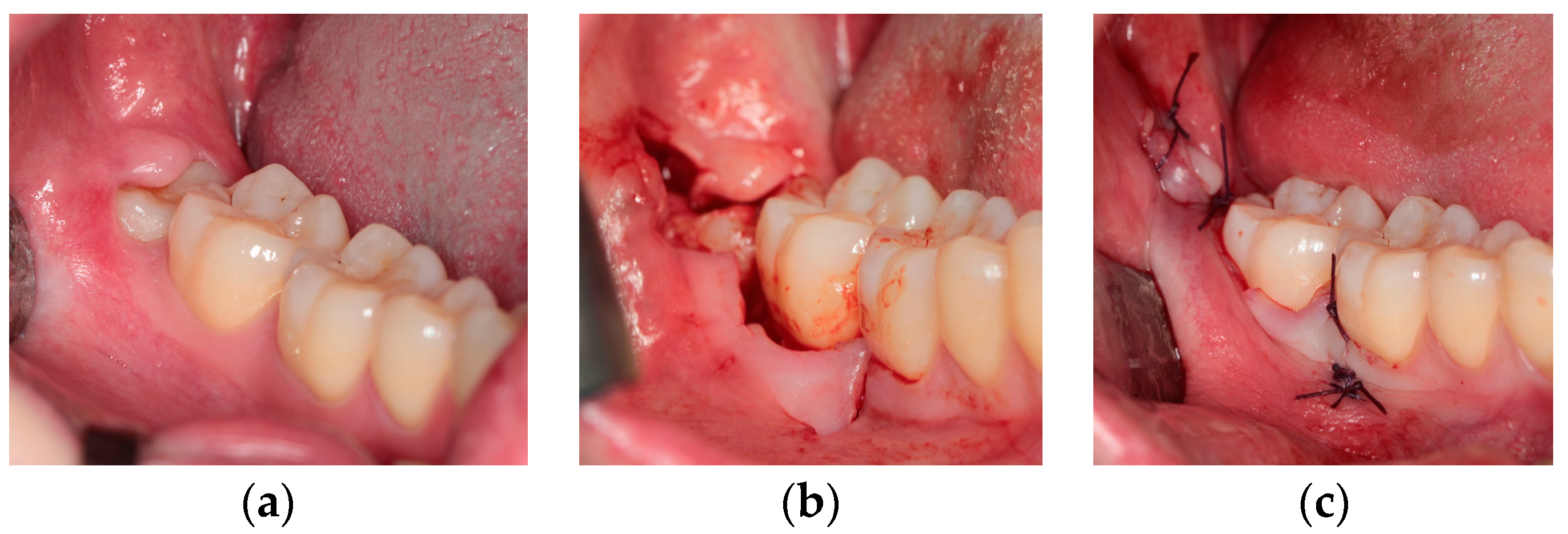
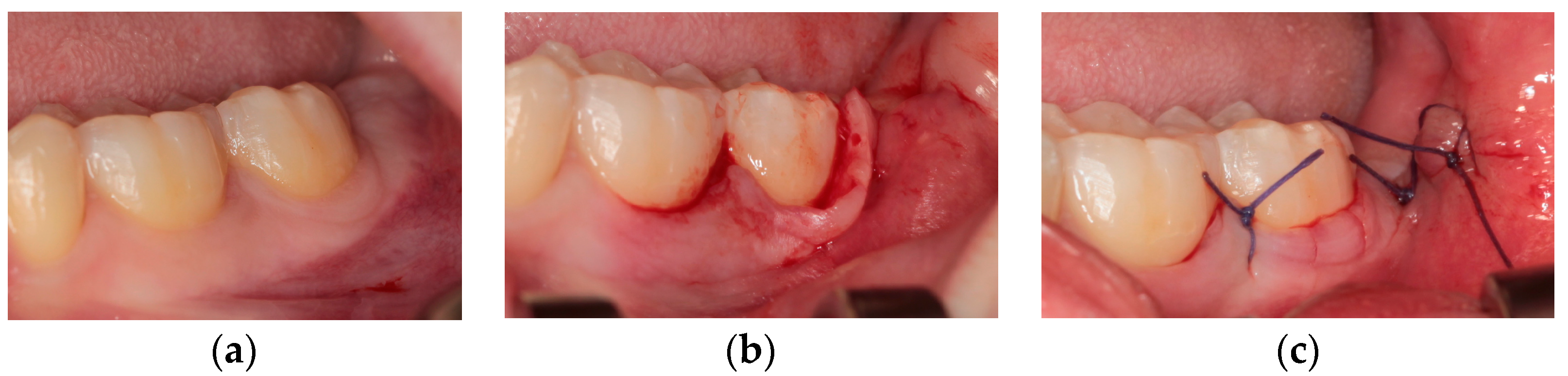
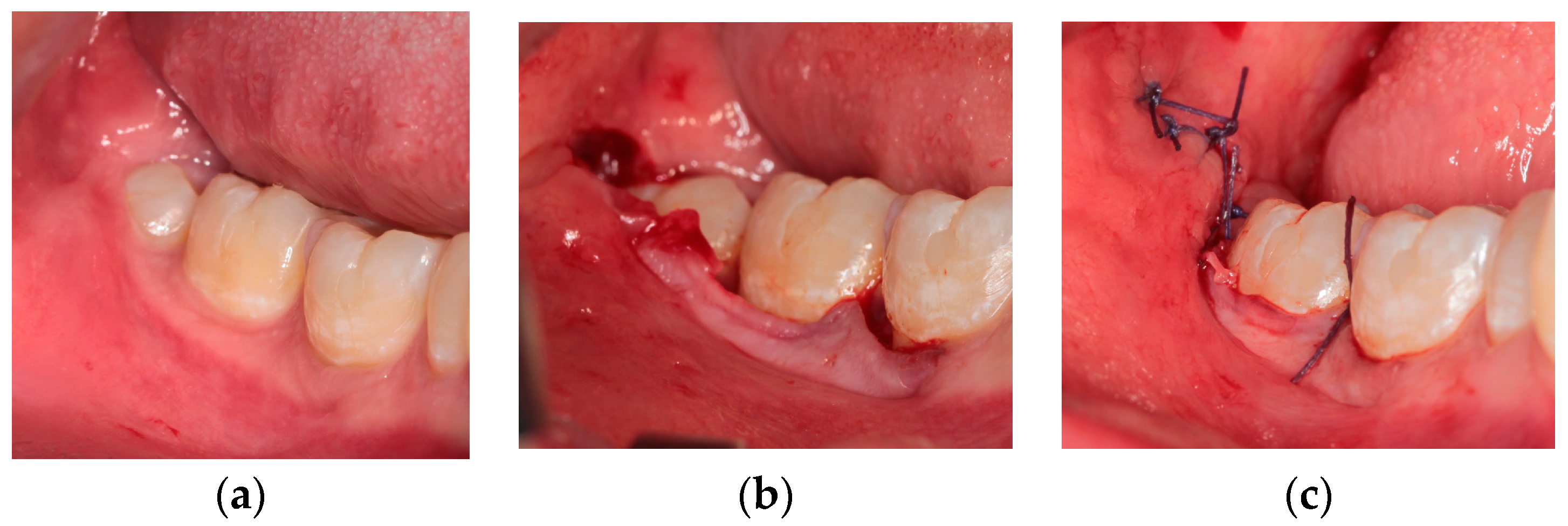
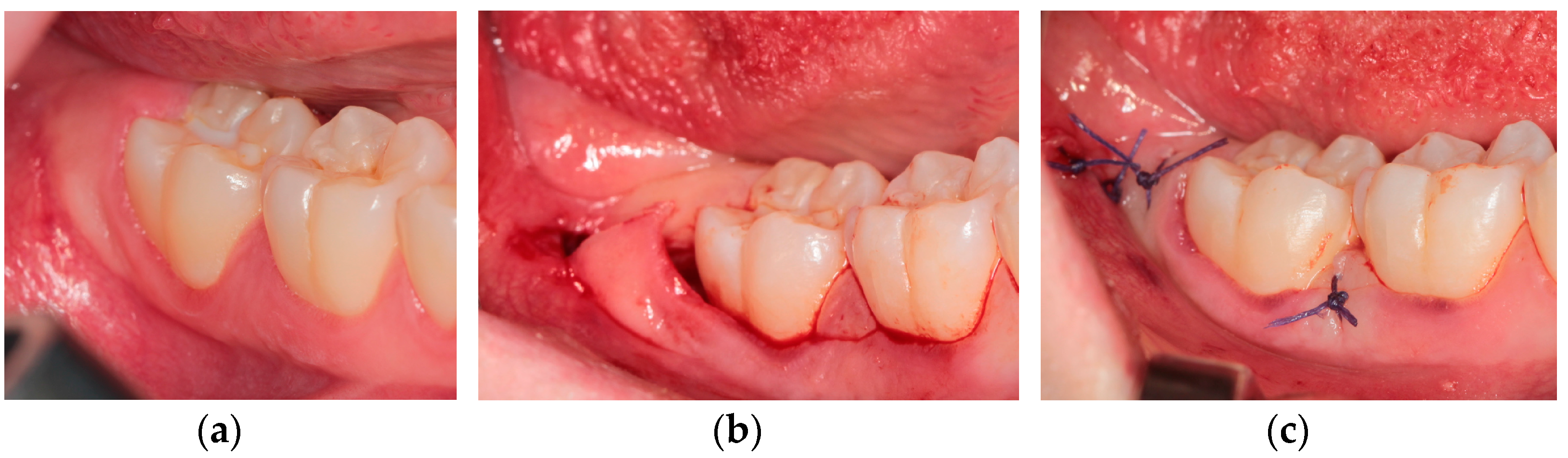
2.2. Surgical Techniques
- Technique I—Trapezoidal flap (TRAP) [18]
- Technique II—Marginal flap (envelope) (MARG) [3]
- Technique III—Flap with papilla detachment (DETP)
- Technique IV—Flap with papilla decapitation (DEC)
2.3. Soft Tissues Assessment
- First molar buccal site PPD, calculated in mm as an average value of mesial, central, and distal sites explored on buccal side of first molar;
- Second molar buccal site PPD/CAL, calculated in mm as an average value of mesial, central, and distal sites explored on buccal side of second molar;
- Second molar distal site VPI, expressed in % as an average value recorded on buccal-distal, central-distal, and lingual-distal sites explored on distal side of second molar;
- Second molar distal site PPD, recorded in mm as an average value recorded on buccal-distal, central-distal, and lingual-distal sites explored on distal side of second molar;
- Second molar buccal-distal site CAL, recorded in mm.
2.4. Statistical Analysis
3. Results
3.1. Study Sample
3.2. Soft Tissues Assessment
3.2.1. Visible Plaque Index
3.2.2. Probing Pocket Depth at First Molar Site
3.2.3. Probing Pocket Depth at Second Molar Site
3.2.4. Clinical Attachment Loss at Second Molar Site
4. Discussion
- -
- DEC and DETP flap, in terms of PPD of first molar site (buccal);
- -
- MARG flap, in terms of PPD of second molar sites (buccal and distal).
- -
- TRAP flap, in terms of PPD of first molar site (buccal);
- -
- DEC flap, in terms of PPD of second molar sites (buccal and distal);
- -
- MARG flap, in terms of CAL of second molar sites (buccal and buccal-distal).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viscuso, M.; Di Crecchio, A.; Pacino, G.A.; Trevisol, L.; Valsecchi, S.; Buttura Da Prato, E.; D’Agostino, A. Disodontiasi del terzo molare. Quad. Med. Chir. 2001, 17, 241–243. [Google Scholar]
- Nocini, P.F.; Consolo, U.; Lo Muzio, L.; De Santis, D.; Salgarelli, A. I lembi in chirurgia orale. Metodiche operative. Quad. Med. Chir. 1991, 7 (Suppl. N. 2), 245–250. [Google Scholar]
- Chen, Y.W.; Lee, C.T.; Hum, L.; Chuang, S.K. Effect of flap design on periodontal healing after impacted third molar extraction: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 363–372. [Google Scholar] [CrossRef]
- Baqain, Z.H.; Al-Shafii, A.; Hamdan, A.A.; Sawair, F.A. Flap design and mandibular third molar surgery: A split mouth randomized clinical study. Int. J. Oral Maxillofac. Surg. 2012, 41, 1020–1024. [Google Scholar] [CrossRef] [PubMed]
- Motamedi, M.H. Preventing periodontal pocket formation after removal of an impacted mandibular third molar. J. Am. Dent. Assoc. 1999, 130, 1482–1484. [Google Scholar] [CrossRef] [PubMed]
- Rosa, A.L.; Carneiro, M.G.; Lavrador, M.A.; Novaes, A.B. Influence of flap design on periodontal healing of second molars after extraction of impacted mandibular third molars. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 404–407. [Google Scholar] [CrossRef]
- Peng, K.Y.; Tseng, Y.C.; Shen, E.C.; Chiu, S.C.; Fu, E.; Huang, Y.W. Mandibular second molar periodontal status after third molar extraction. J. Periodontol. 2001, 72, 1647–1651. [Google Scholar] [CrossRef]
- Chang, H.H.; Lee, J.J.; Kok, S.H.; Yang, P.J. Periodontal healing after mandibular third molar surgery-A comparison of distolingual alveolectomy and tooth division techniques. Int. J. Oral Maxillofac. Surg. 2004, 33, 32–37. [Google Scholar] [CrossRef] [Green Version]
- van Gool, A.V.; Ten Bosch, J.J.; Boering, G. Clinical consequences of complaints and complications after removal of the mandibular third molar. Int. J. Oral Surg. 1977, 6, 29–37. [Google Scholar] [CrossRef]
- Albanese, M.; Da Prato, E.B.; Trevisol, L.; Saia, G.; Viscuso, M.; Di Crecchio, A. Tecnica chirurgica nell’avulsione del terzo molare inferiore. Quad. Med. Chir. 2001, 17, 207–210. [Google Scholar]
- Korkmaz, Y.T.; Mollaoglu, N.; Ozmeriç, N. Does laterally rotated flap design influence the short-term periodontal status of second molars and postoperative discomfort after partially impacted third molar surgery? J. Oral Maxillofac. Surg. 2015, 73, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Schofield, I.D.; Kogon, S.L.; Donner, A. Long-term comparison of two surgical flap designs for third molar surgery on the health of the periodontal tissue of the second molar tooth. J. Can. Dent. Assoc. 1988, 54, 689–691. [Google Scholar] [PubMed]
- Kautto, A.; Vehkalahti, M.M.; Venta, I. Age of patient at the extraction of the third molar. Int. Oral Maxillofac. Surg. 2018, 47, 947–951. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Garcia, A.G.; Sampedro, F.G.; Rey, J.G.; Vila, P.G.; Martin, M.S. Pell-Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molars. Br. J. Oral Maxillofac. Surg. 2000, 38, 585–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matzen, L.H.; Schropp, L.; Spin-Neto, R.; Wenzel, A. Radiographic signs of pathology determining removal of an impacted mandibular third molar assessed in a panoramic image or CBCT. Dentomaxillofacial. Radiol. 2017, 46, 20160330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiapasco, M.; Zaniboni, M. Manuale Illustrato di Chirurgia Orale, 4th ed.; Edra: Milano, Italy, 2020; p. 640. [Google Scholar]
- Borgonovo, A.E.; Giussani, A.; Grossi, G.B.; Maiorana, C. Evaluation of postoperative discomfort after impacted mandibular third molar surgery using three different types of flap. Quintessence Int. 2014, 45, 319–330. [Google Scholar]
- Lindhe, J.; Karring, T.; Lang, N.P. Clinical Periodontology and Implant Dentistry, 6th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2015; 1480p. [Google Scholar]
- Lombardo, G.; Signoriello, A.; Corrocher, G.; Signoretto, C.; Burlacchini, G.; Pardo, A.; Nocini, P.F. A topical desiccant agent in association with manual debridement in the initial treatment of peri-implant mucositis: A clinical and microbiological pilot study. Antibiotics 2019, 8, 82. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef]
- Stephens, R.J.; App, G.R.; Foreman, D.W. Periodontal evaluation of two mucoperiosteal flaps used in removing impacted mandibular third molars. J. Oral Maxillofac. Surg. 1983, 41, 719–724. [Google Scholar] [CrossRef]
- Kirtiloğlu, T.; Bulut, E.; Sümer, M.; Cengiz, I. Comparison of 2 flap designs in the periodontal healing of second molars after fully impacted mandibular third molar extractions. J. Oral Maxillofac. Surg. 2007, 65, 2206–2210. [Google Scholar] [CrossRef] [PubMed]
- Arta, S.A.; Pourabbas Kheyradin, R.; Mesgarzadeh, A.H.; Hassanbaglu, B. Comparison of the influence of two flap designs on periodontal healing after surgical extraction of impacted third molars. J. Dent. Res. Dent. Clin. Dent. Prospects. 2011, 5, 1–4. [Google Scholar] [PubMed]
- Li, Z.B.; Qu, H.L.; Zhou, L.N.; Tian, B.M.; Chen, F.M. Influence of non-impacted third molars on pathologies of adjacent second molars: A retrospective study. J. Periodontol. 2017, 88, 450–456. [Google Scholar] [CrossRef]
- Monaco, G.; Daprile, G.; Tavernese, L.; Corinaldesi, G.; Marchetti, C. Mandibular third molar removal in young patients: An evaluation of 2 different flap designs. J. Oral Maxillofac. Surg. 2009, 67, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Quee, T.A.; Gosselin, D.; Millar, E.P.; Stamm, J.W. Surgical removal of the fully impacted mandibular third molar. the influence of flap design and alveolar bone height on the periodontal status of the second molar. J. Periodontol. 1985, 56, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Tarnow, D.P.; Magner, A.W.; Fletcher, P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J. Periodontol. 1992, 63, 995–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Listgarten, M.A.; Rosenberg, M.M. Histological study of repair following new attachment procedures in human periodontal lesions. J. Periodontol. 1979, 50, 333–344. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Sex | ||
| male | 31 | 38.75 |
| female | 49 | 61.25 |
| Age 1 | 22 ± 4.22 | years |
| Tooth element | ||
| element 38 | 46 | 57.5 |
| element 48 | 34 | 42.5 |
| Tooth class (Pell and Gregory classification) | ||
| IA | 15 | 18.75 |
| IIA | 10 | 12.5 |
| IB | 18 | 22.5 |
| IIB | 19 | 23.75 |
| IIIB | 5 | 6.25 |
| IC | 1 | 1.25 |
| IIC | 6 | 7.5 |
| IIIC | 6 | 7.5 |
| Overall periodontal conditions | ||
| gingival health | 67 | 83.75 |
| moderate gingivitis | 10 | 12.5 |
| severe gingivitis | 3 | 3.75 |
| OVERALL PERIODONTAL DIAGNOSIS (Healthy, Moderate Gingivitis, Severe Gingivitis) | FIRST MOLAR BUCCAL SITE PPD ∆ (T0–T3) | SECOND MOLAR BUCCAL SITE PPD ∆ (T0–T3) | SECOND MOLAR DISTAL SITE PPD ∆ (T0–T3) | SECOND MOLAR DISTAL SITE PLAQUE INDEX ∆ (T0–T3) | SECOND MOLAR BUCCAL SITE CAL ∆ (T0–T3) | SECOND MOLAR BUCCAL-DISTAL SITE CAL ∆ (T0–T3) | ||
|---|---|---|---|---|---|---|---|---|
| p value | p value | p value | p value | p value | p value | |||
| OVERALL | 0.74 | 0.001 * | 0.001 * | 0.34 | 0.53 | 0.42 | ||
| TECHNIQUE | ||||||||
| DEC | 0.88 | 0.01 * | 0.001 * | 0.03 * | 0.51 | 0.29 | ||
| DETP | 0.61 | 0.25 | 0.13 | 0.54 | 0.94 | 0.48 | ||
| MARG | 0.08 | 0.02 * | 0.04 * | 0.01 * | 0.13 | 0.85 | ||
| TRAP | 0.28 | 0.22 | 0.20 | 0.86 | 0.17 | 0.19 |
| DEGREE OF INCLUSION (IA, IIA, IB, IIB, IIIB, IC, IIC, IIIC) | FIRST MOLAR BUCCAL SITE PPD ∆ (T0–T3) | SECOND MOLAR BUCCAL SITE PPD ∆ (T0–T3) | SECOND MOLAR DISTAL SITE PPD ∆ (T0–T3) | SECOND MOLAR DISTAL SITE PLAQUE INDEX ∆ (T0–T3) | SECOND MOLAR BUCCAL SITE CAL ∆ (T0–T3) | SECOND MOLAR BUCCAL-DISTAL SITE CAL ∆ (T0–T3) | ||
|---|---|---|---|---|---|---|---|---|
| p value | p value | p value | p value | p value | p value | |||
| OVERALL | 0.75 | 0.46 | 0.26 | 0.88 | 0.52 | 0.54 | ||
| TECHNIQUE | ||||||||
| DEC | 0.42 | 0.52 | 0.25 | 0.68 | 0.65 | 0.44 | ||
| DISPAP | 0.49 | 0.80 | 0.40 | 0.05 | 0.30 | 0.20 | ||
| MARG | 0.66 | 0.33 | 0.88 | 0.36 | 0.99 | 0.74 | ||
| TRAP | 0.73 | 0.26 | 0.15 | 0.36 | 0.17 | 0.59 |
| T0 | T3 | ∆ (T0–T3) | p Value | ||
|---|---|---|---|---|---|
| OVERALL | 0.13 (0.34) | 0.14 (0.35) | 0.01 (0.43) | 0.79 | |
| TECHNIQUE | |||||
| DEC | 0.06 (0.25) | 0.18 (0.40) | 0.12 (0.50) | 0.31 | |
| DETP | 0.15 (0.36) | 0.25 (0.44) | 0.10 (0.30) | 0.15 | |
| MARG | 0.11 (0.32) | 0.11 (0.32) | 0.01 (0.39) | 0.99 | |
| TRAP | 0.22 (0.42) | 0.05 (0.23) | 0.16 (0.51) | 0.17 | |
| p value | 0.56 | 0.34 | 0.17 |
| T0 | T1 | T2 | T3 | ∆ (T0–T3) | p Value | ||
|---|---|---|---|---|---|---|---|
| OVERALL | 1.65 ± 0.45 | 1.98 ± 0.48 | 1.84 ± 0.44 | 1.79 ± 0.42 | 0.13 ± 0.43 | 0.002 * | |
| TECHNIQUE | |||||||
| DEC | 1.79 ± 0.44 | 2.03 ± 0.49 | 1.94 ± 0.45 | 1.83 ± 0.38 | 0.09 ± 0.37 | 0.06 | |
| DETP | 1.53 ± 0.48 | 1.94 ± 0.54 | 1.82 ± 0.38 | 1.62 ± 0.41 | 0.09 ± 0.45 | 0.59 | |
| MARG | 1.61 ± 0.37 | 1.98 ± 0.45 | 1.79 ± 0.39 | 1.77 ± 0.43 | 0.16 ± 0.44 | 0.04 * | |
| TRAP | 1.76 ± 0.52 | 1.98 ± 0.50 | 1.85 ± 0.54 | 1.96 ± 0.41 | 0.19 ± 0.46 | 0.06 | |
| p value | 0.42 | 0.82 | 0.63 | 0.07 | 0.71 |
| T0 | T1 | T2 | T3 | ∆ (T0–T3) | p Value | ||
|---|---|---|---|---|---|---|---|
| OVERALL | 2.34 ± 0.65 | 3.79 ± 1.06 | 2.94 ± 0.70 | 2.53 ± 0.62 | 0.19 ± 0.64 | 0.004 * | |
| TECHNIQUE | |||||||
| DEC | 2.18 ± 0.65 | 3.72 ± 1.27 | 3.00 ± 0.66 | 2.57 ± 0.76 | 0.38 ± 0.75 | 0.11 | |
| DETP | 1.96 ± 0.50 | 3.51 ± 0.86 | 2.72 ± 0.68 | 2.28 ± 0.66 | 0.31 ± 0.77 | 0.04 * | |
| MARG | 2.49 ± 0.62 | 3.98 ± 1.15 | 2.87 ± 0.76 | 2.56 ± 0.43 | 0.03 ± 0.53 | 0.19 | |
| TRAP | 2.67 ± 0.65 | 3.86 ± 0.94 | 3.22 ± 0.62 | 2.74 ± 0.66 | 0.06 ± 0.47 | 0.46 | |
| p value | 0.003 * | 0.54 | 0.12 | 0.14 | 0.80 |
| T0 | T1 | T2 | T3 | ∆ (T0–T3) | p Value | ||
|---|---|---|---|---|---|---|---|
| OVERALL | 2.89 ± 1.37 | 5.64 ± 2.49 | 4.33 ± 1.68 | 3.34 ± 1.35 | 0.45 ± 1.43 | 0.01 * | |
| TECHNIQUE | |||||||
| DEC | 2.50 ± 1.41 | 5.75 ± 3.31 | 4.68 ± 2.18 | 3.37 ± 1.62 | 0.87 ± 1.74 | 0.16 | |
| DETP | 2.35 ± 0.74 | 4.92 ± 1.47 | 3.75 ± 1.40 | 2.95 ± 1.43 | 0.60 ± 1.50 | 0.19 | |
| MARG | 3.31 ± 1.46 | 6.03 ± 2.27 | 4.29 ± 1.43 | 3.37 ± 1.11 | 0.05 ± 1.31 | 0.55 | |
| TRAP | 3.22 ± 1.51 | 5.77 ± 2.88 | 4.72 ± 1.74 | 3.72 ± 1.31 | 0.50 ± 1.20 | 0.08 | |
| p value | 0.06 | 0.56 | 0.23 | 0.19 | 0.68 |
| T0 | T3 | ∆ (T0–T3) | p Value | ||
|---|---|---|---|---|---|
| OVERALL | 2.70 ± 1.09 | 3.33 ± 0.99 | 0.63 ± 0.87 | 0.0001 * | |
| TECHNIQUE | |||||
| DEC | 2.71 ± 1.09 | 3.43 ± 0.83 | 0.71 ± 0.94 | 0.005 * | |
| DETP | 2.77 ± 1.04 | 3.15 ± 0.89 | 0.37 ± 0.66 | 0.01 * | |
| MARG | 2.42 ± 1.08 | 3.16 ± 1.22 | 0.74 ± 0.92 | 0.001 * | |
| TRAP | 3.02 ± 1.14 | 3.72 ± 0.75 | 0.69 ± 0.95 | 0.01 * | |
| p value | 0.37 | 0.17 | 0.39 |
| T0 | T3 | ∆ (T0–T3) | p Value | ||
|---|---|---|---|---|---|
| OVERALL | 3.91 ± 1.20 | 4.76 ± 1.85 | 0.84 ± 1.61 | 0.0001 * | |
| TECHNIQUE | |||||
| DEC | 3.93 ± 1.28 | 4.56 ± 2.27 | 0.62 ± 1.92 | 0.22 | |
| DETP | 3.75 ± 1.33 | 4.57 ± 1.53 | 0.82 ± 1.33 | 0.01 * | |
| MARG | 3.90 ± 1.20 | 5.05 ± 2.10 | 1.14 ± 1.90 | 0.001 * | |
| TRAP | 4.11 ± 1.02 | 4.72 ± 1.40 | 0.61 ± 1.09 | 0.04 * | |
| p value | 0.80 | 0.68 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castagna, V.; Pardo, A.; Lanaro, L.; Signoriello, A.; Albanese, M. Periodontal Healing after Lower Third Molars Extraction: A Clinical Evaluation of Different Flap Designs. Healthcare 2022, 10, 1587. https://doi.org/10.3390/healthcare10081587
Castagna V, Pardo A, Lanaro L, Signoriello A, Albanese M. Periodontal Healing after Lower Third Molars Extraction: A Clinical Evaluation of Different Flap Designs. Healthcare. 2022; 10(8):1587. https://doi.org/10.3390/healthcare10081587
Chicago/Turabian StyleCastagna, Valentina, Alessia Pardo, Luca Lanaro, Annarita Signoriello, and Massimo Albanese. 2022. "Periodontal Healing after Lower Third Molars Extraction: A Clinical Evaluation of Different Flap Designs" Healthcare 10, no. 8: 1587. https://doi.org/10.3390/healthcare10081587