
Promoting Laparoscopic Anterior Approach for a Very Low Presacral Primary Neuroendocrine Tumor Arising in a Tailgut Cyst

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
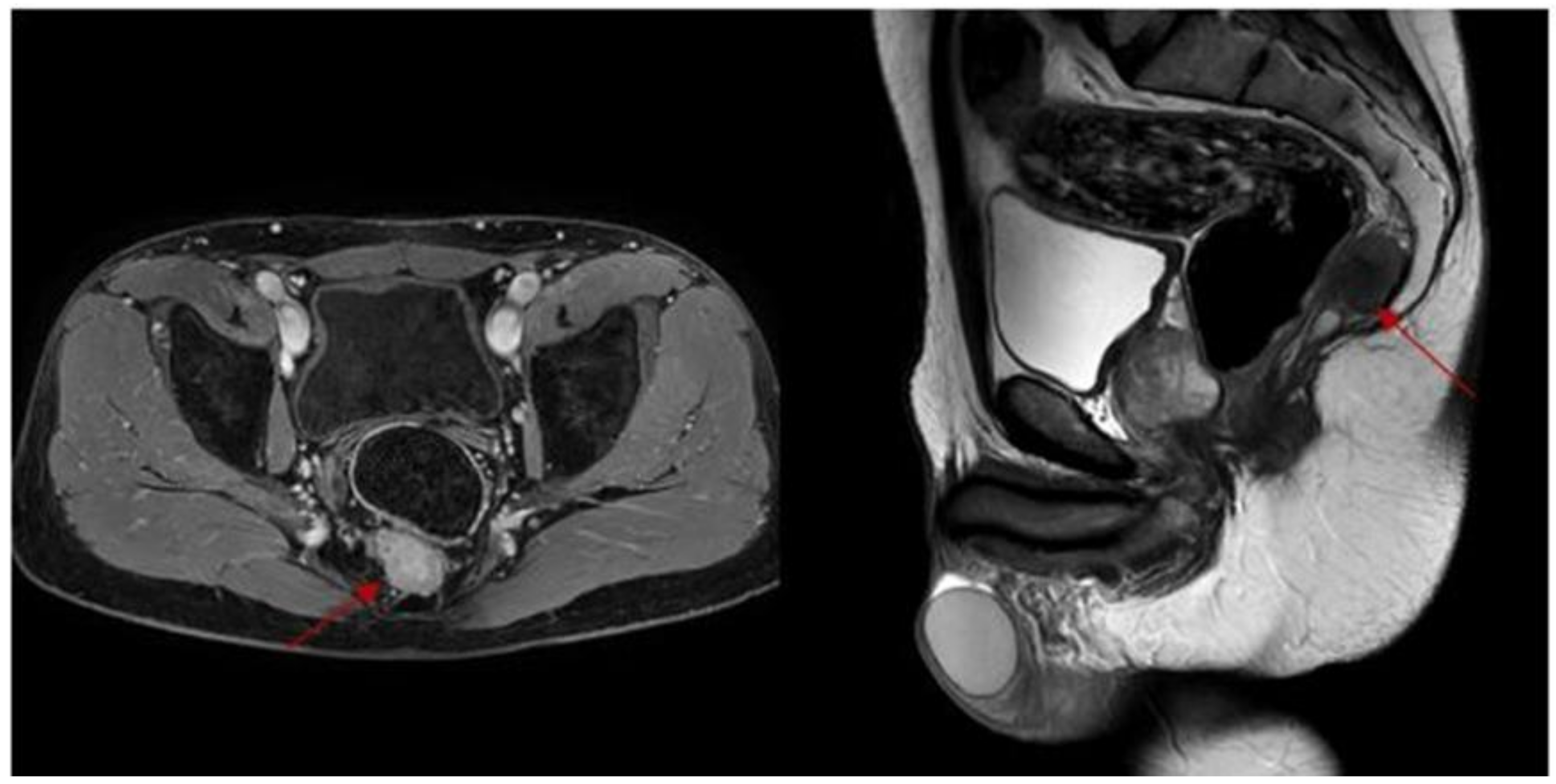
2. Case Report
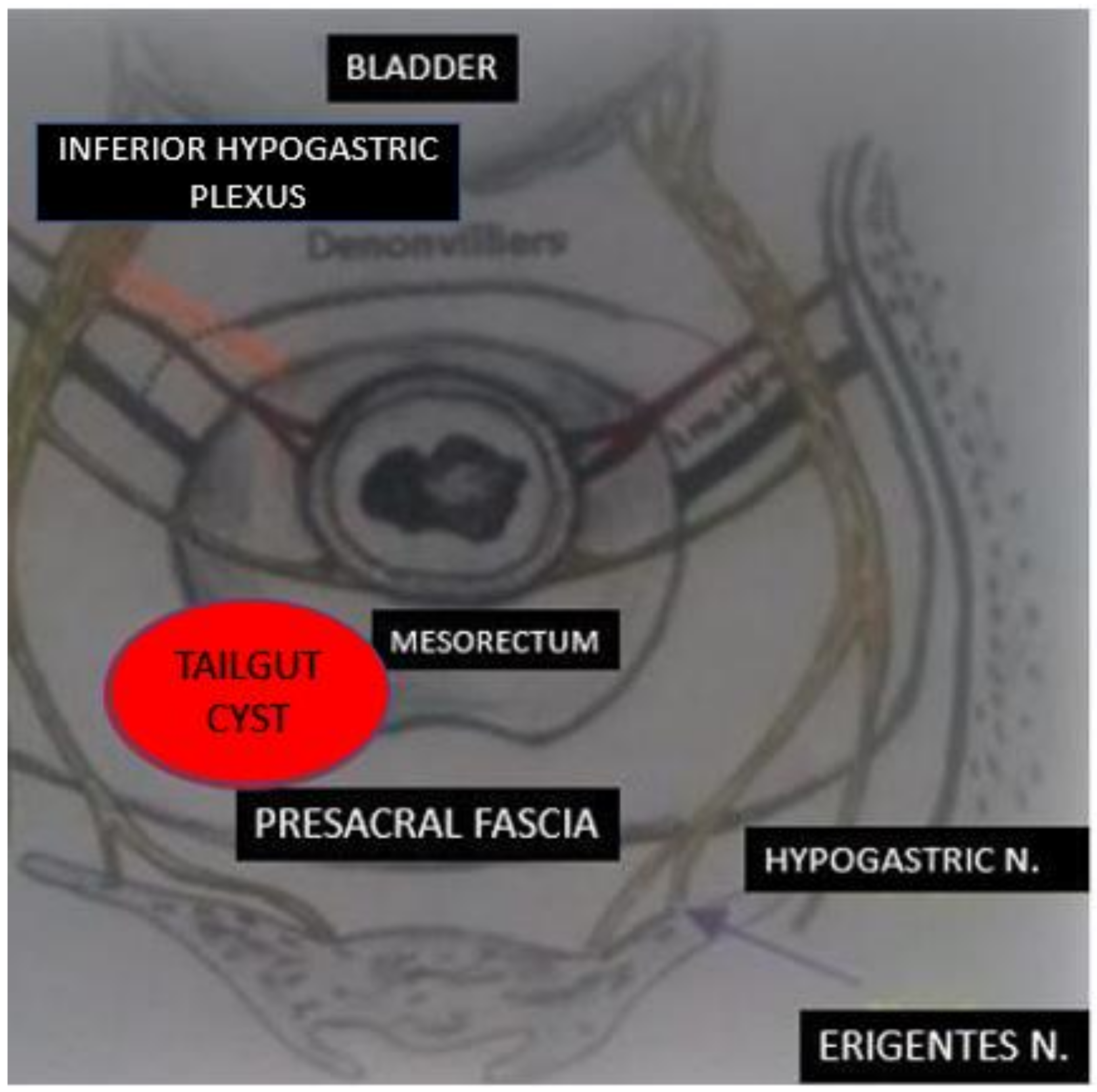
2.1. Surgical Technique
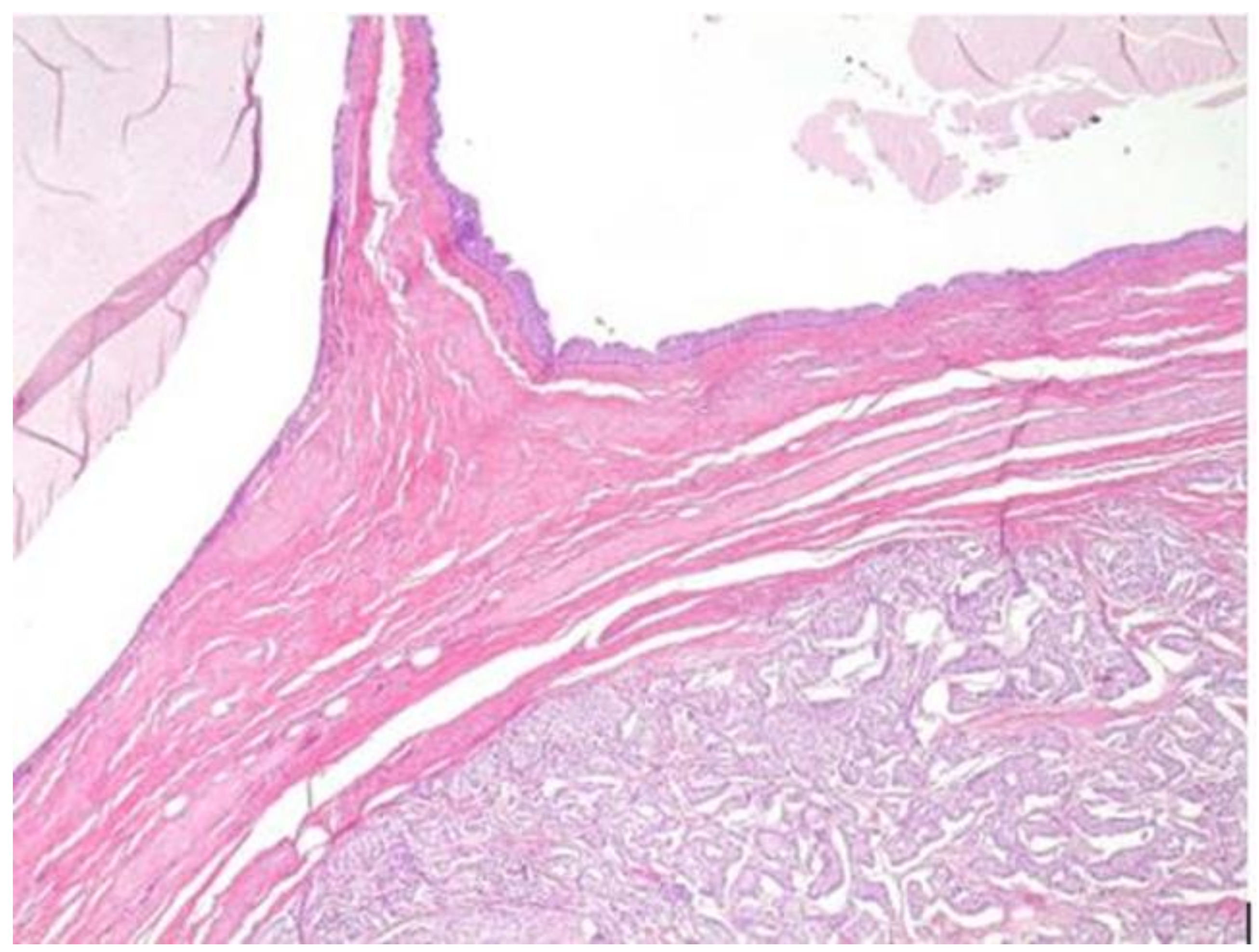
2.2. Pathology
3. Discussion
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Mathis, K.L.; Dozois, E.J.; Grewal, M.S.; Metzger, P.; Larson, D.W.; Devine, R.M. Malignant risk and surgical outcomes of presacral tailgut cysts. Br. J. Surg. 2010, 97, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Dahan, H.; Arrive, L.; Wendum, D.; Docou le Pointe, H.; Djouhri, H.; Tubiana, J.M. Retrorectal developmental cysts in adults: Clinical and radiologic–histopathologic review, differential diagnosis, and treatment. Radiographics 2001, 21, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Broccard, S.P.; Colibaseanu, D.T.; Behm, K.T.; Mishra, N.; Davis, P.; Maimone, K.L.; Merchea, A. Risk of malignancy and outcomes of surgically resected presacral tailgut cysts: A current review of the Mayo Clinic experience. Colorectal. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE guidelines: Consensus-based clinical case report guideline development. J. Clin. Epidemiol. 2014, 67, 46–51. [Google Scholar] [CrossRef]
- Peltrini, R.; Imperatore, N.; Carannante, F.; Cuccurullo, D.; Capolupo, G.T.; Bracale, U.; Caricato, M.; Corcione, F. Age and comorbidities do not affect short-term outcomes after laparoscopic rectal cancer resection in elderly patients. A multi-institutional cohort study in 287 patients. Updates Surg. 2021, 73, 527–537. [Google Scholar] [CrossRef]
- Luglio, G.; Tarquini, R.; Giglio, M.C.; Sollazzo, V.; Peltrini, R.; Sacco, M.; Spiezio, G.; Amato, B.; De Palma, G.D.; Bucci., L. Ventral mesh rectopexy versus conventional suture technique: A single-institutional experience. Aging Clin. Exp. Res. 2017, 29, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Peltrini, R.; Luca, M.; Lionetti, R.; Bracale, U.; Corcione, F. Open veress assisted technique for laparoscopic entry. J. Minim. Access Surg. 2022. [Google Scholar] [CrossRef]
- Mastoraki, A.; Giannakodimos, I.; Panagiotou, K.; Frountzas, M.; Chrysikos, D.; Kykalos, S.; Theodoropoulos, G.E.; Schizas, D. Epidemiology, diagnostic approach and therapeutic management of tailgut cysts: A systematic review. Int. J. Clin. Pract. 2021, 75, e14546. [Google Scholar] [CrossRef]
- Yang, D.M.; Park, C.H.; Jin, W.; Chang, S.K.; Kim, J.E.; Choi, S.J.; Jung, D.H. Tailgut cyst: MRI evaluation. AJR Am. J. Roentgenol. 2005, 184, 1519–1523. [Google Scholar] [CrossRef]
- Chéreau, N.; Lefevre, J.H.; Meurette, G.; Mourra, N.; Shields, C.; Parc, Y.; Tiret, E. Surgical resection of retrorectal tumours in adults: Long-term results in 47 patients. Colorectal. Dis. 2013, 15, e476-82. [Google Scholar] [CrossRef]
- Peltrini, R.; Cantoni, V.; Green, R.; Lionetti, R.; D’Ambra, M.; Bartolini, C.; Corcione, F. Risk of appendiceal neoplasm after interval appendectomy for complicated appendicitis: A systematic review and meta-analysis. Surgeon 2021, 19, e549–e558. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Suhardja, T.S.; Nguyen, T.C.; Teoh, W.M. Neuroendocrine tumour developing within a long-standing tailgut cyst: Case report and review of the literature. Clin. J. Gastroenterol. 2019, 12, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Kodera, K.; Eto, S.; Fukasawa, N.; Kai, W.; Matsumoto, T.; Hirabayashi, T.; Kawahara, H.; Omura, N. Laparoscopic resection of a neuroendocrine tumor that almost fully replaced tailgut cysts: A case report. Surg. Case Rep. 2020, 6, 269. [Google Scholar] [CrossRef] [PubMed]
- Cody, H.S., III; Marcove, R.C.; Quan, S.H. Malignant retrorectal tumors: 28 years’ experience at Memorial Sloan-Kettering Cancer Center. Dis. Colon. Rectum. 1981, 24, 501–506. [Google Scholar] [CrossRef]
- Sica, A.; Casale, B.; Spada, A.; Di Dato, M.T.; Sagnelli, C.; Calogero, A.; Buonavolontà, P.; Salzano, A.; Martinelli, E.; Saracco, E.; et al. Differential Diagnosis: Retroperitoneal Fibrosis and Oncological Diseases. Open Med. 2019, 5, 22–26. [Google Scholar] [CrossRef] [Green Version]
- La Rosa, S.; Boni, L.; Finzi, G.; Vigetti, D.; Papanikolaou, N.; Tenconi, S.M.; Dionigi, G.; Clerici, M.; Garancini, S.; Capella, C. Ghrelin-producing well-differentiated neuroendocrine tumor (carcinoid) of tailgut cyst. Morphological, immunohistochemical, ultrastructural, and RT-PCR study of a case and review of the literature. Endocr. Pathol. 2010, 21, 190–198. [Google Scholar] [CrossRef]
- Sakr, A.; Kim, H.S.; Han, Y.D.; Cho, M.S.; Hur, H.; Min, B.S.; Kim, N.K. Single-center Experience of 24 Cases of Tailgut Cyst. Ann. Coloproctol. 2019, 35, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, L.A.; Van Oppen, D.J. Laparoscopic removal of a benign pelvic retroperitoneal dermoid cyst. J. Am. Assoc. Gynecol. Laparosc. 1995, 2, 223–226. [Google Scholar] [CrossRef]
- Aubert, M.; Mege, D.; Parc, Y.; Rullier, E.; Cotte, E.; Meurette, G.; Zerbib, P.; Trilling, B.; French Research Group of Rectal Cancer Surgery. Management of Retrorectal Tumors: A French Multicentric Experience of 270 Consecutives Cases. Ann. Surg. 2021, 274, 766–772. [Google Scholar] [CrossRef]
- Hassan, I.; Wietfeldt, E.D. Presacral tumors: Diagnosis and management. Clin. Colon. Rectal. Surg. 2009, 22, 84–93. [Google Scholar] [CrossRef] [Green Version]
- Bracale, U.; Pignata, G.; Lirici, M.M.; Hüscher, C.G.; Pugliese, R.; Sgroi, G.; Romano, G.; Spinoglio, G.; Gualtierotti, M.; Maglione, V.; et al. Laparoscopic gastrectomies for cancer: The ACOI-IHTSC national guidelines. Minim. Invasive Ther. Allied. Technol. 2012, 21, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Bracale, U.; Pacelli, F.; Milone, M.; Sodo, M.; Merola, G.; Troiani, T.; Di Salvo, E. Laparoscopic treatment of abdominal unicentric castleman’s disease: A case report and literature review. BMC Surg. 2017, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Bracale, U.; Corcione, F.; Pignata, G.; Andreuccetti, J.; Dolce, P.; Boni, L.; Cassinotti, E.; Olmi, S.; Uccelli, M.; Gualtierotti, M.; et al. Impact of neoadjuvant therapy followed by laparoscopic radical gastrectomy with D2 lymph node dissection in Western population: A multi-institutional propensity score-matched study. J. Surg. Oncol. 2021, 124, 1338–1346. [Google Scholar] [CrossRef] [PubMed]
- Mullaney, T.G.; Lightner, A.L.; Johnston, M.; Kelley, S.R.; Larson, D.W.; Dozois, E.J. A systematic review of minimally invasive surgery for retrorectal tumors. Tech. Coloproctol. 2018, 22, 255–263. [Google Scholar] [CrossRef]
- EuroSurg Collaborative. Safety of hospital discharge before return of bowel function after elective colorectal surgery. Br. J. Surg. 2020, 107, 552–559. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Nuzzo, M.M.; De Werra, C.; Pace, M.; Franca, R.A.; D’Armiento, M.; Bracale, U.; Lionetti, R.; D’Ambra, M.; Calogero, A. Promoting Laparoscopic Anterior Approach for a Very Low Presacral Primary Neuroendocrine Tumor Arising in a Tailgut Cyst. Healthcare 2022, 10, 805. https://doi.org/10.3390/healthcare10050805
Di Nuzzo MM, De Werra C, Pace M, Franca RA, D’Armiento M, Bracale U, Lionetti R, D’Ambra M, Calogero A. Promoting Laparoscopic Anterior Approach for a Very Low Presacral Primary Neuroendocrine Tumor Arising in a Tailgut Cyst. Healthcare. 2022; 10(5):805. https://doi.org/10.3390/healthcare10050805
Chicago/Turabian StyleDi Nuzzo, Maria Michela, Carlo De Werra, Mirella Pace, Raduan Ahmed Franca, Maria D’Armiento, Umberto Bracale, Ruggero Lionetti, Michele D’Ambra, and Armando Calogero. 2022. "Promoting Laparoscopic Anterior Approach for a Very Low Presacral Primary Neuroendocrine Tumor Arising in a Tailgut Cyst" Healthcare 10, no. 5: 805. https://doi.org/10.3390/healthcare10050805