
Cranioplasty after Two Giant Intraosseous Angiolipomas of the Cranium: Case Report and Literature Review

 , ,
, ,
Abstract
:1. Introduction
2. Literature Review about Intraosseous Angiolipomas (IOALs)
3. Case Presentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moldovan, H.; Popescu, D.; Buliga, T.; Filip, A.; Antoniac, I.; Gheorghiţă, D.; Molnar, A. Gastric Adenocarcinoma Associated with Acute Endocarditis of the Aortic Valve and Coronary Artery Disease in a 61-Year-Old Male with Multiple Comorbidities—Combined Surgical Management—Case Report. Medicina 2019, 55, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumitrescu, D.; Savlovschi, C.; Borcan, R.; Pantu, H.; Serban, D.; Gradinaru, S.; Smarandache, G.; Trotea, T.; Branescu, C.; Musat, L.; et al. Caz Clinic—Hernie Diafragmatica Voluminoasa—Abdomen Acut Chirurgical: Dificultati Diagnostice Si Terapeutice. Chirurgia 2011, 106, 657–660. [Google Scholar] [PubMed]
- Lee, C.H.; Son, D.W.; Lee, S.H.; Lee, J.S.; Lee, S.W.; Song, G.S. Spinal Epidural Angiolipoma: A Case Report on Sudden Hemorrhagic Onset and Review of the Literature. J. Korean Soc. Geriatr. Neurosurg. 2021, 17, 20–24. [Google Scholar] [CrossRef]
- Fernando, H.; Mohammad, S.; Baarini, O.; Haddad, A. Angiolipoma of the First Intermetatarsal Space—A Case Study. Foot Ankle Surg. Tech. Rep. Cases 2022, 2, 100177. [Google Scholar] [CrossRef]
- Polte, H.W.; Kolodny, C.; Hooker, P. Intraosseous Angiolipoma of the Mandible. Oral Surg. Oral Med. Oral Pathol. 1976, 41, 7. [Google Scholar] [CrossRef]
- Nguyen, L.; Zwagerman, N.; Grandhi, R.; McFadden, K.; Richardson, R.M. Intraosseous Angiolipoma of the Cranium: Case Report and Review of the Literature. Surg. Neurol. Int. 2014, 5, 79. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.; Van Dellen, J.; Idaewor, P.; Roncaroli, F. Intraosseous Angiolipoma of the Cranium. Neurosurgery 2009, 64, E189–E190. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Josiah, D.T.; Turner, R.C.; Cantu-Durand, D.E.; Williams, H.J.; Gyure, K.; Voelker, J.L. Giant Calvarial Intraosseous Angiolipoma: A Case Report and Review of the Literature. J. Surg. Case Rep. 2016, 2016, rjw051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atilgan, A.O.; Terzi, A.; Agildere, M.; Caner, H.; Ozdemir, B.H. Intraosseous Angiolipoma of the Frontal Bone with a Unique Location: A Clinical and Pathological Case Illustration and Review of the Literature. Indian J. Pathol. Microbiol. 2014, 57, 301. [Google Scholar] [CrossRef] [PubMed]
- Amirjamshidi, A.; Ghasemi, B.; Abbasioun, K. Giant Intradiploic Angiolipoma of the Skull. Report of the First Case with MR and Histopathological Characteristics Reported in the Literature and a Review. Surg. Neurol. Int. 2014, 5, 50. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.M.; Hanft, S.; Xiong, Z. Cranial Intraosseous Angiolipoma: Case Report and Literature Review. Neurosurg. Cases Rev. 2020, 3, 1–5. [Google Scholar] [CrossRef]
- Howard, W.R.; Helwig, E.B. Angiolipoma. Arch. Dermatol. 1960, 82, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Liu, Y.; Hao, X.; Li, C.; Tian, Y. Large Intraosseous Lipoma of the Skull: A Case Report and Review of the Literature. World Neurosurg. 2018, 120, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Eyzaguirre, E.; Liqiang, W.; Karla, G.M.; Rajendra, K.; Alberto, A.; Gatalica, Z. Intraosseous Lipoma. A Clinical, Radiologic, and Pathologic Study of 5 Cases. Ann. Diagn. Pathol. 2007, 11, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Neromyliotis, E.; Sapountzi, M.; Nikas, I.; Karydakis, P.; Mitsios, A.; Sfakianos, G.; Themistocleous, M.S. Fibrous Dysplasia of Occipital and Temporal Bone. A Case Report. Oxf. Med. Case Rep. 2019, 2019, omz039. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.K.; Boyce, A.; Appelman-Dijkstra, N.; Ong, J.; Defabianis, P.; Offiah, A.; Arundel, P.; Shaw, N.; Pos, V.D.; Underhil, A.; et al. Best Practice Management Guidelines for Fibrous Dysplasia/McCune-Albright Syndrome: A Consensus Statement from the FD/MAS International Consortium. Orphanet J. Rare Dis. 2019, 14, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narang, S.; Gangopadhyay, M. Calcaneal Intraosseous Lipoma: A Case Report and Review of the Literature. J. Foot Ankle Surg. 2011, 50, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Altınel, F.; Yerli, H.; Altınörs, M. Calvarial Intraosseous Lipomas: To Surgery or Not to Surgery? Int. J. Med. Rev. Case Rep. 2020, 4, 123–128. [Google Scholar] [CrossRef]
- Jamrozik, Z.; Rosiak, G.; Kierdaszuk, B.; Milczarek, K.; Kamińska, A.; Dziewulska, D.; Krzeski, A. Intraosseous Lipoma of the Sphenoid: A Case Study. Case Rep. Neurol. Med. 2013, 2013, 519341. [Google Scholar] [CrossRef] [PubMed]
- Rivis, M.; Pricop, M.; Talpos, S.; Ciocoiu, R.; Antoniac, I.; Gheorghita, D.; Trante, O.; Moldovan, H.; Grigorescu, G.; Seceleanu, V.; et al. Influence of the Bone Cements Processing on the Mechanical Properties in Cranioplasty. Rev. Chim. 2018, 69, 990–993. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age/Sex | Location | Signs/Symptoms | Other | Radiographic Investigations | Treatment |
|---|---|---|---|---|---|---|
| Yu et al., 2009 [7] | 50/M | Right parietal bone | Asymptomatic | Swelling increasing in size; minor trauma history | CT and angiography: 7 cm focal hypodense lesion with bony spicules associated with hypervascularity and mass effect on the parietal lobe | En-bloc resection of lesion with titanium cranioplasty |
| Nguyen et al., 2014 [6] | 55/M | Right frontal bone | Headache, nausea, vomiting, and double vision | >10 pack-year history of cigarette smoking; also found to have invasive ductal breast carcinoma | CT and MRI: 4.3 cm heterogeneously mixture of trabeculated bone and fatty components with mild mass effect on the adjacent frontal lobe | En-bloc resection of lesion with titanium cranioplasty |
| Atilgan et al., 2014 [9] | 16/F | Right frontal bone | Scalp swelling and headache | No history of traumatic episodes | CT: 2 cm well-defined hypodense-lytic lesion to the right of the frontal lobe | En-bloc resection of lesion with titanium cranioplasty |
| Amirjamshidi et al., 2014 [10] | 41/F | Right frontoparietotemporal bone and part of the occipital bone | Mild headache of about 4 months duration without nausea or vomiting | Lesion grown during the previous 2 years with recently tenderness | CT and MRI: 20 cm densely intraosseous expansile lesion with calcified components and mass effect upon the adjacent dura | En-bloc resection of lesion with titanium cranioplasty |
| Singh et al., 2016 [8] | 30/F | Right parietal bone | Altered sensation over the affected area without any pain with palpation | Lesion present 5 years prior to presentation; began to enlarge after pregnancy | CT and MRI: 6.4 cm calvarial mass with expansion and mass effect on the right parietal lobe | En-bloc resection of lesion with PEEK cranioplasty |
| Morgan et al. [11], 2020 | 61/F | Left frontoparietal bone | Asymptomatic | Swelling; minor head trauma 6 months before; history of squamous cell carcinoma and basal cell carcinoma | CT and MRI: 4.4 cm expansile, spiculated, enhancing lesion with superficial soft tissue component and cerebral compression | En-bloc resection of lesion with cranioplasty |
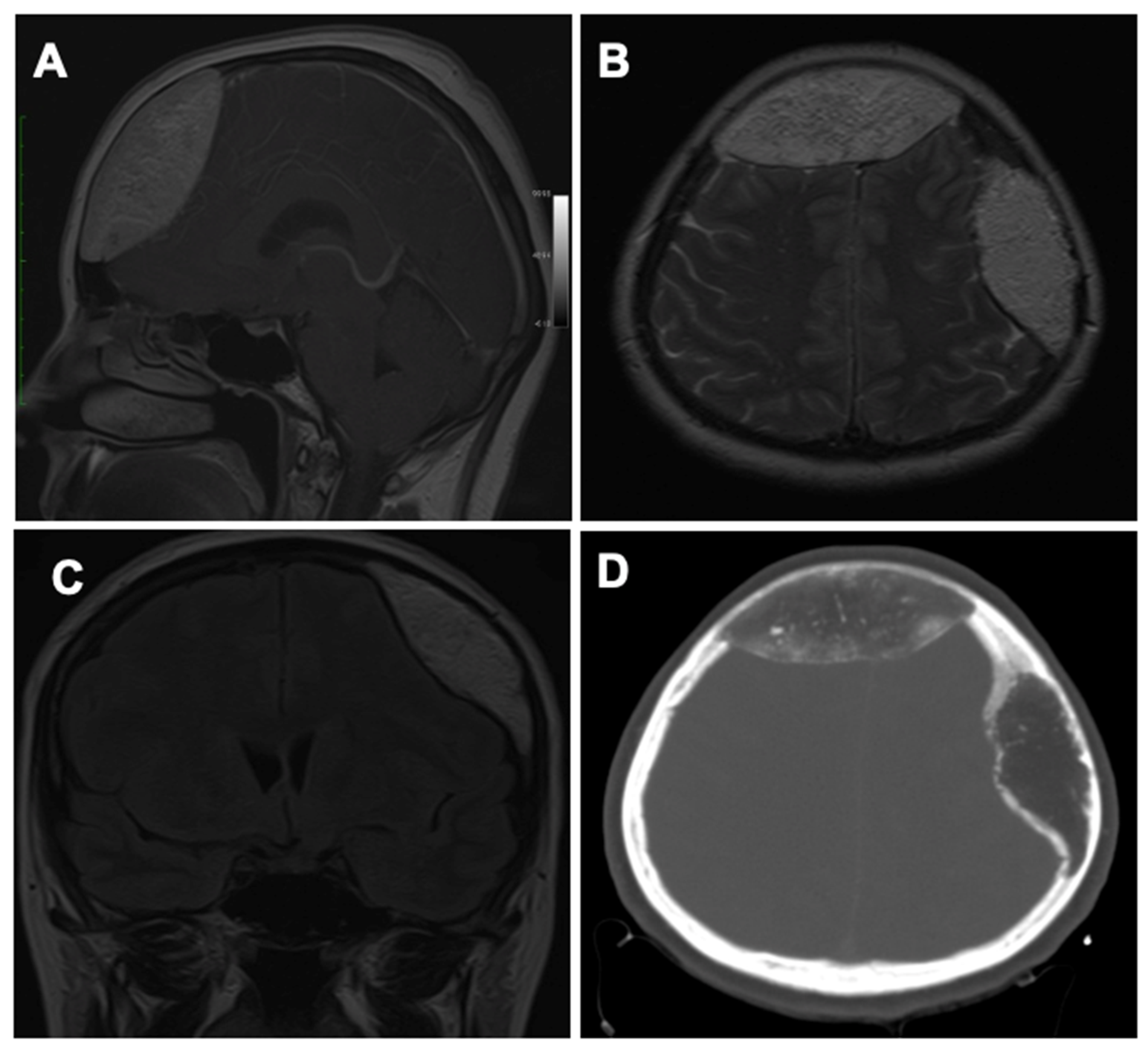
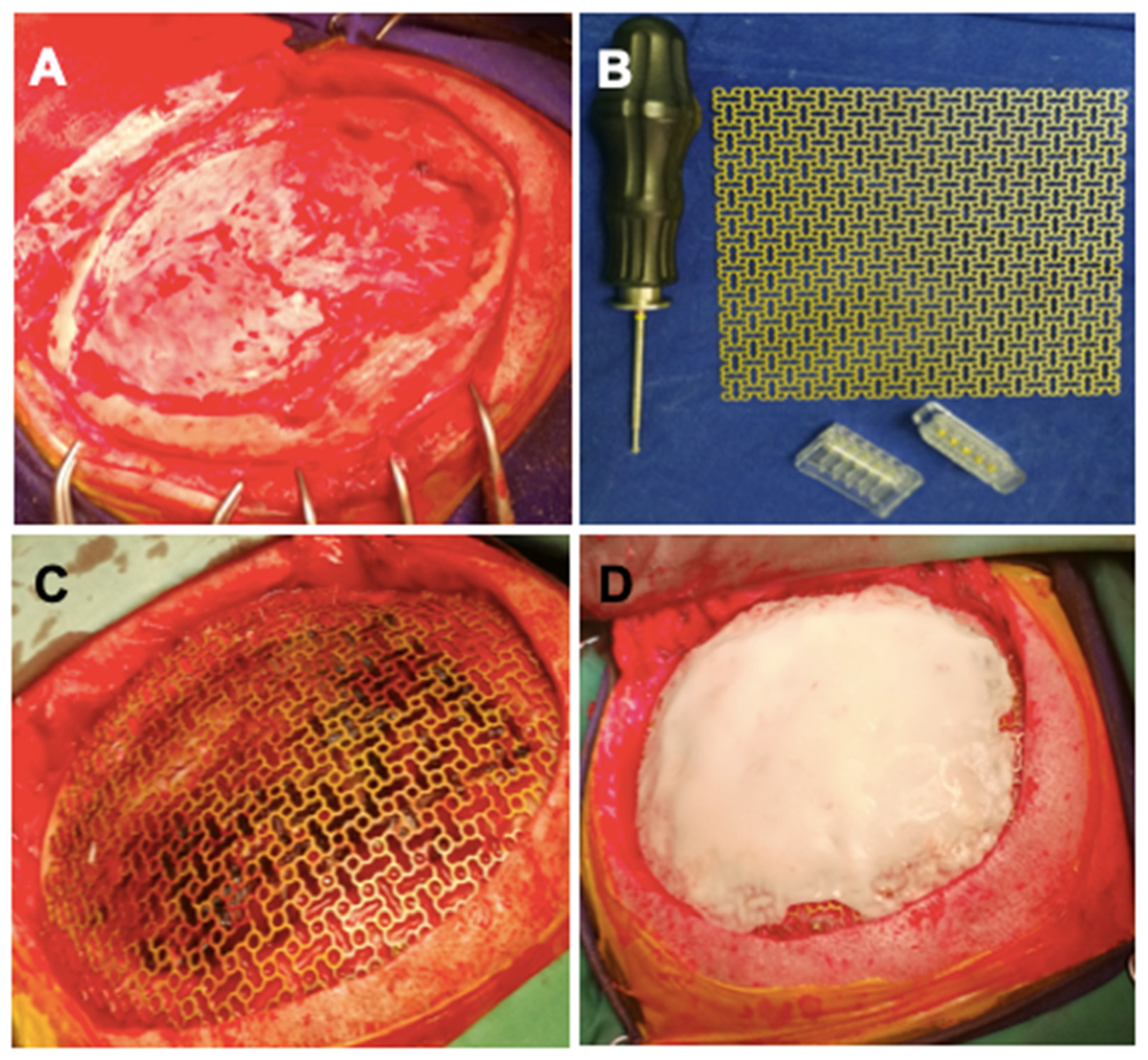
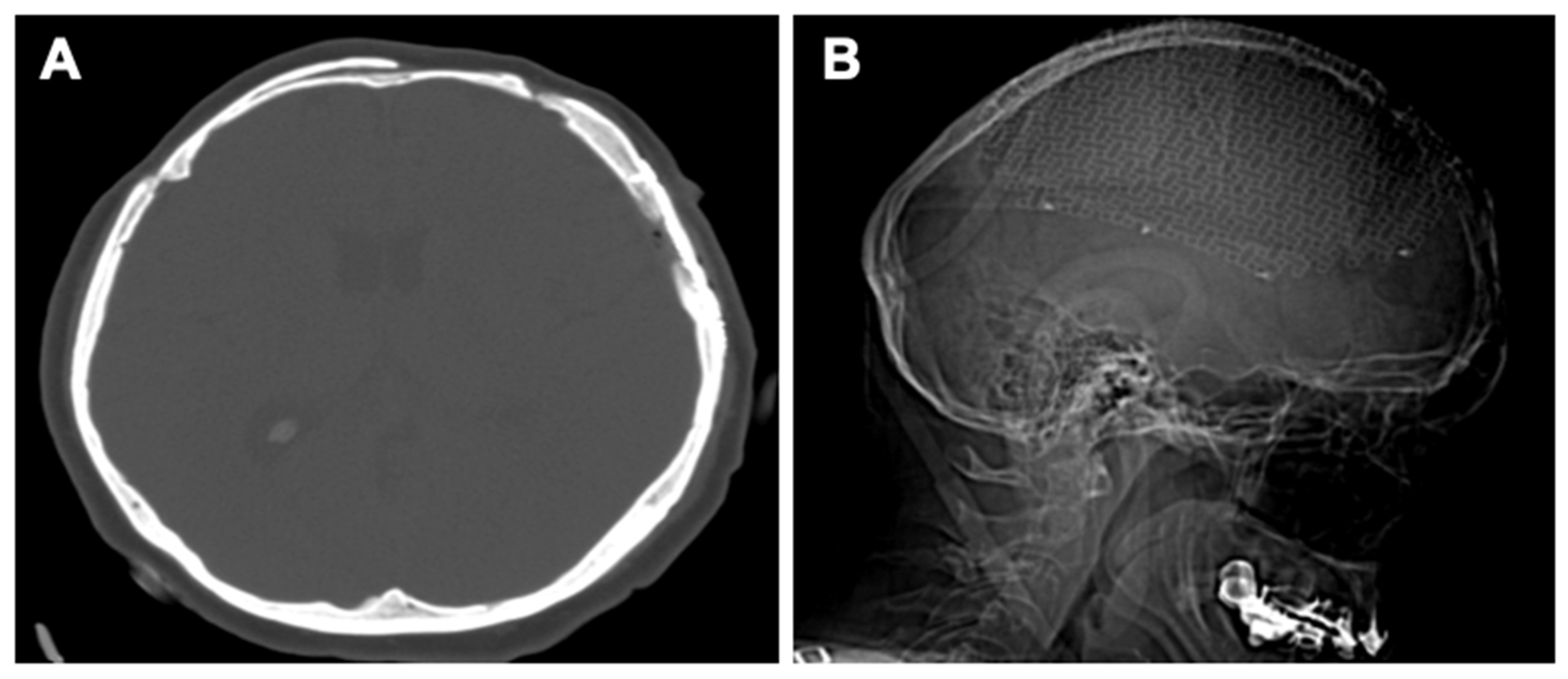
| Current study | 50/F | Frontal bone and left parietal bone | Frontal and parietal headache, nausea, and vomiting | Symptoms increasing in intensity from a month before | CT and MRI: two hypodense lesions (7 cm and 8 cm) with multiple interior calcifications and compressive effect on the cerebral parenchyma | En-bloc resection in two stages: 1. Frontal craniotomy and reconstruction with intact external plate; 2. Left parietal craniotomy with titanium and PMMA cranioplasty |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohan, A.G.; Ciurea, A.V.; Antoniac, I.; Manescu, V.; Bodog, A.; Maghiar, O.; Marcut, L.; Ghiurau, A.; Bodog, F. Cranioplasty after Two Giant Intraosseous Angiolipomas of the Cranium: Case Report and Literature Review. Healthcare 2022, 10, 655. https://doi.org/10.3390/healthcare10040655
Mohan AG, Ciurea AV, Antoniac I, Manescu V, Bodog A, Maghiar O, Marcut L, Ghiurau A, Bodog F. Cranioplasty after Two Giant Intraosseous Angiolipomas of the Cranium: Case Report and Literature Review. Healthcare. 2022; 10(4):655. https://doi.org/10.3390/healthcare10040655
Chicago/Turabian StyleMohan, Aurel George, Alexandru Vlad Ciurea, Iulian Antoniac, Veronica Manescu (Paltanea), Alin Bodog, Octavian Maghiar, Lavinia Marcut, Adrian Ghiurau, and Florian Bodog. 2022. "Cranioplasty after Two Giant Intraosseous Angiolipomas of the Cranium: Case Report and Literature Review" Healthcare 10, no. 4: 655. https://doi.org/10.3390/healthcare10040655