
How to Make Primary Healthcare More Popular: Evidence from the Middle-Aged and Elderly in China

Abstract
:1. Introduction
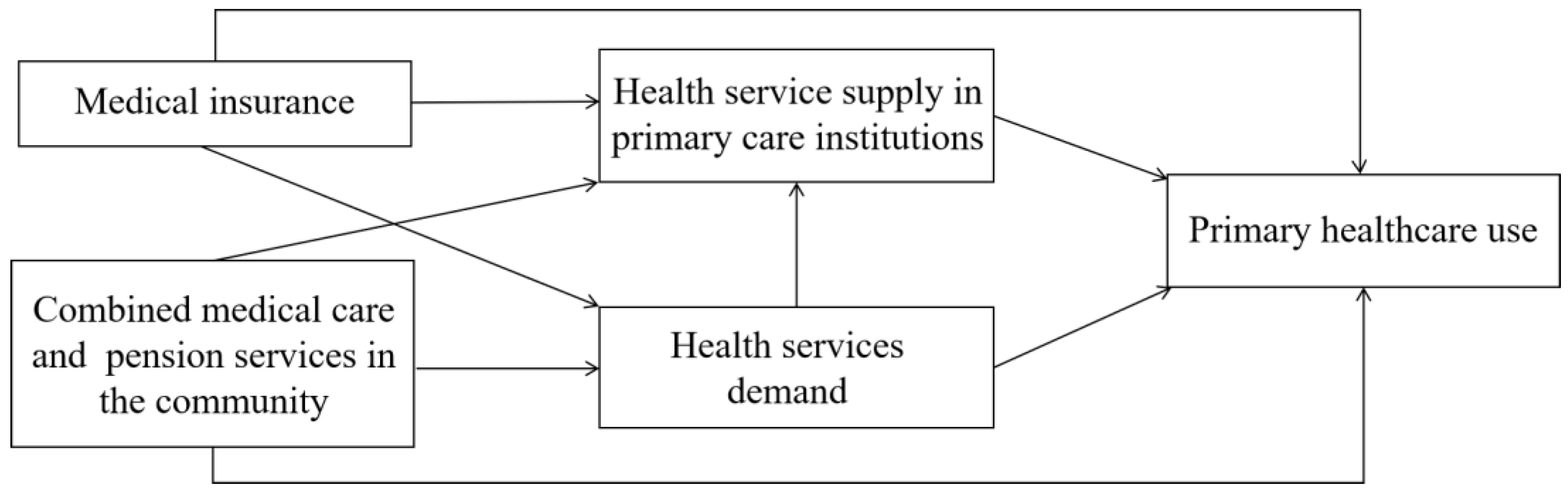
2. Research Framework
2.1. Medical Insurance
2.2. Combined Medical Care and Pension Services in the Community
2.3. Healthcare Services in Primary Care Institutions
2.4. Healthcare Service Demand
3. Materials and Methods
3.1. Data
3.2. Measures
3.3. Statistical Analysis
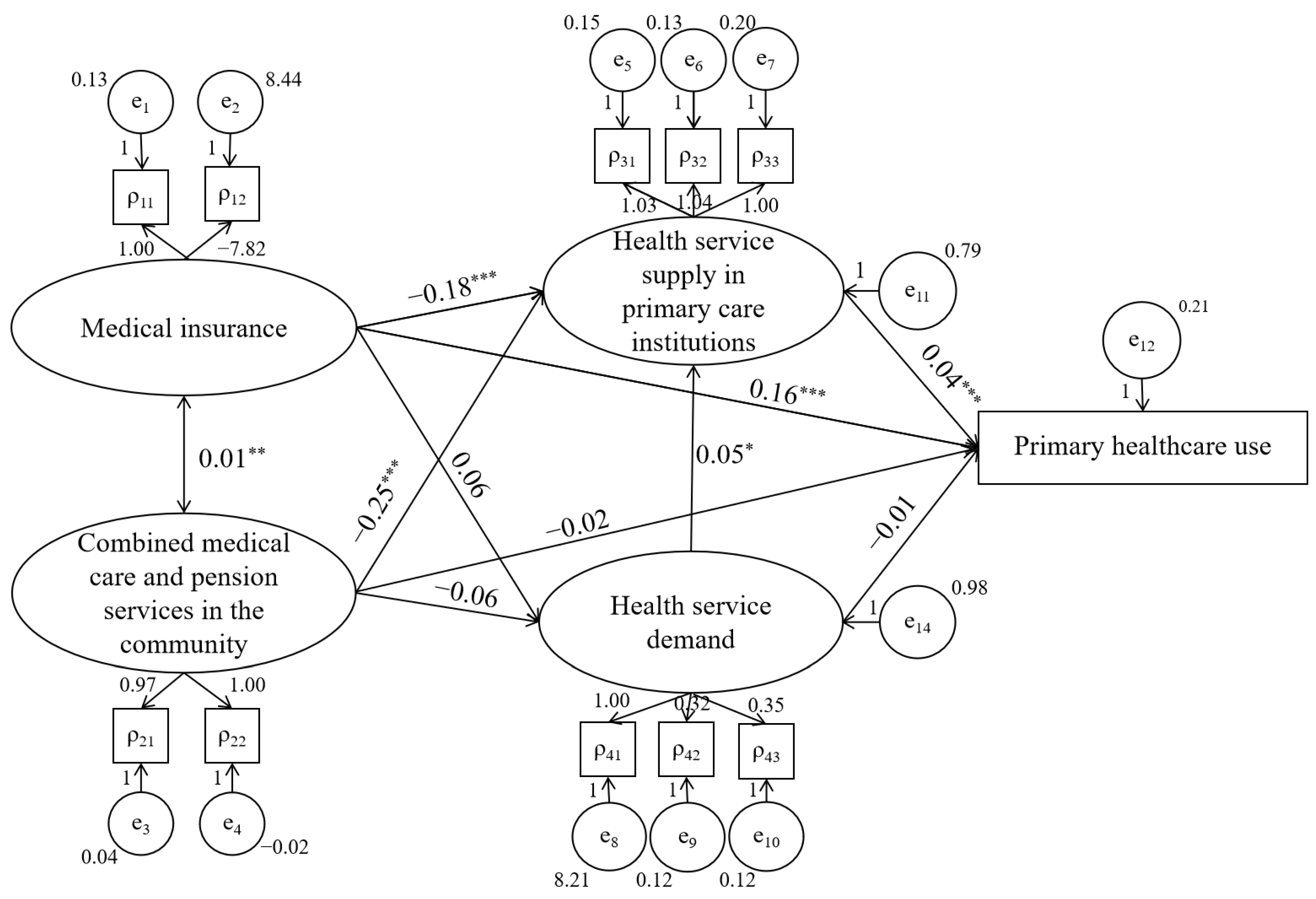
4. Results
4.1. Direct Path
4.2. Indirect Path
5. Discussion
5.1. Medical Insurance in PHC and the Use of PHC
5.2. Combined Medical Care and Pension Services and the Use of PHC
5.3. Limitations and Directions for Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. Declaration of Alma Ata. In Proceedings of the International Conference on Primary Health Care, Alma-Ata, Kazakhstan, 6–12 September 1978; Available online: http://hrlibrary.umn.edu/instree/alma-ata.html (accessed on 7 September 2022).
- Chen, Y.D. Revisiting Alma-Ata Declaration of primary health care, to build a healthy China. Chin. J. Prev. Med. 2018, 52, 457–459. (In Chinese) [Google Scholar] [CrossRef]
- Anonymous. Primary health care in China. Lancet Reg. Health West. Pac. 2020, 3, 100019. [Google Scholar] [CrossRef]
- National Health Commission. 2020 Statistical Bulletin on the Development of my country’s Health and Wellness 2020. Available online: http://www.gov.cn/guoqing/2021-07/22/content_5626526.htm (accessed on 9 September 2022).
- Jin, Y.Z.; Zhu, W.M.; Zhang, Y.G.; Meng, Q.Y. Impact of healthcare system development on healthcare seeking behavior among patients in china. Chin. Health Econ. 2021, 6, 67–70. (In Chinese) [Google Scholar]
- Lu, C.; Zhang, Z.; Lan, X. Impact of china’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef]
- Dugani, S.; Veillard, J.; Evans, T.G. Quality primary health care will drive the realization of universal health coverage. Can. Med. Assoc. J. 2018, 190, E453–E454. [Google Scholar] [CrossRef]
- Saluja, S.; Hochman, M.; Bourgoin, A.; Maxwell, J. Primary Care: The New Frontier for Reducing Readmissions. J. Gen. Intern. Med. 2019, 34, 2894–2897. [Google Scholar] [CrossRef]
- Chen, P.G.; Mehrotra, A.; Auerbach, D. Do We Really Need More Physicians? Responses to Predicted Primary Care Physician Shortages. Med. Care 2014, 52, 95–96. [Google Scholar] [CrossRef]
- Beers, K.H.; Sperati, C.J.; Weisman, D.S.; Abdel-Kader, K.; Soman, S.; Plantinga, L.; Choi, M.J.; Jaar, B.G.; Greer, R.C. Improving Primary Care Delivery for Patients Receiving Maintenance Hemodialysis. Am. J. Kidney Dis. 2021, 78, 886–891. [Google Scholar] [CrossRef]
- Ziegler, E.; Valaitis, R.; Carter, N.; Risdon, C.; Yost, J. Exploring the implementation and delivery of primary care services for transgender individuals in Ontario: Case study protocol. Prim. Health Care Res. Dev. 2020, 2, e14. [Google Scholar] [CrossRef]
- Zhang, T.; Xu, Y.; Ren, J.; Sun, L.; Liu, C. Inequality in the distribution of health resources and health services in China: Hospitals versus primary care institutions. Int. J. Equity Health 2017, 16, 42. [Google Scholar] [CrossRef]
- Mercier, G.; Georgescu, V.; Bousquet, J. Geographic variation in potentially avoidable hospitalizations in France. Health Aff. 2015, 34, 836–843. [Google Scholar] [CrossRef]
- Hong, M.; Thind, A.; Zaric, G.S.; Sarma, S. The impact of improved access to after-hours primary care on emergency department and primary care utilization: A systematic review. Health Policy 2020, 124, 812–818. [Google Scholar] [CrossRef]
- Grumbach, K.; Bodenheimer, T.; Cohen, D.; Phillips, R.L.; Stange, K.C.; Westfall, J.M. Revitalizing the U.S. Primary Care Infrastructure. N. Engl. J. Med. 2021, 385, 1156–1158. [Google Scholar] [CrossRef]
- Holderness, H.; Angier, H.; Huguet, N.; O’Malley, J.; Marino, M.; Springer, R.; DeVoe, J. Where Do Oregon Medicaid Enrollees Seek Outpatient Care Post-affordable Care Act Medicaid Expansion? Med. Care 2019, 57, 788–794. [Google Scholar] [CrossRef]
- Chen, A.; Feng, S.; Zhang, L.; Shi, L. Comparison of Patients’ Perceived Quality of Primary Care Between Urban and Rural Community Health Centers in Guangdong, China. Int. J. Environ. Res. Public Health 2020, 17, 4898. [Google Scholar] [CrossRef]
- Li, L.; Zhao, N.; Zhang, H.Y.; Yang, H.; Yang, J. Patients’ Willingness of First Visit in Primary Medical Institutions and Policy Implications: A National Cross-Sectional Survey in China. Front. Public Health 2022, 10, 842950. [Google Scholar] [CrossRef]
- Song, H.; Zuo, X.; Cui, C.; Meng, K. The willingness of patients to make the first visit to primary care institutions and its influencing factors in Beijing medical alliances: A comparative study of Beijing’s medical resource-rich and scarce regions. BMC Health Serv. Res. 2019, 19, 361. [Google Scholar] [CrossRef]
- Jiang, K.; You, D.; Li, Z.; Wei, W.; Mainstone, M. Effects of rural medical insurance on chronically ill patients’ choice of the same hospital again in rural northern china. Int. J. Environ. Res. Public Health 2018, 15, 731. [Google Scholar] [CrossRef]
- Green, C.; Hollingsworth, B.; Yang, M. The impact of social health insurance on rural populations. Eur. J. Health Econ. 2021, 22, 473–483. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhao, Y.; Shen, C.; Lai, S.; NaWaz, R.; Gao, J. Evaluating the effect of hierarchical medical system on health seeking behavior: A difference-in-differences analysis in china. Soc. Sci. Med. 2021, 268, 113372. [Google Scholar] [CrossRef]
- Gao, L.; Wang, X. Healthcare Supply Chain Network Coordination Through Medical Insurance Strategies with Reference Price Effect. Int. J. Environ. Res. Public Health 2019, 16, 3479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushima, M.; Yamada, H.; Shimamura, Y. Analysis on demand- and supply-side responses during the expansion of health insurance coverage in Vietnam: Challenges and policy implications toward universal health coverage. Rev. Dev. Econ. 2020, 24, 144–166. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, D.; Hou, Z.; Yan, F.; Hou, Z. Association between social health insurance and choice of hospitals among internal migrants in china: A national cross-sectional study. BMJ Open 2018, 8, e018440. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Wu, Z. Will overall planning of urban and rural health insurance systems have effect on health promotion and poverty alleviation: Research based on PSM-DID method. Chin. J. Health Policy 2020, 13, 7–14. (In Chinese) [Google Scholar]
- Zhou, D.; Dang, S.Q. Effect of commercial health insurance on health of residents: Empirical evidence from CGSS data. Chin. J. Health Policy 2021, 14, 8–15. (In Chinese) [Google Scholar]
- Bai, B.; Zhang, Y.; Liu, Y. Influences of Public Medical Insurance System on Labor Health Status and Supply. Iran. J. Public Health 2021, 50, 1658–1667. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Y.; Cai, H.; Zhang, J.; Pan, B.; Bao, G.; Guo, T. Analysis of the status quo of the Elderly’s demands of medical and elderly care combination in the underdeveloped regions of Western China and its influencing factors: A case study of Lanzhou. BMC Geriatr. 2020, 20, 338. [Google Scholar] [CrossRef]
- Liu, C.; Wu, Y.; Chi, X. Relationship preferences and experience of primary care patientsin continuity of care: A case study in beijing, china. BMC Health Serv. Res. 2017, 17, 585. [Google Scholar] [CrossRef]
- Ding, L.M.; Fu, L.P.; Xie, Y. Influencing factors and mechanisms of the combined operation of medical care and health care—A comparative analysis based on multiple cases. China Public Adm. 2022, 2, 83–93. (In Chinese) [Google Scholar] [CrossRef]
- Tao, Z.; Cheng, Y. Modelling the spatial accessibility of the elderly to healthcare services in beijing, china. Environ. Plan. 2019, 46, 1132–1147. [Google Scholar] [CrossRef]
- Gaskin, D.; Vazin, R.; Mccleary, R.; Thorpe, R.J. The maryland health enterprise zone initiative reduced hospital cost and utilization in underserved communities. Health Aff. 2018, 37, 1546–1554. [Google Scholar] [CrossRef]
- Ko, M.S.; Lee, W.H. Analysis of the relationships among perceived service encounter quality, service value, satisfaction and behavioral intention for physical therapy patients. J. Phys. Ther. Sci. 2017, 29, 2000–2003. [Google Scholar] [CrossRef] [PubMed]
- Bensken, W.P.; Dong, W.; Gullett, H.; Etz, R.S.; Stange, K.C. Changing Reasons for Visiting Primary Care Over a 35-Year Period. J. Am. Board Fam. Med. 2021, 34, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Tham, T.Y.; Tran, T.L.; Prueksaritanond, S.; Isidro, J.S.; Setia, S.; Welluppillai, V. Integrated health care systems in Asia: An urgent necessity. Clin. Interv. Aging 2018, 13, 2527–2538. [Google Scholar] [CrossRef] [PubMed]
- Vestjens, L.; Cramm, J.M.; Nieboer, A.P. An integrated primary care approach for frail community-dwelling older persons: A step forward in improving the quality of care. BMC Health Serv. Res. 2018, 18, 28. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Wang, D.; Li, C.; Wang, C.; Wang, M. Medical treatment behaviour of the elderly population in shanghai: Group features and influencing factor analysis. Int. J. Environ. Res. Public Health 2021, 18, 4108. [Google Scholar] [CrossRef]
- Liu, Y.; Zhong, L.; Yuan, S.; van de Klundert, J. Why patients prefer high-level healthcare facilities: A qualitative study using focus groups in rural and urban China. Br. Med. J. Glob. Health 2018, 3, e000854. [Google Scholar] [CrossRef]
- CHARLS Consent Form. 2011. Available online: http://charls.pku.edu.cn/en/page/documentation/2011_national_baseline (accessed on 8 September 2022).
- Zhao, Y.H.; John, S.; Chen, X.X.; Wang, Y. China Health and Retirement Longitudinal Study Wave 4 User’s Guide; National School of Development, Peking University: Beijing, China, 2020. [Google Scholar]
- Fu, Y.; Lin, W.; Yang, Y.; Du, R.; Gao, D. Analysis of diverse factors influencing the health status as well as medical and health service utilization in the floating elderly of China. BMC Health Serv. Res. 2021, 21, 438. [Google Scholar] [CrossRef]
- Tajvar, M.; Yaseri, M.; Karami, B.; Mohammadi, M. Pattern of Outpatient Health Service Utilization by Older People in Iran. Salmand-Iran. J. Ageing 2021, 15, 410–427. [Google Scholar] [CrossRef]
- Zhou, S.; Huang, T.; Li, A.; Wang, Z. Does universal health insurance coverage reduce unmet healthcare needs in China? Evidence from the National Health Service Survey. Int. J. Equity Health 2021, 20, 43. [Google Scholar] [CrossRef]
- Li, Y.; Toseef, M.U.; Jensen, G.A.; Ortiz, K.; González, H.M.; Tarraf, W. Gains in insurance coverage following the affordable care act and change in preventive services use among non-elderly US. Prev. Med. 2021, 148, 106546. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wang, M.; Yuan, C.; Guo, Y. The Present Situation Analysis and Development Countermeasure of the New Mode of the Combination of Wisdom Pension and Medical Care. In Proceedings of the International Conference on Robots & Intelligent System (ICRIS), Haikou, China, 15–16 June 2019; pp. 335–338. [Google Scholar] [CrossRef]
- Li, Y.E.; Sun, X.L. Medical care and convalesce care: Concept determinatio, connotation analysis and evolution logic. Soft Sci. Health 2021, 35, 40–44. [Google Scholar] [CrossRef]
- Cheng, J.M.; Yuan, Y.M.; Lu, W.; Yang, L. Primary health care in china: Is china’s health reform reform for the whole nation? Prim. Health Care Res. Dev. 2017, 18, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Zeng, W.; Yan, L.; Yang, H.; Wen, J.; Li, W. The health service capacity of primary health care in west china: Different perspectives of physicians and their patients. BMC Health Serv. Res. 2019, 19, 143. [Google Scholar] [CrossRef]
- Ilinca, S.; Di Giorgio, L.; Salari, P.; Chuma, J. Socio-economic inequality and inequity in use of health care services in Kenya: Evidence from the fourth Kenya household health expenditure and utilization survey. Int. J. Equity Health 2019, 18, 196. [Google Scholar] [CrossRef] [PubMed]
- Miao, W.; Zhang, X.; Shi, B.; Tian, W.; Wu, B.; Lai, Y.; Li, Y.; Huang, Z.; Xia, Q.; Yang, H.; et al. Multi-dimensional vulnerability analysis on catastrophic health expenditure among middle-aged and older adults with chronic diseases in China. BMC Med. Res. Methodol. 2022, 22, 151. [Google Scholar] [CrossRef]
- Zeng, Y.; Xu, W.; Tao, X. What factors are associated with utilisation of health services for the poor elderly? Evidence from a nationally representative longitudinal survey in China. BMJ Open 2022, 12, e059758. [Google Scholar] [CrossRef]
- Xu, J.; Zheng, J.; Xu, L.; Wu, H. Equity of Health Services Utilization and Expenditure among Urban and Rural Residents under Universal Health Coverage. Int. J. Environ. Res. Public Health 2021, 18, 593. [Google Scholar] [CrossRef]
- Liu, J.; Yin, H.; Zheng, T.; Ilia, B.; Wang, X.; Chen, R.; Hao, Y.; Sun, H.; Jiao, M.; Kang, Z.; et al. Primary health institutions preference by hypertensive patients: Effect of distance, trust and quality of management in the rural Heilongjiang province of China. BMC Health Serv. Res. 2019, 19, 143. [Google Scholar] [CrossRef]
- Gao, K.; Li, B.-L.; Yang, L.; Zhou, D.; Ding, K.-X.; Yan, J.; Gao, Y.-J.; Huang, X.-R.; Zheng, X.-P. Cardiometabolic diseases, frailty, and healthcare utilization and expenditure in community-dwelling Chinese older adults. Sci. Rep. 2021, 11, 87444. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, P.; Lee, J.T.; Oldenburg, B.; van Heusden, A.; Haregu, T.N.; Wang, H. The Prevalence of Metabolic Disease Multimorbidity and Its Associations with Spending and Health Outcomes in Middle-Aged and Elderly Chinese Adults. Front. Public Health 2021, 9, 658706. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H.F.; Rice, J. Little Jiffy, Mark, IV. Educ. Psychol. Meas. 1974, 34, 111–117. [Google Scholar] [CrossRef]
- Barrett, P. Structural equation modelling: Adjudging model fit. Personal. Individ. Differ. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- NeJhaddadgar, N.; Ziapour, A.; Zakkipour, G.; Abbas, J.; Abolfathi, M.; Shabani, M. Effectiveness of telephone-based screening and triage during COVID-19 outbreak in the promoted primary healthcare system: A case study in Ardabil province, Iran. J. Public Health. 2020, 30, 1301–1306. [Google Scholar] [CrossRef]
- Wang, W.; Shan, Z.; Wang, G.; Gu, W.; Zhang, Y.; Lu, J.; Hu, L.; Kuang, J.; Zhao, D.; Dong, Y. Expert recommendations for diabetes with or without COVID-19 management in communities. Chin. J. Endocrinol. Metab. 2020, 36, 185–190. (In Chinese) [Google Scholar]
- Zhang, J.; Chen, Y.; Einav, L.; Levin, J.; Bhattacharya, J. Consolidation of primary care physicians and its impact on healthcare utilization. Health Econ. 2021, 30, 1361–1373. [Google Scholar] [CrossRef]
- Yeoh, E.-K.; Yam, C.H.; Chong, K.-C.; Chow, T.-Y.; Fung, V.L.; Wong, E.L.; Griffiths, S.M. An evaluation of universal vouchers as a demand-side subsidy to change primary care utilization: A retrospective analysis of longitudinal services utilisation and voucher claims data from a survey cohort in Hong Kong. Health Policy 2020, 124, 189–198. [Google Scholar] [CrossRef]
- Silva, A.G.; Queirós, A.; Rocha, N.P. Functioning and primary healthcare utilization in older adults: A 1-year follow-up study. Physiother. Theory Pract. 2018, 35, 278–287. [Google Scholar] [CrossRef]
- Jin, Y.; Xu, J.; Zhu, W.; Zhang, Y.; Xu, L.; Meng, Q. Synergy of policies to strengthen primary care: Evidence from a national repeated cross-sectional study. BMC Health Serv. Res. 2020, 20, 865. [Google Scholar] [CrossRef]
- Shen, X.Z.; Wu, S.X. Dilemma and outlet of the development of secondary hospitals in China. Chin. J. Hosp. Adm. 2021, 37, 864–867. (In Chinese) [Google Scholar]
- Zhang, X.J. Comparative analysis of the development of hospitals and primary healthcare institutions from 2009 to 2018. Chin. J. Hosp. Adm. 2020, 36, 250–255. (In Chinese) [Google Scholar]
- Li, L.I.; Pei, R.; Sun, T.; Liang, G.; LI, G.; Zhang, Z. Research on supply-side reform on community health institutions providing home based pension service. Chin. J. Health Policy 2016, 29, 52–56. (In Chinese) [Google Scholar]



{kind=link}
{kind=link}
| Latent Variable λi | Observed Variable ρij | Definition | M (SD)/% |
|---|---|---|---|
| Medical insurance | Reimbursement rate | Medical insurance reimbursement expenses/Total cost (0–100) | 20.202 (33.171) |
| Type of reimbursement | 1 = No insurance | 62.67% | |
| 2 = Urban employee medical insurance | 6.98% | ||
| 3 = Urban and rural resident medical insurance | 28.53% | ||
| 4 = Government medical insurance | 1.01% | ||
| 5 = Private medical insurance | 0.81% | ||
| Combined medical care and pension services in the community | Medical services in the community pension center | 0 = No | 95.5% |
| 1 = Yes | 4.5% | ||
| Use of pension care in the community | 0 = No | 95.5% | |
| 1 = Yes | 4.5% | ||
| Health service supply in primary care institutions | Number of primary care institutions | Number of primary care institutions per 10,000 people | 7.186 (2.207) |
| Number of beds in primary care institutions | Number of beds in primary medical institutions per 10,000 people | 12.044 (3.514) | |
| Number of the physician in primary care institutions | Health technicians in primary care institutions per 10,000 people | 28.442 (3.273) | |
| Health service demand | Number of chronic diseases | Discrete variable | 4.407 (3.032) |
| ADL | 0 = Without difficulty | 67.78% | |
| 1 = With difficulty | 32.22% | ||
| IADL | 0 = Without difficulty | 62.01% | |
| 1 = With difficulty | 37.99% | ||
| Outpatient use of primary care institutions during the past month | 0 = No | 69.3% | |
| 1 = Yes | 30.7% | ||
| KMO | 0.640 | |
| Bartlett sphericity test | X2 | 11,466.259 |
| df | 55 | |
| p | 0.000 | |
| Index | Fitting Index | Value | Standard |
|---|---|---|---|
| Absolute fit | RMR | 0.061 | <0.08 |
| RMSRA | 0.031 | <0.05 | |
| GFI | 0.994 | >0.90 | |
| AGFI | 0.982 | >0.90 | |
| Χ2/df | 2.941 | 1~3 | |
| Value-added fit | NFI | 0.991 | >0.90 |
| RFI | 0.986 | >0.90 | |
| IFI | 0.994 | >0.90 | |
| TLI | 0.991 | >0.90 | |
| CFI | 0.994 | >0.90 | |
| Simple fit | PCFI | 0.633 | >0.50 |
| PNFI | 0.631 | >0.50 |
| Indirect Paths | Estimate | Bias-Corrected CI (95%) | p-Value |
|---|---|---|---|
| Medical insurance → Supply of PCIs → PHC use | −0.010 | (−0.021, −0.004) | 0.004 *** |
| Medical insurance → Health service demand → PHC use | 0.000 | (−0.005, 0.001) | 0.423 |
| Medical insurance → Health service demand → Supply of PCIs →PHC use | −0.009 | (−0.019, −0.002) | 0.011 ** |
| Combined medical care and pension services in the community → Supply of PCIs → PHC use | −0.010 | (−0.021, −0.004) | 0.004 *** |
| Combined medical care and pension services in the community → Health service demand → PHC use | 0.000 | (−0.001, 0.007) | 0.432 |
| Combined medical care and pension services in community → Health service demand → Supply of PCIs → PHC use | −0.008 | (−0.019, −0.002) | 0.015 ** |
| Health service demand → Supply of PCIs → PHC use | 0.002 | (0.000, 0.006) | 0.025 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, L.; Fang, Y.; Yang, S.; Xu, Y. How to Make Primary Healthcare More Popular: Evidence from the Middle-Aged and Elderly in China. Healthcare 2022, 10, 1783. https://doi.org/10.3390/healthcare10091783
Fu L, Fang Y, Yang S, Xu Y. How to Make Primary Healthcare More Popular: Evidence from the Middle-Aged and Elderly in China. Healthcare. 2022; 10(9):1783. https://doi.org/10.3390/healthcare10091783
Chicago/Turabian StyleFu, Liping, Ya’nan Fang, Shu Yang, and Yanqing Xu. 2022. "How to Make Primary Healthcare More Popular: Evidence from the Middle-Aged and Elderly in China" Healthcare 10, no. 9: 1783. https://doi.org/10.3390/healthcare10091783