
Nurses’ Opinions on Frailty


Abstract
:1. Introduction
2. Methods
2.1. Study Population and Data Collection
2.2. Measurement
2.3. Statistical Analyses
2.4. Ethics Approval
3. Results
3.1. Characteristics of the Respondents
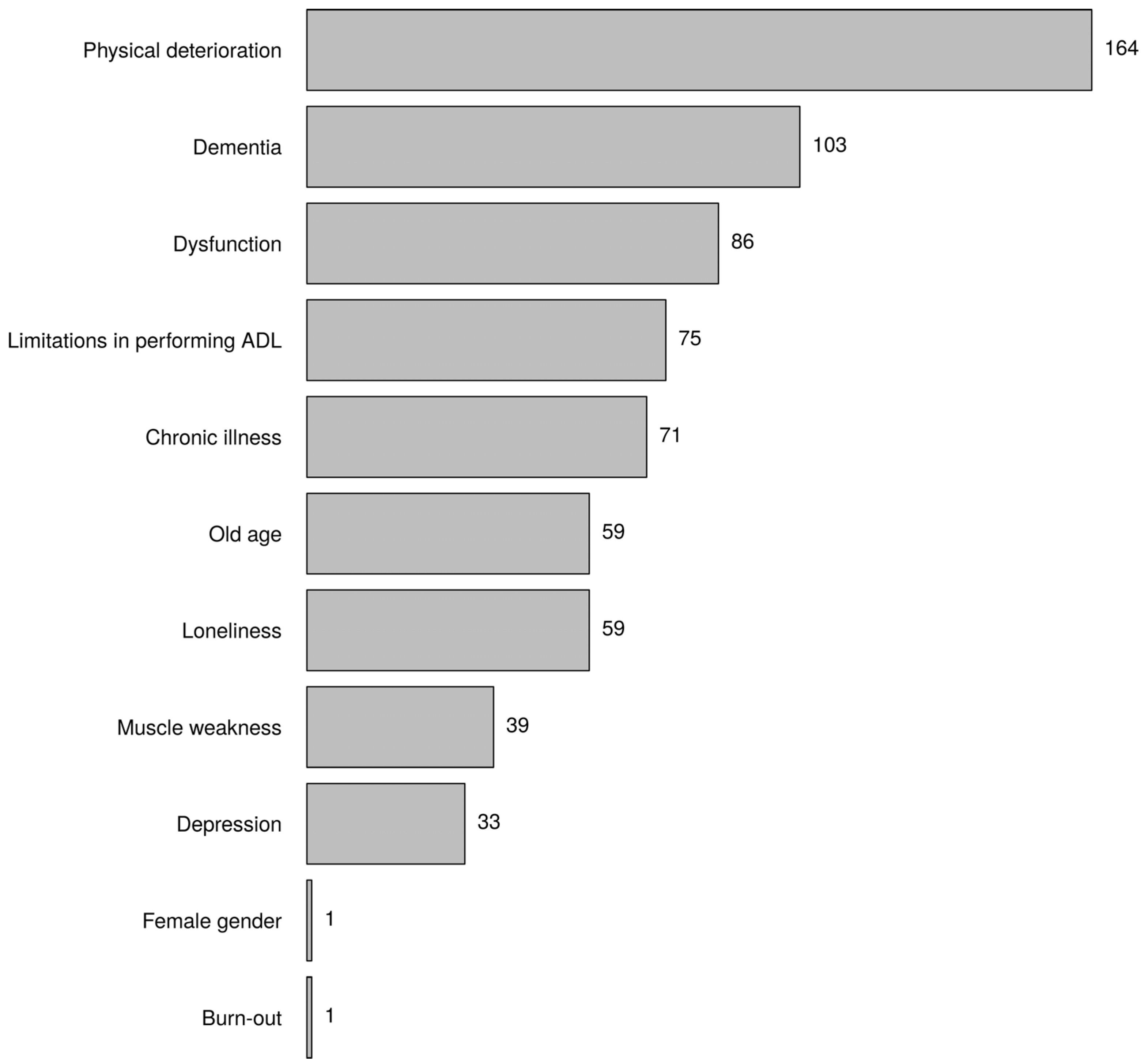
3.2. Keywords of Frailty
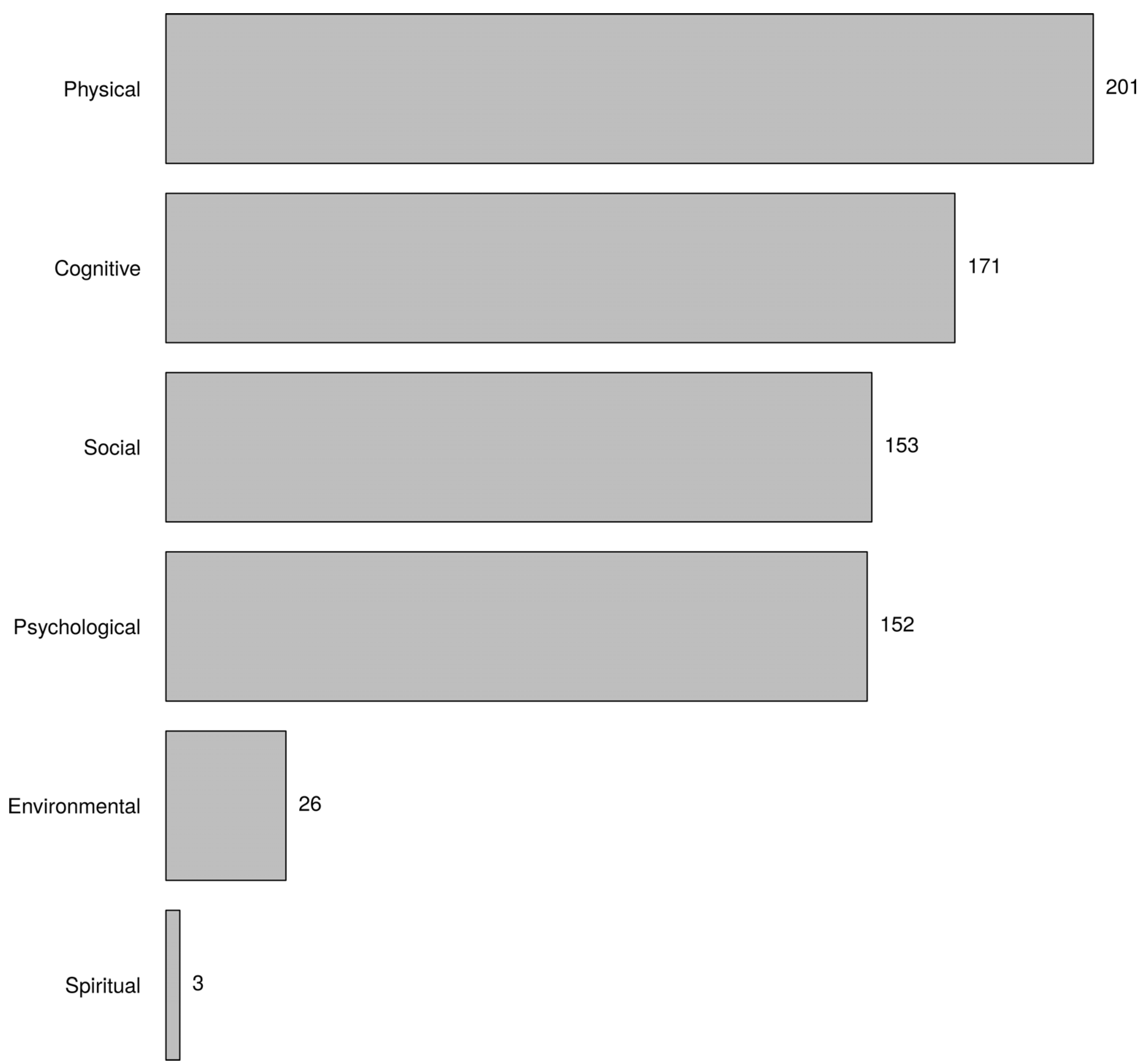
3.3. Frailty Domains
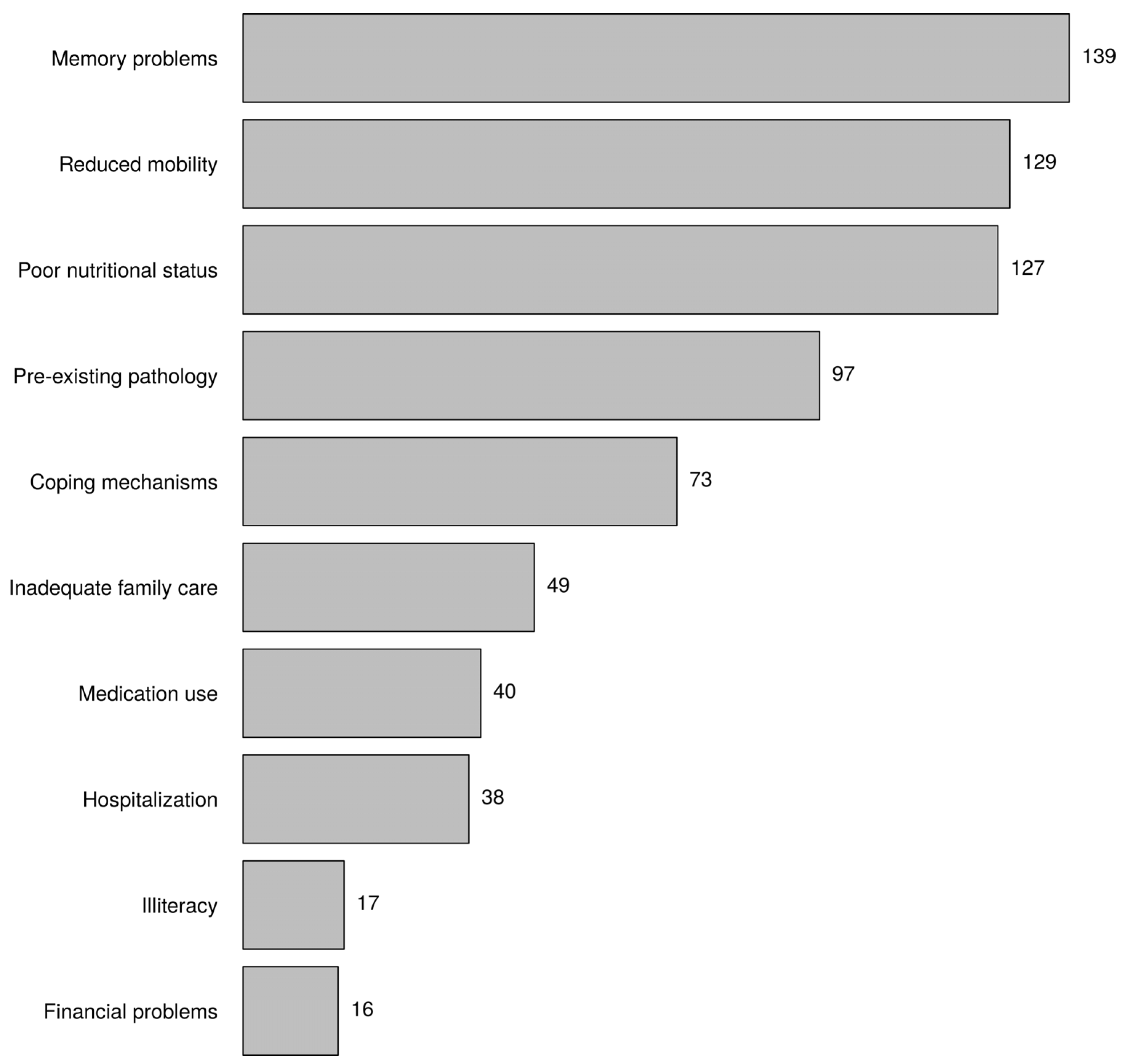
3.4. Causes of Frailty
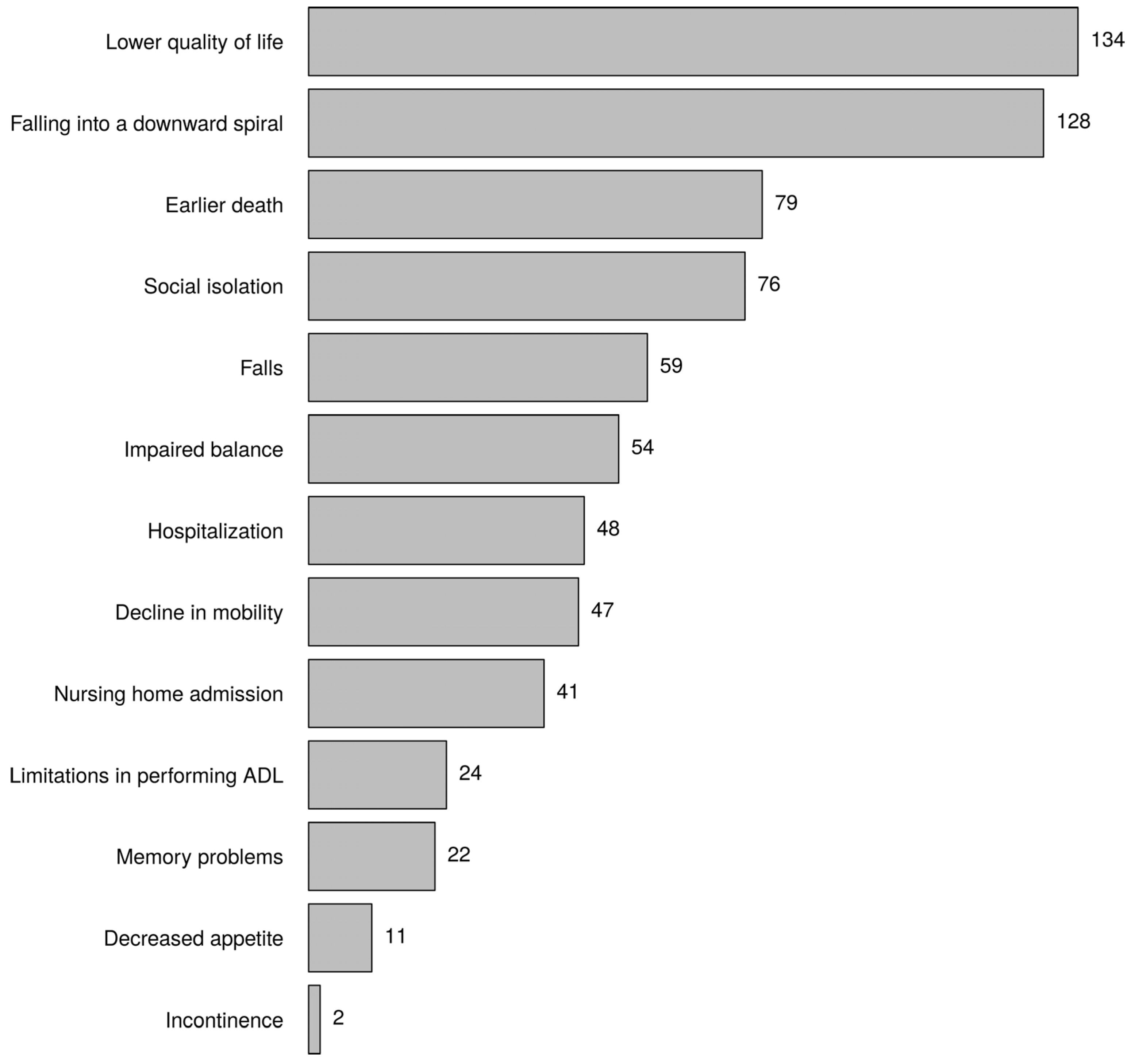
3.5. Consequences of Frailty
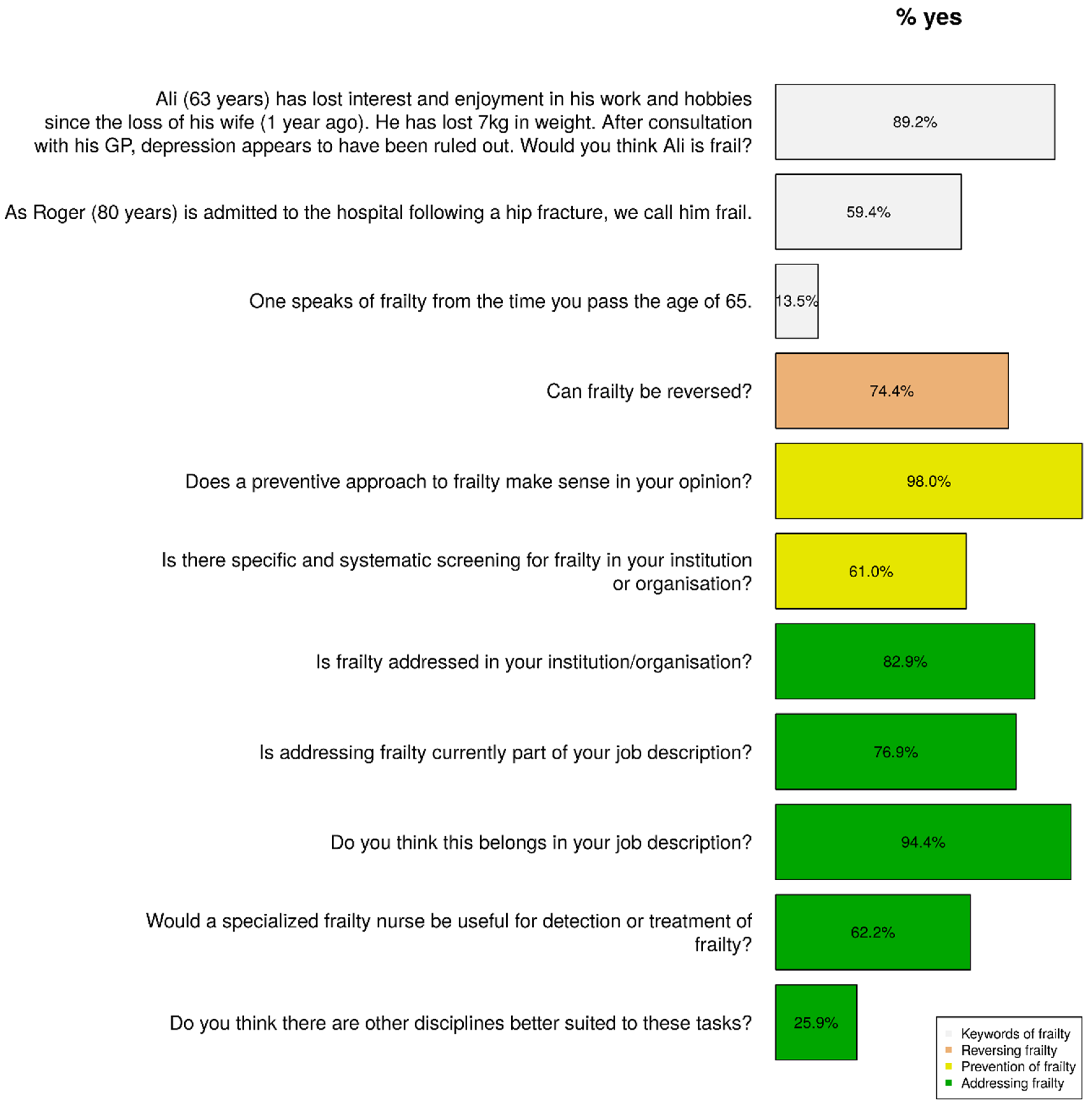
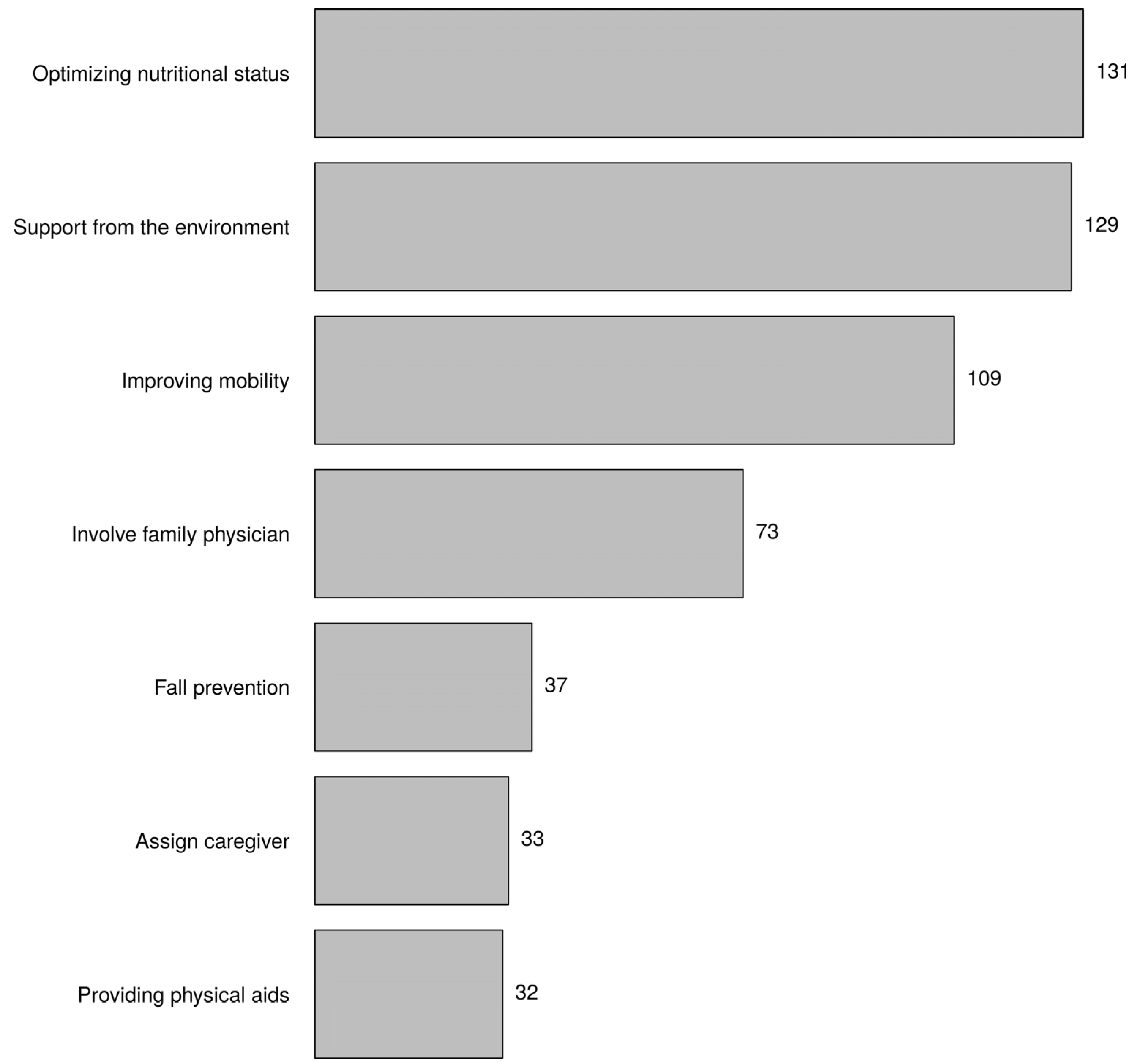
3.6. Reversing Frailty
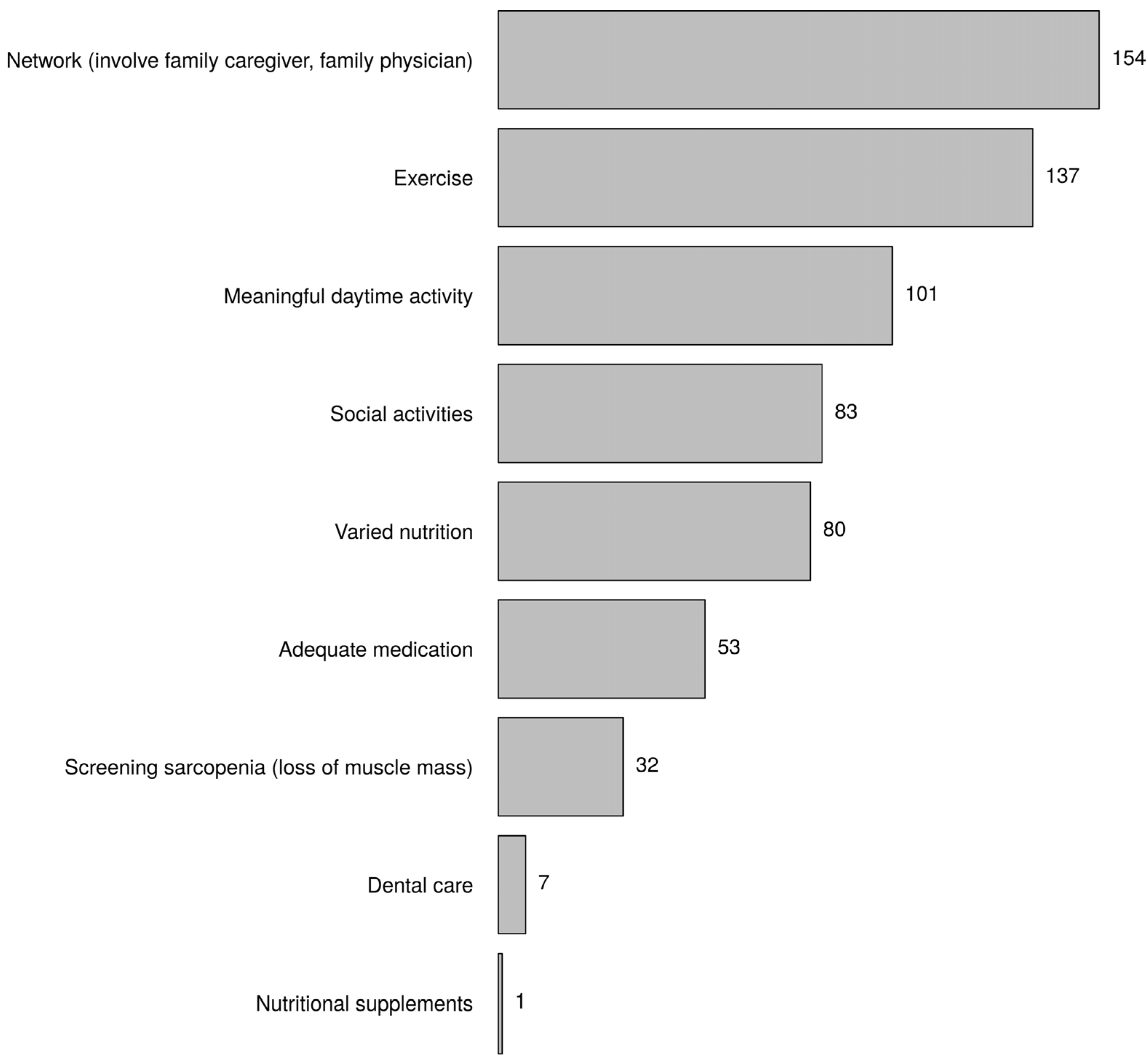
3.7. Prevention of Frailty
3.8. Addressing Frailty
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- United Nations Department of Economic and Social Affairs. Population Division. World Population Prospects. The 2015 Revision. Key findings and advance tables. Working paper No. ESA/P/WP.241. New York. 2015. Available online: http://esa.un.org/unpd/wpp/publications/files/key_findings_wpp_2015.pdf (accessed on 19 July 2017).
- Liu, H.X.; Ding, G.; Yu, W.J.; Liu, T.F.; Yan, A.Y.; Chen, H.Y.; Zhang, A.H. Association between frailty and incident risk of disability in community-dwelling elder people: Evidence from a meta-analysis. Public Health 2019, 175, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a predictor of nursing home placement among community-dwelling older adults: A systematic review and meta-analysis. J. Geriatr. Phys. Ther. 2018, 41, 42–48. [Google Scholar] [CrossRef]
- Chang, S.F.; Lin, H.C.; Cheng, C.L. The relationship of frailty and hospitalization among older people: Evidence from a meta-analysis. J. Nurs. Sch. 2018, 50, 383–391. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between frailty and quality of life among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, S.; Vella-Azzopardi, R.; Beckwee, D.; Habbig, A.K.; Scafoglieri, A.; Jansen, B.; Bautmans, I.; Gerontopole Brussels Study group. Frailty and the prediction of negative health outcomes: A meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1163.e1–1163.e17. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Abellan van Kan, G.; Rolland, Y.M.; Morley, J.E.; Vellas, B. Frailty: Toward a clinical definition. J. Am. Med. Dir. Assoc. 2008, 9, 71–72. [Google Scholar] [CrossRef]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. The Tilburg Frailty Indicator: Psychometric properties. J. Am. Med. Dir. Assoc. 2010, 11, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Obbia, P.; Graham, C.; Duffy, F.J.R.; Gobbens, R.J.J. Preventing frailty in older people: An exploration of primary care professionals’ experiences. Int. J. Older People Nurs. 2020, 15, e12297. [Google Scholar] [CrossRef] [PubMed]
- Coker, J.F.; Martin, M.E.; Simpson, R.M.; Lafortune, L. Frailty: An in-depth qualitative study exploring the views of community care staff. BMC Geriatr. 2019, 19, 47. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, S.; Edberg, A.-K.; Dahlin-Ivanoff, S. Swedish health care professionals’ view of frailty in older persons. J. Appl. Gerontol. 2012, 31, 622–640. [Google Scholar] [CrossRef]
- Avgerinou, C.; Kotsani, M.; Gavana, M.; Andreou, M.; Papageorgiou, D.I.; Roka, V.; Symintiridou, D.; Manolaki, C.; Soulis, G.; Smyrnakis, E. Perceptions, attitudes and training needs of primary healthcare professionals in identifying and managing frailty: A qualitative study. Eur. Geriatr. Med. 2021, 12, 321–332. [Google Scholar] [CrossRef]
- Britton, H. What are community nurses’ experiences of assessing frailty and assisting in planning subsequent interventions? Br. J. Community Nurs. 2017, 22, 440–445. [Google Scholar] [CrossRef]
- Papadopoulou, C.; Barrie, J.; Andrew, M.; Martin, J.; Birt, A.; Raymond Duffy, F.J.; Hendry, A. Perceptions, practices and educational needs of community nurses to manage frailty. Br. J. Community Nurs. 2021, 26, 136–142. [Google Scholar] [CrossRef]
- Warnier, R.M.J.; van Rossum, E.; Du Moulin, M.; van Lottum, M.; Schols, J.; Kempen, G. The opinions and experiences of nurses on frailty screening among older hospitalized patients. An exploratory study. BMC Geriatr. 2021, 21, 624. [Google Scholar] [CrossRef]
- Parish, A.; Kim, J.; Lewallen, K.M.; Miller, S.; Myers, J.; Panepinto, R.; Maxwell, C.A. Knowledge and perceptions about aging and frailty: An integrative review of the literature. Geriatr. Nurs. 2019, 40, 13–24. [Google Scholar] [CrossRef]
- Maxwell, C.A.; Wang, J. Understanding frailty: A nurse’s guide. Nurs. Clin. N. Am. 2017, 52, 349–361. [Google Scholar] [CrossRef]
- Van Hoof, A.; Léonard, S.; Bonnez, Y.; Vermeiren, S. De bekendheid van frailty in de praktijk. Tijdschr. Gerontol. Geriatr. 2022, 53, 1–8. [Google Scholar]
- Central Committee on Research Involving Human Subjects. Available online: https://english.ccmo.nl/investigators/legal-framework-for-medical-scientific-research/your-research-is-it-subject-to-the-wmo-or-not (accessed on 28 January 2021).
- Markle-Reid, M.; Browne, G. Conceptualizations of frailty in relation to older adults. J. Adv. Nurs. 2003, 44, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Petermann-Rocha, F.; Lyall, D.M.; Gray, R.S.; Esteban-Cornejo, I.; Quinn, T.J.; Ho, F.K.; Pell, P.J.; Celis-Morales, C. Associations between physical frailty and dementia incidence: A prospective study from UK Biobank. Lancet 2020, 1, E58–E68. [Google Scholar] [CrossRef]
- Kojima, G.; Taniguchi, Y.; Iliffe, S.; Walters, K. Frailty as a predictor of Alzheimer disease, vascular dementia, and all dementia among community-dwelling older people: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Huang, Y.; Liu, Z.; Shen, R.; Chen, H.; Ma, C.; Zhang, T.; Li, S.; Prince, M. The association between frailty and incidence of dementia in Beijing: Findings from 10/66 dementia research group population-based cohort study. BMC Geriatr. 2020, 20, 138. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Abellan van Kan, A.; Rolland, Y.; Bergman, H.; Morley, J.E.; Kritchevsky, S.B.; Vellas, B. The I.A.N.A Task Force on frailty assessment of older people in clinical practice. J. Nutr. Health Aging 2008, 12, 29–37. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Ward, M.; McGarrigle, C.A.; Kenny, R.A. More than health: Quality of life trajectories among older adults-findings from the Irish Longitudinal Study of Ageing (TILDA). Qual Life Res. 2019, 28, 429–439. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Hawkins, K.; Yeh, C.S. The impact of loneliness on quality of life and patient satisfaction among older, sicker adults. Gerontol. Geriatr. Med. 2015, 1, 2333721415582119. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Toward a conceptual definition of frail community dwelling older people. Nurs. Outlook 2010, 58, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Schuurmans, H.; Steverink, N.; Lindenberg, S.; Frieswijk, N.; Slaets, J.P. Old or frail: What tells us more? J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M962–M965. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Towards an integral conceptual model of frailty. J. Nutr. Health Aging 2010, 14, 175–181. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Schols, J.M. The predictive validity of the Tilburg Frailty Indicator: Disability, health care utilization, and quality of life in a population at risk. Gerontologist 2012, 52, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Andreasen, J. The prediction of readmission and mortality by the domains and components of the Tilburg Frailty Indicator (TFI): A prospective cohort study among acutely admitted older patients. Arch. Gerontol. Geriatr. 2020, 89, 104077. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.J.; van Assen, M.; Augustijn, H.; Goumans, M.; van der Ploeg, T. Prediction of mortality by the Tilburg Frailty Indicator (TFI). J. Am. Med. Dir. Assoc. 2020, 22, 607.e1–607.e6. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Travers, J.; Romero-Ortuno, R.; Bailey, J.; Cooney, M.T. Delaying and reversing frailty: A systematic review of primary care interventions. The British Journal of General Practice: J. R. Coll. Gen. Pract. 2019, 69, e61–e69. [Google Scholar] [CrossRef]
- Takatori, K.; Matsumoto, D. Social factors associated with reversing frailty progression in community-dwelling late-stage elderly people: An observational study. PLoS ONE 2021, 16, e0247296. [Google Scholar] [CrossRef]
- Ambagtsheer, R.C.; Archibald, M.M.; Lawless, M.; Mills, D.; Yu, S.; Beilby, J.J. General practitioners’ perceptions, attitudes and experiences of frailty and frailty screening. Aust. J. Gen. Pract. 2019, 48, 426–433. [Google Scholar] [CrossRef]
- Bleijenberg, N.; Ten Dam, V.H.; Steunenberg, B.; Drubbel, I.; Numans, M.E.; De Wit, N.J.; Schuurmans, M.J. Exploring the expectations, needs and experiences of general practitioners and nurses towards a proactive and structured care programme for frail older patients: A mixed-methods study. J. Adv. Nurs. 2013, 69, 2262–2273. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuven. Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Talar, K.; Hernández-Belmonte, A.; Vetrovsky, T.; Steffl, M.; Kałamacka, E.; Courel-Ibáñez, J. Benefits of resistance training in early and late stages of frailty and sarcopenia: A systematic review and meta-analysis of randomized controlled studies. J. Clin. Med. 2021, 10, 1630. [Google Scholar] [CrossRef]
- Kojima, G. Prevalence of frailty in nursing homes: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J. Factors affecting the collaboration between nurses in community health department and social workers in welfare services department. Int. J. Health Policy Manag. 2008, 18, 125–147. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | ||
|---|---|---|
| N | % | |
| Characteristic | ||
| Gender | ||
| Male | 14 | 5.6 |
| Female | 237 | 94.4 |
| Age category in years | ||
| <44 | 77 | 30.7 |
| 44 – <55 | 81 | 32.3 |
| ≥55 | 91 | 37.1 |
| Working experience in years | ||
| <20 | 70 | 27.9 |
| 20 – <33 | 90 | 35.9 |
| ≥33 | 91 | 36.2 |
| Working hours per week | ||
| <28 | 76 | 30.4 |
| 28 – <32 | 48 | 19.2 |
| ≥32 | 126 | 50.4 |
| Profession | ||
| Nurse | 160 | 63.8 |
| Nurse specialist | 45 | 17.9 |
| Other | 46 | 18.3 |
| Institution | ||
| Hospital | 105 | 41.8 |
| Nursing home | 65 | 25.9 |
| Residential care centre | 16 | 6.4 |
| Primary healthcare | 44 | 17.5 |
| Psychiatric institution | 3 | 1.2 |
| Geriatric rehabilitation centre | 9 | 3.6 |
| Other | 9 | 3.6 |
| Employed in years | ||
| <5 | 73 | 30.3 |
| 5 – <15 | 85 | 35.3 |
| ≥15 | 83 | 34.4 |
| Education | ||
| Post-secondary vocational education | 49 | 19.7 |
| Higher vocational education | 123 | 49.4 |
| Post-higher vocational education | 6 | 2.4 |
| Higher vocational education master | 49 | 19.7 |
| University | 17 | 6.8 |
| Other | 5 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gobbens, R.J.; Vermeiren, S.; Van Hoof, A.; van der Ploeg, T. Nurses’ Opinions on Frailty. Healthcare 2022, 10, 1632. https://doi.org/10.3390/healthcare10091632
Gobbens RJ, Vermeiren S, Van Hoof A, van der Ploeg T. Nurses’ Opinions on Frailty. Healthcare. 2022; 10(9):1632. https://doi.org/10.3390/healthcare10091632
Chicago/Turabian StyleGobbens, Robbert J., Sofie Vermeiren, An Van Hoof, and Tjeerd van der Ploeg. 2022. "Nurses’ Opinions on Frailty" Healthcare 10, no. 9: 1632. https://doi.org/10.3390/healthcare10091632