
Frail Older Adults without Occupational Dysfunction Maintain Good Subjective Well-Being: A Cross-Sectional Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
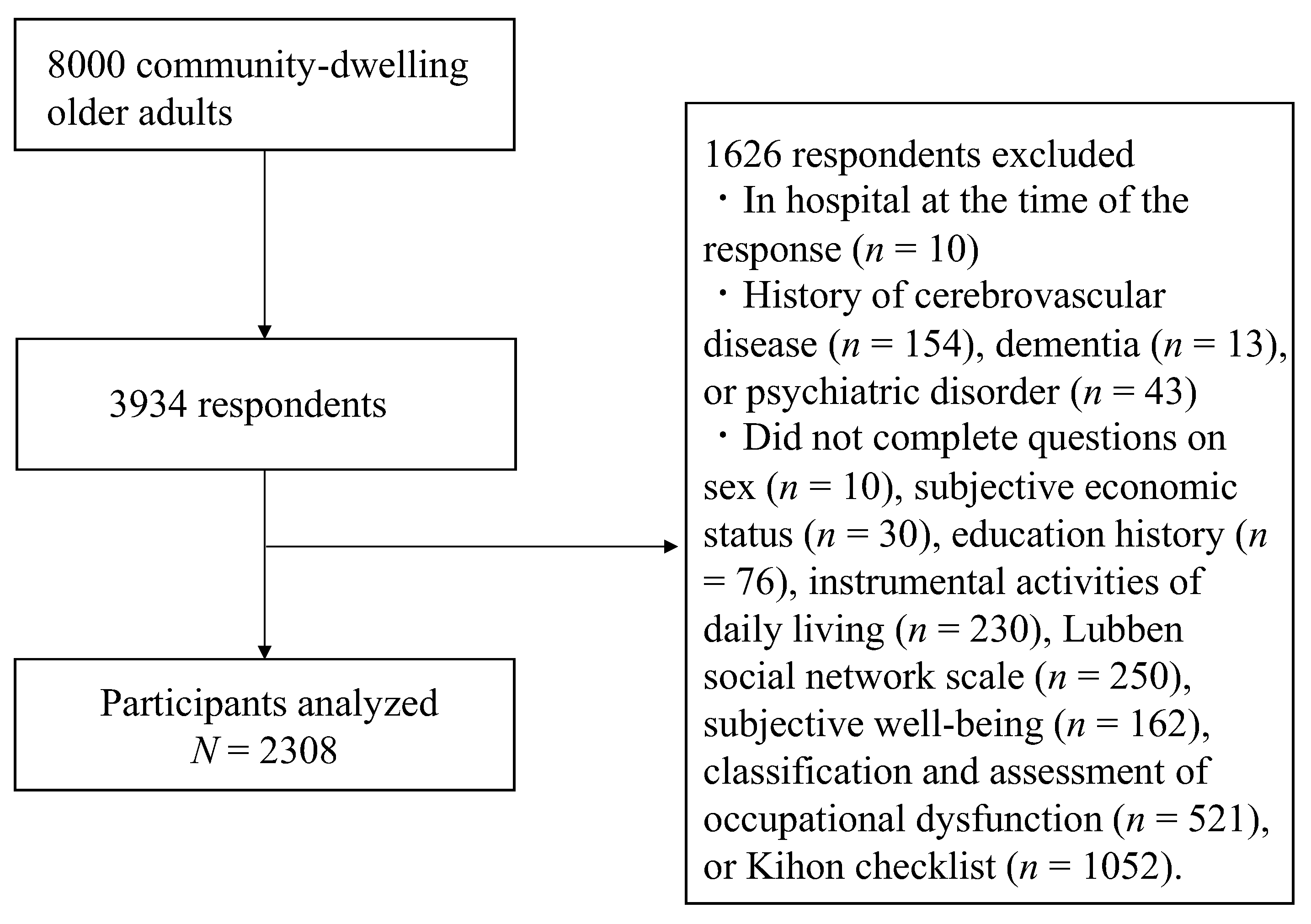
2.1. Participants and Data Collection
2.2. Measurement Variables
2.2.1. Definition of Frailty
2.2.2. Occupational Dysfunction
2.2.3. Subjective Well-Being
2.2.4. Demographic Data
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493737 UK Biobank participants. Lancet Public Health 2018, 3, e323–e332. [Google Scholar] [CrossRef]
- Song, X.; Mitnitski, A.; Rockwood, K. Prevalence and 10-year outcomes of frailty in older adults in relation to deficit accumulation. J. Am. Geriatr. Soc. 2010, 58, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Murayama, H.; Kobayashi, E.; Okamoto, S.; Fukaya, T.; Ishizaki, T.; Liang, J.; Shinkai, S. National prevalence of frailty in the older Japanese population: Findings from a nationally representative survey. Arch. Gerontol. Geriatr. 2020, 91, 104220. [Google Scholar] [CrossRef]
- Chan, D.C.; Tsou, H.H.; Yang, R.S.; Tsauo, J.Y.; Chen, C.Y.; Hsiung, C.A.; Kuo, K.N. A pilot randomized controlled trial to improve geriatric frailty. BMC Geriatr. 2012, 12, 58. [Google Scholar] [CrossRef]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Ota, N.; Shimotoyodome, A.; Hase, T.; Hosoi, E.; Yoshida, H. Effects of exercise and milk fat globule membrane (MFGM) supplementation on body composition, physical function, and hematological parameters in community-dwelling frail Japanese women: A randomized double blind, placebo-controlled, follow-up trial. PLoS ONE 2015, 10, e0116256. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: A randomized controlled trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Sist, X.; Domenich, R.; Jurado, L.; Saiz, A.; Roces, A.; Palomera, E.; Tarradelles, M.; Papiol, M. Effectiveness of an intervention to prevent frailty in pre-frail community-dwelling older people consulting in primary care: A randomised controlled trial. Age Ageing 2017, 46, 401–407. [Google Scholar] [CrossRef]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J. A multicomponent exercise intervention that reverses frailty and improves cognition, emotion, and social networking in the community-dwelling frail elderly: A randomized clinical trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty screening and interventions: Considerations for clinical practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Teraoka, M.; Kyougoku, M. Development of the final version of the classification and assessment of occupational dysfunction scale. PLoS ONE 2015, 10, e0134695. [Google Scholar] [CrossRef] [PubMed]
- Hasebe, S.; Kohiyama, K. Clinical usefulness of occupational therapy focused on the severity of occupational dysfunction among three hospitalized patients in a convalescent rehabilitation ward: A case study. Jpn Occupat. Ther. Res. 2021, 40, 351–358. [Google Scholar]
- Takano, D.; Teraoka, M. Efficacy of Occupation-Based Practice 2.0 in targeting home-visit rehabilitation. Jpn Occupat. Ther. Res. 2019, 38, 358–364. [Google Scholar]
- Government of Kasama City. Statistical Information of Kasama City. Available online: https://www.city.kasama.lg.jp/data/doc/1547708244_doc_81_0.pdf (accessed on 1 August 2022).
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef]
- Okuzono, S.S.; Shiba, K.; Kim, E.S.; Shirai, K.; Kondo, N.; Fujiwara, T.; Kondo, K.; Lomas, T.; Trudel-Fitzgerald, C.; Kawachi, I.; et al. Ikigai and subsequent health and wellbeing among Japanese older adults: Longitudinal outcome-wide analysis. Lancet Reg. Health-West. Pac. 2022, 21, 100391. [Google Scholar] [CrossRef]
- VanderWeele, T.J. On the promotion of human flourishing. Proc. Natl. Acad. Sci. USA 2017, 114, 8148–8156. [Google Scholar] [CrossRef]
- Fordyce, M.W. A review of research on the happiness measures: A sixty second index of happiness and mental health. Soc. Indic. Res. 1988, 20, 355–381. [Google Scholar] [CrossRef]
- Koyano, W.S.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence in the elderly living at home: Development of an index of competence. Jpn J. Public Health 1987, 34, 109–114. [Google Scholar]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Association between social participation and 3-year change in instrumental activities of daily living in community-dwelling elderly adults. J. Am. Geriatr. Soc. 2017, 65, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Kurumatani, N.; Saeki, K. The differential effects of type and frequency of social participation on IADL declines of older people. PLoS ONE 2018, 13, e0207426. [Google Scholar] [CrossRef] [PubMed]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an abbreviated version of the Lubben Social Network Scale among three European Community-dwelling older adult populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadeh, M.; Welmer, A.K.; Dekhtyar, S.; Fratiglioni, L.; Calderón-Larrañaga, A. The role of psychological and social well-being on physical function trajectories in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1579–1585. [Google Scholar] [CrossRef]
- Trevisan, C.; Veronese, N.; Maggi, S.; Baggio, G.; Toffanello, E.D.; Zambon, S.; Sartori, L.; Musacchio, E.; Perissinotto, E.; Crepaldi, G.; et al. Factors influencing transitions between frailty states in elderly adults: The Progetto Veneto Anziani longitudinal study. J. Am. Geriatr. Soc. 2017, 65, 179–184. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Frailty | Robust | Robust | Pre-Frail | Pre-Frail | Frail | Frail |
|---|---|---|---|---|---|---|
| Occupational dysfunction | HOF | OD | HOF | OD | HOF | OD |
| n | 1235 | 101 | 571 | 138 | 175 | 88 |
| Age (years), mean ± SD | 71.5 ± 4.7 | 71.5 ± 4.9 | 72.8 ± 5.0 | 71.8 ± 5.3 | 75.1 ± 5.8 | 73.9 ± 6.0 |
| Female, % (n) | 48.2 (595) | 45.5 (46) | 46.8 (267) | 51.4 (71) | 38.9 (68) | 43.2 (38) |
| Education history (≥ high school), % (n) | 88.5 (1093) | 85.1 (86) | 81.8 (467) | 83.3 (115) | 77.7 (136) | 87.5 (77) |
| Subjective economic status (poor), % (n) | 12.0 (148) | 24.8 (25) | 22.1 (126) | 25.4 (35) | 34.3 (60) | 44.3 (39) |
| IADL ability (disability), % (n) | 4.0 (50) | 4.0 (4) | 10.3 (59) | 5.1 (7) | 23.4 (41) | 14.8 (13) |
| LSNS (points), mean ± SD | 17.9 ± 5.6 | 15.7 ± 6.0 | 15.7 ± 5.7 | 14.3 ± 5.4 | 12.9 ± 5.6 | 12.5 ± 6.2 |
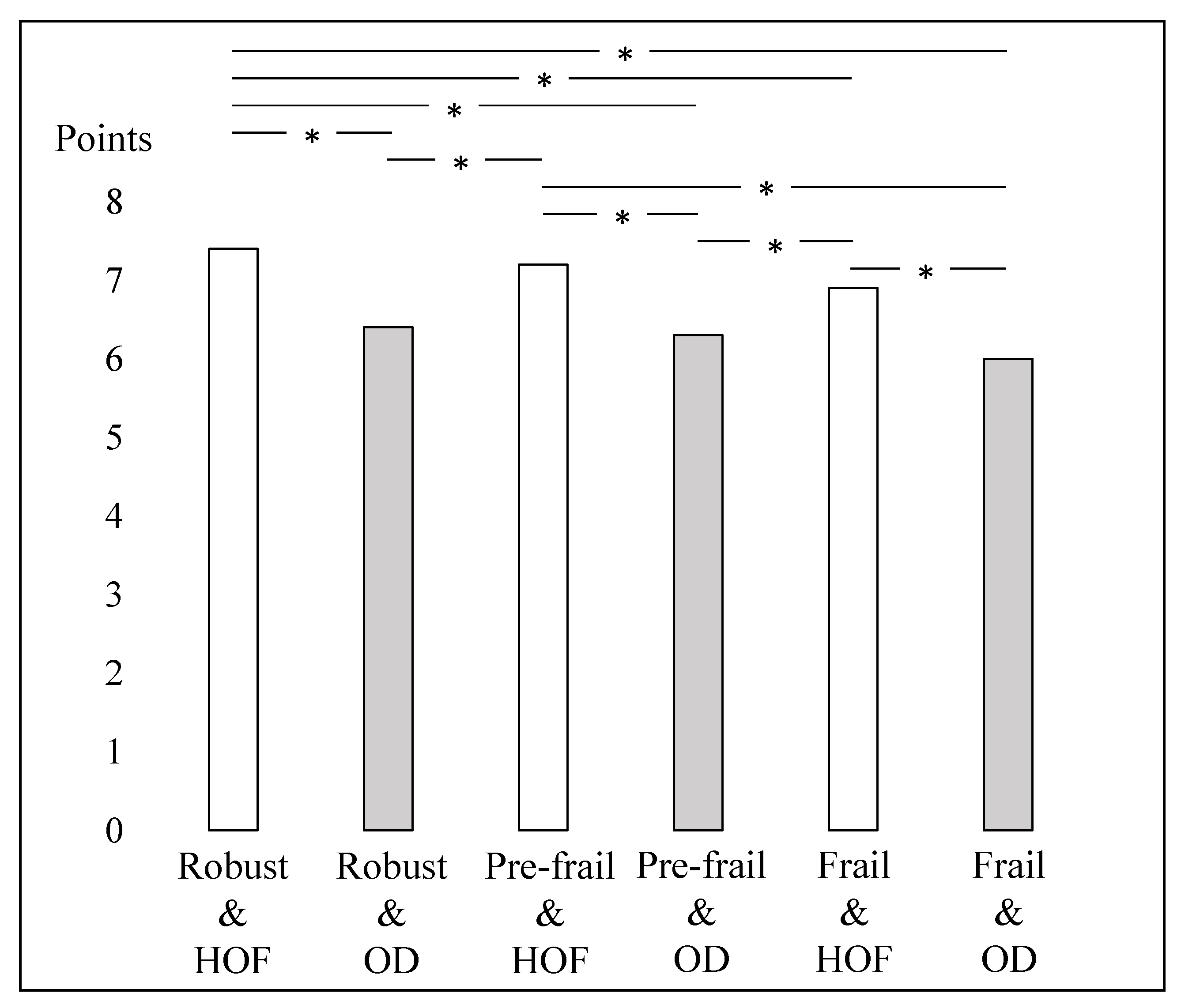
| Subjective well-being (points), mean ± SD | 7.5 ± 1.7 | 6.3 ± 1.8 | 7.1 ± 1.9 | 6.1 ± 1.9 | 6.5 ± 2.0 | 5.5 ± 2.0 |
| CAOD (points), mean ± SD | 28.5 ± 10.3 | 58.9 ± 6.2 | 31.4 ± 10.4 | 59.8 ± 7.3 | 35.9 ± 10.0 | 63.6 ± 10.4 |
| Kihon checklist (points), mean ± SD | 1.5 ± 1.1 | 1.8 ± 1.0 | 5.0 ± 1.0 | 5.4 ± 1.1 | 9.8 ± 2.2 | 10.6 ± 2.7 |
| Crude Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| Mean (95% CI) | ANOVA p | Post hoc Test with Bonferroni Correction | Mean (95% CI) | ANCOVA p | Post hoc Test with Bonferroni Correction | |
| Robust and healthy occupational function (A) | 7.5 (7.4–7.6) | <0.001 | A > B, C, D, E, F C > B, D, E, F E > D, F B > F | 7.4 (7.3–7.5) | <0.001 | A > B, D, E, F C > B, D, F E > D, F |
| Robust and OD (B) | 6.3 (6.0–6.7) | 6.4 (6.1–6.8) | ||||
| Pre-frail and healthy occupational function (C) | 7.1 (7.0–7.3) | 7.2 (7.1–7.4) | ||||
| Pre-frail and OD (D) | 6.1 (5.8–6.4) | 6.3 (6.0–6.6) | ||||
| Frail and healthy occupational function (E) | 6.5 (6.3–6.8) | 6.9 (6.6–7.2) | ||||
| Frail and OD (F) | 5.5 (5.1–5.8) | 6.0 (5.6–6.3) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujii, K.; Fujii, Y.; Kubo, Y.; Tateoka, K.; Liu, J.; Nagata, K.; Nakashima, D.; Okura, T. Frail Older Adults without Occupational Dysfunction Maintain Good Subjective Well-Being: A Cross-Sectional Study. Healthcare 2022, 10, 1922. https://doi.org/10.3390/healthcare10101922
Fujii K, Fujii Y, Kubo Y, Tateoka K, Liu J, Nagata K, Nakashima D, Okura T. Frail Older Adults without Occupational Dysfunction Maintain Good Subjective Well-Being: A Cross-Sectional Study. Healthcare. 2022; 10(10):1922. https://doi.org/10.3390/healthcare10101922
Chicago/Turabian StyleFujii, Keisuke, Yuya Fujii, Yuta Kubo, Korin Tateoka, Jue Liu, Koki Nagata, Daiki Nakashima, and Tomohiro Okura. 2022. "Frail Older Adults without Occupational Dysfunction Maintain Good Subjective Well-Being: A Cross-Sectional Study" Healthcare 10, no. 10: 1922. https://doi.org/10.3390/healthcare10101922