
The Impact of Socioeconomic Factors and Geriatric Syndromes on Frailty among Elderly People Receiving Home-Based Healthcare: A Cross-Sectional Study

 , , and
, , and 
Abstract
:1. Introduction
Aim
2. Material and Methods
2.1. Study Design and Participants
2.2. Instruments
2.2.1. Frailty Assessment
2.2.2. Geriatrics Syndromes
2.2.3. Socioeconomic Factors
2.3. Ethical Consideration
2.4. Data Analysis
3. Results
3.1. Demographic Data of the Participants
3.2. Distribution of the Socio-Economic Factors and Geriatrics Syndromes according to Gender and Frailty Classification
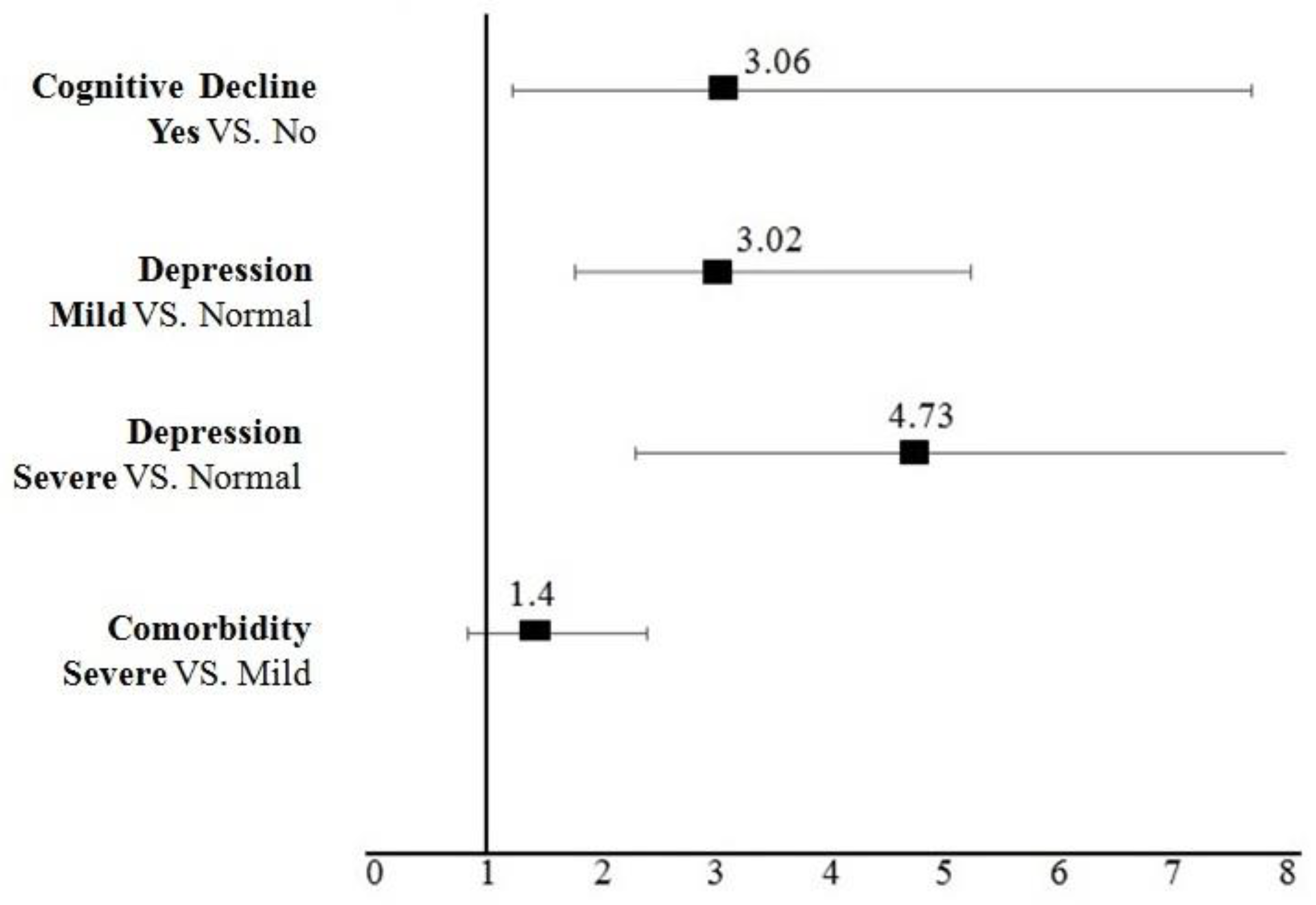
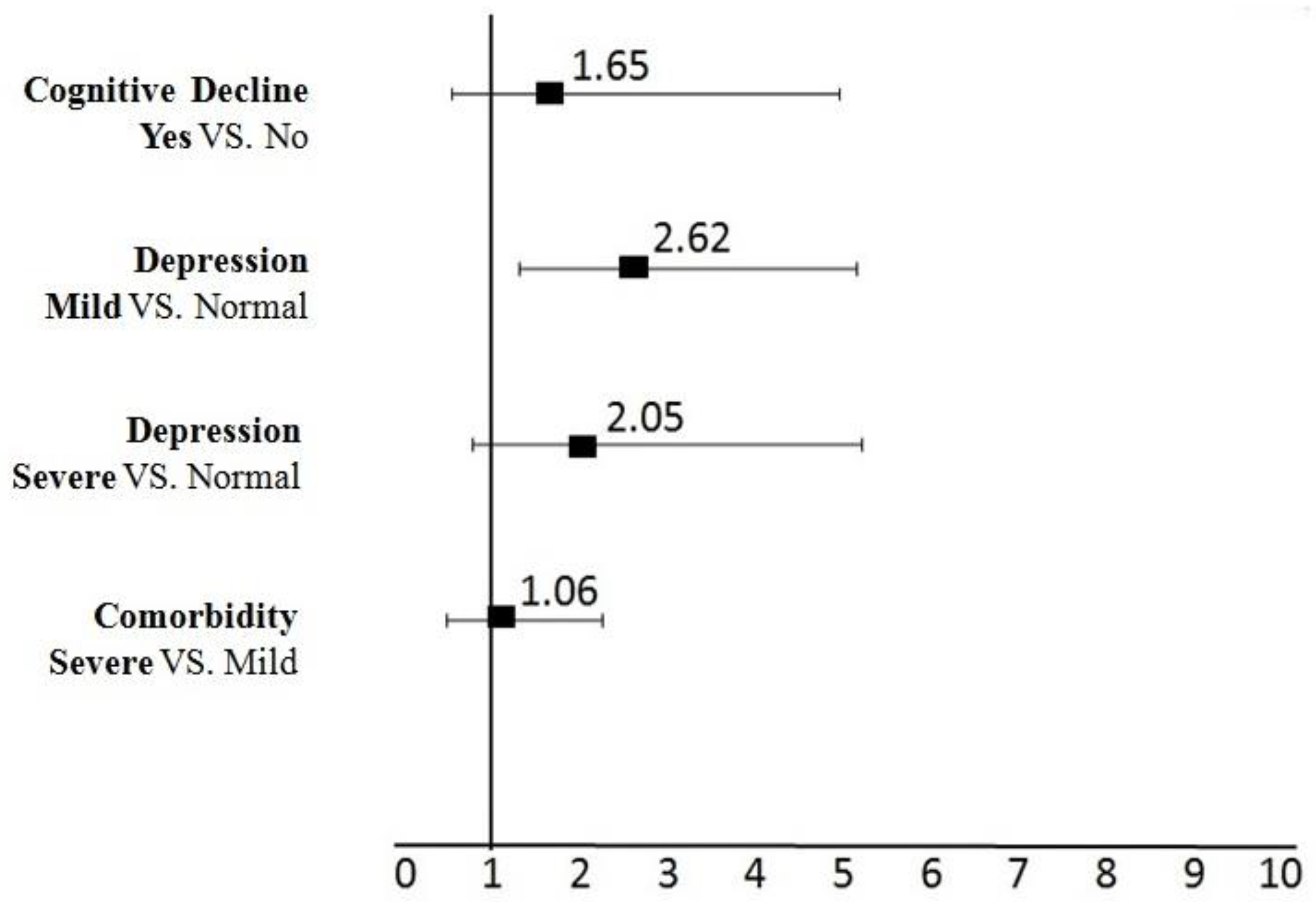
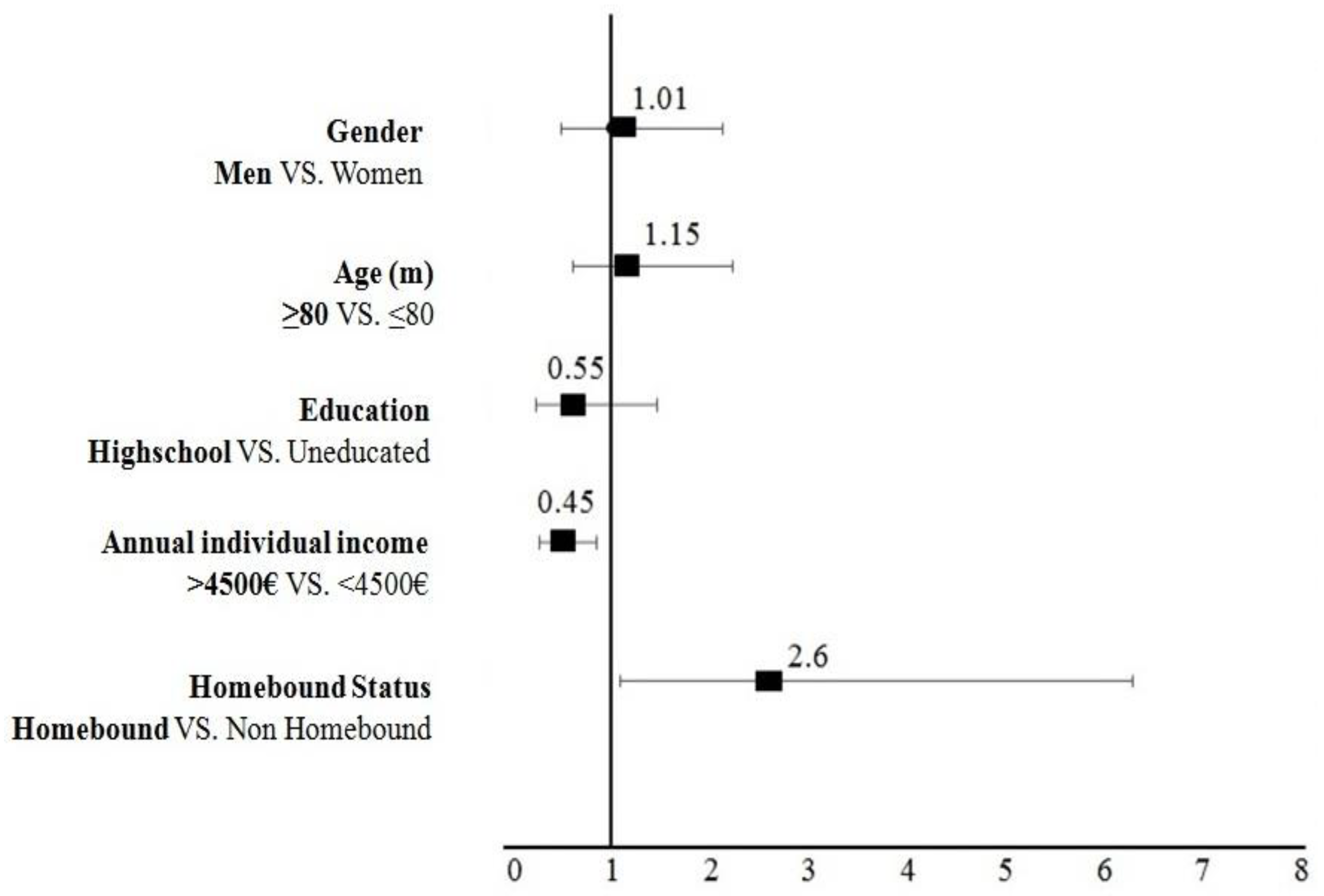
3.3. The impact of Geriatric Syndromes on Frailty
4. Discussion
5. Future Implications
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Makino, K.; Lee, S. Social Frailty Leads to the Development of Physical Frailty among Physically Non-Frail Adults: A Four-Year Follow-Up Longitudinal Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makizako, H.; Kubozono, T.; Kiyama, R.; Takenaka, T.; Kuwahata, S.; Tabira, T.; Kanoya, T.; Horinouchi, K.; Shimada, H.; Ohishi, M. Associations of social frailty with loss of muscle mass and muscle weakness among community-dwelling older adults. Geriatr. Gerontol. Int. 2019, 19, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Walkden, G.J.; Anderson, E.L.; Vink, M.P.; Tilling, K.; Howe, L.D.; Ben-Shlomo, Y. Frailty in older-age European migrants: Cross-sectional and longitudinal analyses of the Survey of Health, Aging and Retirement in Europe (SHARE). Soc. Sci. Med. 2018, 213, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of frailty in middle-aged and older community-dwelling Europeans living in 10 countries. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pioli, G.; Bendini, C.; Pignedoli, P.; Giusti, A.; Marsh, D. Orthogeriatric co-management-managing frailty as well as fragility. Injury 2018, 49, 1398–1402. [Google Scholar] [CrossRef] [PubMed]
- Dalton, A.; Zafirova, Z. Preoperative Management of the Geriatric Patient: Frailty and Cognitive Impairment Assessment. Anesthesiol. Clin. 2018, 36, 599–614. [Google Scholar] [CrossRef]
- Shimada, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Bae, S.; Arai, H. Behavioral Factors Related to the Incidence of Frailty in Older Adults. J. Clin. Med. 2020, 9, 3074. [Google Scholar] [CrossRef]
- Doi, T.; Makizako, H.; Tsutsumimoto, K.; Nakakubo, S.; Kim, M.J.; Kurita, S.; Hotta, R.; Shimada, H. Transitional status and modifiable risk of frailty in Japanese older adults: A prospective cohort study. Geriatr. Gerontol. Int. 2018, 18, 1562–1566. [Google Scholar] [CrossRef]
- Ko, Y.; Choi, K. Prevalence of frailty and associated factors in Korean older women: The KLoSA study. J. Women Aging 2017, 29, 15–25. [Google Scholar] [CrossRef]
- Adamakidou, T.; Kalokerinou-Anagnostopoulou, A. Home health nursing care services in Greece during an economic crisis. Int. Nurs. Rev. 2017, 64, 126–134. [Google Scholar] [CrossRef]
- Kleisiaris, C.; Kaffatou, E.M.; Papathanasiou, I.V.; Androulakis, E.; Panagiotakis, S.; Alvino, S.; Tziraki, C. Assessing the Impact of Frailty on Cognitive Function in Older Adults Receiving Home Care. Transl. Med. UniSa 2019, 19, 27–35. [Google Scholar]
- European Commission EIP on A and HA (EIPonAHA). Available online: https://futurium.ec.europa.eu/en/active-and-healthy-living-digital-world/library/eip-aha-achievements-action-group-a3-lifespan-health-promotion-prevention-age-related-frailty-and (accessed on 5 May 2022).
- Romero-Ortuno, R. The Frailty Instrument for primary care of the Survey of Health, Ageing and Retirement in Europe predicts mortality similarly to a frailty index based on comprehensive geriatric assessment. Geriatr. Gerontol. Int. 2013, 13, 497–504. [Google Scholar] [CrossRef]
- Konstantopoulos, K.; Vogazianos, P.; Doskas, T. Normative Data of the Montreal Cognitive Assessment in the Greek Population and Parkinsonian Dementia. Arch. Clin. Neuropsychol. 2016, 31, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Fountoulakis, K.N.; Tsolaki, M.; Iacovides, A.; Yesavage, J.; O’Hara, R.; Kazis, A.; Ierodiakonou, C. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging Clin. Exp. Res. 1999, 11, 367–372. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Huang, Y.Q.; Gou, R.; Diao, Y.S.; Yin, Q.H.; Fan, W.X.; Liang, Y.P.; Chen, Y.; Wu, M.; Zang, L.; Li, L.; et al. Charlson comorbidity index helps predict the risk of mortality for patients with type 2 diabetic nephropathy. J. Zhejiang Univ. Sci. B 2014, 15, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Liotta, G.; Ussai, S.; Illario, M.; O’Caoimh, R.; Cano, A.; Holland, C.; Roller-Winsberger, R.; Capanna, A.; Grecuccio, C.; Ferraro, M.; et al. Frailty as the Future Core Business of Public Health: Report of the Activities of the A3 Action Group of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). Int. J. Environ. Res. Public Health 2018, 15, 2843. [Google Scholar] [CrossRef] [Green Version]
- Mehrabi, F.; Béland, F. Frailty as a Moderator of the Relationship between Social Isolation and Health Outcomes in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 1675. [Google Scholar] [CrossRef]
- Zanasi, F.; De Santis, G.; Pirani, E. Lifelong Disadvantage and Late Adulthood Frailty. J. Ageing Longev. 2022, 2, 12–25. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Ornstein, K.A.; Leff, B.; Covinsky, K.E.; Ritchie, C.S.; Federman, A.D.; Roberts, L.; Kelley, A.S.; Siu, A.L.; Szanton, S.L. Epidemiology of the Homebound Population in the United States. JAMA Intern. Med. 2015, 175, 1180–1186. [Google Scholar] [CrossRef] [Green Version]
- Hellenic Statistical Authority. Statistics for the Greek Population and Social Conditions—Threshold Property. 2019. Available online: https://www.statistics.gr/en (accessed on 5 May 2022).
- Stolz, E.; Mayerl, H.; Waxenegger, A.; Freidl, W. Explaining the impact of poverty on old-age frailty in Europe: Material, psychosocial and behavioural factors. Eur. J. Public Health 2017, 27, 1003–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niederstrasser, N.G.; Rogers, N.T.; Bandelow, S. Determinants of frailty development and progression using a multidimensional frailty index: Evidence from the English Longitudinal Study of Ageing. PLoS ONE 2019, 14, e0223799. [Google Scholar] [CrossRef] [PubMed]
- Farías-Antúnez, S.; Fassa, A.G. Frailty prevalence and associated factors in the elderly in Southern Brazil, 2014. Epidemiol. Serv. Saude 2019, 28, e2017405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carneiro, J.A.; Cardoso, R.R.; Durães, M.S.; Guedes, M.C.A.; Santos, F.L.; Costa, F.M.D.; Caldeira, A.P. Frailty in the elderly: Prevalence and associated factors. Rev. Bras. Enferm. 2017, 70, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Oyon, J.; Serra-Prat, M.; Ferrer, M.; Llinares, A.; Pastor, N.; Limón, E.; Rejón, T.; Ramírez, S.; Salietti, A. Psychosocial factors associated with frailty in the community-dwelling aged population with depression. A cross-sectional study. Aten. Primaria 2021, 53, 102048. [Google Scholar] [CrossRef]
- Zhang, S.M.; Tang, X.D.; Yang, X.R.; Zheng, R.R.; Xu, L.; Wu, J.H. [Relationship between frailty and depression in elderly patients]. Zhonghua Yi Xue Za Zhi 2017, 97, 3384–3387. [Google Scholar] [CrossRef]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.T.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, T.J.; Chang, H.Y.; Wu, I.C.; Chen, C.C.; Tsai, H.J.; Chiu, Y.F.; Chuang, S.C.; Hsiung, C.A.; Hsu, C.C. Independent association between subjective cognitive decline and frailty in the elderly. PLoS ONE 2018, 13, e0201351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, O.; Duarte, N.; Teixeira, L.; Paul, C. Frailty and depression in centenarians. Int. Psychogeriatr. 2018, 30, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Narayan, M.; Farris, C.; Harris, M.D.; Hiong, F.Y. Development of the International Guidelines for Home Health Nursing. Home Healthc. Now 2017, 35, 494–506. [Google Scholar] [CrossRef] [PubMed]
- Gardner, B.; Jovicic, A.; Belk, C.; Kharicha, K.; Iliffe, S.; Manthorpe, J.; Goodman, C.; Drennan, V.M.; Walters, K. Specifying the content of home-based health behaviour change interventions for older people with frailty or at risk of frailty: An exploratory systematic review. BMJ Open 2017, 7, e014127. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mean ± SD, Median (IQR) | ||
|---|---|---|
| Age (years) | 78.45 ± 7.87, 79.00 (11.00) | |
| N | % | |
| Gender | ||
| Male | 111 | 36.9 |
| Female | 190 | 63.1 |
| Annual individual Income | ||
| ≤4500 | 133 | 45.4 |
| >4500 | 160 | 54.6 |
| Educational Level | ||
| * Uneducated | 245 | 81.4 |
| Highschool | 36 | 12.0 |
| Bachelor/MSc/PhD | 20 | 6.6 |
| Cognitive function a | ||
| Dysfunction (MoCA < 26) | 253 | 87.8 |
| Normal (MoCA ≥ 26) | 35 | 12.2 |
| Frailty status | ||
| Frail | 110 | 38.5 |
| Pre-frail | 130 | 45.5 |
| Non-frail | 46 | 16 |
| Depression | ||
| Severe (GDS 11+) | 41 | 13.6 |
| Mild (GDS 6–10) | 106 | 35.2 |
| Normal (GDS 0–5) | 154 | 51.2 |
| Comorbidity b | ||
| Severe (CCI ≥ 5) | 207 | 70.6 |
| Mild (CCI 2–4) | 86 | 29.4 |
| Normal (CCI 0–1) | 0 | 0 |
| Disability in ADL c | ||
| Dependent (Barthel ≤ 10) | 21 | 7.2 |
| Semi-dependent (Barthel 11–14) | 25 | 8.5 |
| Independent (Barthel 15+) | 247 | 84.3 |
| Homebound status d | ||
| Homebound | 54 | 18.1 |
| Semi-homebound | 48 | 16.1 |
| Non-homebound | 196 | 65.8 |
| Total | Females n (%) | Males n (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| Frailty Status | Frailty Status | |||||||
| n | % | Non-Frail | Pre-Frail | Frail | Non-Frail | Pre-Frail | Frail | |
| Frailty | 286 | 100 | 18(6.3) | 85(29.7) | 79(27.6) | 28(9.8) | 45(15.7) | 31(10.8) |
| Cognitive Function a | ||||||||
| Dysfunction (MoCA < 26) | 242 | 88 | 13(4.7) | 74(26.9) | 70(25.5) | 16(5.8) | 41(14.9) | 28(10.2) |
| Normal (MoCA ≥ 26) | 33 | 12 | 4(1.5) | 10(3.6) | 4(1.5) | 11(4) | 2(0.7) | 2(0.7) |
| Age | ||||||||
| ≤65–79 | 153 | 53.5 | 13(4.6) | 51(17.8) | 40(14) | 18(6.3) | 21(7.3) | 10(3.5) |
| ≥80 | 133 | 46.5 | 5(1.8) | 34(11.9) | 39(13.6) | 10(3.5) | 24(8.4) | 21(7.3) |
| Depression | ||||||||
| Severe (GDS 11+) | 41 | 14.3 | 0(0) | 12(4.2) | 19(6.6) | 1(0.3) | 3(1.1) | 6(2.1) |
| Mild (GDS 6–10) | 96 | 33.6 | 5(1.7) | 24(8.4) | 34(11.9) | 6(2.1) | 13(4.6) | 14(4.9) |
| Normal (GDS 0–5) | 149 | 52.1 | 13(4.6) | 49(17.1) | 26(9.1) | 21(7.3) | 29(10.1) | 11(3.9) |
| Comorbidity b | ||||||||
| Severe (CCI ≥ 5) | 201 | 70.3 | 10(3.5) | 59(20.7) | 57(19.9) | 18(6.3) | 32(11.2) | 25(8.7) |
| Mild (CCI 2–4) | 85 | 29.7 | 8(2.8) | 26(9.1) | 22(7.7) | 10(3.5) | 13(4.5) | 6(2.1) |
| Normal (CCI 0–1) | 0 | 0.0 | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) |
| Disability in ADL c | ||||||||
| Dependent (Barthel ≤ 10) | 19 | 6.7 | 0(0) | 5(1.8) | 13(4.5) | 0(0) | 0(0) | 1(0.4) |
| Semi-dependent (Barthel 11–14) | 25 | 8.7 | 0(0) | 6(2) | 11(3.8) | 0(0) | 3(1.1) | 5(1.8) |
| Independent (Barthel 15+) | 242 | 84.6 | 18(6.3) | 74(25.9) | 55(19.2) | 28(9.8) | 42(14.7) | 25(8.7) |
| Homebound Status d | ||||||||
| Homebound | 51 | 18 | 0(0) | 14(4.9) | 30(10.6) | 0(0) | 3(1.1) | 4(1.4) |
| Semi-Homebound | 42 | 14.9 | 0(0) | 9(3.2) | 19(6.7) | 1(0.4) | 3(1.1) | 10(3.5) |
| Non-Homebound | 190 | 67.1 | 17(6) | 62(21.9) | 30(10.6) | 27(9.5) | 37(13.1) | 17(6) |
| Annual individual Income | ||||||||
| ≤4500 | 125 | 44.6 | 8(2.9) | 30(10.7) | 42(15) | 5(1.8) | 20(7.1) | 20(7.1) |
| >4500 | 155 | 55.4 | 9(3.2) | 53(19) | 36(12.9) | 23(8.2) | 25(8.9) | 9(3.2) |
| Educational Level | ||||||||
| * Uneducated | 230 | 80.4 | 14(4.9) | 70(24.5) | 66(23) | 18(6.3) | 32(11.2) | 30(10.5) |
| Highschool | 36 | 12.6 | 3(1.1) | 10(3.5) | 8(2.8) | 7(2.4) | 8(2.8) | 0(0) |
| Bachelor/MSc/PhD | 20 | 7 | 1(0.4) | 5(1.7) | 5(1.7) | 3(1.1) | 5(1.7) | 1(0.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aravantinou-Karlatou, A.; Kavasileiadou, S.; Panagiotakis, S.; Tziraki, C.; Almegewly, W.; Androulakis, E.; Kleisiaris, C. The Impact of Socioeconomic Factors and Geriatric Syndromes on Frailty among Elderly People Receiving Home-Based Healthcare: A Cross-Sectional Study. Healthcare 2022, 10, 2079. https://doi.org/10.3390/healthcare10102079
Aravantinou-Karlatou A, Kavasileiadou S, Panagiotakis S, Tziraki C, Almegewly W, Androulakis E, Kleisiaris C. The Impact of Socioeconomic Factors and Geriatric Syndromes on Frailty among Elderly People Receiving Home-Based Healthcare: A Cross-Sectional Study. Healthcare. 2022; 10(10):2079. https://doi.org/10.3390/healthcare10102079
Chicago/Turabian StyleAravantinou-Karlatou, Antonia, Savvato Kavasileiadou, Simeon Panagiotakis, Chariklia Tziraki, Wafa Almegewly, Emmanouil Androulakis, and Christos Kleisiaris. 2022. "The Impact of Socioeconomic Factors and Geriatric Syndromes on Frailty among Elderly People Receiving Home-Based Healthcare: A Cross-Sectional Study" Healthcare 10, no. 10: 2079. https://doi.org/10.3390/healthcare10102079