

Association of the Inferior Alveolar Nerve Position and Nerve Injury: A Systematic Review and Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Primary Outcomes
2.3. Electronic Searches
2.4. Searching Other Resources
- We searched references in included articles to serve as a supplement.
- We contacted authors by e-mail regarding unclear data.
2.5. Selection of Studies
2.6. Data Extraction and Management
2.7. Measures of Treatment Effect and Heterogeneity
2.8. Subgroup and Sensitivity Analysis
3. Results
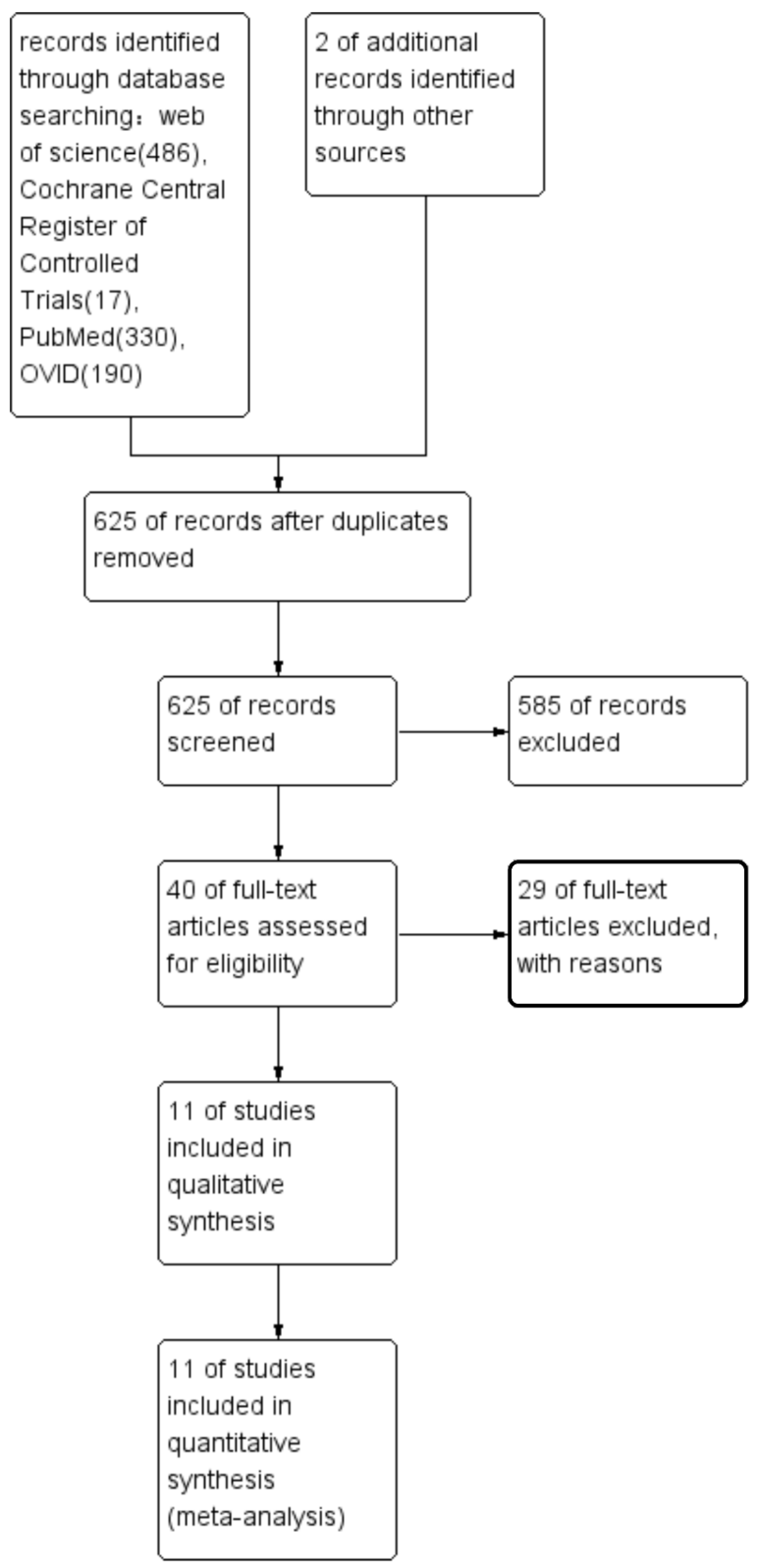
3.1. Study Selection
3.2. Study Characteristics
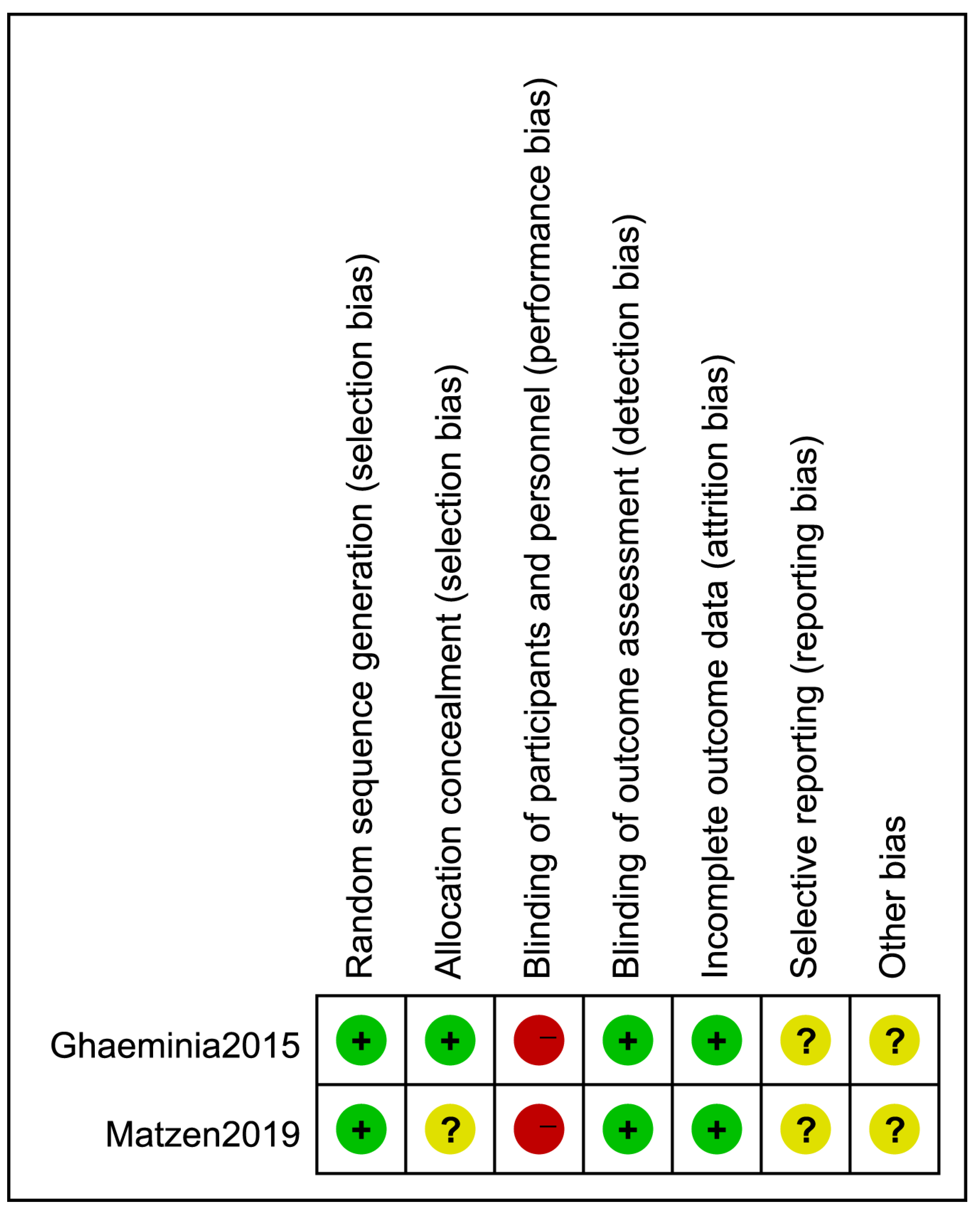
3.3. Quality Assessment
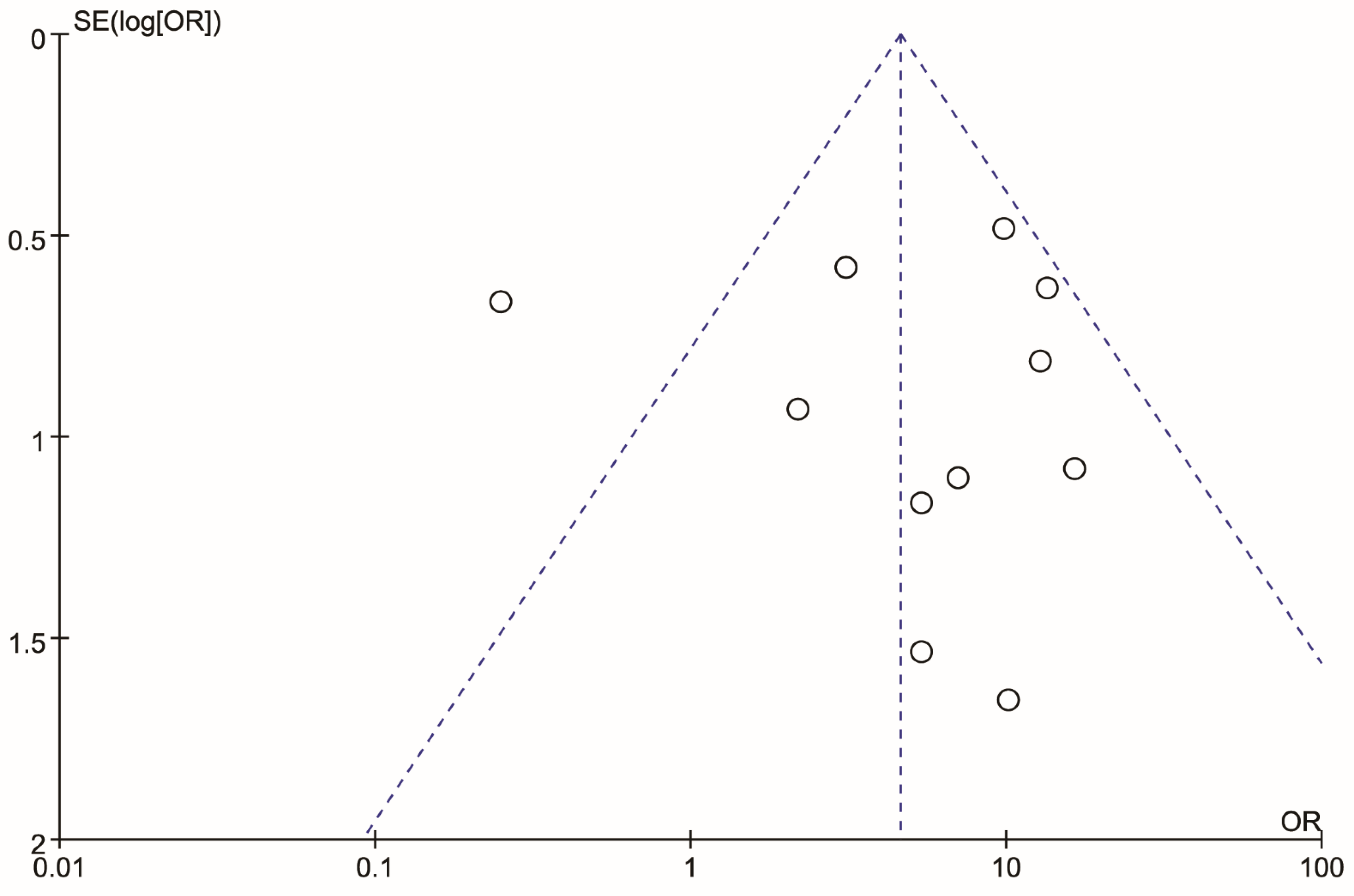
3.4. Risk of Bias in Included Studies
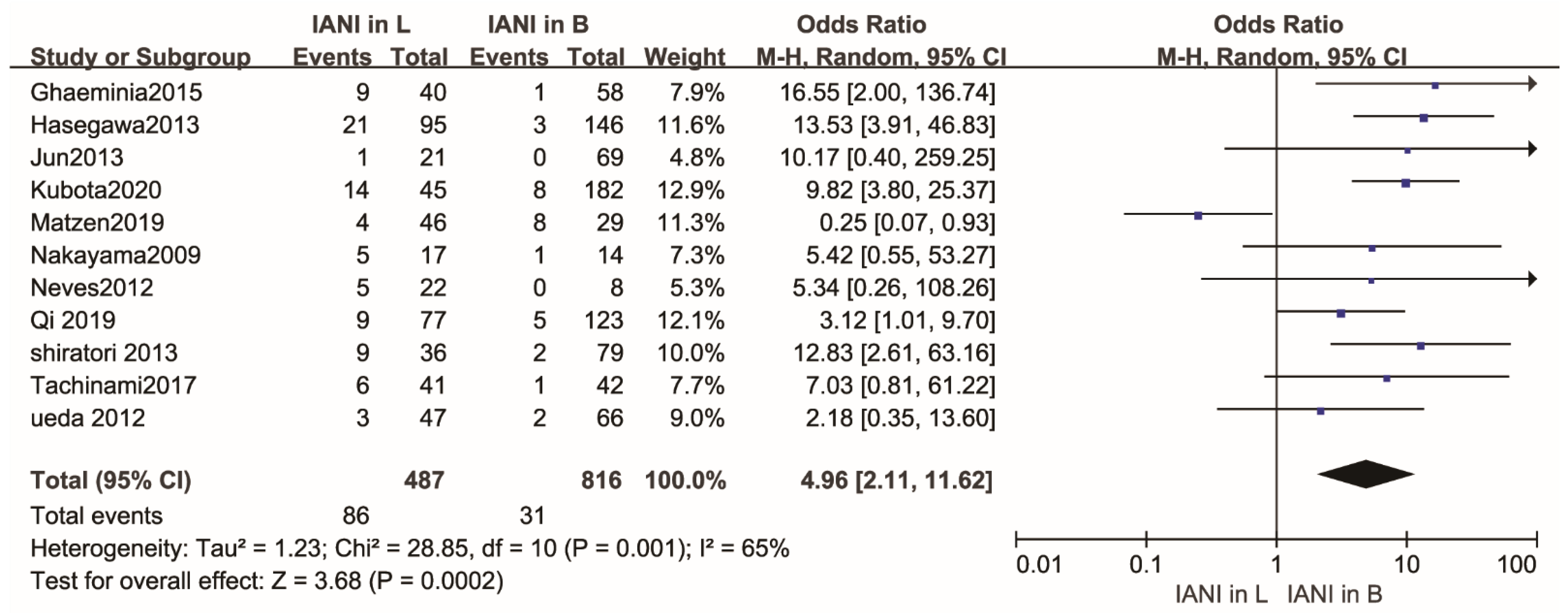
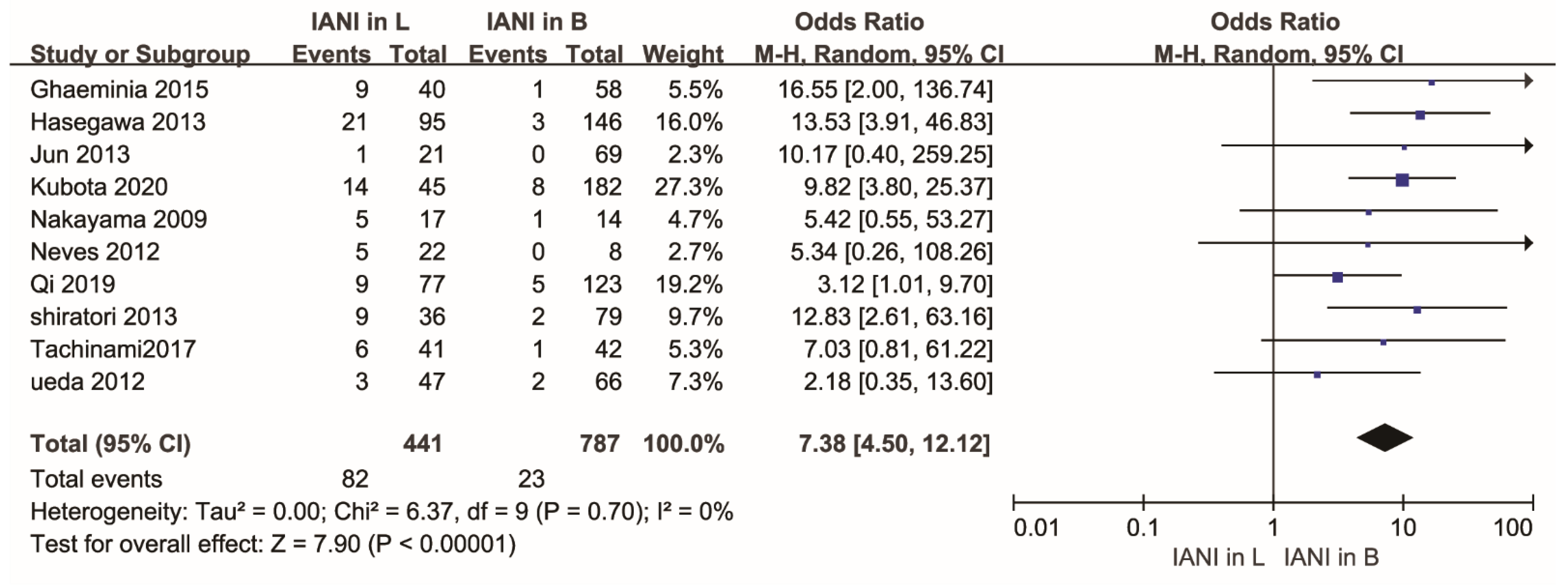
3.5. Quantitative Synthesis
3.6. Data Analysis
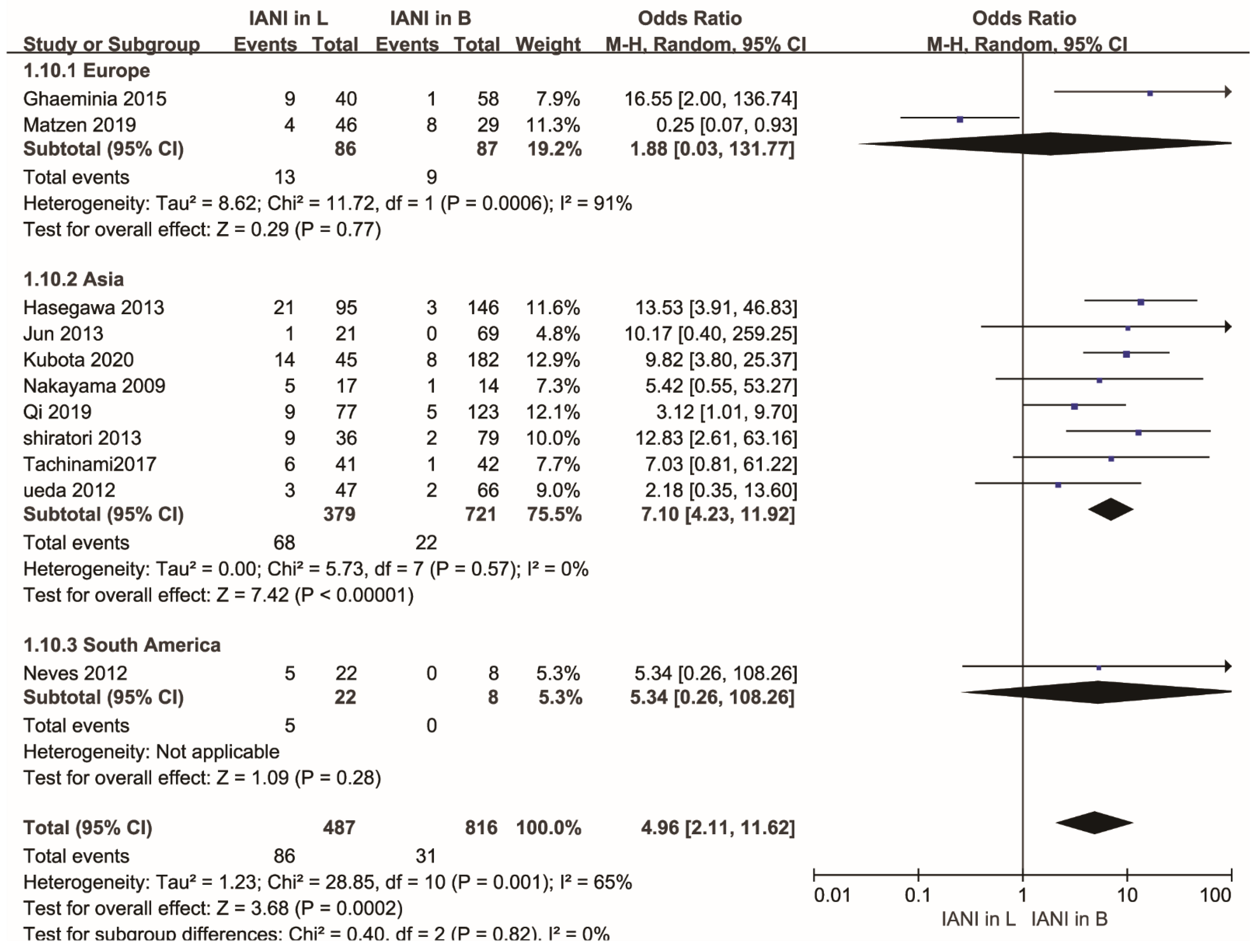
3.7. Subgroup Analysis
3.8. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gu, L.; Zhu, C.; Chen, K.; Liu, X.; Tang, Z. Anatomic study of the position of the mandibular canal and corresponding mandibular third molar on cone-beam computed tomography images. Surg. Radiol. Anat. 2018, 40, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.K.; Leung, Y.Y.; Chow, L.K.; Wong, M.C.; Chan, E.K.; Fok, Y.H. Incidence of neurosensory deficits and recovery after lower third molar surgery: A prospective clinical study of 4338 cases. Int. J. Oral Maxillofac. Surg. 2010, 39, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, E.; Grubor, D.; Chandu, A. Risk factors for permanent injury of inferior alveolar and lingual nerves during third molar surgery. J. Oral Maxillofac. Surg. 2014, 72, 2394–2401. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.H.; Kim, C.H.; Ahn, J.S.; Padwa, B.L.; Kwon, J.J. Anatomical differences in lower third molars visualized by 2D and 3D X-ray imaging: Clinical outcomes after extraction. Int. J. Oral Maxillofac. Surg. 2013, 42, 489–496. [Google Scholar] [CrossRef]
- Blaeser, B.F.; August, M.A.; Donoff, R.B.; Kaban, L.B.; Dodson, T.B. Panoramic radiographic risk factors for inferior alveolar nerve injury after third molar extraction. J. Oral Maxillofac. Surg. 2003, 61, 417–421. [Google Scholar] [CrossRef]
- Lubbers, H.T.; Matthews, F.; Damerau, G.; Kruse, A.L.; Obwegeser, J.A.; Gratz, K.W. Anatomy of impacted lower third molars evaluated by computerized tomography: Is there an indication for 3-dimensional imaging? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 111, 547–550. [Google Scholar] [CrossRef]
- Tassoker, M. Diversion of the mandibular canal: Is it the best predictor of inferior alveolar nerve damage during mandibular third molar surgery on panoramic radiographs? Imaging Sci. Dent. 2019, 49, 213–218. [Google Scholar] [CrossRef]
- Ghaeminia, H.; Gerlach, N.L.; Hoppenreijs, T.J.; Kicken, M.; Dings, J.P.; Borstlap, W.A. Clinical relevance of cone beam computed tomography in mandibular third molar removal: A multicentre, randomised, controlled trial. J. Craniomaxillofac. Surg. 2015, 43, 2158–2167. [Google Scholar] [CrossRef]
- Hasegawa, T.; Ri, S.; Shigeta, T.; Akashi, M.; Imai, Y.; Kakei, Y. Risk factors associated with inferior alveolar nerve injury after extraction of the mandibular third molar—A comparative study of preoperative images by panoramic radiography and computed tomography. Int. J. Oral Maxillofac. Surg. 2013, 42, 843–851. [Google Scholar] [CrossRef]
- Zandi, M.; Shokri, A.; Heidari, A.; Masoud Peykar, E. Objectivity and reliability of panoramic radiographic signs of intimate relationship between impacted mandibular third molar and inferior alveolar nerve. Oral Maxillofac. Surg. 2015, 19, 43–48. [Google Scholar] [CrossRef]
- Qi, W.; Lei, J.; Liu, Y.N.; Li, J.N.; Pan, J.; Yu, G.Y. Evaluating the risk of post-extraction inferior alveolar nerve injury through the relative position of the lower third molar root and inferior alveolar canal. Int. J. Oral Maxillofac. Surg. 2019, 48, 1577–1583. [Google Scholar] [CrossRef]
- Ruga, E.; Gallesio, C.; Boffano, P. Mandibular alveolar neurovascular bundle injury associated with impacted third molar surgery. J. Maxillofac. Surg. 2010, 21, 1175–1177. [Google Scholar] [CrossRef] [PubMed]
- Baqain, Z.H.; Karaky, A.A.; Sawair, F.; Khraisat, A.; Duaibis, R.; Rajab, L.D. Frequency estimates and risk factors for postoperative morbidity after third molar removal: A prospective cohort study. J. Oral Maxillofac. Surg. 2008, 66, 2276–2283. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Han, M.D.; Jeon, K.J.; Huh, J.K.; Park, K.H. Three-dimensional assessment of the anterior and inferior loop of the inferior alveolar nerve using computed tomography images in patients with and without mandibular asymmetry. BMC Oral Health 2021, 21, 71. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, K.; Nonoyama, M.; Takaki, Y.; Kagawa, T.; Yuasa, K.; Izumi, K. Assessment of the relationship between impacted mandibular third molars and inferior alveolar nerve with dental 3-dimensional computed tomography. J. Oral Maxillofac. Surg. 2009, 67, 2587–2591. [Google Scholar] [CrossRef] [PubMed]
- Tachinami, H.; Tomihara, K.; Fujiwara, K.; Nakamori, K.; Noguchi, M. Combined preoperative measurement of three inferior alveolar canal factors using computed tomography predicts the risk of inferior alveolar nerve injury during lower third molar extraction. Int. J. Oral Maxillofac. Surg. 2017, 46, 1479–1483. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2019, 151, 264–269. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available online: www.training.cochrane.org/handbook (accessed on 12 August 2022).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. The Ottawa Hospital Research Institute, 2014. Available online: www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 August 2022).
- Ahmed, M.; Salah, M.K.; Khairy, N. Computer-Aided Design/Computer-Aided Manufacturing Cutting Guides for Odontectomy of Deeply Impacted Mandibular Third Molars. Open Access Maced. J. Med. Sci. 2018, 6, 2395–2401. [Google Scholar] [CrossRef]
- Al Ali, S.; Jaber, M. Correlation of panoramic high-risk markers with the cone beam CT findings in the preoperative assessment of the mandibular third molars. J. Dent. Sci. 2020, 15, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Barone, R.; Clauser, C.; Testori, T.; Del Fabbro, M. Self-assessed neurological disturbances after surgical removal of impacted lower third molar: A pragmatic prospective study on 423 surgical extractions in 247 consecutive patients. Clin. Oral Investig. 2019, 23, 3257–3265. [Google Scholar] [CrossRef]
- Bhat, P.; Cariappa, K.M. Inferior alveolar nerve deficits and recovery following surgical removal of impacted mandibular third molars. J. Maxillofac. Oral Surg. 2012, 11, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Bigagnoli, S.; Greco, C.; Costantinides, F.; Porrelli, D.; Bevilacqua, L.; Maglione, M. CBCT Radiological Features as Predictors of Nerve Injuries in Third Molar Extractions: Multicenter Prospective Study on a Northeastern Italian Population. Dent. J. 2021, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Boffano, P.; Roccia, F.; Gallesio, C.; Karagozoglu, K.; Forouzanfar, T. Inferior alveolar nerve injuries associated with mandibular fractures at risk: A two-center retrospective study. Craniomaxillofac. Trauma Reconstr. 2014, 7, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Burian, E.; Probst, F.A.; Weidlich, D.; Cornelius, C.P.; Maier, L.; Robl, T. MRI of the inferior alveolar nerve and lingual nerve-anatomical variation and morphometric benchmark values of nerve diameters in healthy subjects. Clin. Oral Investig. 2020, 24, 2625–2634. [Google Scholar] [CrossRef] [PubMed]
- Eyrich, G.; Seifert, B.; Matthews, F.; Matthiessen, U.; Heusser, C.K.; Kruse, A.L. 3-Dimensional imaging for lower third molars: Is there an implication for surgical removal? J. Oral Maxillofac. Surg. 2011, 69, 1867–1872. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.C.; Vasconcelos, B.C.; Silva, E.D.; Caldas Ade, F., Jr.; Pita Neto, I.C. Sensitivity and specificity of pantomography to predict inferior alveolar nerve damage during extraction of impacted lower third molars. J. Oral Maxillofac. Surg. 2008, 66, 256–259. [Google Scholar] [CrossRef]
- Guerrero, M.E.; Nackaerts, O.; Beinsberger, J.; Horner, K.; Schoenaers, J.; Jacobs, R. Inferior alveolar nerve sensory disturbance after impacted mandibular third molar evaluation using cone beam computed tomography and panoramic radiography: A pilot study. J. Oral Maxillofac. Surg. 2012, 70, 2264–2270. [Google Scholar] [CrossRef]
- Hasani, A.; Ahmadi Moshtaghin, F.; Roohi, P.; Rakhshan, V. Diagnostic value of cone beam computed tomography and panoramic radiography in predicting mandibular nerve exposure during third molar surgery. Int. J. Oral Maxillofac. Surg. 2017, 46, 230–235. [Google Scholar] [CrossRef]
- Hassani, A.; Rakhshan, V.; Hassani, M.; Aghdam, H.M. Preoperative imaging of the inferior alveolar nerve canal by cone-beam computed tomography and 1-year neurosensory recovery following mandibular setback through bilateral sagittal split ramus osteotomy: A randomized clinical trial. J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 41–48. [Google Scholar] [CrossRef]
- Huang, C.K.; Lui, M.T.; Cheng, D.H. Use of panoramic radiography to predict postsurgical sensory impairment following extraction of impacted mandibular third molars. J. Chin. Med. Assoc. 2015, 78, 617–622. [Google Scholar] [CrossRef] [Green Version]
- Iwanaga, J.; Altafulla, J.J.; Kikuta, S.; Tubbs, R.S. An Anatomical Feasibility Study Using a Great Auricular Nerve Graft for Ipsilateral Inferior Alveolar Nerve Repair. J. Maxillofac. Surg. 2019, 30, 2625–2627. [Google Scholar] [CrossRef] [PubMed]
- Janovics, K.; Soos, B.; Toth, A.; Szalma, J. Is it possible to filter third molar cases with panoramic radiography in which roots surround the inferior alveolar canal? A comparison using cone-beam computed tomography. J. Craniomaxillofac. Surg. 2021, 49, 971–979. [Google Scholar] [CrossRef]
- Jhamb, A.; Dolas, R.S.; Pandilwar, P.K.; Mohanty, S. Comparative efficacy of spiral computed tomography and orthopantomography in preoperative detection of relation of inferior alveolar neurovascular bundle to the impacted mandibular third molar. J. Oral Maxillofac. Surg. 2009, 67, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Kang, F.; Xue, Z.; Zhou, X.; Zhang, X.; Hou, G.; Feng, Y. Coronectomy: A Useful Approach in Minimizing Nerve Injury Compared With Traditional Extraction of Deeply Impacted Mandibular Third Molars. J. Oral Maxillofac. Surg. 2019, 77, 2221.e1–2221.e14. [Google Scholar] [CrossRef]
- Khan, I.; Halli, R.; Gadre, P.; Gadre, K.S. Correlation of panoramic radiographs and spiral CT scan in the preoperative assessment of intimacy of the inferior alveolar canal to impacted mandibular third molars. J. Maxillofac. Surg. 2011, 22, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Cha, I.H.; Kim, S.J.; Kim, M.R. Which risk factors are associated with neurosensory deficits of inferior alveolar nerve after mandibular third molar extraction? J. Oral Maxillofac. Surg. 2012, 70, 2508–2514. [Google Scholar] [CrossRef]
- Korkmaz, Y.T.; Kayipmaz, S.; Senel, F.C.; Atasoy, K.T.; Gumrukcu, Z. Does additional cone beam computed tomography decrease the risk of inferior alveolar nerve injury in high-risk cases undergoing third molar surgery?Does CBCT decrease the risk of IAN injury? Int. J. Oral Maxillofac. Surg. 2017, 46, 628–635. [Google Scholar] [CrossRef]
- Kubota, S.; Imai, T.; Nakazawa, M.; Uzawa, N. Risk stratification against inferior alveolar nerve injury after lower third molar extraction by scoring on cone-beam computed tomography image. Odontology 2020, 108, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Maglione, M.; Costantinides, F.; Bazzocchi, G. Classification of impacted mandibular third molars on cone-beam CT images. J. Clin. Exp. Dent. 2015, 7, e224. [Google Scholar] [CrossRef]
- Matzen, L.H.; Petersen, L.B.; Schropp, L.; Wenzel, A. Mandibular canal-related parameters interpreted in panoramic images and CBCT of mandibular third molars as risk factors to predict sensory disturbances of the inferior alveolar nerve. Int. J. Oral Maxillofac. Surg. 2019, 48, 1094–1101. [Google Scholar] [CrossRef]
- Nakamori, K.; Fujiwara, K.; Miyazaki, A.; Tomihara, K.; Tsuji, M.; Nakai, M. Clinical assessment of the relationship between the third molar and the inferior alveolar canal using panoramic images and computed tomography. J. Oral Maxillofac. Surg. 2008, 66, 2308–2313. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, A.; Fukuta, Y.; Nakasato, H.; Nakasato, S. Evaluation by dental cone-beam computed tomography of the incidence and sites of branches of the inferior dental canal that supply mandibular third molars. Br. J. Oral Maxillofac. Surg. 2016, 54, 1116–1120. [Google Scholar] [CrossRef] [PubMed]
- Padhye, N.M.; Shirsekar, V.U.; Bhatavadekar, N.B. Three-Dimensional Alveolar Bone Assessment of Mandibular First Molars with Implications for Immediate Implant Placement. Int. J. Periodontics Restor. Dent. 2020, 40, e163–e167. [Google Scholar] [CrossRef] [PubMed]
- Neves, F.S.; de Almeida, S.M.; Boscolo, F.N.; Haiter-Neto, F.; Alves, M.C.; Crusoe-Rebello, I. Risk assessment of inferior alveolar neurovascular bundle by multidetector computed tomography in extractions of third molars. Surg. Radiol. Anat. 2012, 34, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Ueda, M.; Nakamori, K.; Shiratori, K.; Igarashi, T.; Sasaki, T.; Anbo, N. Clinical significance of computed tomographic assessment and anatomic features of the inferior alveolar canal as risk factors for injury of the inferior alveolar nerve at third molar surgery. J. Oral Maxillofac. Surg. 2012, 70, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Shiratori, K.; Nakamori, K.; Ueda, M.; Sonoda, T.; Dehari, H. Assessment of the shape of the inferior alveolar canal as a marker for increased risk of injury to the inferior alveolar nerve at third molar surgery: A prospective study. J. Oral Maxillofac. Surg. 2013, 71, 2012–2019. [Google Scholar] [CrossRef]
- Kikuta, S.; Iwanaga, J.; Kusukawa, J.; Tubbs, R.S. An anatomical study of the lingual nerve in the lower third molar area. Anat. Cell Biol. 2019, 52, 140–142. [Google Scholar] [CrossRef]
- Leung, Y.Y. Management and prevention of third molar surgery-related trigeminal nerve injury: Time for a rethink. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 233–240. [Google Scholar] [CrossRef]
- Tojyo, I.; Nakanishi, T.; Shintani, Y.; Okamoto, K.; Hiraishi, Y.; Fujita, S. Risk of lingual nerve injuries in removal of mandibular third molars: A retrospective case-control study. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 40. [Google Scholar] [CrossRef]
- Omran, A.; Hutchison, I.; Ridout, F.; Bose, A.; Maroni, R.; Dhanda, J. Current perspectives on the surgical management of mandibular third molars in the United Kingdom: The need for further research. Br. J. Oral Maxillofac. Surg. 2020, 58, 348–354. [Google Scholar] [CrossRef]
- Laher, A.E.; Motara, F.; Moolla, M. The Ultrasonographic Determination of the Position of the Mental Foramen and its Relation to the Mandibular Premolar Teeth. J. Clin. Diagn Res. 2016, 10, OC23–OC27. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yin, W.; Zhang, R.; Li, J.; Zheng, Y. Diagnostic value of panoramic radiography in predicting inferior alveolar nerve injury after mandibular third molar extraction: A meta-analysis. Aust. Dent. J. 2015, 60, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Cle-Ovejero, A.; Sanchez-Torres, A.; Camps-Font, O.; Gay-Escoda, C.; Figueiredo, R.; Valmaseda-Castellon, E. Does 3-dimensional imaging of the third molar reduce the risk of experiencing inferior alveolar nerve injury owing to extraction?: A meta-analysis. J. Am. Dent. Assoc. 2017, 148, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, Y.B.R.; Beltrami, R.; Tagliabo, A.; Rizzo, S.; Lupi, S.M. Differences between panoramic and Cone Beam-CT in the surgical evaluation of lower third molars. J. Clin. Exp. Dent. 2017, 9, e259. [Google Scholar]
- Del Lhano, N.C.; Ribeiro, R.A.; Martins, C.C.; Assis, N.; Devito, K.L. Panoramic versus CBCT used to reduce inferior alveolar nerve paresthesia after third molar extractions: A systematic review and meta-analysis. Dentomaxillofac. Radiol. 2020, 49, 20190265. [Google Scholar] [CrossRef]
- Lupi, S.M.; Landini, J.; Olivieri, G.; Todaro, C.; Scribante, A.; Rodriguez y Baena, R. Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT. Healthcare 2021, 9, 1747. [Google Scholar] [CrossRef]
- Monaco, G.; Montevecchi, M.; Bonetti, G.A.; Gatto, M.R.; Checchi, L. Reliability of panoramic radiography in evaluating the topographic relationship between the mandibular canal and impacted third molars. J. Am. Dent. Assoc. 2004, 135, 312–318. [Google Scholar] [CrossRef]
- Bozkurt, P.; Gorurgoz, C. Detecting direct inferior alveolar nerve—Third molar contact and canal decorticalization by cone-beam computed tomography to predict postoperative sensory impairment. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 259–263. [Google Scholar] [CrossRef]
- Maegawa, H.; Sano, K.; Kitagawa, Y.; Ogasawara, T.; Miyauchi, K.; Sekine, J. Preoperative assessment of the relationship between the mandibular third molar and the mandibular canal by axial computed tomography with coronal and sagittal reconstruction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 639–646. [Google Scholar] [CrossRef]
- Sedaghatfar, M.; August, M.A.; Dodson, T.B. Panoramic radiographic findings as predictors of inferior alveolar nerve exposure following third molar extraction. J. Oral Maxillofac. Surg. 2005, 63, 3–7. [Google Scholar] [CrossRef]
- Valmaseda-Castellon, E.; Berini-Aytes, L.; Gay-Escoda, C. Inferior alveolar nerve damage after lower third molar surgical extraction: A prospective study of 1117 surgical extractions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Jiang, E.; Shang, Z. 3D Co-culture of Cancer-Associated Fibroblast with Oral Cancer Organoids. J. Dent. Res. 2021, 100, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.Z.; Yang, C.; Fan, X.D.; Yu, C.Q.; Cai, X.Y.; Wang, Y. Anatomic relationship between impacted third mandibular molar and the mandibular canal as the risk factor of inferior alveolar nerve injury. Br. J. Oral Maxillofac. Surg. 2013, 51, e215–e219. [Google Scholar] [CrossRef] [PubMed]
- Kumar Potu, B.; Jagadeesan, S.; Mr Bhat, K.; Rao Sirasanagandla, S. Retromolar foramen and canal: A comprehensive review on its anatomy and clinical applications. Morphologie 2013, 97, 31–37. [Google Scholar] [CrossRef]
- von Arx, T.; Hanni, A.; Sendi, P.; Buser, D.; Bornstein, M.M. Radiographic study of the mandibular retromolar canal: An anatomic structure with clinical importance. J. Endodontol. 2011, 37, 1630–1635. [Google Scholar] [CrossRef]
- Agbaje, J.O.; Heijsters, G.; Salem, A.S.; Van Slycke, S.; Schepers, S.; Politis, C. Coronectomy of Deeply Impacted Lower Third Molar: Incidence of Outcomes and Complications after One Year Follow-Up. J. Oral Maxillofac. Res. 2015, 6, e1. [Google Scholar] [CrossRef]
- Szalma, J.; Lempel, E. [Protecting the inferior alveolar nerve: Coronectomy of lower third molars. Rev. Orv. Hetil. 2017, 158, 1787–1793. [Google Scholar] [CrossRef]
- Goto, S.; Kurita, K.; Kuroiwa, Y.; Hatano, Y.; Kohara, K.; Izumi, M. Clinical and dental computed tomographic evaluation 1 year after coronectomy. J. Oral Maxillofac. Surg. 2012, 70, 1023–1029. [Google Scholar] [CrossRef]
- Alessandri Bonetti, G.; Bendandi, M.; Laino, L.; Checchi, V.; Checchi, L. Orthodontic extraction: Riskless extraction of impacted lower third molars close to the mandibular canal. J. Oral Maxillofac. Surg. 2007, 65, 2580–2586. [Google Scholar] [CrossRef]
- Wang, Y.; He, D.; Yang, C.; Wang, B.; Qian, W. An easy way to apply orthodontic extraction for impacted lower third molar compressing to the inferior alveolar nerve. J. Craniomaxillofac. Surg. 2012, 40, 234–237. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors’ Names | Year | Relative Countries | IANI in L | Sample Size in L | IANI in B | Sample Size in B | Study Design | Age (Years) | Number of P | Follow-Up Time |
|---|---|---|---|---|---|---|---|---|---|---|
| Ghaeminia | 2015 | Netherlands | 9 | 40 | 1 | 58 | an RCT | NM | 5 | 18 months |
| Hasegawa | 2013 | Japan | 21 | 95 | 3 | 146 | a retrospective cohort study | 16–71, A36.2 | NM | 6 months |
| Jun | 2013 | South Korea | 1 | 21 | 0 | 69 | a retrospective cohort study | 17–43, A23.9 | NM | 7 days |
| Kubota | 2020 | Japan | 14 | 45 | 8 | 182 | a retrospective case–control study | 23–55, A39 | NM | 7 days |
| Nakayama | 2009 | Japan | 5 | 17 | 1 | 14 | a retrospective cohort study | 18–56, A39.2 | NM | 7 days |
| Neves | 2012 | Brazil | 5 | 22 | 0 | 8 | a retrospective cohort study | 16–55, A26.4 | NM | 7 days |
| Tachinami | 2017 | Japan | 6 | 41 | 1 | 42 | a retrospective cohort study | 17–90, A31.46 | NM | NM |
| Matzen | 2019 | Denmark | 4 | 46 | 8 | 29 | an RCT | 19–56, A29 | 1 | 6 months |
| Qi | 2019 | China | 9 | 77 | 5 | 123 | a retrospective cohort study | NM | NM | >5 months |
| Ueda | 2012 | Japan | 3 | 47 | 2 | 66 | a retrospective cohort study | 16–74, A31.8 | NM | NM |
| Shiratori | 2013 | Japan | 9 | 36 | 2 | 79 | a prospective cohort study | 18–71, 32.5 | NM | >12 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Ling, Z.; Zhang, H.; Xie, H.; Zhang, P.; Jiang, H.; Fu, Y. Association of the Inferior Alveolar Nerve Position and Nerve Injury: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 1782. https://doi.org/10.3390/healthcare10091782
Li Y, Ling Z, Zhang H, Xie H, Zhang P, Jiang H, Fu Y. Association of the Inferior Alveolar Nerve Position and Nerve Injury: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(9):1782. https://doi.org/10.3390/healthcare10091782
Chicago/Turabian StyleLi, Yangjie, Ziji Ling, Hang Zhang, Hanyu Xie, Ping Zhang, Hongbing Jiang, and Yu Fu. 2022. "Association of the Inferior Alveolar Nerve Position and Nerve Injury: A Systematic Review and Meta-Analysis" Healthcare 10, no. 9: 1782. https://doi.org/10.3390/healthcare10091782