
Effects of Changes in Multiple Chronic Conditions on Medical Costs among Older Adults in South Korea


Abstract
:1. Introduction
2. Materials and Methods
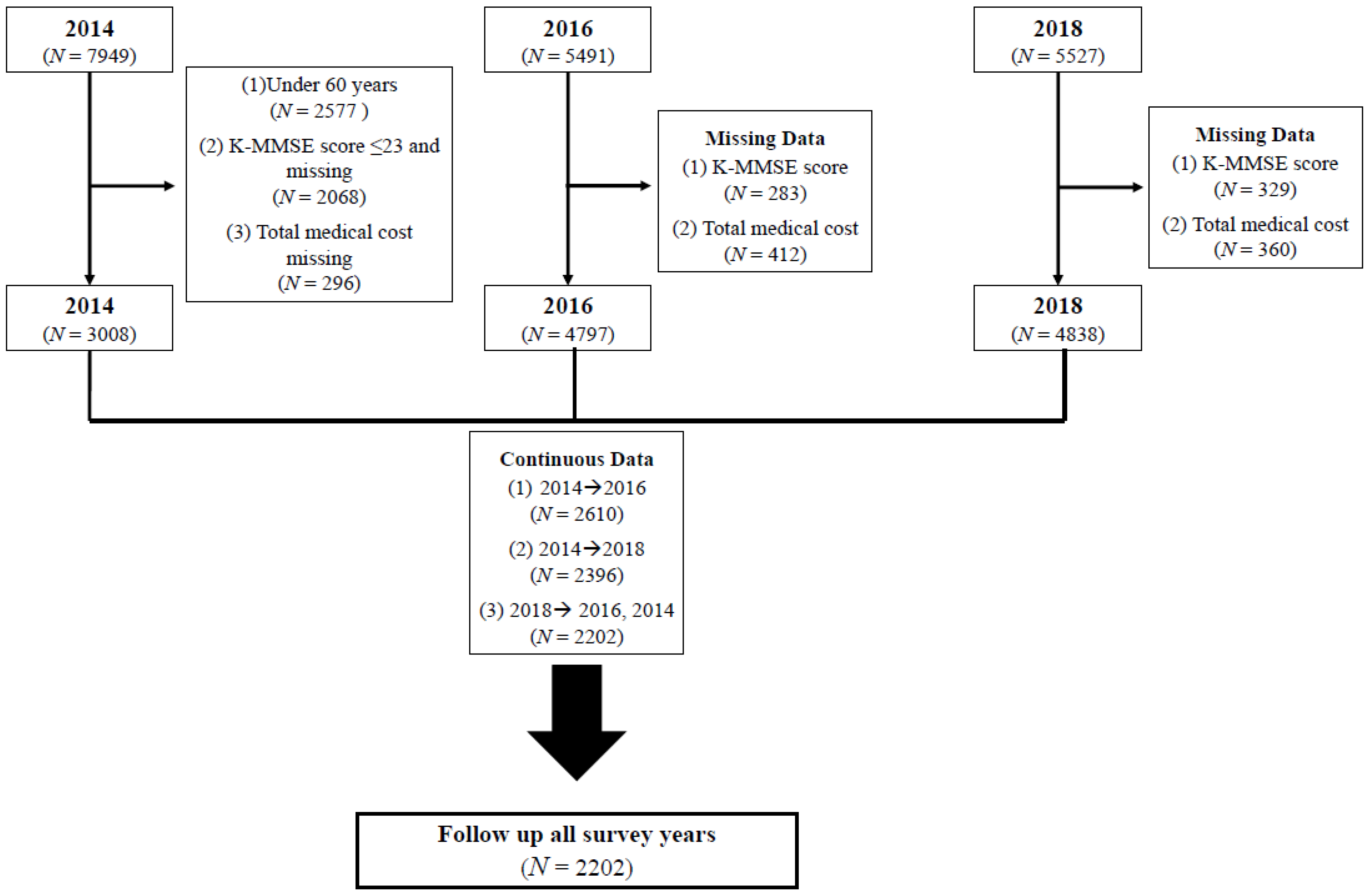
2.1. Study Participants and Database Information
2.2. Medical Cost
2.3. Changes in MCCs
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jakovljevic, M.; Liu, Y.; Cerda, A.; Simonyan, M.; Correia, T.; Mariita, R.M.; Kumara, A.S.; Garcia, L.; Krstic, K.; Osabohien, R. The Global South political economy of health financing and spending landscape-history and presence. J. Med. Econ. 2021, 24, 25–33. [Google Scholar] [CrossRef] [PubMed]
- De Lima, J.D.; Teixeira, I.A.; de Oliveira Silva, F.; Deslandes, A.C. The comorbidity conditions and polypharmacy in elderly patients with mental illness in a middle income country: A cross-sectional study⋆. IBRO Rep. 2020, 9, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Bloom, D.E.; Chisholm, D.; Jané-Llopis, E.; Prettner, K.; Stein, A.; Feigl, A. From Burden to “Best Buys”: Reducing the Economic Impact of Non-communicable Diseases. Program on the Global Demography of Aging. Available online: https://ideas.repec.org/p/gdm/wpaper/7511.html (accessed on 1 January 2022).
- Hopman, P.; Heins, M.J.; Korevaar, J.C.; Rijken, M.; Schellevis, F.G. Health care utilization of patients with multiple chronic diseases in the Netherlands: Differences and underlying factors. Eur. J. Intern. Med. 2016, 35, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.H. Analysis of multiple chronic conditions in older adults: Focusing on outpatient use. Korea Institute for Health and Social Affairs. Issue Focus 2013, 196, 1–8. [Google Scholar]
- Park, E.J.; Bae, J.E.; Song, E.S.; Jung, Y.; Choi, S.G.; Lee, E.J.; Kim, E.J.; Yeom, A.R.; Yoon, Y.M.; Kim, G.S.; et al. 2018 Korea Medical Panel Basic Analysis Report (II.)-Disease Morbidity, Chronic Diseases, Health Behaviors and Health Levels. Korea Institute of Health and Social Research. Available online: http://repository.kihasa.re/kr/handle/201002/37343 (accessed on 5 April 2021).
- Klompstra, L.; Ekdahl, A.W.; Krevers, B.; Milberg, A.; Eckerblad, J. Factors related to health-related quality of life in older people with multimorbidity and high health care consumption over a two-year period. BMC Geriatr. 2019, 19, 187. [Google Scholar] [CrossRef]
- Lee, Y.; Cho, C.C. Examining the effect of multiple chronic condition on cognitive decline and potential moderators among older Koreans: Findings from the Korean Longitudinal Study of Ageing 2006–2016. Arch. Gerontol. Geriatr. 2021, 95, 104424. [Google Scholar] [CrossRef]
- Van Oostrom, S.H.; Picavet, H.S.J.; De Bruin, S.R.; Stirbu, I.; Korevaar, J.C.; Schellevis, F.G.; Baan, C.A. Multimorbidity of chronic diseases and health care utilization in general practice. BMC Fam. Pract. 2014, 15, 61. [Google Scholar] [CrossRef] [Green Version]
- Bähler, C.; Huber, C.A.; Brüngger, B.; Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: A claims data based observational study. BMC Health Serv. Res. 2015, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Cho, Y.; Oh, H. Multiple chronic conditions and risk of cognitive impairment and dementia among older Americans: Findings from the Aging, Demographics, and Memory Study (ADAMS). Aging Neuropsychol. Cogn. 2020, 28, 493–507. [Google Scholar] [CrossRef]
- Leibson, C.L.; Long, K.H.; Ransom, J.E.; Roberts, R.O.; Hass, S.L.; Duhig, A.M.; Smith, C.Y.; Emerson, J.A.; Pankratz, V.S.; Petersen, R.C. Direct medical costs and source of cost differences across the spectrum of cognitive decline: A population-based study. Alzheimer's Dement. 2015, 11, 917–932. [Google Scholar] [CrossRef] [Green Version]
- Michalowsky, B.; Eichler, T.; Thyrian, J.R.; Hertel, J.; Wucherer, D.; Laufs, S.; Fleßa, S.; Hoffmann, W. Medication cost of persons with dementia in primary care in Germany. J. Alzheimer's Dis. 2014, 42, 949–958. [Google Scholar] [CrossRef] [Green Version]
- Jakovljevic, M.; Lamnisos, D.; Westerman, R.; Chattu, V.K.; Cerda, A. Future health spending forecast in leading emerging BRICS markets in 2030: Health policy implications. Health Res. Policy Syst. 2022, 20, 1–14. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Jakab, M.; Gerdtham, U.; McDaid, D.; Ogura, S.; Varavikova, E.; Merrick, J.; Adany, R.; Okunade, A.; Getzen, T.E. Comparative financing analysis and political economy of noncommunicable diseases. J. Med. Econ. 2019, 22, 722–727. [Google Scholar] [CrossRef]
- Abad-Díez, J.M.; Calderón-Larrañaga, A.; Poncel-Falcó, A.; Poblador-Plou, B.; Calderón-Meza, J.M.; Sicras-Mainar, A.; Clerencia-Sierra, M.; Prados-Torres, A. Age and gender differences in the prevalence and patterns of multimorbidity in the older population. BMC Geriatr. 2014, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Stock, S.A.; Stollenwerk, B.; Redaelli, M.; Civello, D.; Lauterbach, K.W. Sex differences in treatment patterns of six chronic diseases: An analysis from the German statutory health insurance. J. Women's Health 2008, 17, 343–354. [Google Scholar] [CrossRef]
- Park, B.; Park, J.; Jun, J.K. Cognitive impairment, depression, comorbidity of the two and associated factors among the early sixties in a rural Korean community. PLoS ONE 2013, 8, e79460. [Google Scholar] [CrossRef]
- Unutmaz, G.D.; Soysal, P.; Tuven, B.; Isik, A.T. Costs of medication in older patients: Before and after comprehensive geriatric assessment. Clin. Interv. Aging 2018, 13, 607. [Google Scholar] [CrossRef]
- Taylor, C.A.; Bouldin, E.D.; Greenlund, K.J.; McGuire, L.C. Comorbid chronic conditions among older adults with subjective cognitive decline, United States, 2015–2017. Innov. Aging 2020, 4, igz045. [Google Scholar] [CrossRef]
- Fukawa, T. Elderly Population Projection and Their Health Expenditure Prospects in Japan. Available online: https://www.scirp.org/journal/paperinformation.aspx?paperid=80147 (accessed on 20 March 2021).
- Song, M.-H. Design and Implementation of Healthcare System for Chronic Disease Management. Available online: https://www.koreascience.or.kr/article/JAKO201832073079599.pdf (accessed on 13 July 2018).
- Kang, S.H.; Ko, E. Factors Associated with Medication Adherence among the Elderly with Chronic Diseases. Korean J. Adult Nurs. 2021, 33, 189–201. [Google Scholar] [CrossRef]
- Kim, C.-H.; Hwang, I.; Yoo, W.-S. The common patterns of multimorbidity and its impact on healthcare cost in Korea. Health Policy Manag. 2014, 24, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Hazra, N.C.; Rudisill, C.; Gulliford, M.C. Determinants of health care costs in the senior elderly: Age, comorbidity, impairment, or proximity to death? Eur. J. Health Econ. 2018, 19, 831–842. [Google Scholar] [CrossRef] [Green Version]
- Sambamoorthi, U.; Tan, X.; Deb, A. Multiple chronic conditions and healthcare costs among adults. Expert Rev. Pharm. Outcomes Res. 2015, 15, 823–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathya, T.; Nagarajan, R.; Selvamani, Y. Multimorbidity as a Risk Factor of Elder Abuse/Mistreatment in India: A Cross-Sectional Study. Available online: https://journals.sagepub.com/doi/10.1177/0886260520980391 (accessed on 15 December 2020).
- Kim, H.S.; Yoo, B.-N.; Lee, E.W. Evaluation of the national chronic diseases management policy: Performance and future directions. Public Health Aff. 2018, 2, 105–120. [Google Scholar] [CrossRef] [Green Version]
- Milani, S.A.; Crooke, H.; Cottler, L.B.; Striley, C.W. Sex differences in frequent ED use among those with multimorbid chronic diseases. Am. J. Emerg. Med. 2016, 34, 2127–2131. [Google Scholar] [CrossRef] [Green Version]
- Van Minh, H.; Pocock, N.S.; Chaiyakunapruk, N.; Chhorvann, C.; Duc, H.A.; Hanvoravongchai, P.; Lim, J.; Lucero-Prisno, D.E., III; Ng, N.; Phaholyothin, N. Progress toward universal health coverage in ASEAN. Glob. Health Action 2014, 7, 25856. [Google Scholar] [CrossRef] [Green Version]
- Tomazic, T.; Jerkovic, O.S. Online interventions for the selective prevention of illicit drug use in young drug users: Exploratory study. J. Med. Internet Res. 2020, 22, e17688. [Google Scholar] [CrossRef]
- Koyanagi, A.; Lara, E.; Stubbs, B.; Carvalho, A.F.; Oh, H.; Stickley, A.; Veronese, N.; Vancampfort, D. Chronic physical conditions, multimorbidity, and mild cognitive impairment in low-and middle-income countries. J. Am. Geriatr. Soc. 2018, 66, 721–727. [Google Scholar] [CrossRef]


{kind=link}
| 2014 | |||
|---|---|---|---|
| Mean | SD 2 | p-Value | |
| Multiple chronic conditions | |||
| Yes | 1163.8 | 1839.2 | <0.0001 |
| No | 456.1 | 942.6 | |
| Cognitive impairment | |||
| No (Normal) | 621.6 | 1257.6 | |
| Yes | - | - | |
| Sex | |||
| Men | 659.1 | 1451.7 | 0.2163 |
| Women | 582.6 | 1016.5 | |
| Age | |||
| 60–69 | 566.6 | 1047.6 | <0.0001 |
| 70–79 | 685.7 | 1485.7 | |
| 80+ | 707.3 | 1418.7 | |
| Educational level | |||
| Less than middle school | 616.0 | 1091.6 | 0.0023 |
| High school or more | 630.7 | 1485.5 | |
| Region | |||
| City | 645.1 | 1318.2 | 0.3740 |
| Rural | 551.8 | 1055.3 | |
| Employment status | |||
| Employed | 592.9 | 1208.6 | 0.4199 |
| Unemployed | 655.8 | 1316.5 | |
| Household income | |||
| 1Q | 791.0 | 1439.1 | 0.0002 |
| 2Q | 562.4 | 944.4 | |
| 3Q | 580.0 | 1236.6 | |
| 4Q | 602.9 | 1342.9 | |
| Marital status | |||
| Unmarried | 597.3 | 1046.1 | 0.3130 |
| Married | 627.0 | 1299.7 | |
| BMI | |||
| Underweight | 528.4 | 1127.1 | <0.0001 |
| Normal | 569.5 | 1291.7 | |
| Obesity | 774.7 | 1165.5 | |
| Self-rated health | |||
| Good | 325.6 | 750.5 | <0.0001 |
| Bad | 798.2 | 1451.3 | |
| Current smoking | |||
| Yes | 494.5 | 913.0 | 0.0013 |
| No | 641.8 | 1302.8 | |
| Current alcohol consumption | |||
| Yes | 565.9 | 1100.6 | 0.0041 |
| No | 653.8 | 1339.2 | |
| Physical activity | |||
| Yes | 637.5 | 1390.9 | 0.3376 |
| No | 610.8 | 1157.6 | |
| ADL/IADL status | |||
| None | 605.1 | 1240.3 | 0.0008 |
| Mild | 774.4 | 1290.3 | |
| Severe | 1324.1 | 1552.1 | |
| Mean (SD) | 621.8 | (1257.6) | |
| Median | 252.1 | ||
| Total | 136,875.6 | ||
| Out-of-Pocket Medical Cost | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total | Hospital admission | Outpatient | Pharmacy | |||||
| β | p-value | β | p-value | β | p-value | β | p-value | |
| Intercept | 6.0634 | <0.0001 | 7.7544 | <0.0001 | 5.0688 | <0.0001 | 5.9254 | <0.0001 |
| Change of multiple chronic diseases | ||||||||
| Bad → Bad | 0.8048 | <0.0001 | 0.1129 | 0.3925 | 0.5073 | <0.0001 | 0.5907 | <0.0001 |
| Bad → Good | 0.1133 | 0.1069 | −0.1373 | 0.2682 | 0.1779 | 0.0854 | 0.0081 | 0.8884 |
| Good → Bad | 0.6737 | <0.0001 | 0.1052 | 0.3829 | 0.4392 | <0.0001 | 0.3938 | <0.0001 |
| Good → Good | ref. | ref. | ref. | ref. | ||||
| Cognitive impairment | ||||||||
| Yes | 0.2156 | 0.0079 | 0.2002 | 0.2429 | 0.1284 | 0.0642 | 0.2143 | <0.0001 |
| No (Normal) | ref. | ref. | ref. | ref. | ||||
| Sex | ||||||||
| Men | ref. | ref. | ref. | ref. | ||||
| Women | −0.1786 | 0.0051 | −0.0693 | 0.4804 | −0.0108 | 0.8885 | −0.2498 | <0.0001 |
| Age | ||||||||
| 60–69 | ref. | ref. | ref. | ref. | ||||
| 70–79 | −0.0834 | 0.1702 | −0.0661 | 0.5565 | 0.0900 | 0.2187 | −0.0530 | 0.1808 |
| 80+ | −0.1480 | 0.1582 | −0.1523 | 0.5243 | 0.0544 | 0.5833 | 0.0060 | 0.9374 |
| Educational level | ||||||||
| Less than middle school | ref. | ref. | ref. | ref. | ||||
| High school or more | −0.0285 | 0.6397 | −0.0187 | 0.8562 | −0.1261 | 0.0509 | −0.0295 | 0.5008 |
| Region | ||||||||
| City | ref. | ref. | ref. | ref. | ||||
| Rural | 0.0129 | 0.8301 | 0.2086 | 0.0276 | 0.0178 | 0.8078 | −0.0012 | 0.9813 |
| Employment status | ||||||||
| Yes | ref. | ref. | ref. | ref. | ||||
| No | 0.1203 | 0.0214 | 0.0048 | 0.8946 | 0.0462 | 0.5179 | 0.0048 | 0.8946 |
| Household income | ||||||||
| 1Q (Lowest) | 0.0141 | 0.8677 | −0.2090 | 0.2002 | −0.2214 | 0.0147 | 0.0670 | 0.2749 |
| 2Q | −0.1978 | 0.0040 | −0.3547 | 0.0106 | −0.2205 | 0.0032 | 0.0037 | 0.9442 |
| 3Q | 0.0323 | 0.6546 | −0.0004 | 0.9976 | −0.0680 | 0.3898 | 0.0230 | 0.6159 |
| 4Q (Highest) | ref. | ref. | ref. | ref. | ||||
| Marital status | ||||||||
| Unmarried | −0.0059 | 0.9384 | 0.1015 | 0.4992 | −0.0633 | 0.4652 | −0.0927 | 0.0843 |
| Married | ref. | ref. | ref. | ref. | ||||
| BMI | ||||||||
| Underweight | 0.0735 | 0.5818 | −0.0877 | 0.6712 | −0.0558 | 0.6811 | 0.0340 | 0.7335 |
| Normal | ref. | ref. | ref. | ref. | ||||
| Obesity | 0.1423 | 0.0118 | −0.0900 | 0.3548 | 0.1173 | 0.0912 | 0.0687 | 0.0756 |
| Current smoking | ||||||||
| Yes | −0.1931 | 0.0252 | −0.0305 | 0.8350 | −0.1420 | 0.0317 | −0.1022 | 0.1267 |
| No | ref. | ref. | ref. | ref. | ||||
| Current alcohol consumption | ||||||||
| Yes | −0.0960 | 0.0731 | −0.2153 | 0.0168 | −0.1586 | 0.0053 | −0.0273 | 0.5642 |
| No | ref. | ref. | ref. | ref. | ||||
| Self-rated health | ||||||||
| Good | ref. | ref. | ref. | ref. | ||||
| Bad | 0.6927 | <0.0001 | 0.2899 | 0.0126 | 0.4164 | <0.0001 | 0.2923 | <0.0001 |
| Physical activity | ||||||||
| Yes | ref. | ref. | ref. | ref. | ||||
| No | −0.0769 | 0.0295 | 0.1476 | 0.1011 | −0.0617 | 0.2462 | −0.0769 | 0.0295 |
| ADL/IADL status | ||||||||
| None | ref. | ref. | ref. | ref. | ||||
| Mild | 0.2908 | 0.0674 | 0.4331 | 0.0482 | 0.1846 | 0.2518 | −0.1057 | 0.0905 |
| Severe | 1.0950 | <0.0001 | 0.6426 | 0.0018 | 0.6496 | 0.0045 | −0.3490 | 0.0013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Nam, J.Y. Effects of Changes in Multiple Chronic Conditions on Medical Costs among Older Adults in South Korea. Healthcare 2022, 10, 742. https://doi.org/10.3390/healthcare10040742
Park S, Nam JY. Effects of Changes in Multiple Chronic Conditions on Medical Costs among Older Adults in South Korea. Healthcare. 2022; 10(4):742. https://doi.org/10.3390/healthcare10040742
Chicago/Turabian StylePark, Soojin, and Jin Young Nam. 2022. "Effects of Changes in Multiple Chronic Conditions on Medical Costs among Older Adults in South Korea" Healthcare 10, no. 4: 742. https://doi.org/10.3390/healthcare10040742