
Appropriate Needle Length Determined by Ultrasonic Echography for Intramuscular Injection in Japanese Elderly over 50 Years

Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects
2.2. Study Design
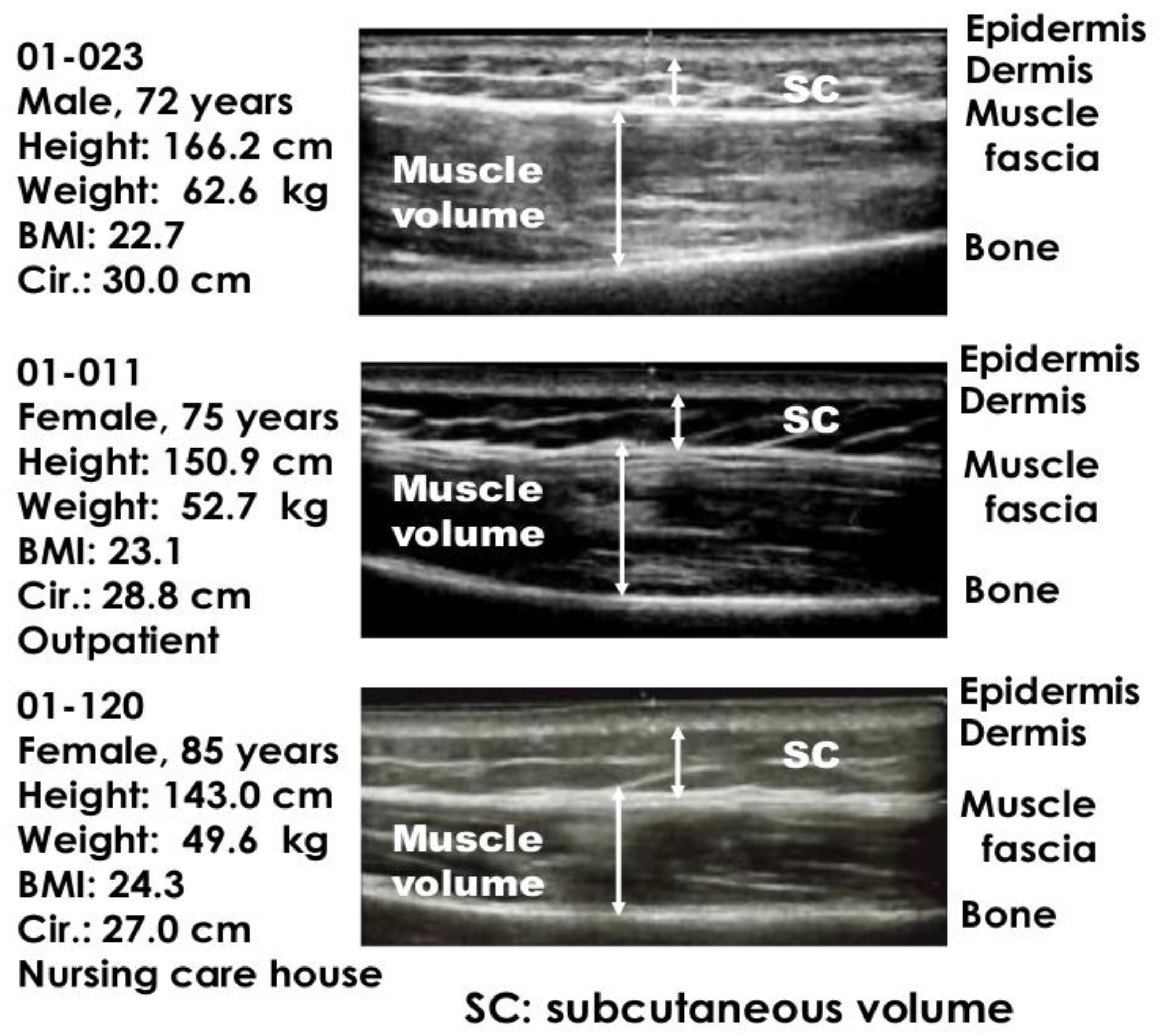
2.3. Ultrasonic Echography
2.4. Statistical Analyses
3. Results
3.1. Body Weight, Height, BMI, and Circumference of Upper Arm in Different Age Groups
3.2. The Depth from Skin Surface to Muscle Fascia and Bone in Different Age Groups
3.3. The Depth from Skin Surface to Muscle Fascia and Bone in Different Genders
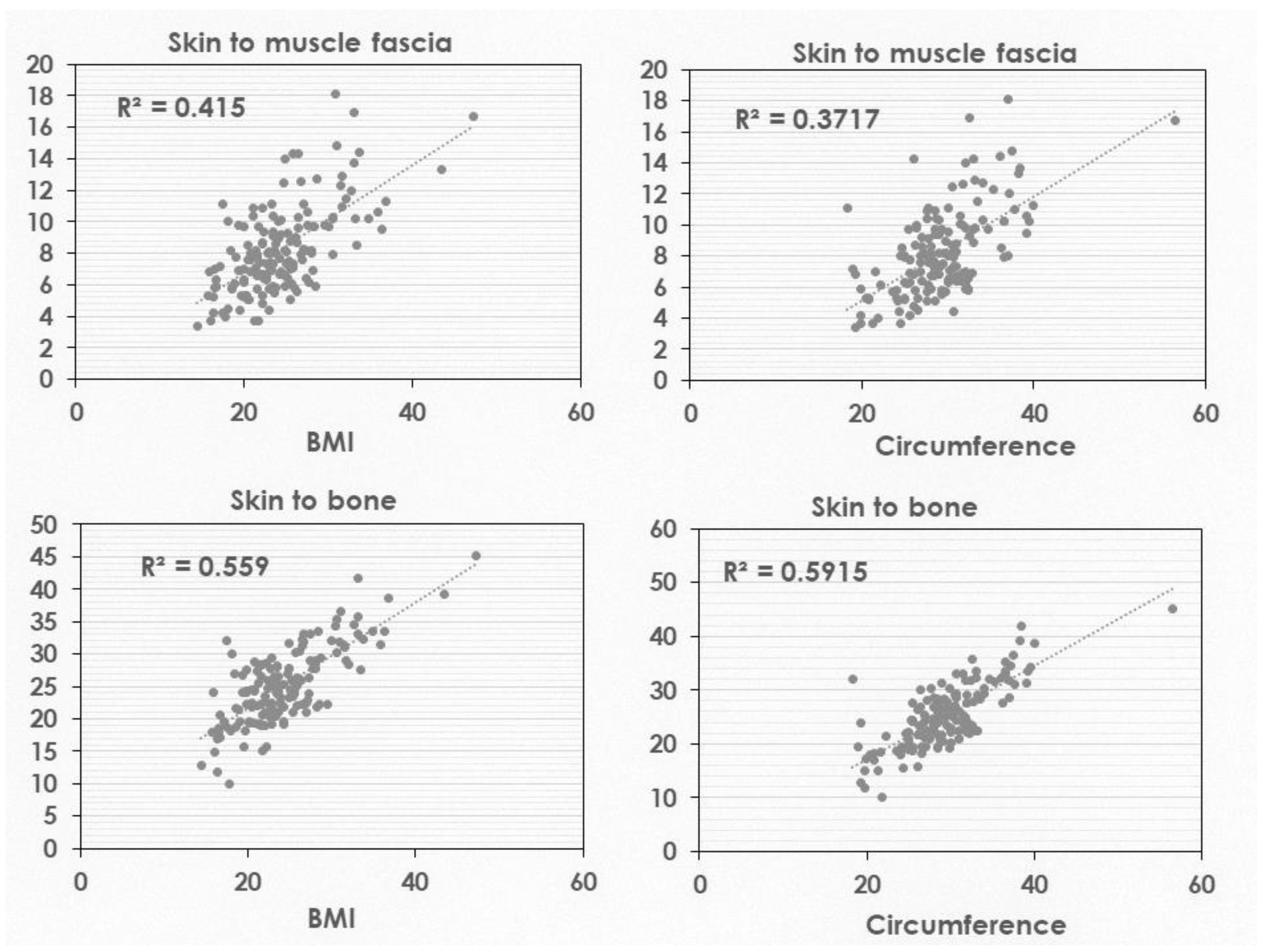
3.4. Correlation between Subcutaneous Mass and Body Structure (BMI and Circumference)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saitoh, A.; Okabe, N. Current issues with the immunization program in Japan: Can we fill the vaccine gap. Vaccine 2012, 30, 4752–4756. [Google Scholar] [CrossRef]
- Yamamoto, S.; Kuroki, T.; Kurai, K.; Lino, S. Comparison of results for Phase I studies with recombinant and plasma-derived hepatitis B vaccines, and controlled study comparing intramuscular and subcutaneous injections of recombinant hepatitis B vaccine. J. Infect. 1986, 13, 53–60. [Google Scholar] [CrossRef]
- Japan Pediatric Society, Committee on Muscular Contracture. A report of muscular contracture. J. Jpn. Pediatr. Soc. 1983, 87, 1067–1099. (In Japanese) [Google Scholar]
- Hagen, R. Contracture of the quadriceps muscle in children. A report of 12 cases. Acta Orthop. Scand. 1968, 39, 565–578. [Google Scholar] [CrossRef]
- Kashiwagi, Y.; Maeda, M.; Kawashima, H.; Nakayama, T. Inflammatory responses following intramuscular and subcutaneous immunization with aluminum-adjuvanted or non-adjuvanted vaccines. Vaccine 2014, 32, 3393–3401. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, T. Vaccine choronicle in Japan. J. Infect. Chemother. 2013, 19, 787–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pharmaceuticals and Medical Devices Agency. Summary of the Report on the Surveillance Results of HPV Vaccines. Available online: https://www.mhlw.go.jp/content/10601000/1-2.pdf (accessed on 15 March 2022).
- Gagliardi, A.M.Z.; Andriolo, B.N.G.; Soares, B.G.O.; de Oliveira Gomes, J.; Andriolo, R.B.; Canteiro Cruz, E. Vaccines for preventing herpes zoster in older adults. Cochrane Database Syst. Rev. 2019, 2019, CD008858. [Google Scholar] [CrossRef] [Green Version]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Cook, I.F.; Williamson, M.; Pond, D. Definition of needle length required for intramuscular deltoid injection in elderly adults: An ultrasonographic study. Vaccine 2006, 24, 937–940. [Google Scholar] [CrossRef]
- Centers for Disease Control. Vaccine Recommendations and Guidelines of the ACIP General Best Practice Guidelines for immunization; Advisory Committee on Immunization Practices (ACIP) General Best Guidance for Immunization (cdc.gov). Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/downloads/general-recs.pdf (accessed on 15 March 2022).
- Rudenko, L.G.; Arden, N.H.; Grigorieva, E.; Naychin, A.; Rekstin, A.; Klimov, A.I.; Donina, S.; Desheva, J.; Holman, R.C.; DeGuzman, A.; et al. Immunogenicity and efficacy of Russian live attenuated and US inactivated vaccine alone and in combination in nursing home residents. Vaccine 2001, 19, 308–318. [Google Scholar] [CrossRef]
- Zuckerman, J.N. The importance of injecting vaccines into muscle: Different patients need different needle sizes. BMJ 2000, 321, 1237–1238. [Google Scholar] [CrossRef]
- Nakayama, T.; Kojdera, U.; Fujino, M.; Tanaka, T.; Yatabe, K.; Hashiguchi, T.; Sato, T.; Kino, M. Appropriate Needle Lengths Determined Using Ultrasonic Echograms for Intramuscular Injections in Japanese Infants. Open J. Pediatr. 2016, 6, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Herzog, C. Influence of parenteral administration routes and additional factors on vaccine safety and immunogenicity: A review of recent literature. Expert. Rev. Vaccines 2014, 13, 399–415. [Google Scholar] [CrossRef]
- Petousis-Harris, H. Vaccine injection technique and reactogenicity—Evidence for practice. Vaccine 2008, 26, 6299–6304. [Google Scholar] [CrossRef] [PubMed]
- Ols, S.; Yang, L.; Thompson, E.A.; Pushparai, P.; Tran, K.; Liang, F.; Lin, A.; Eriksson, B.; Hedestam, G.B.K.; Wyatt, R.T.; et al. Route of vaccine administration alters antigen trafficking but not innate or adaptive immunity. Cell Rep. 2020, 30, 3964–3971.e7. [Google Scholar] [CrossRef] [PubMed]
- Diggle, L.; Deeks, J.J.; Pollard, A.J. Effect of needle size on immunogenicity and reactogenicity of vaccines in infants: Randomised controlled trial. BMJ 2006, 333, 571. [Google Scholar] [CrossRef] [Green Version]
- Cook, I.F. Evidence based route of administration of vaccines. Hum. Vacccines 2008, 4, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Ikeno, D.; Kimachi, K.; Kino, Y.; Harada, S.; Yoshida, K.; Tochihara, S.; Itamura, S.; Odagiri, T.; Tashiro, M.; Okada, K.; et al. Immunogenicity of an inactivated adjuvanted whole-virion influenza A (H5N1, NIBRG-14) vaccine administered by intramuscular or subcutaneous injection. Microbiol. Immunol. 2010, 54, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Cook, I.F.; Barr, I.; Hartel, G.; Pond, D.; Hampson, A.W. Reactogenicity and immunogenicity of an inactivated influenza vaccine administered by intramuscular or subcutaneous injection in elderly adults. Vaccine 2006, 24, 2395–2402. [Google Scholar] [CrossRef] [PubMed]
- Cook, I.F.; Pond, D.; Hartel, G. Comparative reactogenicity and immunogenicity of 23 valent pneumococcal vaccine administered by intramuscular or subcutaneous injection in elderly adults. Vaccine 2007, 25, 4767–4774. [Google Scholar] [CrossRef] [PubMed]
- Diez-Domingo, J.; Weinke, T.; de Lomas, J.G.; Meyer, C.U.; Bertrand, I.; Eymin, C.; Thomas, S.; Sadorge, C. Comparison of intramuscular and subcutaneous administration of a herpes zoster live-attenuated vaccine in adults aged ≥ 50 years: A randomised non-inferiority clinical trial. Vaccine 2015, 33, 789–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vink, P.; Shiramoto, M.; Ogawa, M.; Eda, M.; Douha, M.; Heineman, T.; Lal, H. Safety and immunogenicity of a Herpes Zoster subunit vaccine in Japanese population aged ≥ 50 years when administered subcutaneously vs. intramuscularly. Hum. Vacccines Immunother. 2017, 13, 574–578. [Google Scholar] [CrossRef] [Green Version]
- CDC. Vaccine Administration: Intramuscular (IM) Injection Adults 19 Years Age and Older. In Vaccine Administration: Intramuscular (IM) Injections: Adults 19 Years of Age and Older; CDC: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/vaccines/hcp/admin/downloads/IM-Injection-adult.pdf (accessed on 15 March 2022).



{kind=link}
{kind=link}
| Category | Male | Female |
|---|---|---|
| 50–64 years (n = 50) | 26 | 24 |
| 65–74 years (n = 50) | 25 | 25 |
| ≥75 years | ||
| Outpatients (n = 20) | 14 | 6 |
| Needed nursing care (n = 18) | 8 | 10 |
| Nursing home bed-ridden (n = 18) | 8 | 10 |
| Total (n = 156) | 81 | 75 |
| Height (cm) | Body Weight (kg) | BMI | Circumference (cm) | |
|---|---|---|---|---|
| 50–64 years (n = 50) | 164.34 ± 8.86 ** | 73.32 ± 20.44 ** | 26.96 ± 6.40 * | 32.09 ± 5.59 * |
| 65–74 years (n = 50) | 159.60 ± 9.05 * | 63.33 ± 10.34 ** | 24.81 ± 3.79 ** | 30.02 ± 3.20 ** |
| ≥75 years (n = 38) | 155.34 ± 9.66 | 54.95 ± 10.34 ** | 22.64 ± 2.97 ** | 27.30 ± 3.28 ** |
| Nursing home (n = 18) | 154.72 ± 8.20 | 44.64 ± 9.99 | 18.46 ± 2.72 | 22.90 ± 3.66 |
| Age Group | Epidermis | SC Volume | Muscle Volume | Skin Surface to Muscle Fascia | Skin Surface to Bone |
|---|---|---|---|---|---|
| 50–64 years (n = 50) | 2.26 ± 0.54 | 6.90 ± 3.01 | 19.44 ± 4.44 | 9.16 ± 3.02 | 28.60 ± 5.91 |
| ≥75 years (n = 38) | 1.93 ± 0.54 ** | 5.58 ± 2.03 * | 15.02 ± 3.15 ** | 7.52 ± 2.13 ** | 22.54 ± 3.85 ** |
| Outpatients (n = 20) | 1.87 ± 0.46 | 5.65 ± 1.60 | 15.31 ± 3.48 | 7.51 ± 1.72 | 22.82 ± 4.06 * |
| need nursing care (n = 18) | 2.01 ± 0.61 | 5.52 ± 2.46 | 14.70 ± 2.80 | 7.53 ± 2.56 | 22.23 ± 3.68 |
| Bedridden (n = 18) | 1.71 ± 0.39 | 4.73 ± 1.79 | 13.03 ± 3.75 | 6.44 ± 2.05 | 19.47 ± 5.55 * |
| Subcutaneous Mass in Subjects 50–64 Years | |||||
|---|---|---|---|---|---|
| Epidermis | Subcutaneous Volume | Muscle Volume | Skin Surface to Muscle Fascia | Skin Surface to Bone | |
| Male (n = 26) | 2.51 ± 0.55 ** | 5.62 ± 2.80 | 20.23 ± 4.21 | 8.12 ± 2.94 | 28.36 ± 5.62 |
| Female (n = 24) | 2.00 ± 0.39 | 8.29 ± 2.63 ** | 18.58 ± 4.60 | 10.29 ± 2.74 ** | 28.87 ± 6.33 |
| Subcutaneous Mass in subjects 65–74 Years | |||||
| Male (n = 26) | 2.27 ± 0.43 ** | 5.10 ± 1.55 | 16.82 ± 2.29 | 7.37 ± 1.75 | 24.19 ± 2.76 |
| Female (n = 24) | 1.83 ± 0.37 | 7.72 ± 3.06 ** | 17.09 ± 3.94 | 9.55 ± 3.20 ** | 26.64 ± 5.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakayama, T.; Sekino, H.; Aihara, H.; Kino, M. Appropriate Needle Length Determined by Ultrasonic Echography for Intramuscular Injection in Japanese Elderly over 50 Years. Healthcare 2022, 10, 800. https://doi.org/10.3390/healthcare10050800
Nakayama T, Sekino H, Aihara H, Kino M. Appropriate Needle Length Determined by Ultrasonic Echography for Intramuscular Injection in Japanese Elderly over 50 Years. Healthcare. 2022; 10(5):800. https://doi.org/10.3390/healthcare10050800
Chicago/Turabian StyleNakayama, Tetsuo, Hisakuni Sekino, Hirokazu Aihara, and Minoru Kino. 2022. "Appropriate Needle Length Determined by Ultrasonic Echography for Intramuscular Injection in Japanese Elderly over 50 Years" Healthcare 10, no. 5: 800. https://doi.org/10.3390/healthcare10050800