
Two-Month Individually Supervised Exercise Therapy Improves Walking Speed, Step Length, and Temporal Gait Symmetry in Chronic Stroke Patients: A before–after Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
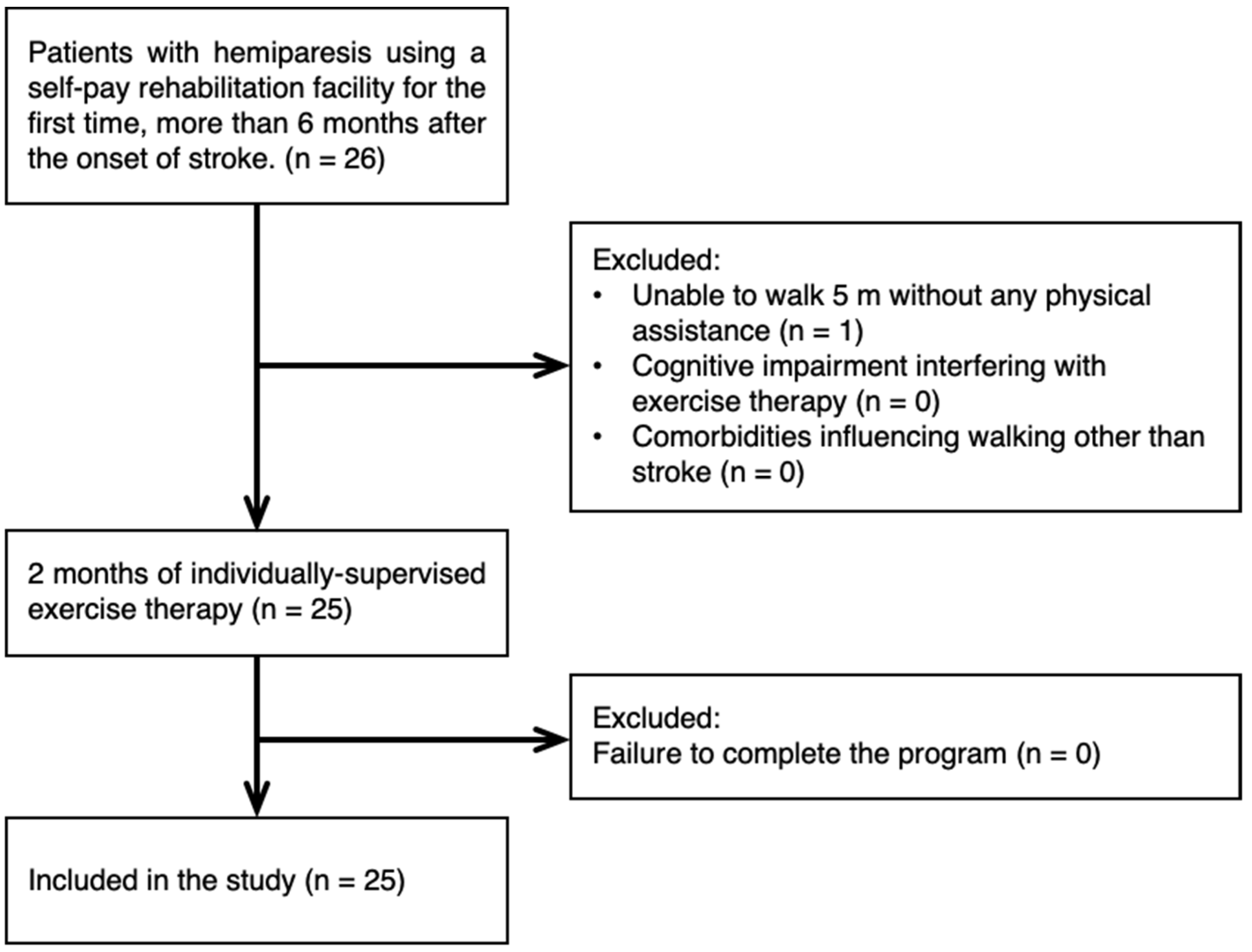
2.1. Design and Subjects
2.2. Intervention
2.3. Measurement and Analysis
2.4. Statistical Analysis
2.5. Ethical Considerations
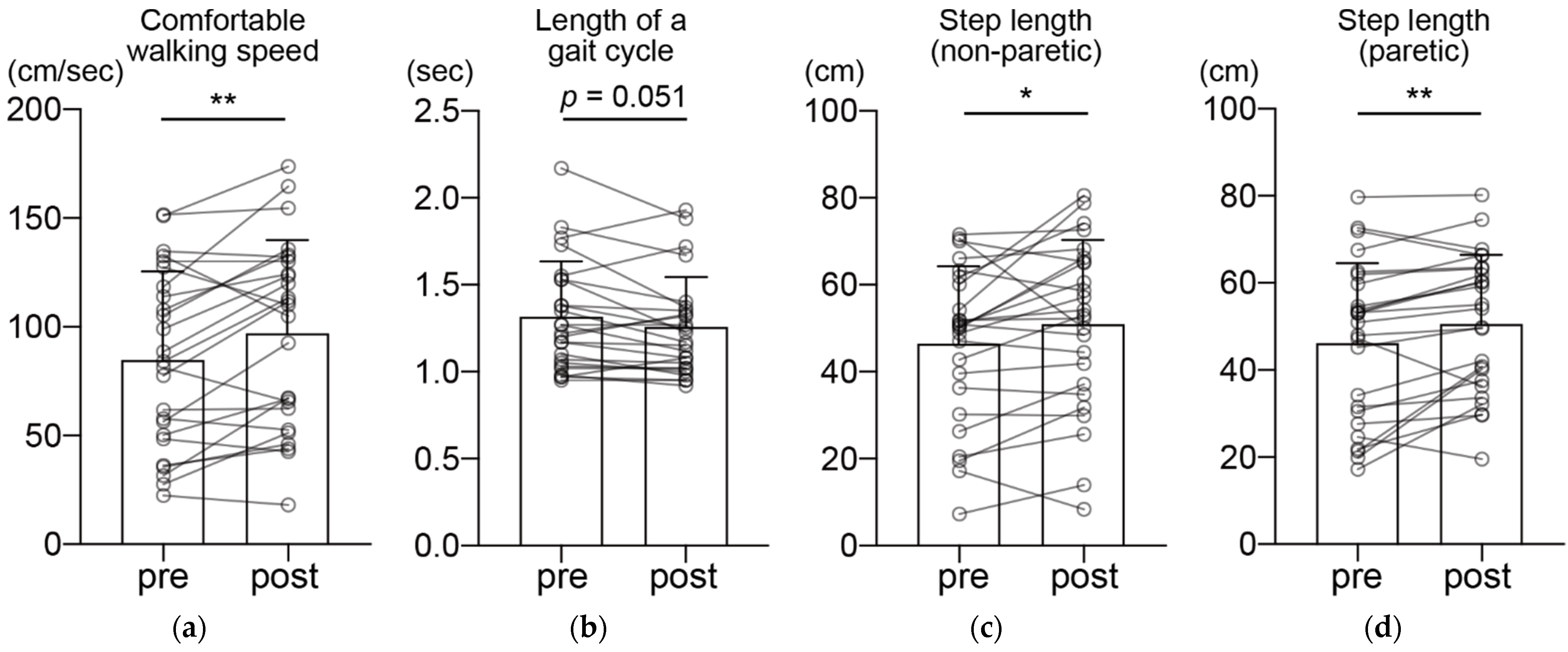
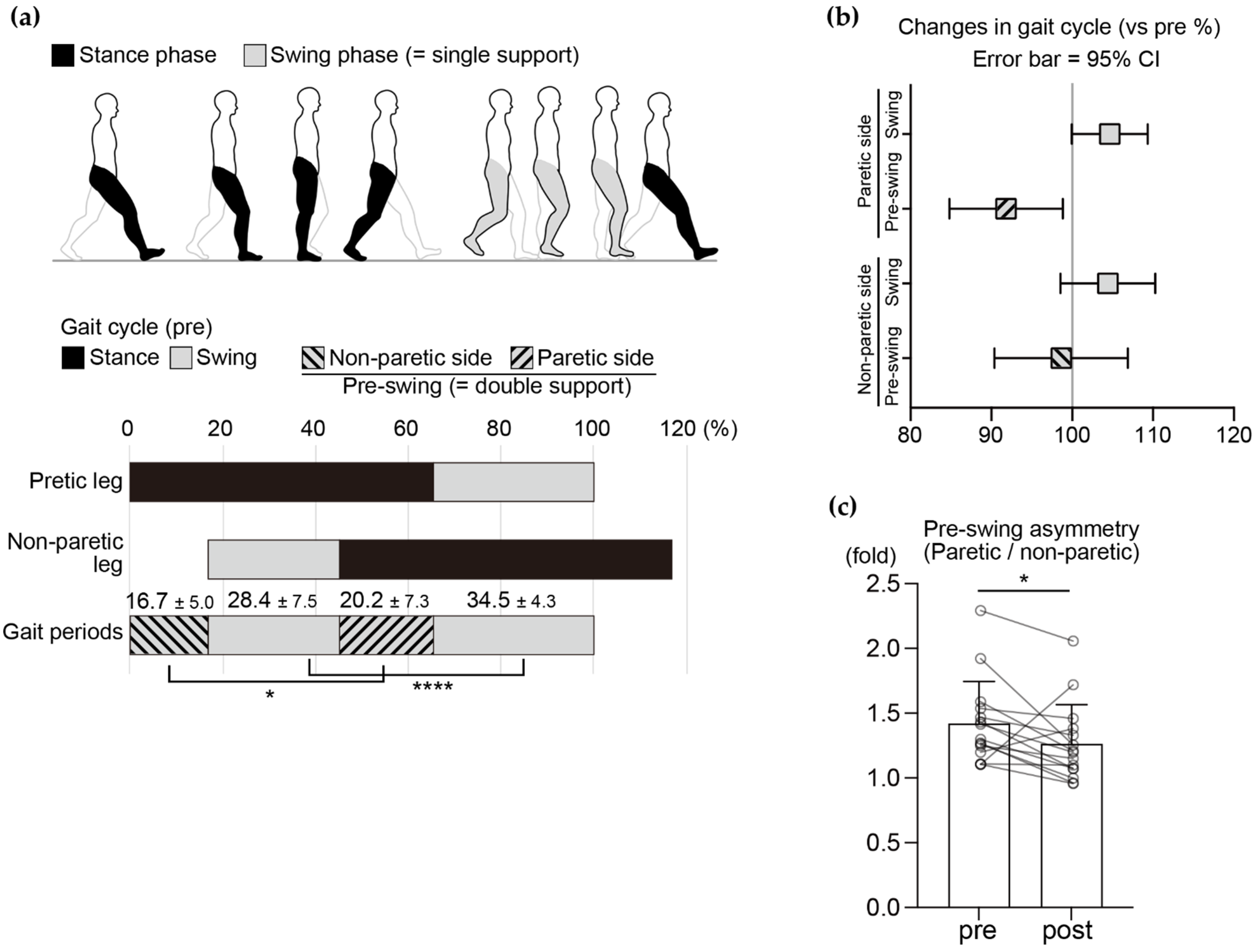
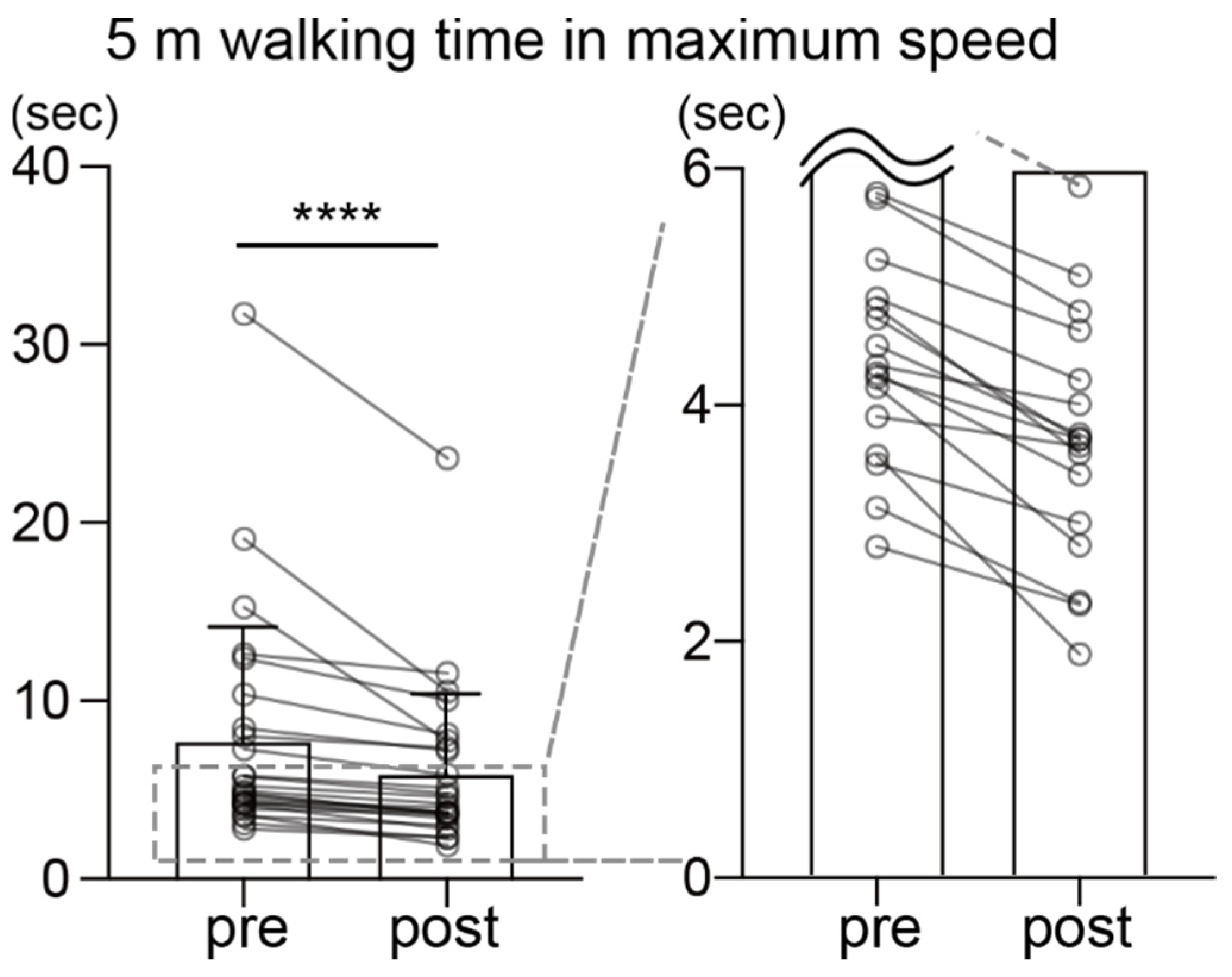
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; RayDorsey, E.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Mayo, N.E.; Wood-Dauphinee, S.; Ahmed, S.; Gordon, C.; Higgins, J.; McEwen, S.; Salbach, N. Disablement following stroke. Disabil. Rehabil. 1999, 21, 258–268. [Google Scholar] [CrossRef] [PubMed]
- SLord, E.; McPherson, K.; McNaughton, H.K.; Rochester, L.; Weatherall, M. Community ambulation after stroke: How important and obtainable is it and what measures appear predictive? Arch. Phys. Med. Rehabil. 2004, 85, 234–239. [Google Scholar]
- Han, E.Y.; Im, S.H.; Kim, B.R.; Seo, M.J.; Kim, M.O. Robot-assisted gait training improves brachial-ankle pulse wave velocity and peak aerobic capacity in subacute stroke patients with totally dependent ambulation: Randomized controlled trial. Medicine 2016, 95, e5078. [Google Scholar] [CrossRef]
- Alexander, L.D.; Black, S.E.; Patterson, K.K.; Gao, F.; Danells, C.J.; McIlroy, W.E. Association between gait asymmetry and brain lesion location in stroke patients. Stroke 2009, 40, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Awad, L.N.; Palmer, J.A.; Pohlig, R.T.; Binder-Macleod, S.A.; Reisman, D.S. Walking speed and step length asymmetry modify the energy cost of walking after stroke. Neurorehabilit. Neural Repair 2015, 29, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Wei, T.S.; Liu, P.T.; Chang, L.W.; Liu, S.Y. Gait asymmetry, ankle spasticity, and depression as independent predictors of falls in ambulatory stroke patients. PLoS ONE 2017, 12, e0177136. [Google Scholar] [CrossRef]
- Lewek, M.D.; Bradley, C.E.; Wutzke, C.J.; Zinder, S.M. The relationship between spatiotemporal gait asymmetry and balance in individuals with chronic stroke. J. Appl. Biomech. 2014, 30, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Lewek, M.D.; Feasel, J.; Wentz, E.; Brooks, F.P., Jr.; Whitton, M.C. Use of visual and proprioceptive feedback to improve gait speed and spatiotemporal symmetry following chronic stroke: A case series. Phys. Ther. 2012, 92, 748–756. [Google Scholar] [CrossRef]
- Reisman, D.S.; McLean, H.; Keller, J.; Danks, K.A.; Bastian, A.J. Repeated split-belt treadmill training improves poststroke step length asymmetry. Neurorehabil. Neural Repair 2013, 27, 460–468. [Google Scholar] [CrossRef] [Green Version]
- Lewek, M.D.; Braun, C.H.; Wutzke, C.; Giuliani, C. The role of movement errors in modifying spatiotemporal gait asymmetry post stroke: A randomized controlled trial. Clin. Rehabil. 2018, 32, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, A.; Ofluoglu, D.; Hirai, B.; Kim, S. The effect of an ankle-foot orthosis on temporal spatial parameters and asymmetry of gait in hemiparetic patients. PMR 2009, 1, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Simons, C.D.; van Asseldonk, E.H.; van der Kooij, H.; Geurts, A.C.; Buurke, J.H. Ankle-foot orthoses in stroke: Effects on functional balance, weight-bearing asymmetry and the contribution of each lower limb to balance control. Clin. Biomech. 2009, 24, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.S.; Yang, H.S.; Jung, S.; Kang, C.S.; Jang, S.; Kim, D.H. Effect of reducing assistance during robot-assisted gait training on step length asymmetry in patients with hemiplegic stroke: A randomized controlled pilot trial. Medicine 2018, 97, e11792. [Google Scholar] [CrossRef]
- Tanaka, H.; Nankaku, M.; Nishikawa, T.; Hosoe, T.; Yonezawa, H.; Mori, H.; Kikuchi, T.; Nishi, H.; Takagi, Y.; Miyamoto, S.; et al. Spatiotemporal gait characteristic changes with gait training using the hybrid assistive limb for chronic stroke patients. Gait Posture 2019, 71, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef]
- Hatano, E. Long-term Care Insurance in Japan: How physicians are involved in providing rehabilitation for the elderly. Jpn. Med. Assoc. J. 2012, 55, 231–239. [Google Scholar]
- Miura, S.; Miyata, R.; Matsumoto, S.; Higashi, T.; Wakisaka, Y.; Ago, T.; Kitazono, T.; Iihara, K.; Shimodozono, M. Quality Management Program of Stroke Rehabilitation Using Adherence to Guidelines: A Nationwide Initiative in Japan. J. Stroke Cerebrovasc. Dis. 2019, 28, 2434–2441. [Google Scholar] [CrossRef]
- Lauzière, S.; Miéville, C.; Betschart, M.; Aissaoui, R.; Nadeau, S. Plantarflexor weakness is a determinant of kinetic asymmetry during gait in post-stroke individuals walking with high levels of effort. Clin. Biomech. 2015, 30, 946–952. [Google Scholar] [CrossRef]
- Balasubramanian, C.K.; Bowden, M.G.; Neptune, R.R.; Kautz, S.A. Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch. Phys. Med. Rehabil. 2007, 88, 43–49. [Google Scholar] [CrossRef]
- Pang, M.Y.; Eng, J.J.; Dawson, A.S.; Gylfadottir, S. The use of aerobic exercise training in improving aerobic capacity in individuals with stroke: A meta-analysis. Clin. Rehabil. 2006, 20, 97–111. [Google Scholar] [CrossRef] [Green Version]
- Umberger, B.R. Stance and swing phase costs in human walking. J. R. Soc. Interface 2010, 7, 1329–1340. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of walking handicap in the stroke population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Goldie, P.A.; Matyas, T.A.; Evans, O.M. Gait after stroke: Initial deficit and changes in temporal patterns for each gait phase. Arch. Phys. Med. Rehabil. 2001, 82, 1057–1065. [Google Scholar] [CrossRef]
- Malone, L.A.; Bastian, A.J. Spatial and temporal asymmetries in gait predict split-belt adaptation behavior in stroke. Neurorehabil. Neural Repair 2014, 28, 230–240. [Google Scholar] [CrossRef]
- Patterson, K.K.; Parafianowicz, I.; Danells, C.J.; Closson, V.; Verrier, M.C.; Staines, W.R.; Black, S.E.; McIlroy, W.E. Gait asymmetry in community-ambulating stroke survivors. Arch. Phys. Med. Rehabil. 2008, 89, 304–310. [Google Scholar] [CrossRef]
- Kharb, A.; Saini, V.; Jain, Y.; Dhiman, S. A review of gait cycle and its parameters. IJCEM Int. J. Comput. Eng. Manag. 2011, 13, 78–83. [Google Scholar]
- Pinzur, M.S.; Sherman, R.; DiMonte-Levine, P.; Trimble, J. Gait changes in adult onset hemiplegia. Am. J. Phys. Med. 1987, 66, 228–237. [Google Scholar] [CrossRef]
- Gaviria, M.; D’Angeli, M.; Chavet, P.; Pelissier, J.; Peruchon, E.; Rabischong, P. Plantar dynamics of hemiplegic gait: A methodological approach. Gait Posture 1996, 4, 297–305. [Google Scholar] [CrossRef]
- Patterson, K.K.; Gage, W.H.; Brooks, D.; Black, S.E.; McIlroy, W.E. Evaluation of gait symmetry after stroke: A comparison of current methods and recommendations for standardization. Gait Posture 2010, 31, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Tate, J.J.; Milner, C.E. Real-time kinematic, temporospatial, and kinetic biofeedback during gait retraining in patients: A systematic review. Phys. Ther. 2010, 90, 1123–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Quervain, I.A.; Simon, S.R.; Leurgans, S.; Pease, W.S.; McAllister, D. Gait pattern in the early recovery period after stroke. J. Bone Jt. Surg. Am. 1996, 78, 1506–1514. [Google Scholar] [CrossRef] [Green Version]
- Rozanski, G.M.; Wong, J.S.; Inness, E.L.; Patterson, K.K.; Mansfield, A. Longitudinal change in spatiotemporal gait symmetry after discharge from inpatient stroke rehabilitation. Disabil. Rehabil. 2020, 42, 705–711. [Google Scholar] [CrossRef]
- Schmid, A.; Duncan, P.W.; Studenski, S.; Lai, S.M.; Richards, L.; Perera, S.; Wu, S. Improvements in speed-based gait classifications are meaningful. Stroke 2007, 38, 2096–2100. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, L.R.; de Oliveira, C.Q.; Ada, L.; Michaelsen, S.M.; Teixeira-Salmela, L.F. Walking training with cueing of cadence improves walking speed and stride length after stroke more than walking training alone: A systematic review. J. Physiother. 2015, 61, 10–15. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| n | 25 |
| Sex (male/female) | 18/7 |
| Age (years) | 61.9 ± 11.1 |
| Type of stroke (infraction/hemorrhage) | 13/12 |
| Paretic side (left/right) | 18/7 |
| Median period from onset (months) | 19 (range: 6 to 192) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshioka, K.; Watanabe, T.; Maruyama, N.; Yoshioka, M.; Iino, K.; Honda, K.; Hayashida, K. Two-Month Individually Supervised Exercise Therapy Improves Walking Speed, Step Length, and Temporal Gait Symmetry in Chronic Stroke Patients: A before–after Trial. Healthcare 2022, 10, 527. https://doi.org/10.3390/healthcare10030527
Yoshioka K, Watanabe T, Maruyama N, Yoshioka M, Iino K, Honda K, Hayashida K. Two-Month Individually Supervised Exercise Therapy Improves Walking Speed, Step Length, and Temporal Gait Symmetry in Chronic Stroke Patients: A before–after Trial. Healthcare. 2022; 10(3):527. https://doi.org/10.3390/healthcare10030527
Chicago/Turabian StyleYoshioka, Kiyoshi, Tatsunori Watanabe, Norikazu Maruyama, Mizuki Yoshioka, Keita Iino, Kimikazu Honda, and Koshiro Hayashida. 2022. "Two-Month Individually Supervised Exercise Therapy Improves Walking Speed, Step Length, and Temporal Gait Symmetry in Chronic Stroke Patients: A before–after Trial" Healthcare 10, no. 3: 527. https://doi.org/10.3390/healthcare10030527