
Video-Assisted Intubating Stylet Technique for Difficult Intubation: A Case Series Report

 , and
, and
Abstract
:1. Introduction
2. Cases Presentation
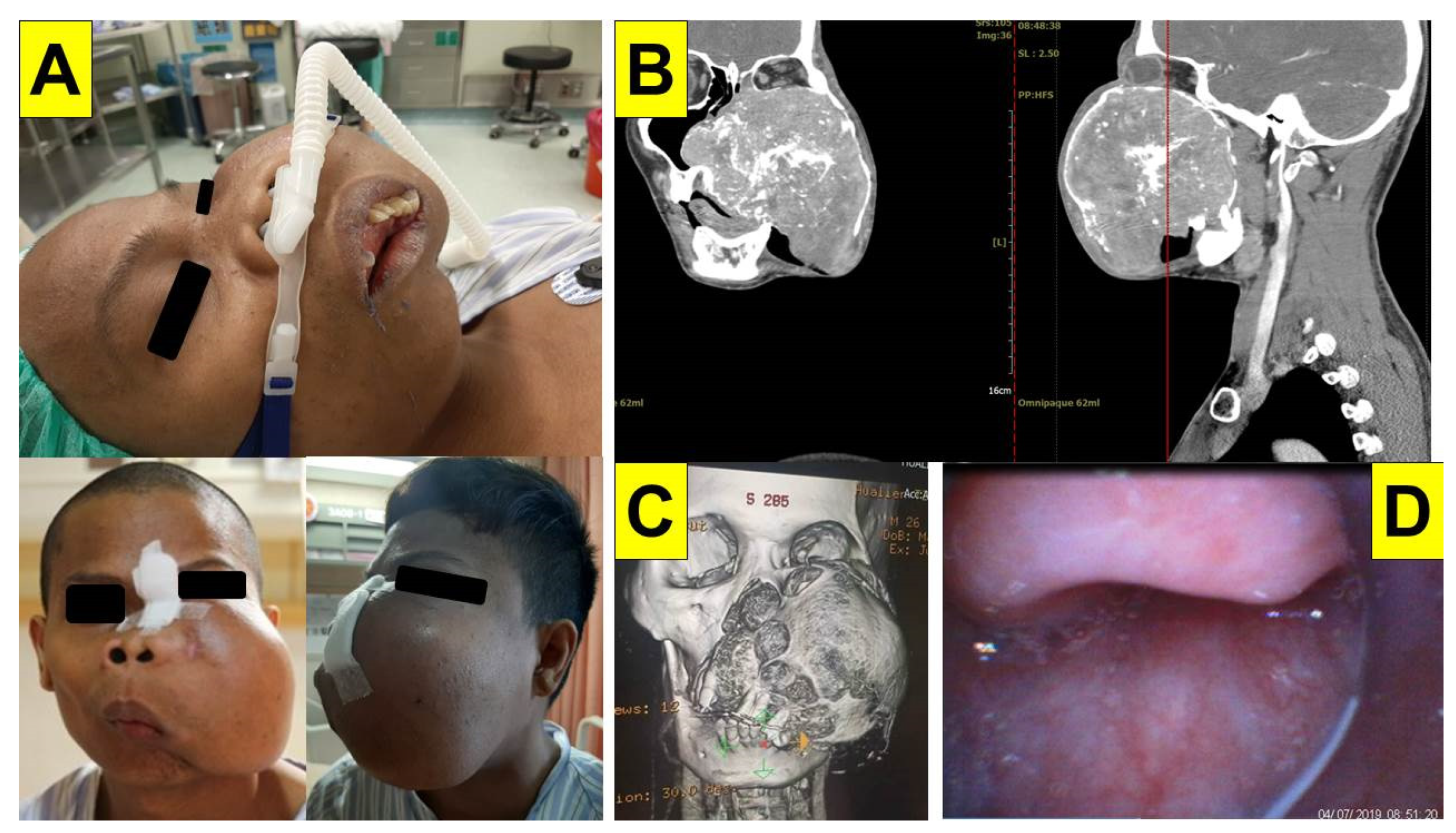
2.1. Case 1: Giant Cemento-Ossifying Fibroma
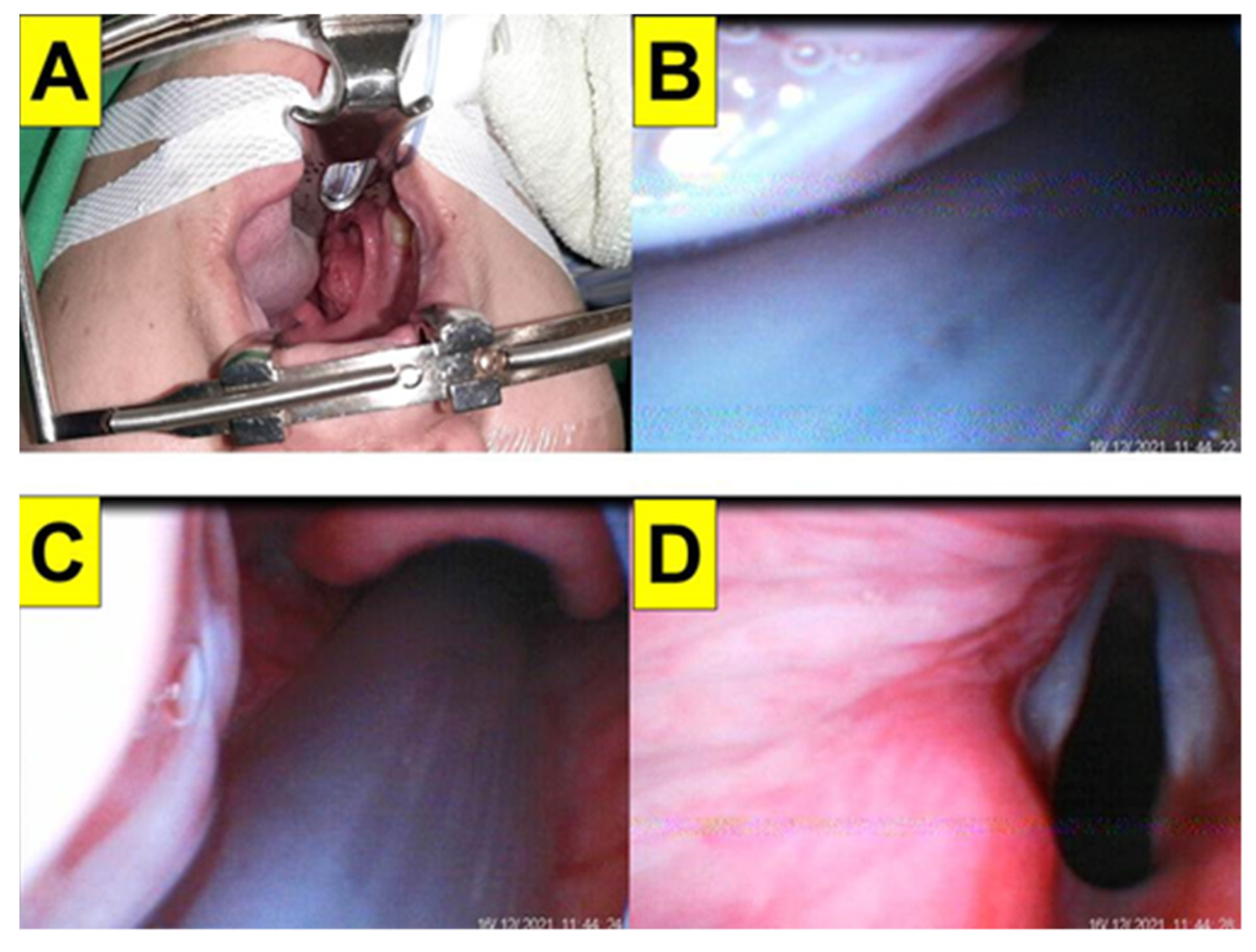
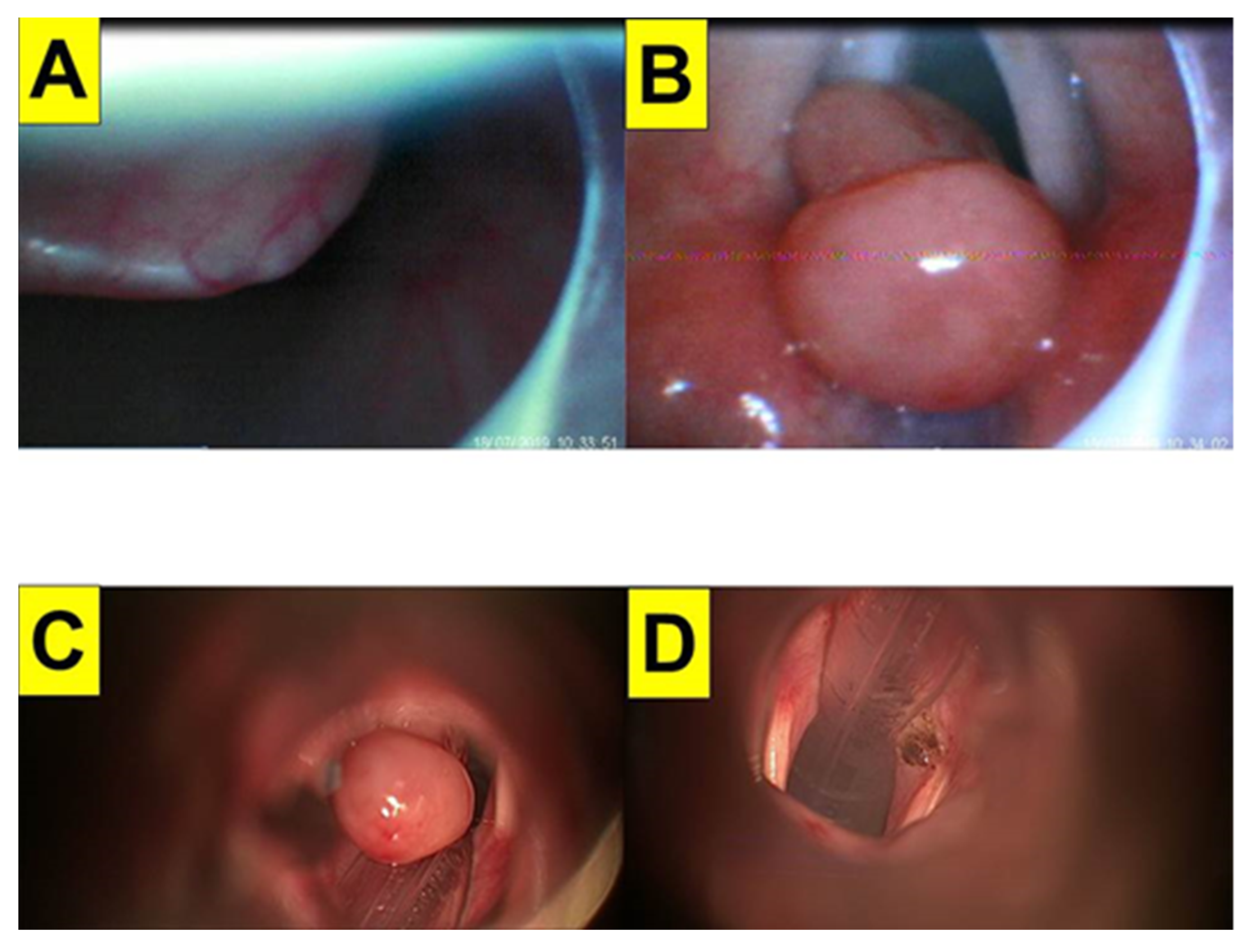
2.2. Case 2: Enlarged Palatine Tonsils
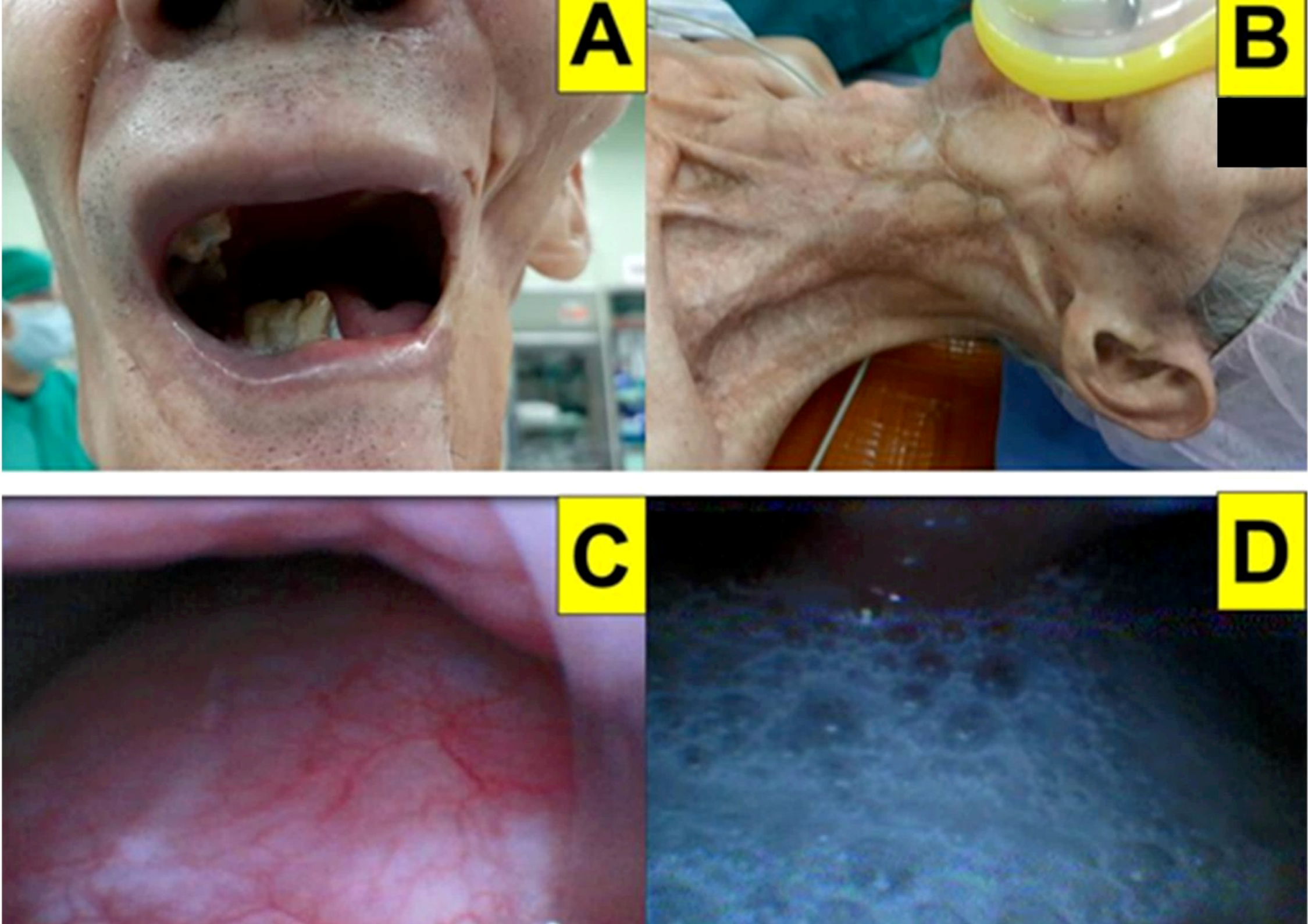
2.3. Case 3: Lower Gum Carcinoma with Neck Radiation Fibrosis
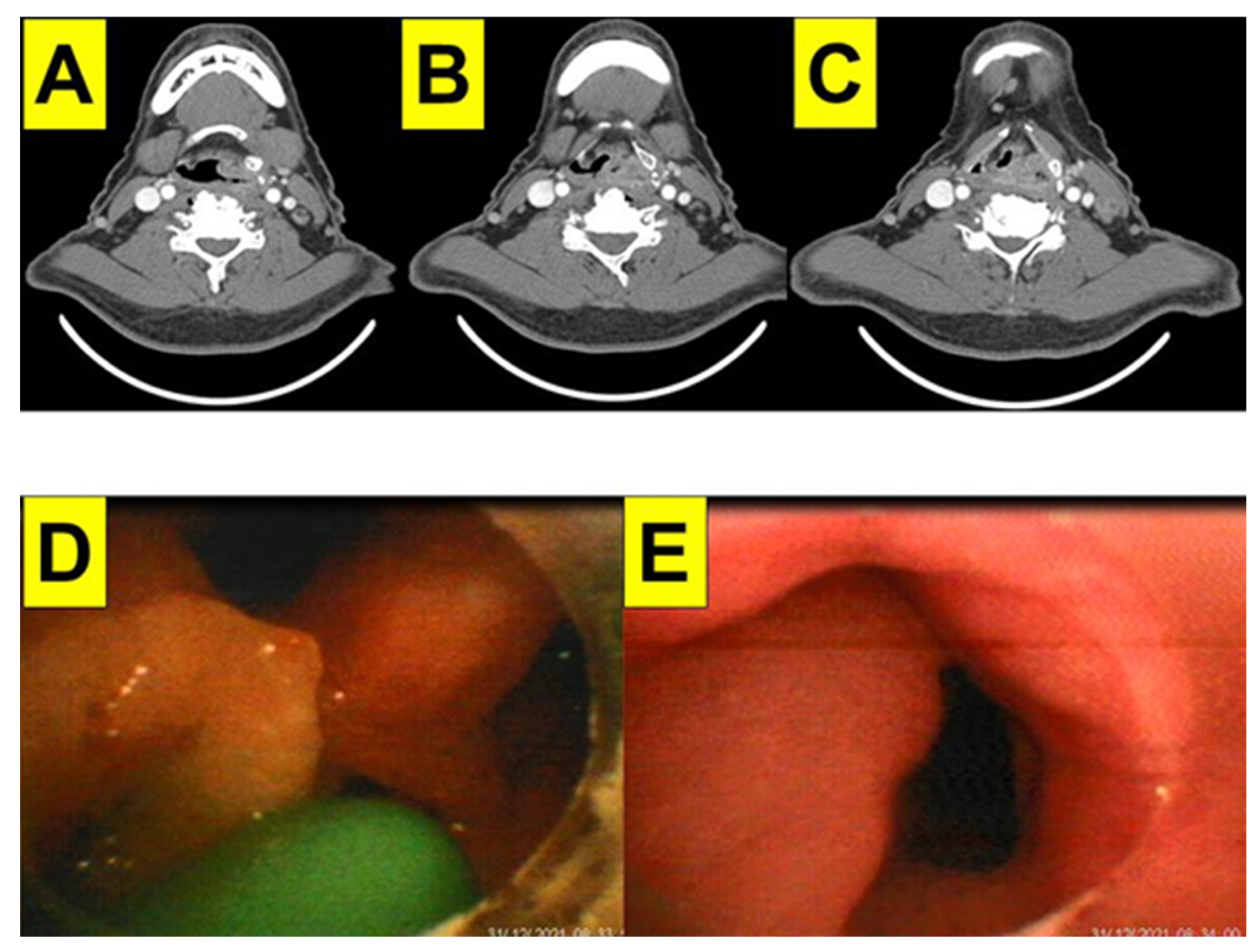
2.4. Case 4: Hypopharyngeal Cancer
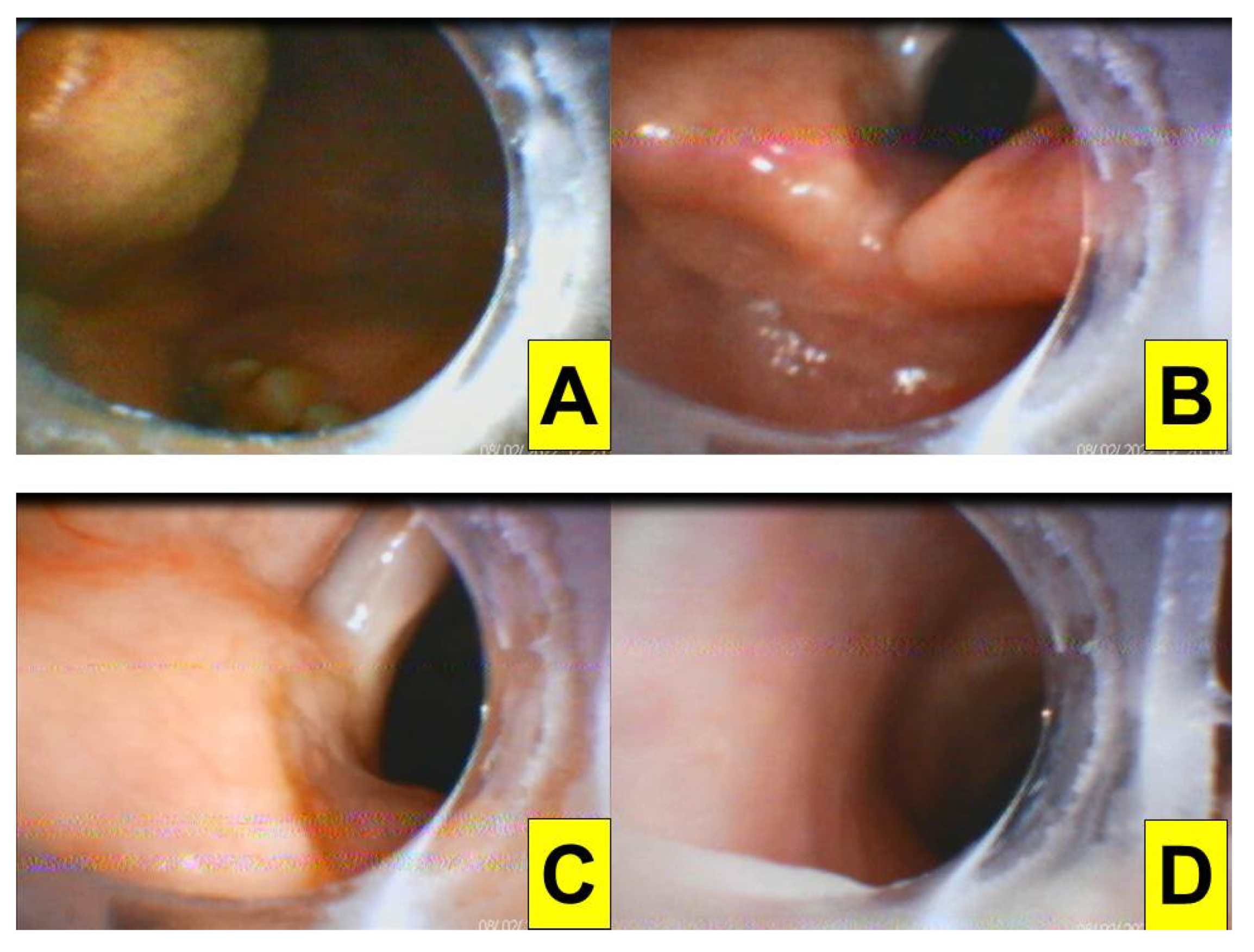
2.5. Case 5: Vocal Cord Granuloma
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benumof, J.L. Management of the difficult adult airway. With special emphasis on awake tracheal intubation. Anesthesiology 1991, 75, 1087–1110. [Google Scholar] [PubMed]
- Mort, T.C. Emergency tracheal intubation: Complications associated with repeated laryngoscopic attempts. Anesth. Analg. 2004, 99, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology 2022, 136, 31–81. [Google Scholar]
- Law, J.A.; Duggan, L.V.; Asselin, M.; Baker, P.; Crosby, E.; Downey, A.; Hung, O.R.; Jones, P.M.; Lemay, F.; Noppens, R.; et al. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: Part 1. Difficult airway management encountered in an unconscious patient. Can. J. Anaesth. 2021, 68, 1373–1404. [Google Scholar] [PubMed]
- Law, J.A.; Duggan, L.V.; Asselin, M.; Baker, P.; Crosby, E.; Downey, A.; Hung, O.R.; Kovacs, G.; Lemay, F.; Noppens, R.; et al. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: Part 2. Planning and implementing safe management of the patient with an anticipated difficult airway. Can. J. Anaesth. 2021, 68, 1405–1436. [Google Scholar] [PubMed]
- Healy, D.W.; Maties, O.; Hovord, D.; Kheterpal, S. A systematic review of the role of videolaryngoscopy in successful orotracheal intubation. BMC Anesthesiol. 2012, 12, 32. [Google Scholar] [CrossRef] [Green Version]
- Matek, J.; Kolek, F.; Klementova, O.; Michalek, P.; Vymazal, T. Optical devices in tracheal intubation-State of the art in 2020. Diagnostics 2021, 11, 575. [Google Scholar] [CrossRef]
- Shikani, A.H. New “seeing” stylet-scope and method for the management of the difficult airway. Otolaryngol. Head Neck Surg. 1999, 120, 113–116. [Google Scholar] [CrossRef]
- Levitan, R.M. Design rationale and intended use of a short optical stylet for routine fiberoptic augmentation of emergency laryngoscopy. Am. J. Emerg. Med. 2006, 24, 490–495. [Google Scholar] [CrossRef]
- Cheng, T.; Wang, L.K.; Wu, H.Y.; Yang, X.D.; Zhang, X.; Jiao, L. Shikani optical stylet for awake nasal intubation in patients undergoing head and neck surgery. Laryngoscope 2021, 131, 319–325. [Google Scholar] [CrossRef]
- Fan, H.; Cao, H.; Sun, Y.; Chen, K.; Diao, Y.; Zhou, N.; Yao, G.; Zhou, J.; Zhang, T. Endotracheal intubation in elective cervical surgery: A randomized, controlled, assessor-blinded study. Medicine 2017, 96, e7817. [Google Scholar] [CrossRef] [PubMed]
- Lovich-Sapola, J.; Johnson, F.; Smith, C.E. Anesthetic considerations for oral, maxillofacial, and neck trauma. Otolaryngol. Clin. N. Am. 2019, 52, 1019–1035. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Feng, L.; Lewis, C.M. A data review of airway management in patients with oral cavity or oropharyngeal cancer: A single-institution experience. BMC Anesthesiol. 2019, 19, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Gupta, A.; Sarma, R.; Batra, A.; Madan, K. Video laryngoscopy vs. direct laryngoscopy for nasotracheal intubation in oromaxillofacial surgery: A systematic review and meta-analysis of randomized controlled trials. Korean J. Anesthesiol. 2021, 74, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Paolini, J.B.; Donati, F.; Drolet, P. Review article: Video-laryngoscopy: Another tool for difficult intubation or a new paradigm in airway management? Can. J. Anaesth. 2013, 60, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Eskander, A.; de Almeida, J.R.; Irish, J.C. Acute upper airway obstruction. N. Engl. J. Med. 2019, 381, 1940–1949. [Google Scholar] [CrossRef]
- Waberski, A.T.; Espinel, A.G.; Reddy, S.K. Anesthesia safety in otolaryngology. Otolaryngol. Clin. N. Am. 2019, 52, 63–73. [Google Scholar] [CrossRef]
- Ravindran, B.; Korandiarkunnel Paul, F.; Vyakarnam, P. Acute upper airway obstruction due to tonsillitis necessitating emergency cricothyroidotomy. BMJ Case Rep. 2021, 14, e242500. [Google Scholar] [CrossRef]
- Kim, S.M.; Kim, H.J. Successful advancement of endotracheal tube with combined fiberoptic bronchoscopy and videolaryngoscopy in a patient with a huge goiter. SAGE Open Med. Case Rep. 2020, 8, 2050313X20923232. [Google Scholar] [CrossRef]
- Huitink, J.M.; Zijp, L. Laryngeal radiation fibrosis: A case of failed awake flexible fibreoptic intubation. Case Rep. Anesthesiol. 2011, 2011, 878910. [Google Scholar] [CrossRef] [Green Version]
- Moorthy, S.S.; Gupta, S.; Laurent, B.; Weisberger, E.C. Management of airway in patients with laryngeal tumors. J. Clin. Anesth. 2005, 17, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Nakahira, J.; Sawai, T.; Matsunami, S.; Minami, T. Worst-case scenario intubation of laryngeal granuloma: A case report. BMC Res. Notes 2014, 7, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmeyr, R.; Llewellyn, R.; Fagan, J.J. Multidisciplinary difficult airway challenges: Perioperative management of glottic and supraglottic tumors. Oper. Tech. Otolaryngol. Head Neck Surg. 2020, 31, 120–127. [Google Scholar] [CrossRef]
- Clarke, M.B.; Forster, P.; Cook, T.M. Airway management for tonsillectomy: A national survey of UK practice. Br. J. Anaesth. 2007, 99, 425–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, S.W.; McCahon, R.A. Management of the airway in maxillofacial surgery: Part 1. Br. J. Oral Maxillofac. Surg. 2018, 56, 463–468. [Google Scholar] [CrossRef]
- Shindo, Y.; Toda, S.; Kido, K.; Masaki, E. Massive ameloblastoma: A case report of difficult fiberoptic intubation. Ann. Med. Surg. 2018, 32, 6–9. [Google Scholar] [CrossRef]
- Asbjørnsen, H.; Kuwelker, M.; Søfteland, E. A case of unexpected difficult airway due to lingual tonsil hypertrophy. Acta Anaesthesiol. Scand. 2008, 52, 310–312. [Google Scholar] [CrossRef]
- Zhang, X.; Cavus, O.; Zhou, Y.; Dusitkasem, S. Airway management during anesthetic induction of secondary laryngectomy for recurrent laryngeal cancer: Three cases of report and analysis. Case Rep. Front. Med. 2018, 5, 264. [Google Scholar] [CrossRef] [Green Version]
- Pieters, B.M.A.; Maas, E.H.A.; Knape, J.T.A.; van Zundert, A.A.J. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: A systematic review and meta-analysis. Anaesthesia 2017, 72, 1532–1541. [Google Scholar] [CrossRef] [Green Version]
- Aziz, M.F.; Dillman, D.; Fu, R.; Brambrink, A.M. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology 2012, 116, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Turkstra, T.P.; Pelz, D.M.; Shaikh, A.A.; Craen, R.A. Cervical spine motion: A fluoroscopic comparison of Shikani Optical Stylet vs Macintosh laryngoscope. Can. J. Anaesth. 2007, 54, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, D.; Tong, S.Y.; Jin, J.H.; Tang, G.Z.; Sui, J.H.; Wei, L.X.; Deng, X.M. Shikani Optical Stylet-guided intubation via the intubating laryngeal airway in patients with scar contracture of the face and neck. Chin. Med. Sci. J. 2013, 28, 195–200. [Google Scholar] [CrossRef]
- Yang, M.; Kim, J.A.; Ahn, H.J.; Choi, J.W.; Kim, D.K.; Cho, E.A. Double-lumen tube tracheal intubation using a rigid video-stylet: A randomized controlled comparison with the Macintosh laryngoscope. Br. J. Anaesth. 2013, 111, 990–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Li, X.X.; Guo, X.Y.; Jun Wang, J. Shikani Optical Stylet versus Macintosh laryngoscope for intubation in patients undergoing surgery for cervical spondylosis: A randomized controlled trial. Chin. Med. J. 2017, 130, 297–302. [Google Scholar] [CrossRef]
- Wang, Y.H.; Xue, F.S.; Li, H.X.; Liu, Y.Y. Comparing Shikani Optical Stylet and Macintosh laryngoscope for orotracheal intubation. Chin. Med. J. 2017, 130, 1629–1630. [Google Scholar] [CrossRef]
- Kucaba, G.; Muster, M.; Filip, D.; Horeczy, B.; Szarpak, L.; Woloszczuk-Gebicka, B. Pressure on the incisors during direct laryngoscopy and intubation using the Shikani Optical Stylet™. Am. J. Emerg. Med. 2017, 35, 1370–1372. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, M.; Wang, Q.; Liu, C. Comparison of the Shikani Optical Stylet and Macintosh laryngoscope for orotracheal intubation with topical anesthesia in critically ill patients. Clin. Med. Res. 2018, 7, 84–91. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Y.; Liu, Z.; Zhang, Q.; Wu, W.; Zheng, Z.; Zhang, Z. Application of second-generation Shikani optical stylet in critically ill patients undergoing cerebral aneurysm embolization. J. Int. Med. Res. 2019, 47, 1565–1572. [Google Scholar] [CrossRef] [Green Version]
- Tuzuner-Oncul, A.M.; Kucukyavuz, Z. Prevalence and prediction of difficult intubation in maxillofacial surgery patients. J. Oral Maxillofac. Surg. 2008, 66, 1652–1658. [Google Scholar] [CrossRef]
- Mahrous, R.S.S.; Ahmed, A.M.M. The Shikani Optical Stylet as an alternative to awake fiberoptic intubation in patients at risk of secondary cervical spine injury: A randomized controlled trial. J. Neurosurg. Anesthesiol. 2018, 30, 354–358. [Google Scholar] [CrossRef]
- Ma, Y.; Wang, Y.; Shi, P.; Cao, X.; Ge, S. Ultrasound-guided versus Shikani optical stylet-aided tracheal intubation: A prospective randomized study. BMC Anesthesiol. 2020, 20, 221. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yue, H.; Li, J. Comparison of three tracheal intubation techniques in thyroid tumor patients with a difficult airway: A randomized controlled trial. Med. Princ. Pract. 2014, 23, 448–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, N.; Li, M.; Shi, S.; Li, T.Z.; Zhang, B.X. Shikani™ Seeing Optical Stylet-aided tracheal intubation in patients with a large epiglottic cyst. Chin. Med. J. 2011, 124, 2795–2798. [Google Scholar] [PubMed]
- Seo, H.; Lee, G.; Ha, S.I.; Song, J.G. An awake double lumen endotracheal tube intubation using the Clarus Video System in a patient with an epiglottic cyst: A case report. Korean J. Anesthesiol. 2014, 66, 157. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | |
|---|---|---|---|---|---|
| First-attempt success | Yes | Yes | Yes | Yes | Yes |
| Overall success rate | 100% | ||||
| Laryngeal & glottic view | Full | Full | Full | Full | Full |
| Time to intubate (from lip to trachea) | 24 s | 12 s | 25 s | 26 s | 50 s |
| Degree of difficulty for intubation | Easy | Easy | Easy | Easy | Easy |
| Required additional external maneuvers | No | No | No | No | No |
| Complications (tissue injuries, autonomic overstimulation, hypoxia) | No | No | No | No | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsay, P.-J.; Yang, C.-P.; Luk, H.-N.; Qu, J.Z.; Shikani, A. Video-Assisted Intubating Stylet Technique for Difficult Intubation: A Case Series Report. Healthcare 2022, 10, 741. https://doi.org/10.3390/healthcare10040741
Tsay P-J, Yang C-P, Luk H-N, Qu JZ, Shikani A. Video-Assisted Intubating Stylet Technique for Difficult Intubation: A Case Series Report. Healthcare. 2022; 10(4):741. https://doi.org/10.3390/healthcare10040741
Chicago/Turabian StyleTsay, Pei-Jiuan, Chih-Pin Yang, Hsiang-Ning Luk, Jason Zhensheng Qu, and Alan Shikani. 2022. "Video-Assisted Intubating Stylet Technique for Difficult Intubation: A Case Series Report" Healthcare 10, no. 4: 741. https://doi.org/10.3390/healthcare10040741