


Systematic Review of Evening Primrose (Oenothera biennis) Preparations for the Facilitation of Parturition
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
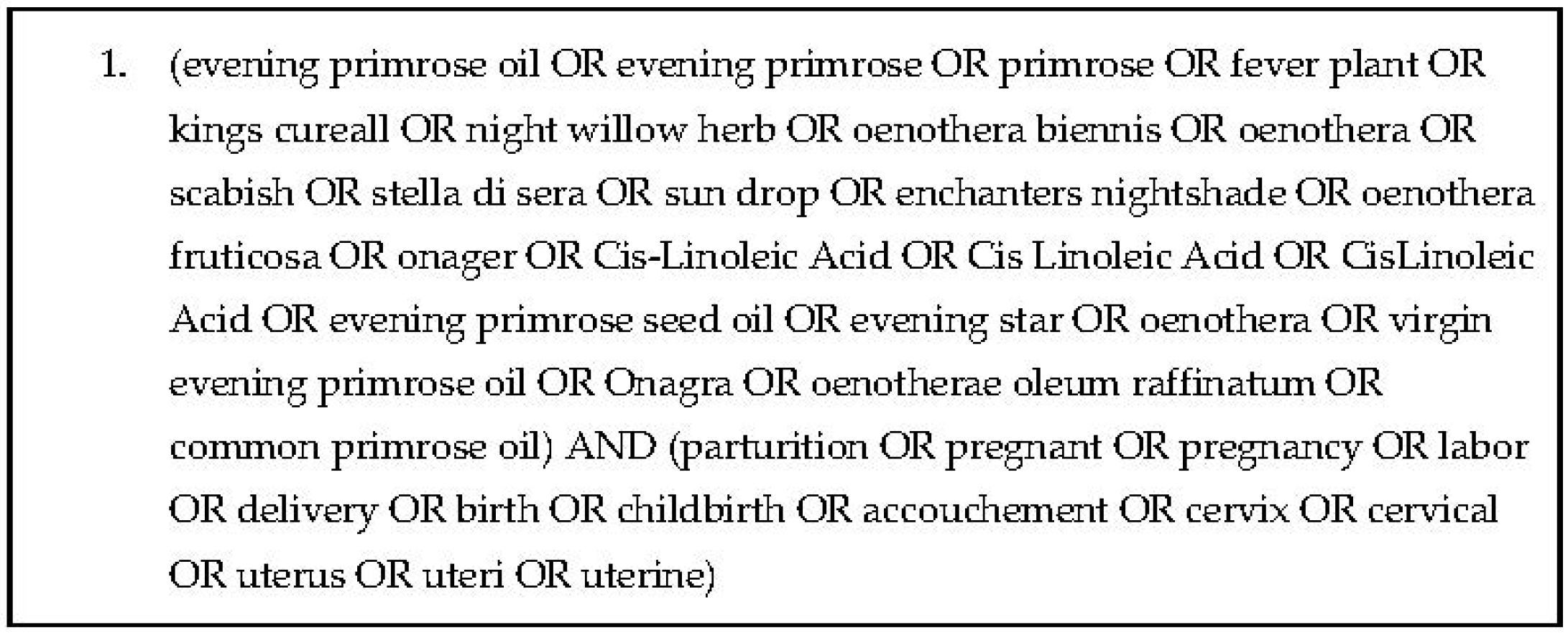
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Data Synthesis
2.5. Risk-of-Bias Assessment
3. Results
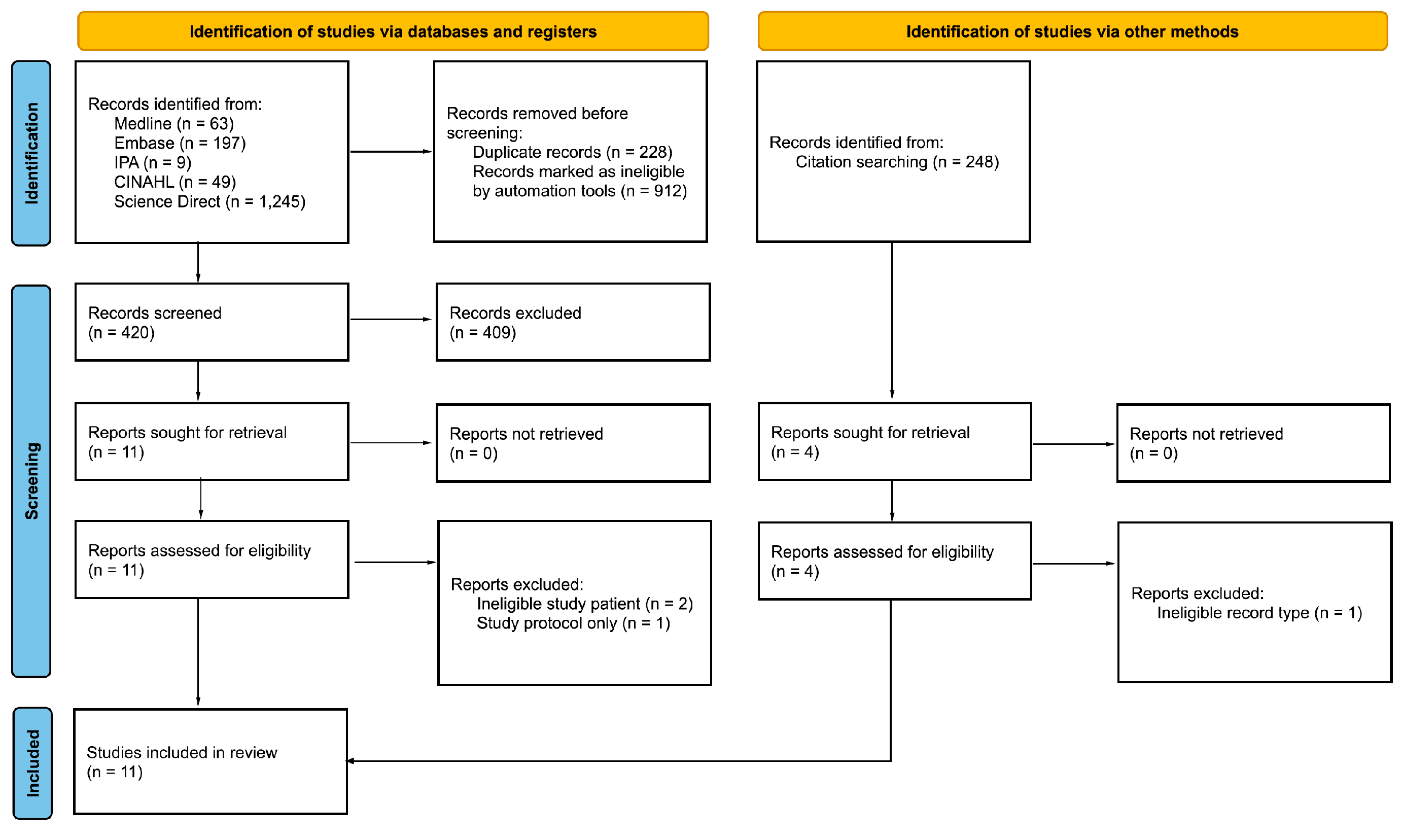
3.1. Search Results
3.2. Risk-of-Bias Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K. Births: Final data for 2019. Natl. Vital. Stat. Rep. 2021, 70, 1–50. [Google Scholar] [PubMed]
- ACOG. ACOG practice bulletin No. 146: Management of late-term and postterm pregnancies. Obs. Gynecol. 2014, 124, 390–396. [Google Scholar] [CrossRef] [PubMed]
- ACOG. ACOG practice bulletin No. 107: Induction of labor. Obs. Gynecol. 2009, 114, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Grobman, W.A.; Rice, M.M.; Reddy, U.M.; Tita, A.T.; Silver, R.M.; Mallet, G.; Hill, K.; Thom, E.A.; El-Sayed, Y.Y.; Perez-Delboy, A.; et al. Labor induction versus expectant Management in low-risk nulliparous women. N. Engl. J. Med. 2018, 379, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.R. Cervical ripening and labor induction and augmentation, 5th edition. J. Obs. Gynecol. Neonatal Nurs. 2020, 24 (Suppl. S49), S1–S41. [Google Scholar]
- Bishop, E.H. Pelvic scoring for elective induction. Obs. Gynecol. 1964, 24, 266–268. [Google Scholar]
- Gibson, K.S.; Waters, T.P. Measures of success: Prediction of successful labor induction. Semin. Perinatol. 2015, 39, 475–482. [Google Scholar] [CrossRef]
- Tenore, J. Methods for cervical ripening and induction of labor. Am. Fam. Physician 2003, 67, 2123–2128. [Google Scholar]
- McFarlin, B.; Gibson, M.H.; O’Rear, J.; Harman, P. A national survey of herbal preparation use by nurse-midwives for labor stimulation review of the literature and recommendations for practice. J. Midwifery Women’s Health 1999, 44, 205–216. [Google Scholar] [CrossRef]
- Timoszuk, M.; Bielawska, K.; Skrzydlewska, E. Evening primrose (Oenothera biennis) biological activity dependent on chemical composition. Antioxidants 2018, 7, 108–119. [Google Scholar] [CrossRef] [Green Version]
- Beites, C.L.; Morgan, L. Evening primrose oil for cervical ripening. Can. J. Comp. Med. 2014, 13, 47–49. [Google Scholar]
- Degolier, T.; Lyle, C.; Ortmann, A. Aqueous extracts from evening primrose seeds (Oenothera biennis) contract isolated uterine tissues but have no effect on isolated cervical tissues. Int. J. Herb. Med. 2017, 5, 10–16. [Google Scholar]
- Leaver, H.; Lytton, F.; Dyson, H.; Watson, M.L.; Mellor, D.J. The effect of dietary ω3 and ω6 polyunsaturated fatty acids on gestation, parturition and prostaglandin E2 in intrauterine tissues and the kidney. Prog. Lipid Res. 1986, 25, 143–146. [Google Scholar] [CrossRef]
- Guivernau, M.; Meza, N.; Barja, P.; Roman, O. Clinical and experimental study on the long-term effect of dietary gamma-linolenic acid on plasma lipids, platelet aggregation, thromboxane formation, and prostacyclin production. Prostaglandins Leukot. Essent. Fat. Acids 1994, 51, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Bayles, B. Evening primrose oil. Am. Fam. Physician 2009, 80, 1405–1408. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 372, 71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.I.; Elbers, R.G.; Blencowe, N.S.; Bourton, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. Br. Med. J. 2019, 366, 4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. Br. Med. J. 2016, 355, 4919. [Google Scholar] [CrossRef] [Green Version]
- Dove, D.; Johnson, P. Oral evening primrose oil: Its effect on length of pregnancy and selected intrapartum outcomes in low-risk nulliparous women. J. Nurse Midwifery 1999, 44, 320–324. [Google Scholar] [CrossRef]
- Wedig, K.; Whitsett, J.A. Down the primrose path: Petechiae in a neonate exposed to herbal remedy for labor parturition. J. Pediatr. 2008, 52, 140. [Google Scholar] [CrossRef]
- Zahran, K.; Elsayh, K.; Makhlouf, E.; Abd-Elaleem, J. Evening primrose oil for induction of labour in postdate pregnancies—A randomized placebo controlled clinical trial. J. Egypt Soc. Gynaecol. Obs. 2009, 35, 495–499. [Google Scholar]
- Jahdi, F.; Kalati, M.; Kashanian, M.; Naseri, M.; Haghani, H. Effect of oral evening primrose capsules on ripening of the cervix in nulliparous Iranian pregnant women (a randomized trial). Acta Med. Mediterr. 2016, 32, 1273–1279. [Google Scholar]
- Diansuy, N.N.; Aguilar, A.S. The effectiveness of evening primrose oil gel capsule as a cervical ripening agent during labor induction as measured by bishop score on term singleton pregnant patients. Philipp. J. Obstet. Gynecol. 2017, 41, 1–4. [Google Scholar]
- Kalati, M.; Kashanian, M.; Jahdi, F.; Naseri, M.; Haghani, H.; Sheikhansari, N. Evening primrose oil and labour, is it effective? A randomised clinical trial. Obstet. Gynecol. 2018, 38, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Najafi, M.; Loripoor, M.; Saghafi, Z.; Kazemi, M. The effect of vaginal evening primrose on the Bishop score of term nulliparous women. Nurs. Pract. Today 2019, 6, 202–211. [Google Scholar] [CrossRef]
- Hashemnejad, M.; Ataei, M.; Modarresi, M.; Forutan, F. Investigating the effect of primrose capsule (primula flower oil) on cervix preparation and commencement of child delivery pains. Rev. Latinoam. 2019, 14, 118–122. [Google Scholar]
- Bahmani, S.; Hesamy, K.; Shahgheibi, S.; Roshani, D.; Shahoei, R. Comparison of the effect of vaginal capsule of evening primrose oil and misoprostol on cervical ripening of nulliparous women with post-term pregnancy. J. Pharm. Res. Int. 2019, 26, 1–9. [Google Scholar] [CrossRef]
- Mirzadeh, N.; Sheikhan, Z.; Simbar, M.; Mehrolhasani, Y.; Saffar, A.; Yeganeh, Z. Comparison effects of vaginal misoprostol with vaginal evening primrose on ripening cervix in nulliparous women. Adv. Nurs. Midwifery 2020, 29, 33–40. [Google Scholar]
- Azad, A.; Pourtaheri, M.; Darsareh, F.; Heidari, S.; Mehrnoush, V. Evening primrose oil for cervical ripening prior to labor induction in post-term pregnancies: A randomized controlled trial. Eur. J. Integr. Med. 2022, 51, 102123. [Google Scholar] [CrossRef]
- Micromedex RED BOOK. Available online: https://www-micromedexsolutions-com (accessed on 6 December 2022).
- Martens-Lobenhoffer, J.; Meyer, F. Pharmacokinetic data of gamma-linolic acid in healthy volunteers after the administration of evening primrose oil (Epogam). Int. J. Clin. Pharmacol. Ther. 1998, 36, 363–366. [Google Scholar]
- Cant, A.; Shay, J.; Horrobin, D.F. The effect of maternal supplementation with linoleic and gamma-linolenic acids on the fat composition and content of human milk: A placebo-controlled trial. J. Nutr. Sci. Viaminol. 1991, 37, 573–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Wider, B.; Shang, H.; Li, X.; Ernst, E. Quality of herbal medicines: Challenges and solutions. Complement. Ther. Med. 2012, 20, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine. Statement on Elective Induction of Labor in Low-Risk Nulliparous Women at Term: The ARRIVE Trial. 2019. Available online: https://www.smfm.org/publications/258-smfm-statement-elective-induction-of-labor-in-low-risk-nulliparous-women-at-term-the-arrive-trial (accessed on 20 October 2022).
- American Society for Reproductive Medicine. Practice Committee Documents. Available online: https://www.asrm.org/news-and-publications/practice-committee-documents (accessed on 20 October 2022).



{kind=link}
{kind=link}
| Authors (Year) | Design (Partici-Pants) | Population, Study Location | Intervention | Control | Duration |
|---|---|---|---|---|---|
| Dove et al. (1999) [19] | Retrospective quasi-experimental study (n = 108) | Peripartum persons, United States | EP 500 mg capsule by mouth 3 times daily for 1 week at 37 weeks gestation, then 500 mg once daily until delivery | No EP | 37 weeks gestation until delivery |
| Wedig et al. (2008) [20] | Case study (n = 1) | 31 year old Female | EP 500 mg 13 capsules total vaginally and orally | N/A | N/A |
| Zahran et al. (2009) [21] | RCT (n = 240) | Peripartum persons, Egypt | EP 1000 mcg capsules by mouth every 12 h for up to 10 days | Placebo | 10 days |
| Jahdi et al. (2016) [22] | RCT (n = 80) | Peripartum persons, Iran | EP 1000 mg capsule by mouth every 12 h for 7 days | Placebo | 7 days |
| Diansuy et al. (2017) [23] | Quasi-experimental study (n = 13) | Peripartum persons, Philippines | EP 1000 mg 2 capsules vaginally once | None | Day of labor |
| Bahmani et al. (2018) [27] | RCT (n = 130) | Peripartum persons, Iran | EP 500 mg capsule vaginally and misoprostol 25 mcg SL if ineffective after 6 h 2 additional doses of each could be given | Misoprostol 25 mcg SL/Placebo | 7 days |
| Kalati et al. (2018) [24] | RCT (n = 80) | Peripartum persons, Iran | EP 1000 mg capsule by mouth twice daily for 7 days | Placebo | 7 days |
| Hashemnajad et al. (2019) [26] | RCT (n = 162) | Peripartum persons, Iran | EP 1000 mg 2 capsules vaginally once | Placebo | Day of labor |
| Najafi et al. (2019) [25] | RCT (n = 86) | Peripartum persons, Iran | EP 1000 mg capsule vaginally once daily from 38 weeks gestation until delivery | Placebo | 38 weeks gestation until delivery |
| Mirzadeh et al. (2020) [28] | RCT (n = 100) | Peripartum persons, Iran | EP 1000 mg capsule vaginally once daily for 7 days | Misoprostol 25 mcg vaginally | 7 days |
| Azad et al. (2022) [29] | RCT (n = 175) | Peripartum persons, Iran | EP 1000 mg (two 500 mg capsules) inserted intravaginally 6 h before labor induction with oxytocin | Placebo | Day of labor |
| Authors (Year) | Mean Bishop Score after Intervention | Mean Time in 1st Stage of Labor (Min) | Mean Time in 2nd Stage of Labor (Min) | Mean Time in 3rd Stage of Labor (Min) | Mean Total Time in Labor (Hours) |
|---|---|---|---|---|---|
| Dove et al. (1999) [19] | NR | NR | NR | NR | EP: 15.66 ± 10.27 Placebo: 12.67 ± 6.15 (p = 0.002) |
| Zahran et al. (2009) [21] | EP (induced labor onset): 6.8 ± 1.4 Placebo (induced labor onset): 6.6 ± 1.3 p > 0.05 EP (spontaneous labor onset): 8.4 ± 2.2 Placebo (spontaneous labor onset): 7.4 ± 2.0 p > 0.05 | NR | NR | NR | EP (induced labor): 14.2 ± 3.9 Placebo (induced labor): 17.8 ± 3.2 p > 0.05 EP (spontaneous labor): 8.2 ± 2.9 Placebo (spontaneous labor): 10.0 ± 3.5 p < 0.05 |
| Jahdi et al. (2016) [22] | EP: 3.60 ± 1.75 Placebo: 4.35 ± 2.34 (p = 0.431) | NR | NR | NR | NR |
| Diansuy et al. (2017) [23] | Improvement in Bishop score (n = 11) Score of 4 or higher (n = 4) | NR | NR | NR | NR |
| Bahmani et al. (2018) [27] | EP and misoprostol: 5.08 ± 1.62 Placebo and misoprostol: 3.08 ± 1.72 (p < 0.05) | NR | NR | NR | NR |
| Kalati et al. (2018) [24] | EP: 3.60 ± 1.75 Placebo: 4.35 ± 2.34 (p = 0.110) | EP: 524.48 ± 240.21 Placebo: 530.62 ± 223.37 (p = 0.906) | EP: 45.75 ± 31.71 Placebo: 57.37 ± 33.12 (p = 0.113) | EP: 8.12 ± 5.27 Placebo: 7.50 ± 3.39 (p = 0.530) | EP: 9.63 ± 4.62 Placebo: 9.92 ± 4.33 |
| Najafi et al. (2019) [25] | EP: 5.93 ± 2.42 Placebo: 2.81 ± 2.02 (p = 0.001) | EP: 283.55 ± 297.41 Placebo: 525.95 ± 306.95 (p = 0.006) | EP: 249.55 ± 131.27 Placebo: 226.52 ± 132.53 (p = 0.52) | EP: 54.7 ± 36.11 Placebo: 64.75 ± 43.63 (p = 0.36) | EP: 9.79 ± 7.75 Placebo: 13.6 ± 8.05 |
| Mirzadeh et al. (2020) [28] | EP: 5.38 ± 0.93 Misoprostol: 5.19 ± 1.114 (p = 0.272) | NR | NR | NR | NR |
| Azad et al. (2022) [29] | EP: 6.96 ± 0.18 Placebo: 3.67 ± 0.25 | EP: 220.2 ± 64.8 Placebo: 205.2 ± 69.6 (p = 0.244) | EP: 438.6 ± 127.8 Placebo: 588.6 ± 64.8 (p = 0.031) | EP: 68.31 ± 12.13 Placebo: 70.31 ± 11.03 (p = 0.531) | EP: 726.6 ± 67.8 Placebo: 864 ± 48 (p = 0.036) |
| Authors (Year) | Safety Results |
|---|---|
| Wedig et al. (2008) [20] | Newborn had diffuse ecchymoses and petechiae on trunk, extremities, and face |
| Zahran et al. (2009) [21] | Diarrhea (EP: n = 5; placebo: n = 5; p = NS) Nausea/vomiting (EP: n = 15; placebo: n = 12; p = NS) Meconium aspiration (EP: n = 3; placebo: n = 4; p = NS) Apgar score < 7 at 1 min (EP: n = 16; placebo: n = 14; p = NS) Apgar score < 7 at 5 min (EP: n = 5; placebo: n = 4; p = NS) NICU admissions (EP: n = 4; placebo: n = 2; p = NS) |
| Jahdi et al. (2016) [22] | Increased blood pressure (placebo: n = 1) Decreased heart rate and bleeding (placebo: n = 3) |
| Kalati et al. (2018) [24] | No adverse events were observed or reported in either group |
| Hashemnejad et al. (2019) [26] | No adverse events were observed or reported in either group |
| Najafi et al. (2019) [25] | Abnormal hemorrhage during first 2 h after delivery EP: n = 3 (7%) Placebo: n = 4 (9.5%) (p = 0.66) |
| Mirzadeh et al. (2020) [28] | Pain EP: n = 18 (40%) misoprostol: n = 41 (74.5%) Nausea and vomiting EP: n = 12 (26.7%) misoprostol: n = 36 (65.5%) (p < 0.001) Bleeding at admission EP: n = 5 (11.1%) misoprostol: n = 1 (1.8%) (p < 0.001) |
| Azad et al. (2022) [29] | No adverse events were observed or reported in either group |
| Randomized Controlled Trials | ||||||||
| Authors (Year) | Overall RoB | Randomization | Outcome Deviations | Missing Data | Outcome Measures | Results Selection | - | - |
| Zahran et al. (2009) [21] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Jahdi et al. (2016) [22] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Kalati et al. (2016) [24] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Bahmani et al. (2018) [27] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Hashemnajad et al. (2019) [26] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Najafi et al. (2019) [25] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Mirzadeh et al. (2020) [28] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Azad et al. (2022) [29] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | - | - |
| Non-Randomized Studies | ||||||||
| Authors (Year) | Overall RoB | Participant Selection | Intervention Deviations | Missing Data | Outcome Measures | Results Selection | Intervention Classification | Confounding |
| Dove et al. (1999) [19] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ |
| Diansuy et al. (2017) [23] | ⬤ | ⬤ Favors intervention | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ |
| Case Reports | ||||||||
| Authors (Year) | Overall RoB | Demographics | History | Condition | Outcome Measures | Intervention | Results | Adverse Events |
| Wedig et al. (2008) [20] | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ | ⬤ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hutcherson, T.C.; Cieri-Hutcherson, N.E.; Lycouras, M.M.; Koehler, D.; Mortimer, M.; Schaefer, C.J.; Costa, O.S.; Bohlmann, A.L.; Singhal, M.K. Systematic Review of Evening Primrose (Oenothera biennis) Preparations for the Facilitation of Parturition. Pharmacy 2022, 10, 172. https://doi.org/10.3390/pharmacy10060172
Hutcherson TC, Cieri-Hutcherson NE, Lycouras MM, Koehler D, Mortimer M, Schaefer CJ, Costa OS, Bohlmann AL, Singhal MK. Systematic Review of Evening Primrose (Oenothera biennis) Preparations for the Facilitation of Parturition. Pharmacy. 2022; 10(6):172. https://doi.org/10.3390/pharmacy10060172
Chicago/Turabian StyleHutcherson, Timothy C., Nicole E. Cieri-Hutcherson, Maggie M. Lycouras, Dharmista Koehler, Madison Mortimer, Christina J. Schaefer, Olivia S. Costa, Ashley L. Bohlmann, and Mudit K. Singhal. 2022. "Systematic Review of Evening Primrose (Oenothera biennis) Preparations for the Facilitation of Parturition" Pharmacy 10, no. 6: 172. https://doi.org/10.3390/pharmacy10060172