
Retrospective Study of Appropriate Primary Prevention in Postmenopausal Women Presenting with a Major Adverse Cardiovascular Endpoint (MACE)


Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
2.1. Study Design and Setting
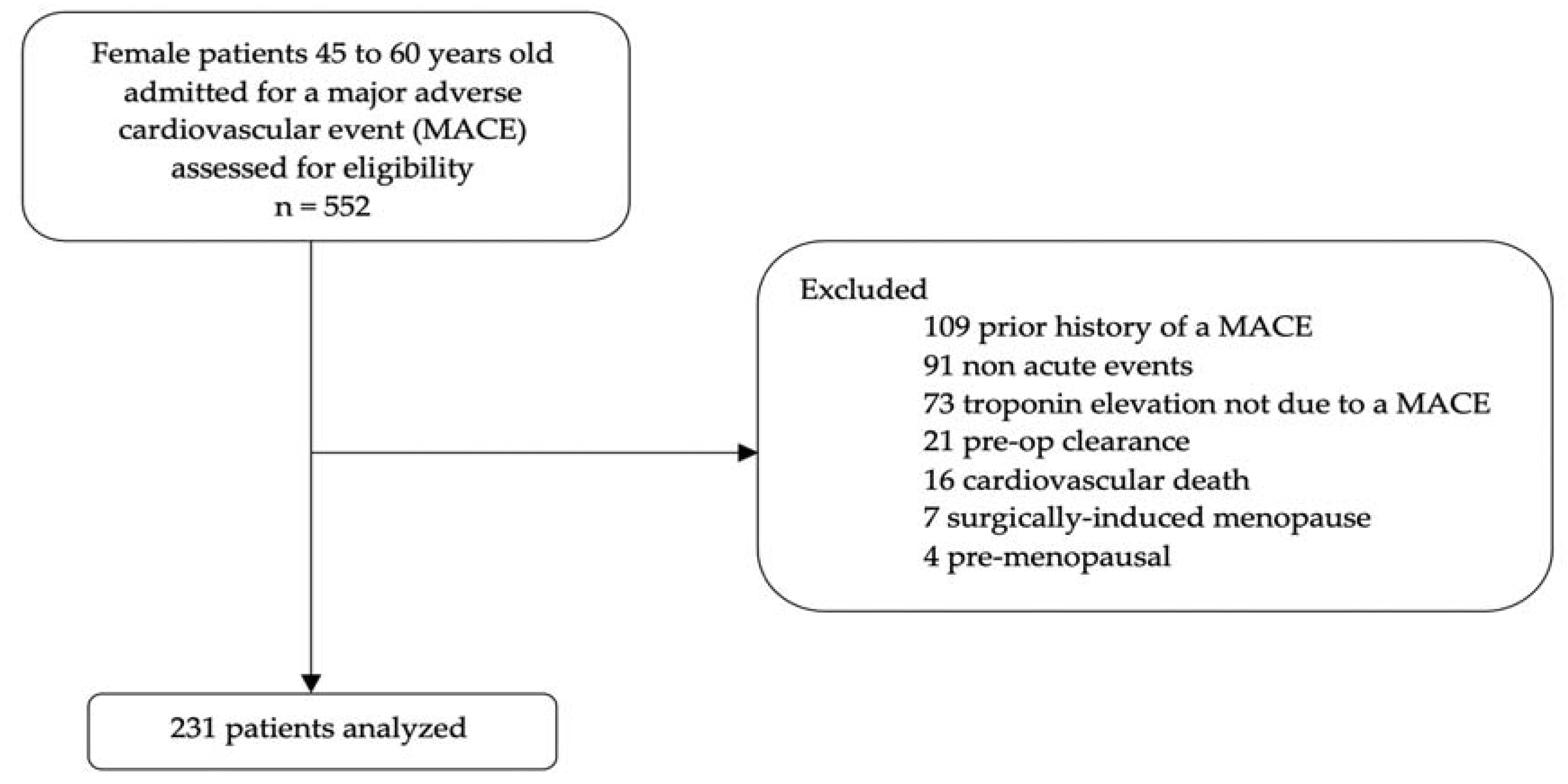
2.2. Participants
2.3. Variables
2.4. Bias
2.5. Study Size
2.6. Statistical Methods
3. Results
3.1. Participants
3.2. Descriptive Data
3.3. Outcome Data
3.4. Other Analyses
4. Discussion
4.1. Key Results and Interpretation
4.2. Limitations
4.3. Generalizability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahmad, F.B.; Cisewski, J.A.; Miniño, A.; Anderson, R.N. Provisional Mortality DataUnited States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guidelines on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; De Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [PubMed]
- Ridker, P.M.; Cook, N.R.; Lee, I.-M.; Gordon, D.; Gaziano, J.M.; Manson, J.E.; Hennekens, C.H.; Buring, J.E. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N. Engl. J. Med. 2005, 352, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Brotons, C.; Coppolecchia, R.; Cricelli, C.; Darius, H.; Gorelick, P.B.; Howard, G.; Pearson, A.T.; Rothwell, P.M.; Ruilope, L.M.; et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): A randomised, double-blind, placebo-controlled trial. Lancet 2018, 392, 1036–1046. [Google Scholar] [CrossRef]
- ASCEND Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K. Effects of aspirin for primary prevention in persons with diabetes mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar] [CrossRef] [PubMed]
- McNeil, J.J.; Wolfe, R.; Woods, R.L.; Tonkin, A.M.; Donnan, G.A.; Nelson, M.R.; Reid, C.M.; Lockery, J.E.; Kirpach, B.; Storey, E.; et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Health Elderly. N. Engl. J. Med. 2018, 379, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Aggarwal, B.; Beckie, T.M.; Hodis, H.N.; Johnson, A.E.; Langer, R.D.; Limacher, M.C.; Manson, J.E.; Stefanick, M.L.; Allison, M.A. American Heart Association Prevention Science Committee of the Council on Epidemiology and Prevention; and Council on Cardiovascular and Stroke Nursing. Menopause transition and cardiovascular disease risk: Implications for timing of early prevention: A scientific statement from the American Heart Association. Circulation 2020, 142, e506–e532. [Google Scholar] [PubMed]
- Attard, R.; Dingli, P.; Doggen, C.J.; Cassar, K.; Farrugia, R.; Wettinger, S.B. The impact of passive and active smoking on inflammation, lipid profile and the risk of myocardial infarction. Open Heart 2017, 4, e000620. [Google Scholar] [CrossRef] [Green Version]
- Jorm, L.R.; Shepherd, L.C.; Rogers, K.D.; Blyth, F.M. Smoking and use of primary care services: Findings from a population-based cohort study linked with administrative claims data. BMC Health Serv. Res. 2012, 12, 263. [Google Scholar] [CrossRef]
- Saba, M.; Diep, J.; Saini, B.; Dhippayom, T. Meta-analysis of the effectiveness of smoking cessation interventions in community pharmacy. J. Clin. Pharm. Ther. 2014, 39, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Berthold, H.K.; Gouni-Berthold, I.; Bohm, M.; Krone, W.; Bestehorn, K.P. Patterns and predictors of statin prescription in patients with type 2 diabetes. Cardiovasc. Diabetol. 2009, 8, 25. [Google Scholar] [CrossRef]
- Santschi, V.; Chiolero, A.; Burnand, B.; Colosimo, A.L.; Paradis, G. Impact of pharmacist care in the management of cardiovascular disease risk factors: A systematic review and meta-analysis of randomized trials. Arch. Intern. Med. 2011, 171, 1441–1453. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Mathews, A.; Swanson, J.; Mhaskar, R.; Mathews, A.; Ayoubi, N.; Mirza, A.S. Aspirin use for cardiovascular disease prevention in the uninsured population. SAGE Open Med. 2020, 8, 2050312120938224. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, S.A.; Cerulli, J.; Zeolla, M.M.; Cottrell, J.S.; Weck, M.B.; Faragon, J.J. Community Pharmacy Target Intervention Program to Improve Aspirin Use in Persons with Diabetes. J. Am. Pharm. Assoc. 2005, 45, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Blenkinsopp, A.; Anderson, C.; Armstrong, M. Systematic review of the effectiveness of community pharmacy-based interventions to reduce risk behaviours and risk factors for coronary heart disease. J. Public Health Med. 2003, 25, 144–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Inappropriate Use of Primary Prevention Therapy | |
|---|---|
| Aspirin | Aspirin use without indication |
| Aspirin with indication but without use | |
| Use of aspirin 325 mg | |
| Statin | Patients with diabetes without statin |
| Patients with diabetes but on low-intensity statin | |
| Statin use without indication | |
| Statin with indication but without use | |
| Antihypertensive | Hypertension treatment without indication |
| Hypertension treatment indicated without use | |
| Non-first line treatment for hypertension |
| Variable | Descriptionn n = 231 * |
|---|---|
| Age, median (years) | 55 |
| Race, n (%) | |
| White | 154/231 (66.7) |
| Black | 52/231 (22.5) |
| Other | 25/231 (10.8) |
| Obese (BMI > 30), n (%) | 129/229 (46.5) |
| Current smokers, n (%) | 120/231 (51.9) |
| Current PCP use, n (%) | 190/231 (82.3) |
| Patients with diabetes, n (%) | 70/231 (30.3) |
| Patients with insurance, n (%) | 206/211 (97.6) |
| Appropriate use (all), n (%) | 86/211 (40.8) |
| Appropriate use of aspirin, n (%) | 144/211 (68.2) |
| Appropriate use of statin, n (%) | 127/217 (58.5) |
| Appropriate use of hypertension treatment, n (%) | 191/231 (82.7) |
| Variable | Appropriate Use n = 86 | Inappropriate Use I n = 125 | p-Value |
|---|---|---|---|
| Age, median (years) n = 231 | 55 | 55 | 0.5722 # |
| Race, n (%) | 0.8922 ^ | ||
| White | 60/86 (69.8) | 83/125 (66.4) | |
| Black | 15/86 (17.4) | 28/125 (22.4) | |
| Other | 11/86 (12.8) | 14/125 (11.2) | |
| Obese patients, n (%) | 40/86 (46.5) | 69/125 (55.2) | 0.2622 * |
| Current smokers, n (%) | 35/86 (40.7) | 72/125 (57.6) | 0.0177 * |
| Current PCP use, n (%) | 76/86 (88.4) | 97/125 (77.6) | 0.0474 * |
| Patients with diabetes, n (%) | 13/86 (15.1) | 48/125 (38.4) | 0.0002 * |
| Patients with insurance, n (%) | 86/86 (100) | 120/125 (96.0) | 0.0811 * |
| Inappropriate Use of Primary Prevention Therapy | Number of Subjects (n, %) |
|---|---|
| Aspirin use without indication | 26 (12.3) |
| Aspirin with indication but without use | 41 (19.4) |
| Use of aspirin 325 mg | 4 (1.9) |
| Patients with diabetes without statin | 38 (17.5) |
| Patients with diabetes but on low-intensity statin | 4 (1.8) |
| Statin use without indication | 13 (6.0) |
| Statin with indication but without use | 35 (16.1) |
| Hypertension treatment without indication | 4 (1.7) |
| Hypertension treatment indicated without use | 34 (14.7) |
| Non-first line treatment for hypertension | 2 (0.9) |
| Variable | Appropriate Use of Aspirin n = 144 | p-Value | Appropriate Use of Statins n = 127 | p-Value | Appropriate HTN Treatment n = 191 | p-Value |
|---|---|---|---|---|---|---|
| Age, median (years) | 56 | 0.8630 # | 55 | 0.4944 # | 56 | 0.5675 # |
| Race, n (%) | 0.1359 ^ | 0.1109 ^ | 0.8256 ^ | |||
| White | 103 (71.5) | 92 (72.4) | 129 (67.5) | |||
| Black | 24 (16.7) | 21 (16.5) | 42 (22.0) | |||
| Other | 17 (11.8) | 14 (11.0) | 20 (10.5) | |||
| Obese patients, n (%) | 71 (49.3) | 0.3394 * | 64 (50.4) | 0.6084 * | 98 (51.3) | 0.7172 * |
| Current smokers, n (%) | 67 (46.5) | 0.0473 * | 53 (41.7) | 0.0005 * | 98 (51.3) | 0.6709 * |
| Patients with diabetes, n (%) | 30 (20.8) | 0.0001 * | 30 (23.6) | 0.0060 * | 53 (27.7) | 0.0649 * |
| Patients with a PCP, n (%) | 117 (81.3) | 0.6815 * | 110 (86.6) | 0.0366 * | 160 (83.8) | 0.1868 * |
| Patients with insurance, n (%) | 143 (99.3) | 0.0361 * | 125 (98.4) | 0.6512 * | 187 (97.9) | 1.0000 * |
| Effect | Point Estimates | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Current smokers | 2.157 | 1.21–3.86 | 0.0096 $ |
| Patients with a PCP | 0.482 | 0.22–1.03 | 0.0608 $ |
| Patients with diabetes | 3.825 | 1.92–7.61 | 0.0001 $ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cieri-Hutcherson, N.E.; Lomakina, A.; Chilbert, M.R. Retrospective Study of Appropriate Primary Prevention in Postmenopausal Women Presenting with a Major Adverse Cardiovascular Endpoint (MACE). Pharmacy 2022, 10, 105. https://doi.org/10.3390/pharmacy10050105
Cieri-Hutcherson NE, Lomakina A, Chilbert MR. Retrospective Study of Appropriate Primary Prevention in Postmenopausal Women Presenting with a Major Adverse Cardiovascular Endpoint (MACE). Pharmacy. 2022; 10(5):105. https://doi.org/10.3390/pharmacy10050105
Chicago/Turabian StyleCieri-Hutcherson, Nicole E., Aleksandra Lomakina, and Maya R. Chilbert. 2022. "Retrospective Study of Appropriate Primary Prevention in Postmenopausal Women Presenting with a Major Adverse Cardiovascular Endpoint (MACE)" Pharmacy 10, no. 5: 105. https://doi.org/10.3390/pharmacy10050105