
A Tale of Two Cities: COVID-19 Vaccine Hesitancy as a Result of Racial, Socioeconomic, Digital, and Partisan Divides
Abstract
:1. Introduction
1.1. Racial Dividesf
1.2. Socioeconomic Divides
1.3. Digital Divides
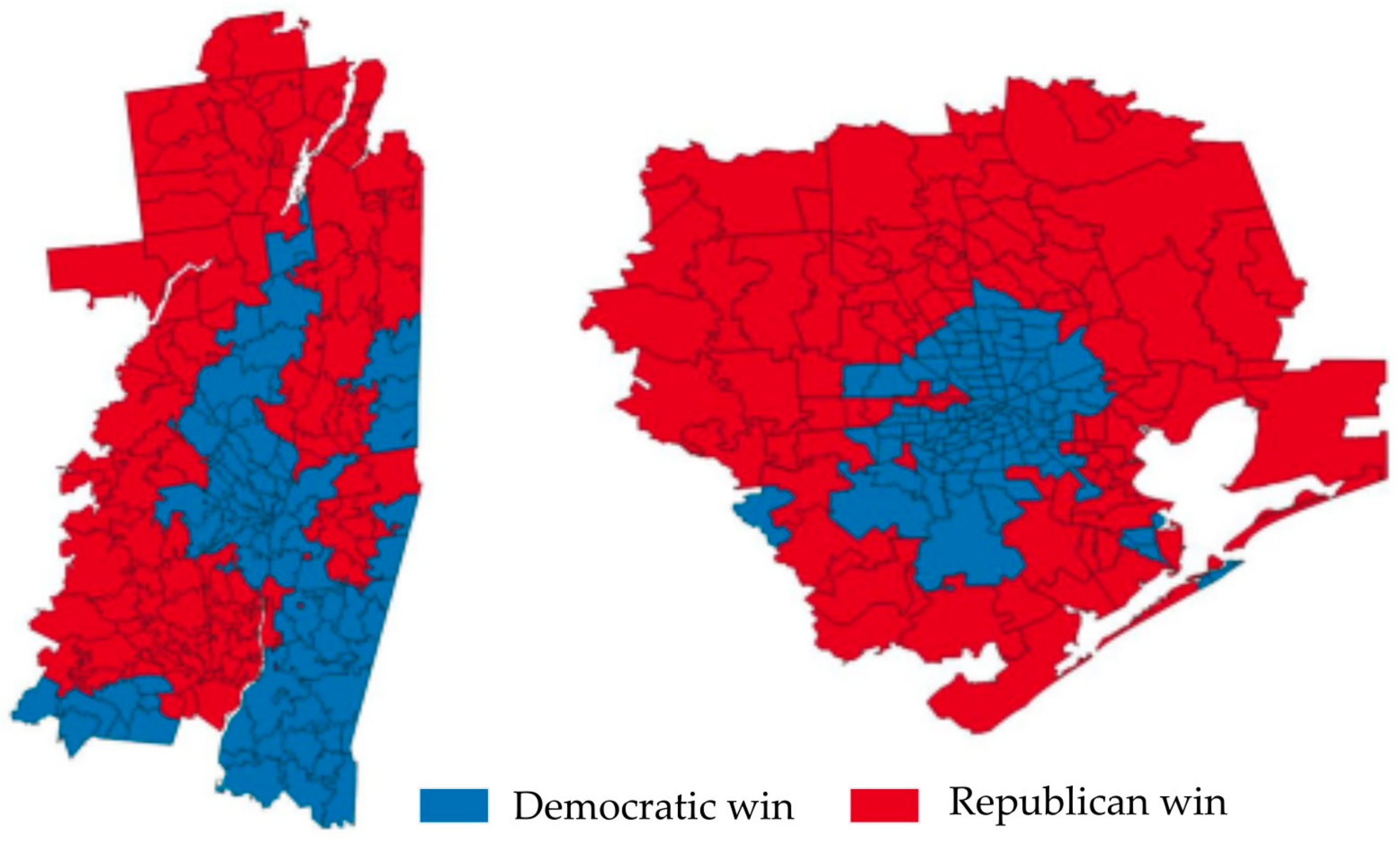
1.4. Partisan Divides
2. Materials and Methods
3. Results
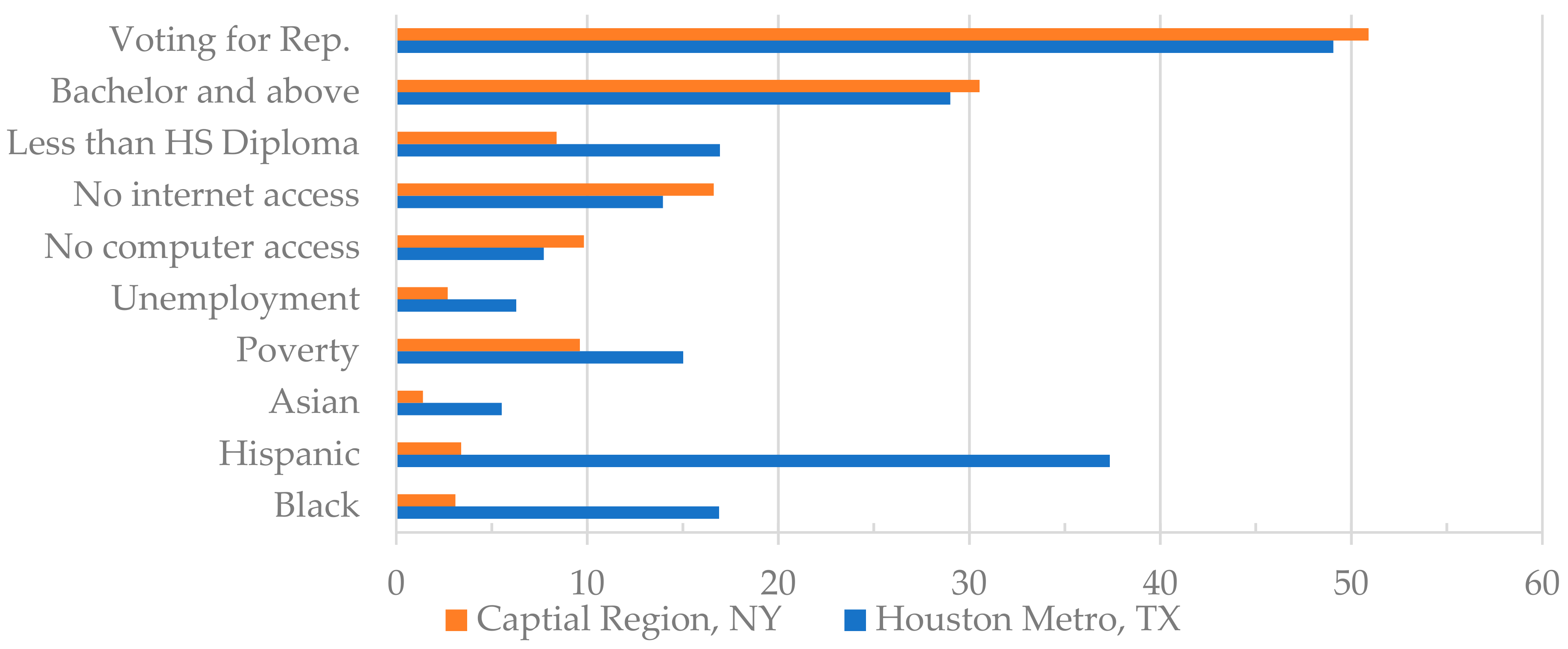
3.1. Disparities between Two Areas
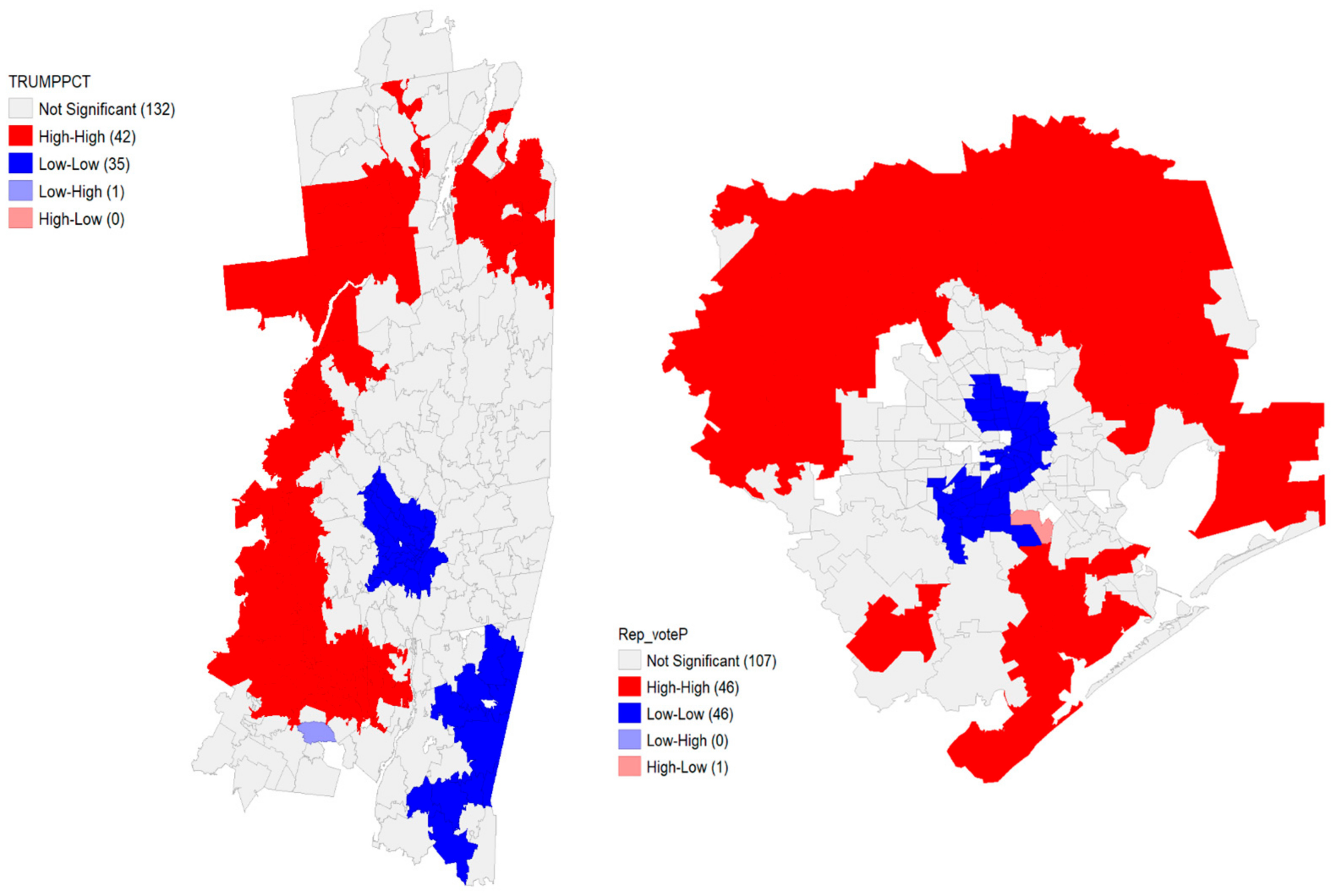
3.2. Disparities within Each Region
3.3. Correlation among Factors
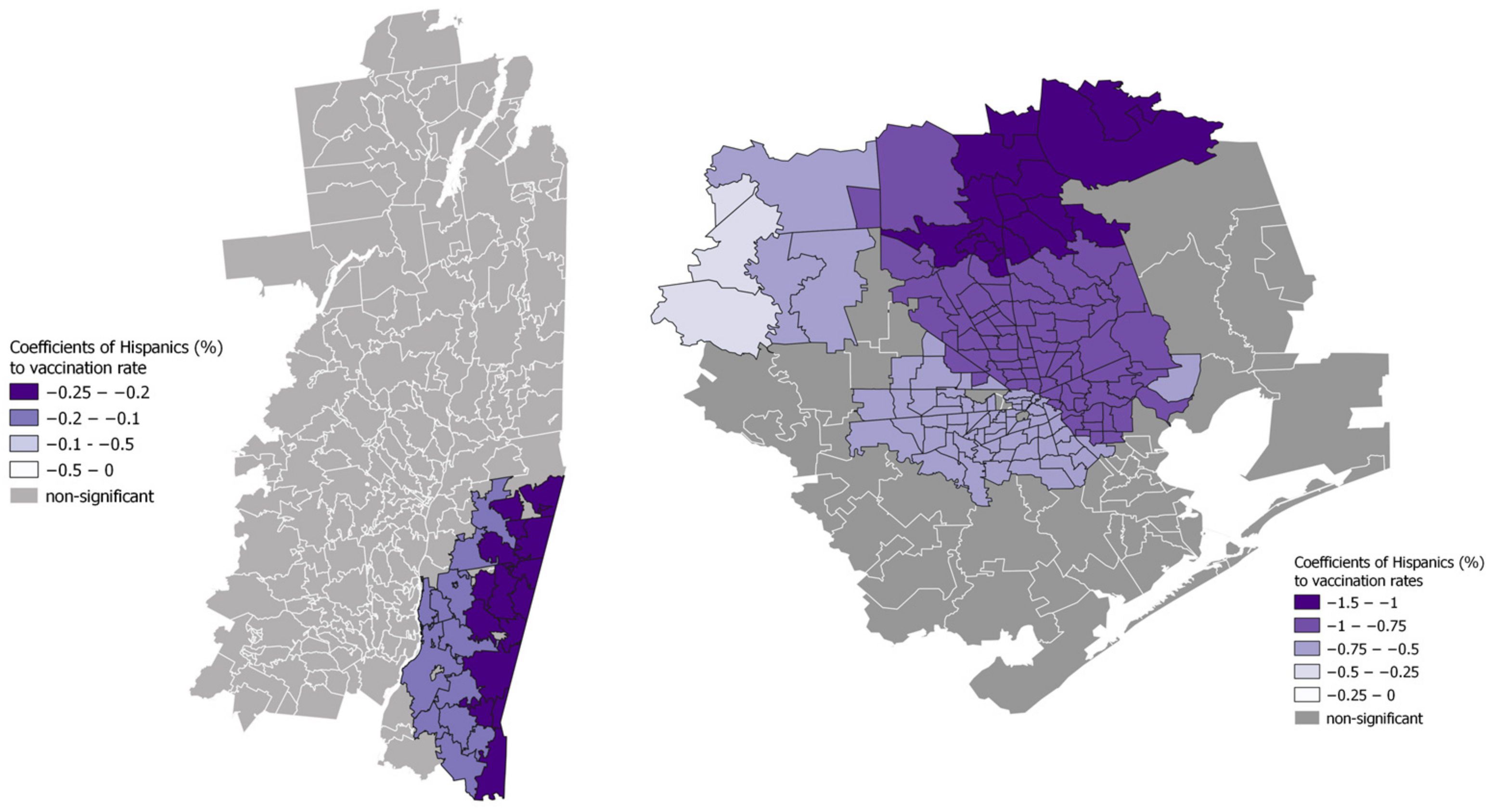
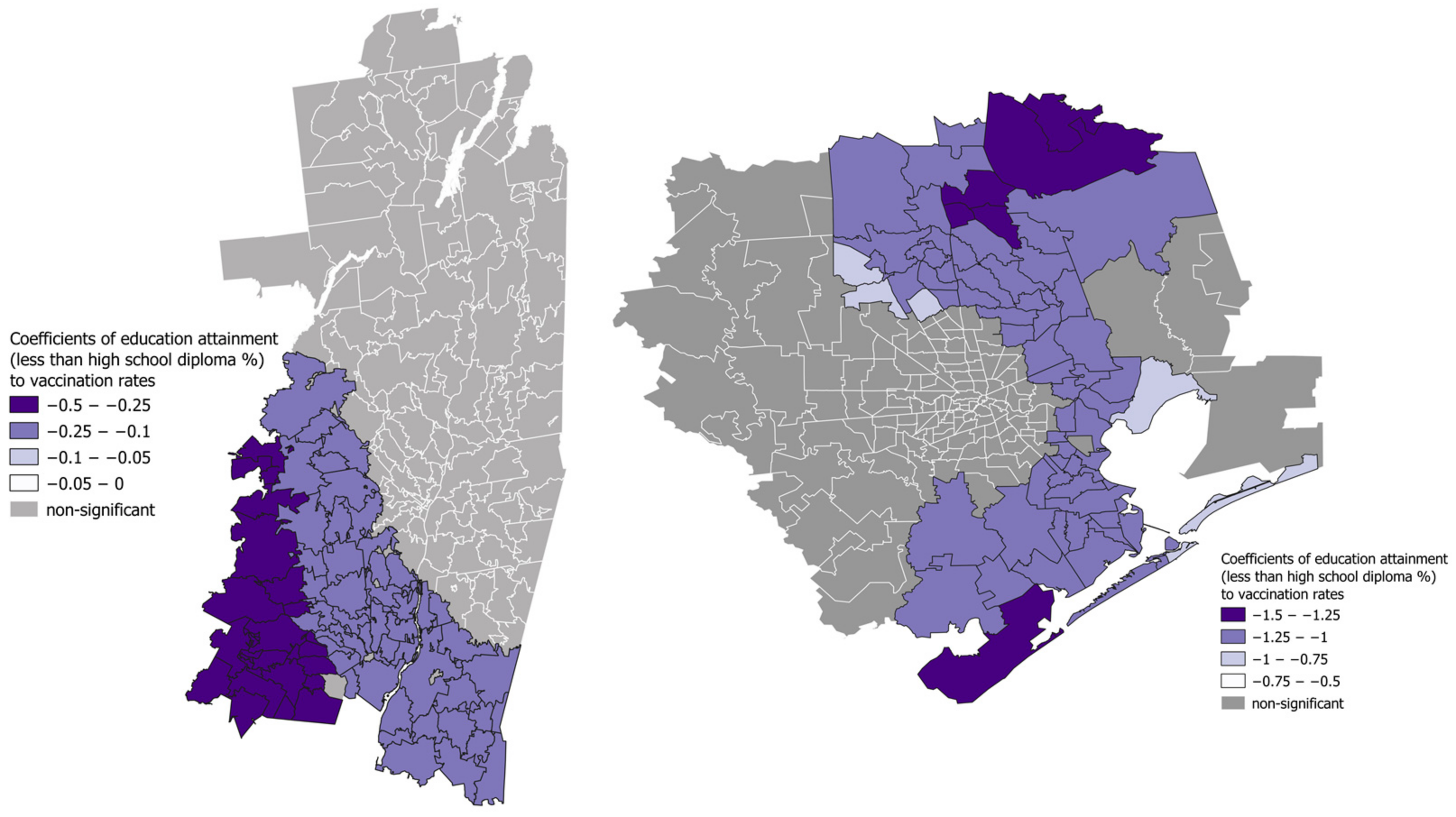
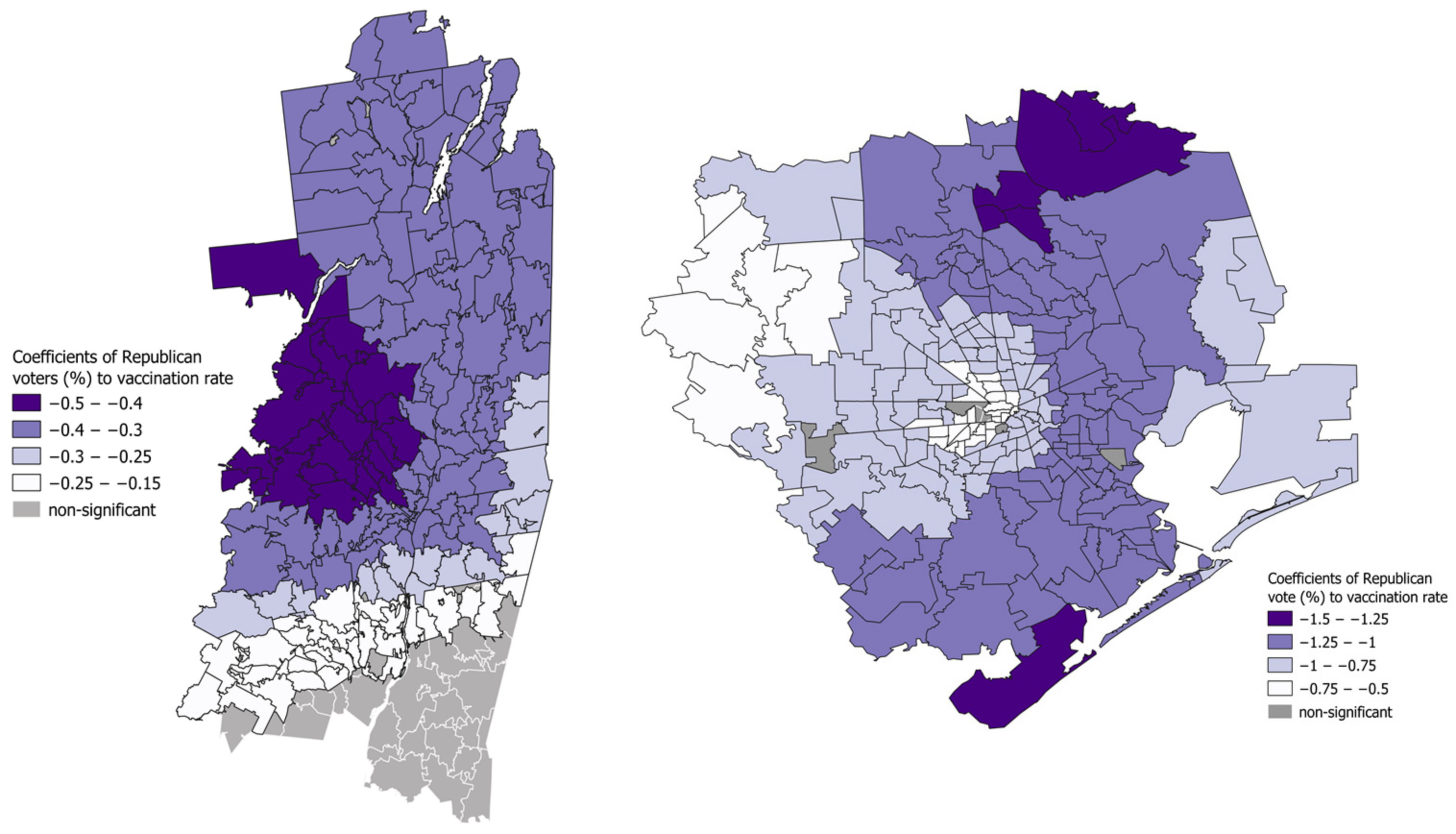
3.4. Regression
4. Discussions
4.1. Racial Divides
4.2. Socioeconomic Divides
4.3. Digital Divides
4.4. Political Divides
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- US Coronavirus Vaccine Tracker. Available online: https://usafacts.org/visualizations/covid-vaccine-tracker-states/ (accessed on 6 July 2022).
- Galarce, E.M.; Minsky, S.; Viswanath, K. Socioeconomic Status, Demographics, Beliefs and A (H1N1) Vaccine Uptake in the United States. Vaccine 2011, 29, 5284–5289. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, D.R.; Henneman, L.; Hirasing, R.A.; Van der Wal, G. Attitudes and Risk Perception of Parents of Different Ethnic Backgrounds Regarding Meningococcal C Vaccination. Vaccine 2005, 23, 3329–3335. [Google Scholar] [CrossRef] [PubMed]
- Brumfiel, G. Vaccine Refusal May Put Herd Immunity At Risk, Researchers Warn. NPR 2021, 7. [Google Scholar]
- Troiano, G.; Nardi, A. Vaccine Hesitancy in the Era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Lupton, R.N.; Hare, C. Conservatives Are More Likely to Believe That Vaccines Cause Autism. The Washington Post, 2015. Available online: https://www.washingtonpost.com/news/monkey-cage/wp/2015/03/01/conservatives-are-more-likely-to-believe-that-vaccines-cause-autism/(accessed on 8 January 2023).
- Hornsey, M.J.; Finlayson, M.; Chatwood, G.; Begeny, C.T. Donald Trump and Vaccination: The Effect of Political Identity, Conspiracist Ideation and Presidential Tweets on Vaccine Hesitancy. J. Exp. Soc. Psychol. 2020, 88, 103947. [Google Scholar] [CrossRef]
- Njoku, A.; Joseph, M.; Felix, R. Changing the Narrative: Structural Barriers and Racial and Ethnic Inequities in COVID-19 Vaccination. Int. J. Environ. Res. Public Health 2021, 18, 9904. [Google Scholar] [CrossRef]
- Yancy, C.W. COVID-19 and African Americans. JAMA 2020, 323, 1891–1892. [Google Scholar] [CrossRef] [Green Version]
- CDC. COVID-19 Hospitalization and Death by Race/Ethnicity. Available online: https://stacks.cdc.gov/view/cdc/91857 (accessed on 29 December 2021).
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and Disparities of Intention to Vaccinate against COVID-19. Soc. Sci. Med. 2021, 272, 113638. [Google Scholar] [CrossRef]
- Hamel, L.; Kirzinger, A.; Lopes, L.; Sparks, G.; Brodie, M. KFF COVID-19 Vaccine Monitor: January 2021. KFF, 2021. Available online: https://www.kff.org/coronavirus-covid-19/report/kff-covid-19-vaccine-monitor-january-2021/(accessed on 8 January 2023).
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. eClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Anderson, K.F.; Ray-Warren, D. Racial-Ethnic Residential Clustering and Early COVID-19 Vaccine Allocations in Five Urban Texas Counties. J. Health Soc. Behav. 2022, 63, 472–490. [Google Scholar] [CrossRef]
- Börjesson, M.; Enander, A. Perceptions and Sociodemographic Factors Influencing Vaccination Uptake and Precautionary Behaviours in Response to the A/H1N1 Influenza in Sweden. Scand. J. Public Health 2014, 42, 215–222. [Google Scholar] [CrossRef]
- Hilyard, K.M.; Freimuth, V.S.; Musa, D.; Kumar, S.; Quinn, S.C. The Vagaries of Public Support for Government Actions in Case of a Pandemic. Health Aff. 2010, 29, 2294–2301. [Google Scholar] [CrossRef]
- Myers, L.B.; Goodwin, R. Determinants of Adults’ Intention to Vaccinate against Pandemic Swine Flu. BMC Public Health 2011, 11, 15. [Google Scholar] [CrossRef] [Green Version]
- Hilton, S.; Smith, E. Public Views of the UK Media and Government Reaction to the 2009 Swine Flu Pandemic. BMC Public Health 2010, 10, 697. [Google Scholar] [CrossRef] [Green Version]
- Majid, U.; Ahmad, M. The Factors That Promote Vaccine Hesitancy, Rejection, or Delay in Parents. Qual. Health Res. 2020, 30, 1762–1776. [Google Scholar] [CrossRef]
- Press, V.G.; Huisingh-Scheetz, M.; Arora, V.M. Inequities in Technology Contribute to Disparities in COVID-19 Vaccine Distribution. JAMA Health Forum 2021, 2, e210264. [Google Scholar] [CrossRef]
- Saha, S. US Digital Divide Threatens Vaccine Access for Older People. Human Rights Watch, 2021. Available online: https://www.hrw.org/news/2021/02/08/us-digital-divide-threatens-vaccine-access-older-people(accessed on 8 January 2023).
- Vogels, E.A. Some Digital Divides Persist between Rural, Urban and Suburban America. Pew Research Center, 2021. Available online: https://www.pewresearch.org/fact-tank/2021/08/19/some-digital-divides-persist-between-rural-urban-and-suburban-america/(accessed on 8 January 2023).
- Anderson, M. About a Quarter of Rural Americans Say Access to High-Speed Internet Is a Major Problem; Pew Research Center: Washington, DC, USA, 2018. [Google Scholar]
- Goel, R.K.; Nelson, M.A. COVID-19 Internet Vaccination Information and Vaccine Administration: Evidence from the United States. J. Econ. Finance 2021, 45, 716–734. [Google Scholar] [CrossRef]
- Webb Hooper, M.; Nápoles, A.M.; Pérez-Stable, E.J. No Populations Left behind: Vaccine Hesitancy and Equitable Diffusion of Effective COVID-19 Vaccines. J. Gen. Intern. Med. 2021, 36, 2130–2133. [Google Scholar] [CrossRef] [PubMed]
- de Vries, H.; Verputten, W.; Preissner, C.; Kok, G. COVID-19 Vaccine Hesitancy: The Role of Information Sources and Beliefs in Dutch Adults. Int. J. Environ. Res. Public Health 2022, 19, 3205. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-P.; Chen, Y.-Y.; Yang, K.-C.; Lai, F.; Huang, C.-H.; Chen, Y.-N.; Tu, Y.-C. The Prevalence and Impact of Fake News on COVID-19 Vaccination in Taiwan: Retrospective Study of Digital Media. J. Med. Internet Res. 2022, 24, e36830. [Google Scholar] [CrossRef]
- Cao, J.; Ramirez, C.M.; Alvarez, R.M. The Politics of Vaccine Hesitancy in the United States. Soc. Sci. Q. 2022, 103, 42–54. [Google Scholar] [CrossRef]
- Sharma, M.; Davis, R.E.; Wilkerson, A.H. COVID-19 Vaccine Acceptance among College Students: A Theory-Based Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4617. [Google Scholar] [CrossRef]
- Sparks, G.; Lopes, L.; Montero, A.; Hamel, L.; Brodie, M. KFF COVID-19 Vaccine Monitor: April 2022. KFF, 2022. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-april-2022/(accessed on 8 January 2023).
- Lasher, E.; Fulkerson, G.; Seale, E.; Thomas, A.; Gadomski, A. COVID-19 Vaccine Hesitancy and Political Ideation among College Students in Central New York: The Influence of Differential Media Choice. Prev. Med. Rep. 2022, 27, 101810. [Google Scholar] [CrossRef]
- Public Religion Research Institute. Religious Identities and the Race Against the Virus: Engaging Faith Communities on COVID-19 Vaccination: (Wave 1: March 2021); Public Religion Research Institute: Washington, DC, USA, 2021. [Google Scholar]
- Protestants, E. Religious Landscape Study; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Gamio, L.; Walker, A.S. Where the Delta Wave Has Driven up COVID-19 Vaccinations; New York Times: New York, NY, USA, 2021. [Google Scholar]
- US Census Bureau. U.C. 2016–2020 ACS 5-Year Estimates. Available online: https://www.census.gov/programs-surveys/acs/technical-documentation/table-and-geography-changes/2020/5-year.html (accessed on 26 July 2022).
- Park, A.; Smart, C.; Taylor, R.; Watkins, M. An Extremely Detailed Map of the 2020 Election; New York Times: New York, NY, USA, 2021. [Google Scholar]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; John Wiley & Sons: Hoboken, NJ, USA, 2003; ISBN 0-470-85525-8. [Google Scholar]
- Urban, R.C.; Nakada, L.Y.K. GIS-Based Spatial Modelling of COVID-19 Death Incidence in São Paulo, Brazil. Environ. Urban. 2020, 33, 229–238. [Google Scholar] [CrossRef]
- Nakaya, T.; Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Poisson Regression for Disease Association Mapping. Stat. Med. 2005, 24, 2695–2717. [Google Scholar] [CrossRef] [Green Version]
- Cook, A.C.; Hill, N.J.; Trichka, M.I.; Hwang, G.J.; Sommers, P.M. Who Voted for Trump in 2016? Open J. Soc. Sci. 2017, 5, 199. [Google Scholar] [CrossRef] [Green Version]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M.E. Geographically Weighted Regression: A Method for Exploring Spatial Nonstationarity. Geogr. Anal. 1996, 28, 281–298. [Google Scholar] [CrossRef]
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global Trends in Emerging Infectious Diseases. Nature 2008, 451, 990–993. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NY (Capital Region) | TX (Houston Metro) | |
|---|---|---|
| Number of ZCTAs | 221 (93 Dem., 128 Rep.) | 213 (113 Dem., 100 Rep.) |
| Population | 1,151,703 | 6,881,708 |
| Avg. vaccination rate | 56.45% | 54.41% |
| Capital Region Vax Rate | Houston Metro Vax Rate | |
|---|---|---|
| Voting for Rep. candidate | −0.139 * | −0.226 ** |
| Bachelor and above | 0.385 ** | 0.772 ** |
| Less than high school | −0.276 ** | −0.463 ** |
| No internet access | −0.142 * | −0.459 ** |
| No computer | −0.003 | −0.388 ** |
| Unemployment | −0.112 | −0.243 ** |
| Poverty | −0.238 ** | −0.377 ** |
| Asian | 0.101 | 0.577 ** |
| Hispanic | −0.161 * | −0.306 ** |
| Capital Region, NY | Houston Metro, TX | |||
|---|---|---|---|---|
| GAU.S.SIAN | GWR | GAU.S.SIAN | GWR | |
| AIC | 578.455 | 567.773 | 377.849 | 349.354 |
| AICc | 581.561 | 571.459 | 380.983 | 363.685 |
| R2 | 0.156 | 0.265 | 0.661 | 0.77 |
| Adj. R2 | 0.122 | 0.199 | 0.647 | 0.725 |
| NY | TX | |
|---|---|---|
| Blacks | 0.044 | −0.665 ** |
| Asians | 0.061 | 0.14 * |
| Hispanics | −0.16 * | −0.282 * |
| Unemployment | −0.055 | −0.008 |
| Poverty | −0.202 * | −0.091 |
| No access to the internet | −0.004 | −0.02 |
| Less than a high school diploma | −0.162 * | −0.403 ** |
| Voting for Rep. presidential candidate | −0.193 * | −0.985 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, R.; Erickson, D.; Belcaid, M.; Chinedu, M.F.; Akanbi, O.O. A Tale of Two Cities: COVID-19 Vaccine Hesitancy as a Result of Racial, Socioeconomic, Digital, and Partisan Divides. ISPRS Int. J. Geo-Inf. 2023, 12, 158. https://doi.org/10.3390/ijgi12040158
Li R, Erickson D, Belcaid M, Chinedu MF, Akanbi OO. A Tale of Two Cities: COVID-19 Vaccine Hesitancy as a Result of Racial, Socioeconomic, Digital, and Partisan Divides. ISPRS International Journal of Geo-Information. 2023; 12(4):158. https://doi.org/10.3390/ijgi12040158
Chicago/Turabian StyleLi, Rui, Daniel Erickson, Mareyam Belcaid, Madu Franklin Chinedu, and Oluwabukola Olufunke Akanbi. 2023. "A Tale of Two Cities: COVID-19 Vaccine Hesitancy as a Result of Racial, Socioeconomic, Digital, and Partisan Divides" ISPRS International Journal of Geo-Information 12, no. 4: 158. https://doi.org/10.3390/ijgi12040158