


Dopamine D1 Agonists: First Potential Treatment for Late-Stage Parkinson’s Disease
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
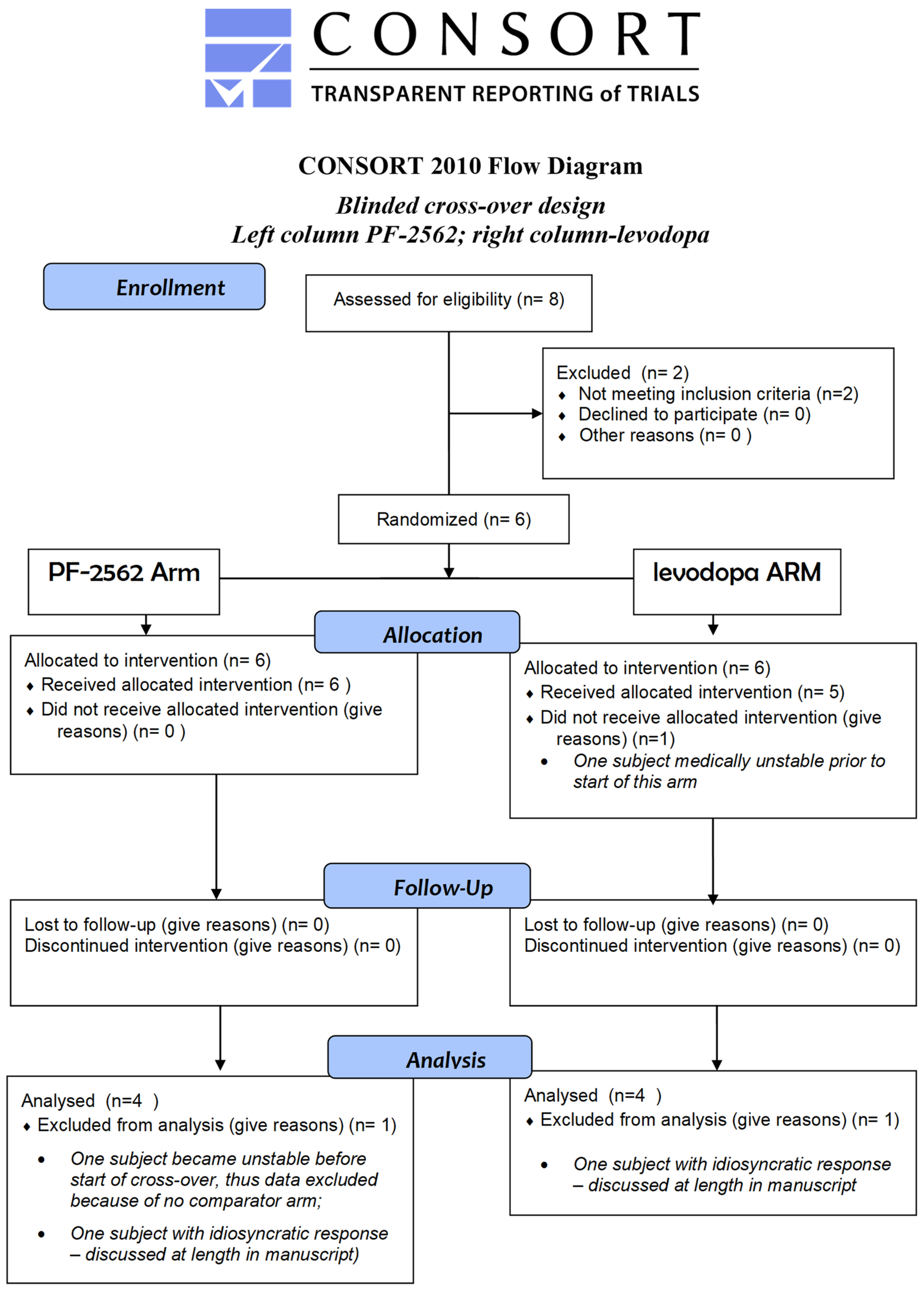
2.1. Study Design, Subjects, and Randomization
2.2. Study Compound Choice
2.3. Quantitative Data and Metrics
2.4. Qualitative Interviews
2.5. Convergent Mixed Methods Design
2.6. Analysis
3. Results
3.1. Participants
3.2. Quantitative Results
3.3. Qualitative Caregiver Interview
3.4. Mixed Methods Results
4. Discussion
4.1. Mechanisms of Action of Levodopa vs. D1 Agonist in LsPD
4.2. Unresolved Mechanisms in These Findings
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Details of Quantitative Analysis
Appendix A.2. Details of Qualitative Analysis
Appendix A.3. Importance of Caregiver Perspectives
Appendix A.4. Mixed Methods in a Phase I Study


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Class | Target(s) | Current Status | Clinical Effects | Side Effects |
|---|---|---|---|---|
| Levodopa (indirect dop- amine agonist) [levodopa/carbidopa-based combinations or formulations] | Results in dopamine that targets all dopamine receptors At higher doses, may affect “off-target” receptors due to “off-site” DA | Standard-of-care for Parkinson’s disease since 1967 (formulations include Sinemet, Parcopa, Duopa, Rytary; Stalevo; Bendopa, Inbrija) | Very effective in early and mid-stage disease | More side effects with disease progression (dyskinesias, on-off; hypotension; drowsiness and hallucinations in later stages) |
| “D1 agonists” (D1–D5 non-selective) | Dihydrexidine (full agonist) | Non-human primates; Phase Ib | Very effective in severely PD non-human primates | Severe hypotension in humans; short-acting; injectable only |
| ABT-431 (full agonist) | two published Phase II trials | Very effective in mid-stage PD | Hypotension; nausea; injectable only | |
| PF-06412562 (PF-2562) | Phase IIa | Effective in mid-stage PD | Hypotension; nausea | |
| tavapadon (PF-06649751) | Phase III | Effective in mid-stage PD | Hypotension; nausea | |
| “Dopamine agonists” (selective D2/D3) | cabergoline (Dostinex) | (Withdrawn, valvulopathy) | Moderate efficacy (does not match levodopa); used for earlier stage PD and as adjuvant | Hypotension; obsessive and compulsive disorders; Drowsiness; hallucinations |
| pramipexole (Mirapex) | Approved drug | |||
| ropinirole (Requip) | Approved drug | |||
| “Dopamine agonists” (selective D2/D3 with some D1 affinity) | bromocriptine (Parlodel) | Approved drug; D1 antagonist | Moderate efficacy | Hypotension; obsessive and compulsive disorders; Drowsiness, hallucinations |
| pergolide (Permax) | Withdrawn (valvulopathy); D1 partial agonist | More effective than bromocriptine | ||
| rotigotine (Neupro) | Approved drug (patch) | Patch only | ||
| apomorphine (Apokyn) | Approved drug (injection or sublingual) | Short-acting; effective for rescue |
| Mean ± SD | ||
|---|---|---|
| Levodopa | Baseline | 83.7 ± 26.2 |
| Day 2, time 2 | 81.6 ± 24.7 | |
| Day 2, time 3 | 84.8 ± 22.8 | |
| Day 3, time 2 | 88.2 ± 27.2 | |
| Day 3, time 3 | 82.2 ± 25.6 | |
| PF-2562 | Baseline | 81.5 ± 19.5 |
| Day 2, time 2 | 90.0 ± 26.1 | |
| Day 2, time 3 | 83.8 ± 27.4 | |
| Day 3, time 2 | 79.4 ± 30.1 | |
| Day 3, time 3 | 82.8 ± 28.7 |

References
- Cotzias, G.C.; Van Woert, M.H.; Schiffer, L.M. Aromatic amino acids and modification of parkinsonism. N. Engl. J. Med. 1967, 276, 374–379. [Google Scholar] [CrossRef]
- Goldstein, M.; Lieberman, A.; Pearson, J. Relatively high levels of dopamine in nucleus accumbens of levodopa treated patients with Parkinson’s disease. J. Neural Transm. 1982, 54, 129–134. [Google Scholar] [CrossRef]
- Barone, P. Neurotransmission in Parkinson’s disease: Beyond dopamine. Eur. J. Neurol. 2010, 17, 364–376. [Google Scholar] [CrossRef]
- Munoz, A.; Lopez-Lopez, A.; Labandeira, C.M.; Labandeira-Garcia, J.L. Interactions between the Serotonergic and Other Neurotransmitter Systems in the Basal Ganglia: Role in Parkinson’s Disease and Adverse Effects of L-DOPA. Front. Neuroanat. 2020, 14, 26. [Google Scholar] [CrossRef] [PubMed]
- Shin, E.; Tronci, E.; Carta, M. Role of Serotonin Neurons in L-DOPA- and Graft-Induced Dyskinesia in a Rat Model of Parkinson’s Disease. Park. Dis. 2012, 2012, 370190. [Google Scholar] [CrossRef] [PubMed]
- Navailles, S.; Carta, M.; Guthrie, M.; De Deurwaerdere, P. L-DOPA and serotonergic neurons: Functional implication and therapeutic perspectives in Parkinson’s disease. Cent. Nerv. Syst. Agents Med. Chem. 2011, 11, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Coelho, M.; Ferreira, J.J. Late-stage Parkinson disease. Nat. Rev. Neurol. 2012, 8, 435–442. [Google Scholar] [CrossRef]
- Fox, S.; Gannon, E.; Cashell, A.; Kernohan, W.G.; Lynch, M.; McGlade, C.; O’Brien, T.; O’Sullivan, S.S.; Sweeney, C.; Timmons, S. Survey of Health Care Workers Suggests Unmet Palliative Care Needs in Parkinson’s Disease. Mov. Disord. Clin. Pract. 2015, 2, 142–148. [Google Scholar] [CrossRef]
- Lex, K.M.; Larkin, P.; Osterbrink, J.; Lorenzl, S. A Pilgrim’s Journey-When Parkinson’s Disease Comes to an End in Nursing Homes. Front. Neurol. 2018, 9, 1068. [Google Scholar] [CrossRef] [PubMed]
- Visanji, N.; Marras, C. The relevance of pre-motor symptoms in Parkinson’s disease. Expert Rev. Neurother. 2015, 15, 1205–1217. [Google Scholar] [CrossRef]
- Kaltenboeck, A.; Johnson, S.J.; Davis, M.R.; Birnbaum, H.G.; Carroll, C.A.; Tarrants, M.L.; Siderowf, A.D. Direct costs and survival of medicare beneficiaries with early and advanced Parkinson’s disease. Park. Relat. Disord. 2012, 18, 321–326. [Google Scholar] [CrossRef]
- Low, J.A.; Pang, W.S.; Chan, D.K.; Chye, R. A palliative care approach to end-stage neurodegenerative conditions. Ann. Acad. Med. Singap. 2003, 32, 778–784. [Google Scholar] [PubMed]
- Thomas, S.; MacMahon, D. Parkinson’s disease, palliative care and older people: Part 1. Nurs. Older People 2004, 16, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.; Cheng, E.; Siebens, H.C.; Lee, M.L.; Mittman, B.S.; Ganz, D.A.; Vickrey, B. Study protocol of “CHAPS”: A randomized controlled trial protocol of Care Coordination for Health Promotion and Activities in Parkinson’s Disease to improve the quality of care for individuals with Parkinson’s disease. BMC Neurol. 2015, 15, 258. [Google Scholar] [CrossRef] [PubMed]
- Bouca-Machado, R.; Titova, N.; Chaudhuri, K.R.; Bloem, B.R.; Ferreira, J.J. Palliative Care for Patients and Families with Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 132, 475–509. [Google Scholar] [CrossRef]
- Di Luca, D.G.; Singer, C.; Margolesky, J.H. Palliative Care in Parkinson Disease—Is It Beneficial for All? JAMA Neurol. 2020, 77, 1450. [Google Scholar] [CrossRef]
- Garau, L.; Govoni, S.; Stefanini, E.; Trabucchi, M.; Spano, P.F. Dopamine receptors: Pharmacological and anatomical evidences indicate that two distinct dopamine receptor populations are present in rat striatum. Life Sci. 1978, 23, 1745–1750. [Google Scholar] [CrossRef]
- Kebabian, J.W.; Calne, D.B. Multiple receptors for dopamine. Nature 1979, 277, 93–96. [Google Scholar] [CrossRef]
- Neve, K.A.; Neve, R.L. The Dopamine Receptors; Humana Press: Totowa, NJ, USA, 1997; ISBN 978-1-4757-2635-0. [Google Scholar]
- Dearry, A.; Gingrich, J.A.; Falardeau, P.; Fremeau, R.T., Jr.; Bates, M.D.; Caron, M.G. Molecular cloning and expression of the gene for a human D1 dopamine receptor. Nature 1990, 347, 72–76. [Google Scholar] [CrossRef]
- Monsma, F.J., Jr.; Mahan, L.C.; McVittie, L.D.; Gerfen, C.R.; Sibley, D.R. Molecular cloning and expression of a D1 dopamine receptor linked to adenylyl cyclase activation. Proc. Natl. Acad. Sci. USA 1990, 87, 6723–6727. [Google Scholar] [CrossRef]
- Sunahara, R.K.; Niznik, H.B.; Weiner, D.M.; Stormann, T.M.; Brann, M.R.; Kennedy, J.L.; Gelernter, J.E.; Rozmahel, R.; Yang, Y.L.; Israel, Y.; et al. Human dopamine D1 receptor encoded by an intronless gene on chromosome 5. Nature 1990, 347, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.Y.; Grandy, D.K.; Thambi, L.; Kushner, J.A.; Van Tol, H.H.; Cone, R.; Pribnow, D.; Salon, J.; Bunzow, J.R.; Civelli, O. Cloning and expression of human and rat D1 dopamine receptors. Nature 1990, 347, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Mailman, R.; Huang, X.; Nichols, D.E. Parkinson’s disease and D1 dopamine receptors. Curr. Opin. Investig. Drugs Lond. Engl. 2001, 2, 1582–1591. [Google Scholar]
- Mailman, R.B.; Huang, X. Dopamine receptor pharmacology. Handb. Clin. Neurol. 2007, 83, 77–105. [Google Scholar] [CrossRef]
- Konta, B.; Frank, W. The treatment of Parkinson’s disease with dopamine agonists. GMS Health Technol. Assess. 2008, 4, Doc05. [Google Scholar]
- Newman-Tancredi, A.; Cussac, D.; Audinot, V.; Nicolas, J.P.; De Ceuninck, F.; Boutin, J.A.; Millan, M.J. Differential actions of antiparkinson agents at multiple classes of monoaminergic receptor. II. Agonist and antagonist properties at subtypes of dopamine D2-like receptor and α1/α2-adrenoceptor. J. Pharmacol. Exp. Ther. 2002, 303, 805–814. [Google Scholar] [CrossRef]
- Millan, M.J.; Maiofiss, L.; Cussac, D.; Audinot, V.; Boutin, J.A.; Newman-Tancredi, A. Differential actions of antiparkinson agents at multiple classes of monoaminergic receptor. I. A multivariate analysis of the binding profiles of 14 drugs at 21 native and cloned human receptor subtypes. J. Pharmacol. Exp. Ther. 2002, 303, 791–804. [Google Scholar] [CrossRef]
- Huang, X.; Lawler, C.P.; Lewis, M.M.; Nichols, D.E.; Mailman, R.B. D1 dopamine receptors. Int. Rev. Neurobiol. 2001, 48, 65–139. [Google Scholar]
- Mailman, R.B.; Nichols, D.E. Dopamine D1 receptor agonists as antiparkinson drugs. Trends Pharmacol. Sci. 1998, 19, 255–256. [Google Scholar]
- Taylor, J.R.; Lawrence, M.S.; Redmond, D.E., Jr.; Elsworth, J.D.; Roth, R.H.; Nichols, D.E.; Mailman, R.B. Dihydrexidine, a full dopamine D1 agonist, reduces MPTP-induced parkinsonism in monkeys. Eur. J. Pharmacol. 1991, 199, 389–391. [Google Scholar] [CrossRef]
- Mailman, R.B.; Yang, Y.; Huang, X. D1, not D2, dopamine receptor activation dramatically improves MPTP-induced parkinsonism unresponsive to levodopa. Eur. J. Pharmacol. 2021, 892, 173760. [Google Scholar] [CrossRef]
- Rascol, O.; Blin, O.; Thalamas, C.; Descombes, S.; Soubrouillard, C.; Azulay, P.; Fabre, N.; Viallet, F.; Lafnitzegger, K.; Wright, S.; et al. ABT-431, a D1 receptor agonist prodrug, has efficacy in Parkinson’s disease. Ann. Neurol. 1999, 45, 736–741. [Google Scholar] [CrossRef]
- Rascol, O.; Nutt, J.G.; Blin, O.; Goetz, C.G.; Trugman, J.M.; Soubrouillard, C.; Carter, J.H.; Currie, L.J.; Fabre, N.; Thalamas, C.; et al. Induction by dopamine D1 receptor agonist ABT-431 of dyskinesia similar to levodopa in patients with Parkinson disease. Arch. Neurol. 2001, 58, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.L.F.; Zhang, L.; Davoren, J.; Dounay, A.B.; Viktorovich, I.; Lee, C.; Mente, S.R.; O’Neil, S.V.; Rogers, B.N.; Subramanyam, C. Heteroaromatic Compounds and Their Use as Dopamine D1 Ligands. U.S. Patent 10077272 B2, 2018. [Google Scholar]
- Gray, D.L.; Allen, J.A.; Mente, S.; O’Connor, R.E.; DeMarco, G.J.; Efremov, I.; Tierney, P.; Volfson, D.; Davoren, J.; Guilmette, E.; et al. Impaired β-arrestin recruitment and reduced desensitization by non-catechol agonists of the D1 dopamine receptor. Nat. Commun. 2018, 9, 674. [Google Scholar] [CrossRef] [PubMed]
- Papapetropoulos, S.; Liu, W.; Duvvuri, S.; Thayer, K.; Gray, D.L. Evaluation of D1/D5 Partial Agonist PF-06412562 in Parkinson’s Disease following Oral Administration. Neurodegener. Dis. 2018, 18, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Riesenberg, R.; Werth, J.; Zhang, Y.; Duvvuri, S.; Gray, D. PF-06649751 efficacy and safety in early Parkinson’s disease: A randomized, placebo-controlled trial. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420911296. [Google Scholar] [CrossRef] [PubMed]
- Sohur, U.S.; Gray, D.L.; Duvvuri, S.; Zhang, Y.; Thayer, K.; Feng, G. Phase 1 Parkinson’s Disease Studies Show the Dopamine D1/D5 Agonist PF-06649751 is Safe and Well Tolerated. Neurol. Ther. 2018, 7, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Lewis, M.M.; Van Scoy, L.J.; De Jesus, S.; Eslinger, P.J.; Arnold, A.C.; Miller, A.J.; Fernandez-Mendoza, J.; Snyder, B.; Harrington, W.; et al. The D1/D5 Dopamine Partial Agonist PF-06412562 in Advanced-Stage Parkinson’s Disease: A Feasibility Study. J. Park. Dis. 2020, 10, 1515–1527. [Google Scholar] [CrossRef] [PubMed]
- Miyasaki, J.M.; Kluger, B. Palliative care for Parkinson’s disease: Has the time come? Curr. Neurol. Neurosci. Rep. 2015, 15, 26. [Google Scholar] [CrossRef]
- Klietz, M.; Eichel, H.V.; Staege, S.; Kutschenko, A.; Respondek, G.; Huber, M.K.; Greten, S.; Hoglinger, G.U.; Wegner, F. Validation of the Parkinson’s Disease Caregiver Burden Questionnaire in Progressive Supranuclear Palsy. Park. Dis. 2021, 2021, 9990679. [Google Scholar] [CrossRef]
- Gulunay, A.; Cakmakli, G.Y.; Yon, M.I.; Ulusoy, E.K.; Karakoc, M. Frequency of non-motor symptoms and their impact on the quality of life in patients with Parkinson’s disease: A prospective descriptive case series. Psychogeriatrics 2020, 20, 206–211. [Google Scholar] [CrossRef]
- Deck, B.L.; Xie, S.X.; Choi, G.; Rick, J.; Siderowf, A.; Rudovsky, S.; Chen-Plotkin, A.; Duda, J.E.; Morley, J.F.; Dahodwala, N.; et al. Cognitive Functional Abilities in Parkinson’s Disease: Agreement between Patients and Informants. Mov. Disord. Clin. Pract. 2019, 6, 440–445. [Google Scholar] [CrossRef]
- Creswell, J.W.C.; David, J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; Sage Publishing: Thousand Oaks, CA, USA, 2017; ISBN 9781506386706. [Google Scholar]
- Santos-Garcia, D.; de Deus Fonticoba, T.; Suarez Castro, E.; Aneiros Diaz, A.; McAfee, D. 5-2-1 Criteria: A Simple Screening Tool for Identifying Advanced PD Patients Who Need an Optimization of Parkinson’s Treatment. Park. Dis. 2020, 2020, 7537924. [Google Scholar] [CrossRef] [PubMed]
- Panisset, M.; Roudier, M.; Saxton, J.; Boller, F. Severe impairment battery. A neuropsychological test for severely demented patients. Arch. Neurol. 1994, 51, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef]
- Fahn, S.; Elton, R.L. UPDRS-development-committee. In Recent Developements in Parkinson’s Disease; Fahn, S., Marsen, C.D., Goldstein, M., Calne, D., Eds.; Macmillan: New York, NY, USA, 1987; p. 433. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications: Thousand Oaks, CA USA, 2018; ISBN 978-1483344379/1483344371. [Google Scholar]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs-principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [PubMed]
- Guba, E.G.; Lincoln, Y.S. Effective Evaluation: Improving the Usefulness of Evaluation Results through Responsive and Naturalistic Approaches; Jossey-Bass: San Francisco, CA, USA, 1981. [Google Scholar]
- Kluger, B.M.; Dolhun, R.; Sumrall, M.; Hall, K.; Okun, M.S. Palliative Care and Parkinson’s Disease: Time to Move Beyond Cancer. Mov. Disord. 2021, 36, 1325–1329. [Google Scholar] [CrossRef]
- Senderovich, H.; Jimenez Lopez, B. Integration of palliative care in Parkinson’s disease management. Curr. Med. Res. Opin. 2021, 37, 1745–1759. [Google Scholar] [CrossRef]
- Creswell, J.W.; Klassen, A.C.; Plano Clark, V.L.; Smith, K.C. Best Practices for Mixed Methods Research in the Health Sciences; Office of Behavioral and Social Sciences Research (OBSSR): Bethesda, MD, USA, 2011.
- Prizer, L.P.; Gay, J.L.; Wilson, M.G.; Emerson, K.G.; Glass, A.P.; Miyasaki, J.M.; Perkins, M.M. A Mixed-Methods Approach to Understanding the Palliative Needs of Parkinson’s Patients. J. Appl. Gerontol. 2020, 39, 834–845. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.; Lloyd, K.; Dankova, J.; Hornykiewicz, O. L-DOPA treatment in Parkinson’s disease: Effect on dopamine and related substances in discrete brain regions. Experientia 1971, 27, 1048–1049. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, K.G.; Davidson, L.; Hornykiewicz, O. The neurochemistry of Parkinson’s disease: Effect of L-dopa therapy. J. Pharmacol. Exp. Ther. 1975, 195, 453–464. [Google Scholar] [PubMed]
- de la Fuente-Fernandez, R.; Sossi, V.; Huang, Z.; Furtado, S.; Lu, J.Q.; Calne, D.B.; Ruth, T.J.; Stoessl, A.J. Levodopa-induced changes in synaptic dopamine levels increase with progression of Parkinson’s disease: Implications for dyskinesias. Brain 2004, 127, 2747–2754. [Google Scholar] [CrossRef]
- Peralta, C.; Strafella, A.P.; van Eimeren, T.; Ceravolo, R.; Seppi, K.; Kaasinen, V.; Arena, J.E.; Lehericy, S.; International Parkinson Movement Disorders Society-Neuroimaging Study Group. Pragmatic Approach on Neuroimaging Techniques for the Differential Diagnosis of Parkinsonisms. Mov. Disord. Clin. Pract. 2022, 9, 6–19. [Google Scholar] [CrossRef]
- Buddhala, C.; Loftin, S.K.; Kuley, B.M.; Cairns, N.J.; Campbell, M.C.; Perlmutter, J.S.; Kotzbauer, P.T. Dopaminergic, serotonergic, and noradrenergic deficits in Parkinson disease. Ann. Clin. Transl. Neurol. 2015, 2, 949–959. [Google Scholar] [CrossRef]
- Rinne, U.K.; Sonninen, V.; Hyyppa, M. Effect of L-dopa on brain monoamines and their metabolites in Parkinson’s disease. Life Sci. 1971, 10, 549–557. [Google Scholar] [CrossRef]
- Yeung, E.Y.H.; Cavanna, A.E. Sleep Attacks in Patients with Parkinson’s Disease on Dopaminergic Medications: A Systematic Review. Mov. Disord. Clin. Pract. 2014, 1, 307–316. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Pal, S.; Brefel-Courbon, C. ‘Sleep attacks’ or ‘unintended sleep episodes’ occur with dopamine agonists: Is this a class effect? Drug Saf. 2002, 25, 473–483. [Google Scholar] [CrossRef]
- Jenner, P. Preventing and controlling dyskinesia in Parkinson’s disease—A view of current knowledge and future opportunities. Mov. Disord. 2008, 23 (Suppl. S3), S585–S598. [Google Scholar] [CrossRef]
- Mulas, G.; Espa, E.; Fenu, S.; Spiga, S.; Cossu, G.; Pillai, E.; Carboni, E.; Simbula, G.; Jadzic, D.; Angius, F.; et al. Differential induction of dyskinesia and neuroinflammation by pulsatile versus continuous l-DOPA delivery in the 6-OHDA model of Parkinson’s disease. Exp. Neurol. 2016, 286, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.M.; Laureno, R. Less Pulsatile Levodopa Therapy (6 Doses Daily) Is Associated with a Reduced Incidence of Dyskinesia. J. Mov. Disord. 2019, 12, 37–42. [Google Scholar] [CrossRef]
- Calandrella, D.; Antonini, A. Pulsatile or continuous dopaminomimetic strategies in Parkinson’s disease. Park. Relat. Disord. 2012, 18 (Suppl. S1), S120–S122. [Google Scholar] [CrossRef] [PubMed]
- Barroso-Chinea, P.; Bezard, E. Basal Ganglia circuits underlying the pathophysiology of levodopa-induced dyskinesia. Front. Neuroanat. 2010, 4, 131. [Google Scholar] [CrossRef] [PubMed]
- Grace, A.A.; Lodge, D.J.; Belujon, P. TouchNeurolgy: Movement Disorders, Parkinson’s Disease; TouchNeurology: Stockport, UK, 2011. [Google Scholar]
- Young, D.; Popiolek, M.; Trapa, P.; Fonseca, K.R.; Brevard, J.; Gray, D.L.; Kozak, R. D1 Agonist Improved Movement of Parkinsonian Nonhuman Primates with Limited Dyskinesia Side Effects. ACS Chem. Neurosci. 2020, 11, 560–566. [Google Scholar] [CrossRef]
- Davoren, J.E.; Nason, D.; Coe, J.; Dlugolenski, K.; Helal, C.; Harris, A.R.; LaChapelle, E.; Liang, S.; Liu, Y.; O’Connor, R.; et al. Discovery and Lead Optimization of Atropisomer D1 Agonists with Reduced Desensitization. J. Med. Chem. 2018, 61, 11384–11397. [Google Scholar] [CrossRef]
- Lovenberg, T.W.; Brewster, W.K.; Mottola, D.M.; Lee, R.C.; Riggs, R.M.; Nichols, D.E.; Lewis, M.H.; Mailman, R.B. Dihydrexidine, a novel selective high potency full dopamine D-1 receptor agonist. Eur. J. Pharmacol. 1989, 166, 111–113. [Google Scholar] [CrossRef]
- Yang, Y.; Lee, S.-M.; Imamura, F.; Gowda, K.; Amin, S.; Mailman, R.B. D1 dopamine receptors intrinsic activity and functional selectivity affect working memory in prefrontal cortex. Mol. Psychiatry 2021, 26, 645–655. [Google Scholar] [CrossRef]
- Arnsten, A.F.; Girgis, R.R.; Gray, D.L.; Mailman, R.B. Novel Dopamine Therapeutics for Cognitive Deficits in Schizophrenia. Biol. Psychiatry 2017, 81, 67–77. [Google Scholar] [CrossRef]
- Sierra, M.; Carnicella, S.; Strafella, A.P.; Bichon, A.; Lhommee, E.; Castrioto, A.; Chabardes, S.; Thobois, S.; Krack, P. Apathy and Impulse Control Disorders: Yin & Yang of Dopamine Dependent Behaviors. J. Park. Dis. 2015, 5, 625–636. [Google Scholar] [CrossRef]
- Urban, J.D.; Clarke, W.P.; von Zastrow, M.; Nichols, D.E.; Kobilka, B.; Weinstein, H.; Javitch, J.A.; Roth, B.L.; Christopoulos, A.; Sexton, P.M.; et al. Functional selectivity and classical concepts of quantitative pharmacology. J. Pharmacol. Exp. Ther. 2007, 320, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Lawler, C.P.; Prioleau, C.; Lewis, M.M.; Mak, C.; Jiang, D.; Schetz, J.A.; Gonzalez, A.M.; Sibley, D.R.; Mailman, R.B. Interactions of the novel antipsychotic aripiprazole (OPC-14597) with dopamine and serotonin receptor subtypes. Neuropsychopharmacology 1999, 20, 612–627. [Google Scholar] [CrossRef] [PubMed]
- Mailman, R.B.; Nichols, D.E.; Lewis, M.M.; Blake, B.L.; Lawler, C.P. Dopamine Receptor Subtypes: From Basic Science to Clinical Application; Jenner, P., Demirdemar, R., Eds.; IOS Stockton Press: Amsterdam, The Netherlands, 1998; pp. 64–83. [Google Scholar]
- Urs, N.M.; Daigle, T.L.; Caron, M.G. A dopamine D1 receptor-dependent β-arrestin signaling complex potentially regulates morphine-induced psychomotor activation but not reward in mice. Neuropsychopharmacology 2011, 36, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Felsing, D.E.; Chen, H.; Raval, S.R.; Allen, J.A.; Zhou, J. Synthesis and Pharmacological Evaluation of Noncatechol G Protein Biased and Unbiased Dopamine D1 Receptor Agonists. ACS Med. Chem. Lett. 2019, 10, 792–799. [Google Scholar] [CrossRef]
- Lewis, M.M.; Huang, X.; Nichols, D.E.; Mailman, R.B. D1 and functionally selective dopamine agonists as neuroprotective agents in Parkinson’s disease. CNS Neurol. Disord. Drug Targets 2006, 5, 345–353. [Google Scholar] [CrossRef]
- Mailman, R.B. GPCR functional selectivity has therapeutic impact. Trends Pharmacol. Sci. 2007, 28, 390–396. [Google Scholar] [CrossRef]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research Through Joint Displays. Ann. Fam. Med. 2015, 13, 554. [Google Scholar] [CrossRef]
- Trang, I.; Katz, M.; Galifianakis, N.; Fairclough, D.; Sillau, S.H.; Miyasaki, J.; Kluger, B.M. Predictors of general and health-related quality of life in Parkinson’s disease and related disorders including caregiver perspectives. Park. Relat. Disord. 2020, 77, 5. [Google Scholar] [CrossRef]
- O’Cathain, A. A Practical Guide to Using Qualitative Research with Randomized Clinical Trials, 1st ed.; Oxford University Press: Oxford, UK, 2018; ISBN 0198802080. [Google Scholar]
- Van Scoy, L.J.; Green, M.J.; Creswell, J.D.; Thiede, T.; Wiegand, D.; La, I.S.; Lipnick, D.; Johnson, R.; Dimmock, A.E.; Foy, A.; et al. Generating a New Outcome Variable Using Mixed Methods in a Randomized Controlled Trial: The Caregiver Study—An Advance Care Planning Investigation. J. Mix. Methods Res. 2020, 1558689820970686, 20. [Google Scholar] [CrossRef]



| Construct | Quantitative Measure | Qualitative Measure (Caregiver Interviews) |
|---|---|---|
| Motor | MDS-UPDRS-III-motor subscale | Tell me about [patient]’s normal level of [alertness, cognition, facial expression, movement or rigidity, sleep]. How has [patient]’s [alertness, cognition, facial expression, movement or rigidity, sleep] been over the past two days? Tell me about that. PROMPTS (if needed): Can you give some examples of things that you have noticed? How is [patient]’s level of [alertness, cognition, facial expression, movement or rigidity, sleep] different compared to a week ago? How, if at all, has this changed since the infusion started? When did you notice these changes? Have you noticed these kinds of changes before? Tell me more about that. |
| Alertness | Glasgow Coma scale (GCS) Stanford Sleepiness Scale (SSS) | |
| Cognition | Severe Impairment Battery (SIB) Frontal Assessment Battery (FAB) | |
| Sleep | Sleep efficiency | |
| Overall | Clinician Global Clinical Impression of Change (GCI-C) modified for late-stage stage PD patients Caregiver Global Clinical Impression of Change (GCI-C) questionnaire | How do you think [patient] responded to the treatment over the past two days? Can you give some examples of things that you have noticed? How, if at all, has [patient] changed since the infusion started? |
| ID | Demographic, Key Medical and Surgery Milestones | Current Medication | Disease Stages and Severity * | Caregiver Perspective Key Narrative/Phrases from Qualitative Interviews |
|---|---|---|---|---|
| 1 | M, PD at 36–40 y; pallidotomy at 46–50 y; wheelchair use at 61–65 y; PEG at 61–65 y | DA drugs: Parcopa; Non-DA drugs: rivastigmine transdermal | HY stage: 5; MD-GCI-S: 6 CG-GCI-S: 96 | Periods of intermittent wakefulness between mid-am to later-pm, less alert after levodopa. Requires two people to help him out of bed, stiff in am. Incontinent at baseline. |
| 3 | M, PD at 55–60 y; STN-DBS at 66–70 y; walker and wheelchair use at 76–80 y | DA drugs: Sinemet R and CR; Non-DA drugs: Vitamin B12 | HY Stage: 4–5; MD-GCI-S: 4 CG-GCI-S: 37 | Trouble with concentration, often not remembering things. Discomfort with social interactions, doesn’t smile, appears sad. Sleepy after drugs. Hard time getting up, freezing. Uses a chair lift. Often days & nights ‘mixed up’. |
| 4 | F, PD at 56–60 y; STN-DBS at 61–65 y; Walker use at 66–70 y; Wheelchair use at 66–70 y | DA drugs: Sinemet R & CR, Rytary, selegiline, pramipexole; Non-DA Drugs: dexlansoprazole, melatonin, midodrine, donepezil, memantine, clozapine, rimantadine, methylphenidate, venlafaxine fludrocortisdone | HY Stage: 4–5; MD-GCI-S: 5 CG-GCI-S: 52 | Confusion, peaks and valleys, emotional, a blank facial expression. Often urgency and incontinence and constipation. Sleeps deeply >14 h/day. Has a lot of dreaming and vocalization, particularly in second half of the night. Nocturnal movements wax and wane. Some difficulty with swallowing pills. |
| 6 | F, PD at 56–60 y; Walker use at 76–80 y; Wheelchair at 76–80 | DA drugs: Rytary, Sinemet; Non-DA drugs: gabapentin, donepezil, lorazepam, quetiapine, melatonin, tramadol | HY Stage: 4–5; MD-GCI-S: 4 CG-GCI-S: 10 | Some mild short-term memory problems. Naps 3–4 h per day, frequent awakenings at night with vocalizations. Mild swallowing problems if she eats too quickly. |
| 7 | M, PD at 51–55 y; Cane use at 71–75 y; Wheelchair use at 71–75 y | DA drugs: Rytary, rasagiline; Non-DA drugs: donepezil | HY Stage: 4–5; MD-GCI-S: 4 CG-GCI-S: 38 | Varying in alertness, doesn’t communicate much with facial expressions, shows strong emotions occasionally. Stooped posture with head tilted right. Issues with frozen foot. Yells in sleep, frequent dreams. |
| 8 | M, PD dx at 41–45 y; Levodopa was stopped due to severe drossiness at 66–70 y; Bed-bound at 66–70 y | DA drugs: none; Non-DA drugs: none | HY Stage: 5: MD-GCI-S: 6 CG-GCI-S: 64 | Sleeps for days at a time, not very cognitive when awake, has difficulty verbalizing. Does not connect with others or TV or music. Does not move, feed, or hold anything. Lacks facial expression. Vocalizes in dreams, occasionally move leg in sleep. |
| Motor Function | ||||||||
| UPDRS-III (+Score Better) | Clinician | Caregiver | ||||||
| Levodopa | PF-2562 | Levodopa | PF-2562 | Levodopa | PF-2562 | |||
| 1 | −2 | 16 | 2 | 1 | 0.2 | 0.6 | ||
| 3 | 4 | 3 | 1 | 3 | −0.3 | 1.7 | ||
| 4 | 1 | −2 | 0 | 2 | −0.2 | 1 | ||
| 7 | −1 | −2 | 0 | 0 | −0.4 | 0.4 | ||
| 8 | −14 | −24 | 2 | 4 | 2.2 | 0.4 | ||
| Alertness | ||||||||
| GCS (+score better) | SSS (−score better) | Clinician | Caregiver | |||||
| ID | Levodopa | PF-2562 | Levodopa | PF-2562 | Levodopa | PF-2562 | Levodopa | PF-2562 |
| 1 | 2 | −3 | −1 | 1 | 2 | 2 | 2 | 3 |
| 3 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 3 |
| 4 | 1 | −1 | −1 | 1 | 1 | 3 | −1 | 2 |
| 7 | 0 | 0 | −1 | 0 | 0 | 0 | 0 | 1 |
| 8 | −6 | −3 | −4 | −2 | 2 | 0 | 3 | 1 |
| Cognitive function | ||||||||
| SIB (+score better) | FAB (+score better) | Clinician | Caregiver | |||||
| ID | Levodopa | PF-2562 | Levodopa | PF-2562 | Levodopa | PF-2562 | Levodopa | PF-2562 |
| 1 | 0 | 0 | −3 | 0 | 1 | 1 | 0 | 0.7 |
| 3 | −1 | 1 | 1 | −3 | 0 | 1 | 0 | 1.7 |
| 4 | −1 | 1 | 3 | −3 | −1 | 3 | −0.5 | 1.5 |
| 7 | 0 | 0 | 1 | −2 | 0 | 0 | −0.3 | 0 |
| 8 | 0 | 0 | −3 | 0 | 1 | 0 | 1.7 | 0.2 |
| Sleep | ||||||||
| SE (+score better) | Clinician | Caregiver | ||||||
| Levodopa | PF-2562 | Levodopa | PF-2562 | Levodopa | PF-2562 | |||
| 1 | −3.4 | −9.4 | 2 | 0 | 1 | 3 | ||
| 3 | N/A | N/A | 0 | 0 | 0 | 2 | ||
| 4 | N/A | N/A | 0 | 0 | 0 | 0 | ||
| 7 | 0.5 | −6 | 0 | 0 | −1 | 2 | ||
| 8 | 33.5 | 32.7 | 2 | 0 | 1 | 0 | ||
| Data Transformation | Additional Qualitative Insights | Quotes | ||
|---|---|---|---|---|
| Subject 1 | Levodopa | Improved cognitive engagement (alertness/cognition) Improved motor and strength Either mildly improved or no ∆ swallowing | CG notes that patient was more alert and social than at home, but also attributes this to a change in environment and rigidity of schedule, increased stimulation from staff. Patient looking around room, calling staff by name, and had improved facial expressions and movements. More closed mouth (‘peaceful’) breathing. Unclear if changes in sleep or napping. | “…he is certainly more alert and aware, however it’s comparable to when he has a really good day at home” “…the high point was…, where he picked the hat up and… trying very hard to put it on…he reached out and took hold of [research assistant’s] hand,…looked at him,….attended to him, and… asked [him] for the hat…that was probably the most…purposeful activity we have seen in a while”. |
| PF-2562 | Improved cognitive engagement (alertness/cognition) Improved motor and strength Either mildly improved or unchanged swallowing | Has had some moments of alertness at home, but not nearly as long as here. Try to speak, had improved alertness and cognition, better movements and strength when pushing things away. Jerking movements of arms. Less drooling. Unclear if changes in sleep or napping | “…I was enjoying the alertness and interaction during, and it was so long…really good to have him that alert” “… he definitely engaged [more}…if you spoke to him, he would turn back… those moments are shorter at home”. “He could set his foot up so his knee was up high,… cross his legs, and I have seen him at home struggle to cross his legs… there are a couple of very purposeful things that actually worked both yesterday…& this afternoon”. | |
| Subject 3 | Levodopa | No ∆ cognitive engagement (alertness/cognition), movement Wax & wane in facial expression No ∆ swallowing or breathing | Overall, no major changes Needs assistance with balance, standing, walking Worse toe tapping | “I would say [alertness has been] the same as at home”. “We went around last evening and he froze up a good bit…the same as at home…instead of [MD] just holding on to him a little…, he did okay, but it’s not like last [PF] week… just the same as home, he’s not real steady. Somebody definitely has to hold on to him or he’d fall”. |
| PF-2562 | Improved cognitive engagement (alertness/cognition) Improved facial expression Improved movement and muscle weakness No ∆ swallowing or breathing | Much improved walking compared to home, able to do side steps, he was ‘walking right along’ (with MD) Improved mood and alertness; able to pay attention and follow along with a TV show Smiling for first time in 2 years Less messy eating, eating well with a spoon | “I see his personality today. like before he got Parkinson’s…he was just a lot of fun and [came] up with wise cracks and stuff and he was just like his old self today…” “We couldn’t believe how good he was walking here. Even made the side steps to come back and get on his chair again, so that was definitely an improvement from home”. | |
| Subject 4 | Levodopa | No ∆ in facial expression Mild/slight improved cognitive engagement (alertness/cognition), movement | Difficult to assess changes because she commonly has peaks and valleys Wax and wane at baseline. Somewhat improved focus on walking | “…it’s not terribly far off from home…I would say that on average she has been as good if not just a hair better here”. “I would say slightly better here…but even here, she is off crashing into things”. |
| PF-2562 | No ∆ in cognitive engagement (alertness/cognition) or waxing and waning Worse facial expression | Appears less erratic, less waxing and waning. More consistent focus, less distraction on her tasks Very deep sleep, nearly unresponsive, urinated in bed | “She is more consistently off– there are still ups and downs but it’s less distant between the peaks and valleys”. | |
| Subject 7 | Levodopa | Worse cognitive engagement (alertness/cognition) Worse movements No ∆ in balance No ∆ in bladder | Overall, more lethargic and worse cognition, although some improved alertness on day 2 that CG attributes to posture in chair and new setting; became more lethargic once acclimated, hard to arouse Twitching and jumpy during sleep | “We could not arouse him….he was a little bit interactive with the ice water and then [research assistant] finally just got real in his face and started talking to him in that man voice… that was the first time he opened his eyes. It was taking him longer sometimes to come up with what he wanted to say”. “He was twitching and jumping…I have never seen that”. |
| PF-2562 | Improved cognitive engagement:(alertness/cognition) and facial expression. Worse movements and strength Improved balance | Better mood and interaction, felt ‘energized’ and ‘optimistic’ although notes some grogginess on Day 2. Interactions and stimulation have been helpful. Slower movements and muscle weakness More frequent urination, sensed need to go | “He said ‘I feel energized, I feel excited about today. I feel like doing things’ a couple of times”. I think the movements are a little bit slower than when he is on his typical [meds]…the pace has been pretty slow but…he hasn’t been losing his balance. He has been…much better today” [with regards to balance]. | |
| Subject 8 | Levodopa | Improved cognitive engagement (alertness/cognition) Improved facial expressions Improved movements Unclear ∆ twitching | Dramatic response in alertness, responsiveness, memory, and communication Shook someone’s hand to greet them, able to move more Became more tired and lethargic as day wore on | “Today it seemed to change completely. He made conversation, he greeted people…he responded to questions and could bring up some memories and verbalize them… it’s a big change today”. “That’s something a little new [twitching], it’s not that he has never done it at home… he jerks, but, yeah, he has been twitching and jerking quite a bit here…I wouldn’t say it’s increased necessarily. Today right now we are seeing quite a bit of it, but last week was more”. |
| PF-2562 | No ∆ or improved cognitive engagement (alertness/cognition) No ∆ facial expression No ∆ swallowing Waxing and waning movements and rigidity | Worse twitching of arms and legs No major changes noted by CG CG notes increased stimulation from environment | “[He] has been very stimulated… so many people coming and going and all the activity, a lot more than he gets at home…but I don’t think it is any different than what he would have responded to before”. “I don’t see a big change in [movement or muscle tone]……he’s been very stiff, very rigid, um, but I think this morning he was a little looser…When he was examined, things seem to be better, but he’s back to being very stiff and rigid”. “Um…he was very twitchy today which was something new”. |
| Domain of Interest | Quantitative | Qualitative | Data Integration | Conclusion | ||
|---|---|---|---|---|---|---|
| Rater | Clinician | Caregiver | ||||
| Scale | GCI | GCI | Interview | |||
| Motor | Equivocal | Equivocal | Favored PF-2562 in first 4 subjects | Favored PF-2562 in first 4 subjects | PF-2562 was superior to levodopa, according to caregiver data. |
|
| Alertness | Equivocal | Equivocal | Favored PF-2562 in first 4 subjects | Favored PF-2562 in first 4 subjects | PF-2562 was superior to levodopa, according to caregiver data. | |
| Cognition | Equivocal | Equivocal | Favored PF-2562 in first 4 subjects | Favored PF-2562 in first 4 subjects | PF-2562 was superior to levodopa, according to caregiver data. | |
| Sleep | Incomplete | Equivocal | Equivocal | Equivocal | Sleep data is incomplete and equivocal between the two drugs. | |
| Ligand | Emax Adenylate Cyclase Stimulation (% Dopamine) | Emax β-Arrestin Recruitment (% Dopamine) |
|---|---|---|
| PF-2562 | 41 ± 15% | ND |
| Dopamine | 100 ± 9% | 100 ± 3% |
| Dihydrexidine | 103 ± 14 | 210 ± 25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewis, M.M.; Van Scoy, L.J.; De Jesus, S.; Hakun, J.G.; Eslinger, P.J.; Fernandez-Mendoza, J.; Kong, L.; Yang, Y.; Snyder, B.L.; Loktionova, N.; et al. Dopamine D1 Agonists: First Potential Treatment for Late-Stage Parkinson’s Disease. Biomolecules 2023, 13, 829. https://doi.org/10.3390/biom13050829
Lewis MM, Van Scoy LJ, De Jesus S, Hakun JG, Eslinger PJ, Fernandez-Mendoza J, Kong L, Yang Y, Snyder BL, Loktionova N, et al. Dopamine D1 Agonists: First Potential Treatment for Late-Stage Parkinson’s Disease. Biomolecules. 2023; 13(5):829. https://doi.org/10.3390/biom13050829
Chicago/Turabian StyleLewis, Mechelle M., Lauren J. Van Scoy, Sol De Jesus, Jonathan G. Hakun, Paul J. Eslinger, Julio Fernandez-Mendoza, Lan Kong, Yang Yang, Bethany L. Snyder, Natalia Loktionova, and et al. 2023. "Dopamine D1 Agonists: First Potential Treatment for Late-Stage Parkinson’s Disease" Biomolecules 13, no. 5: 829. https://doi.org/10.3390/biom13050829