
Effects of Exercise on Inflammatory Markers in Individuals with Chronic Kidney Disease: A Systematic Review and Meta-Analysis
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration and Protocol
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Methodological Assessment
2.6.1. PEDro
2.6.2. Quality of Evidence
2.7. Data Analysis
3. Results
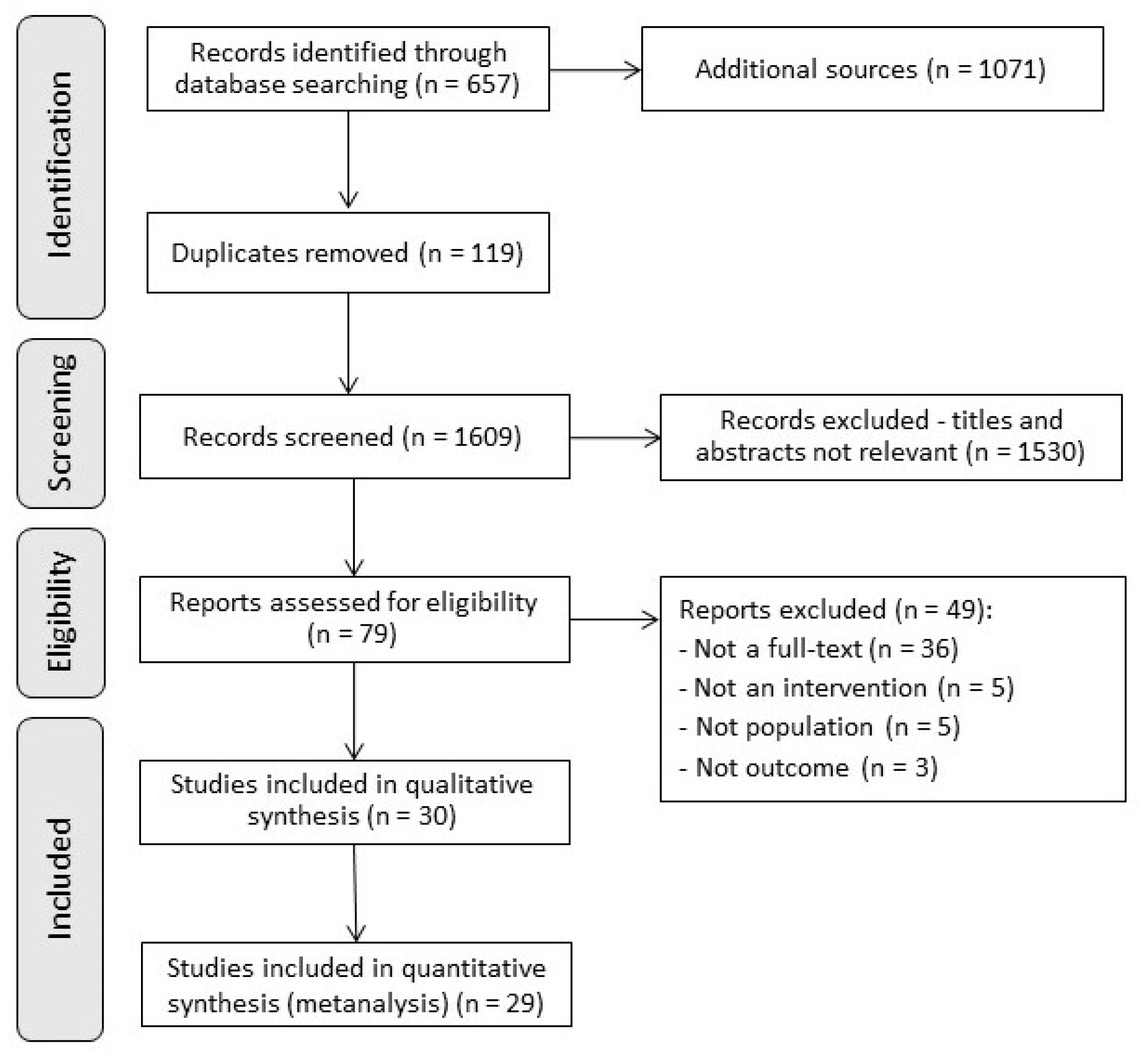
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.2.1. Participants
3.2.2. Intervention
3.2.3. Methodological Quality
3.2.4. Quality of Evidence
3.2.5. Publication Bias
3.2.6. Inflammatory Markers
3.3. Interventions Effects
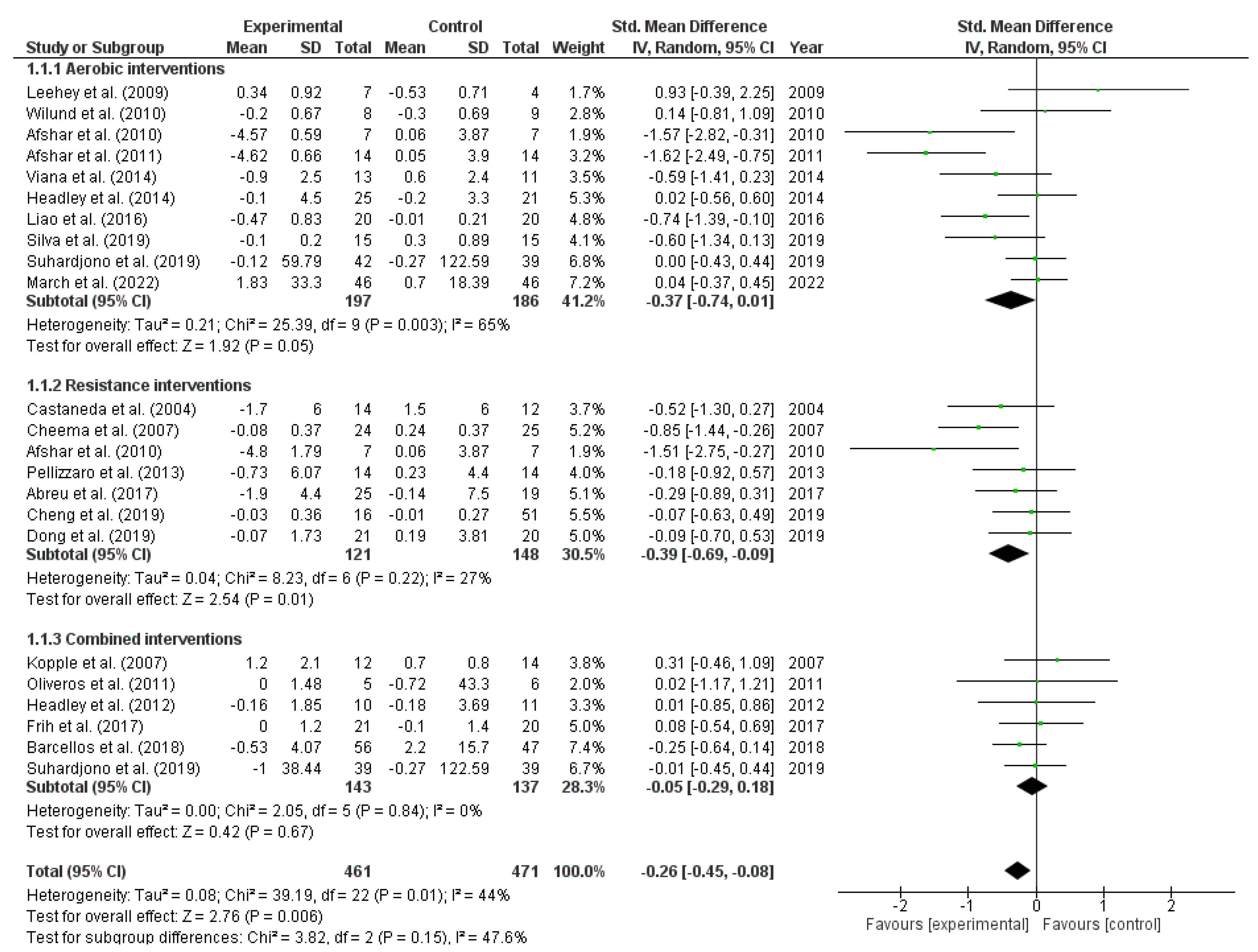
3.3.1. Exercise Effects on C-Reactive Protein
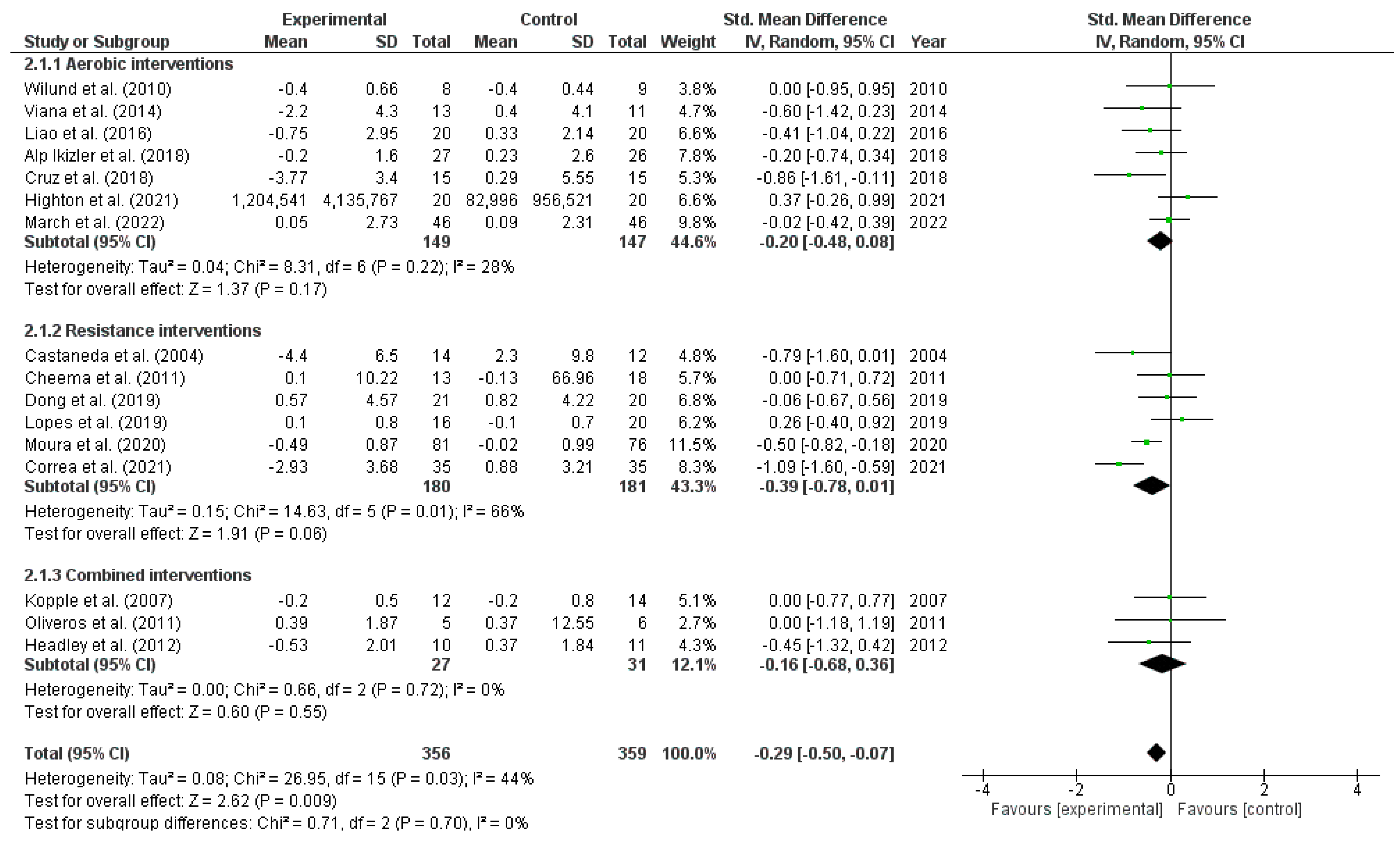
3.3.2. Exercise Effects on Interleukin 6
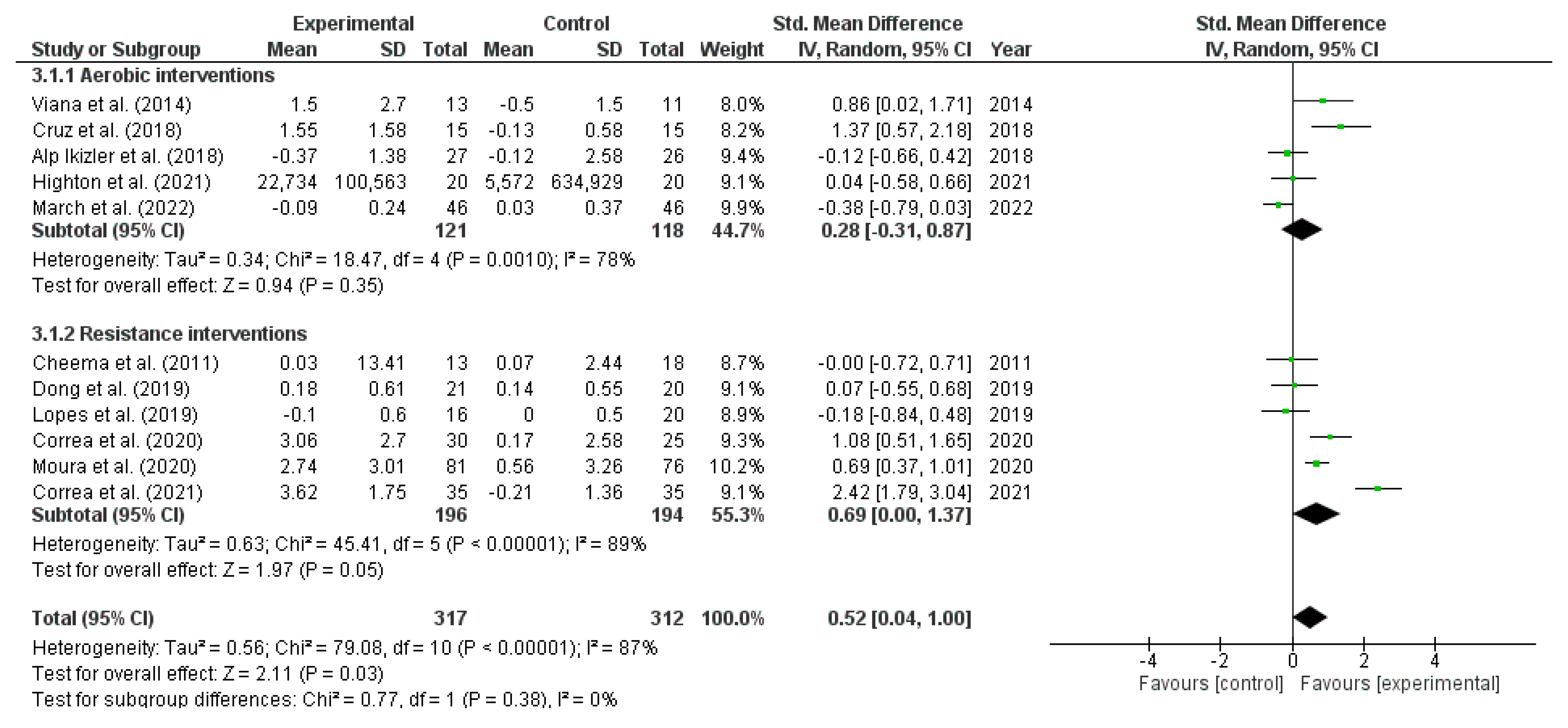
3.3.3. Exercise Effects on Interleukin 10
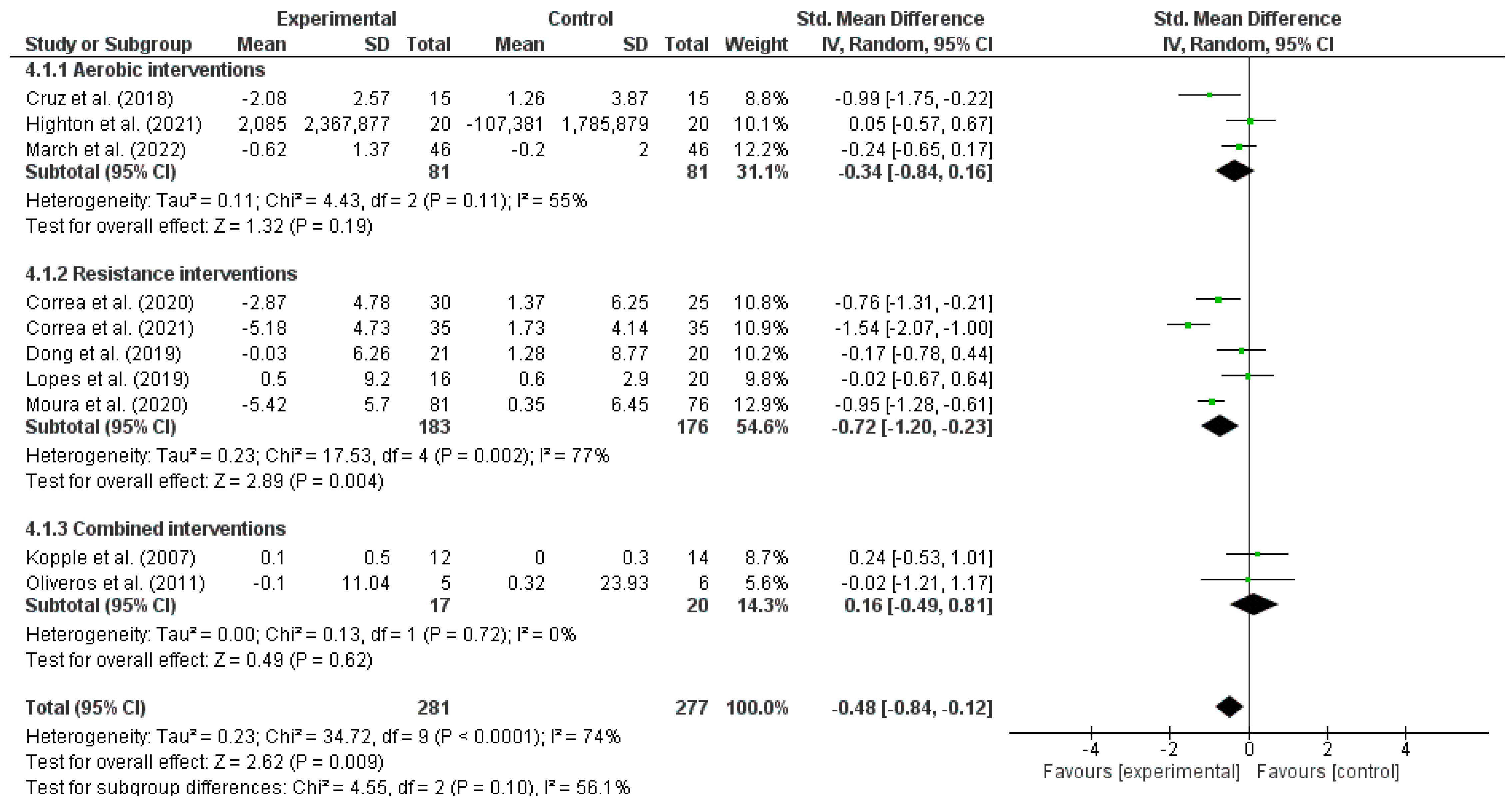
3.3.4. Exercise Effects on Tumor Necrosis Factor-Alpha
4. Discussion
4.1. Main Findings
4.2. Interventions Effects
4.2.1. C-Reactive Protein
4.2.2. Interleukin 6
4.2.3. Interleukin 10
4.2.4. Tumor Necrosis Factor-Alpha
4.3. Clinical Applicability
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akchurin, O.M.; Kaskel, F. Update on inflammation in chronic kidney disease. Blood Purif. 2015, 39, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Bazeley, J.; Bieber, B.; Li, Y.; Morgenstern, H.; de Sequera, P.; Combe, C.; Yamamoto, H.; Gallagher, M.; Port, F.K.; Robinson, B.M. C-Reactive Protein and Prediction of 1-Year Mortality in Prevalent Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 2452–2461. [Google Scholar] [CrossRef] [Green Version]
- Mihai, S.; Codrici, E.; Popescu, I.D.; Enciu, A.-M.; Albulescu, L.; Necula, L.G.; Mambet, C.; Anton, G.; Tanase, C. Inflammation-related mechanisms in chronic kidney disease prediction, progression, and outcome. J. Immunol. Res. 2018, 2018, 2180373. [Google Scholar] [CrossRef] [Green Version]
- Moura, S.R.G.; Corrêa, H.L.; Neves, R.V.P.; Santos, C.A.R.; Neto, L.S.S.; Silva, V.L.; Souza, M.K.; Deus, L.A.; Reis, A.L.; Simões, H.G.; et al. Effects of resistance training on hepcidin levels and iron bioavailability in older individuals with end-stage renal disease: A randomized controlled trial. Exp. Gerontol. 2020, 139, 111017. [Google Scholar] [CrossRef]
- Leal, D.V.; Ferreira, A.; Watson, E.L.; Wilund, K.R.; Viana, J.L. Muscle-Bone Crosstalk in Chronic Kidney Disease: The Potential Modulatory Effects of Exercise. Calcif. Tissue Int. 2021, 108, 461–475. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.P.; Ribeiro, H.S.; Neri, S.G.R.; Almeida, L.S.; Oliveira, J.S.; Viana, J.L.; Lima, R.M. Prevalence of low bone mineral density (T-score ≤ −2.5) in the whole spectrum of chronic kidney disease: A systematic review and meta-analysis. Osteoporos. Int. 2023, 34, 467–477. [Google Scholar] [CrossRef]
- Vianna, H.R.; Soares, C.M.B.M.; Tavares, M.S.; Teixeira, M.M.; Silva, A.C.S.e. Inflamação na doença renal crônica: Papel de citocinas. J. Bras. Nefrol. 2011, 33, 351–364. [Google Scholar] [CrossRef] [Green Version]
- Andrade-Oliveira, V.; Foresto-Neto, O.; Watanabe, I.K.M.; Zatz, R.; Câmara, N.O.S. Inflammation in renal diseases: New and old players. Front. Pharmacol. 2019, 10, 1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, B.K. Muscles and their myokines. J. Exp. Biol. 2011, 214, 337–346. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–610. [Google Scholar] [CrossRef]
- Dai, L.; Golembiewska, E.; Lindholm, B.; Stenvinkel, P. End-Stage Renal Disease, Inflammation and Cardiovascular Outcomes. Contrib. Nephrol. 2017, 191, 32–43. [Google Scholar]
- Jesus, J.; Mahmut, C.; Yilmaz, I.; Lindholm, B.; Stenvinkel, P. Cytokine Dysregulation in Chronic Kidney Disease: How Can We Treat It? Blood Purif. 2008, 26, 291–299. [Google Scholar]
- Cheema, B.S.B.; Abas, H.; Smith, B.C.F.; O’sullivan, A.J.; Chan, M.; Patwardhan, A.; Kelly, J.; Gillin, A.; Pang, G.; Lloyd, B.; et al. Effect of resistance training during hemodialysis on circulating cytokines: A randomized controlled trial. Eur. J. Appl. Physiol. 2011, 111, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Cruz LG da Zanetti, H.R.; Andaki, A.C.R.; Mota GR da Barbosa Neto, O.; Mendes, E.L. Intradialytic aerobic training improves inflammatory markers in patients with chronic kidney disease: A randomized clinical trial. Mot. Rev. Educ. Física. 2018, 24, 1–5. [Google Scholar]
- Mendes, S.; Leal, D.V.; Baker, L.A.; Ferreira, A.; Smith, A.C.; Viana, J.L. The Potential Modulatory Effects of Exercise on Skeletal Muscle Redox Status in Chronic Kidney Disease. Int. J. Mol. Sci. 2023, 24, 6017. [Google Scholar] [CrossRef]
- Bishop, N.C.; Burton, J.O.; Graham-Brown, M.P.M.; Stensel, D.J.; Viana, J.L.; Watson, E.L. Exercise and chronic kidney disease: Potential mechanisms underlying the physiological benefits. Nat. Rev. Nephrol. 2023, 19, 244–256. [Google Scholar] [CrossRef]
- Petersen, A.M.W.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Barcellos, F.C.; Del Vecchio, F.B.; Reges, A.; Mielke, G.; Santos, I.S.; Umpierre, D.; Bohlke, M.; Hallal, P. Exercise in patients with hypertension and chronic kidney disease: A randomized controlled trial. J. Hum. Hypertens. 2018, 32, 397–407. [Google Scholar] [CrossRef]
- Oliveira ESilva, V.R.; Stringuetta Belik, F.; Hueb, J.C.; de Souza Gonçalves, R.; Costa Teixeira Caramori, J.; Perez Vogt, B.; Barretti, P.; Zanati Bazan, S.G.; De Stefano, G.M.M.F.; Martin, L.C.; et al. Aerobic Exercise Training and Nontraditional Cardiovascular Risk Factors in Hemodialysis Patients: Results from a Prospective Randomized Trial. Cardiorenal Med. 2019, 9, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, H.L.; Moura, S.R.G.; Neves, R.V.P.; Tzanno-Martins, C.; Souza, M.K.; Haro, A.S.; Costa, F.; Silva, J.A.B.; Stone, W.; Honorato, F.S.; et al. Resistance training improves sleep quality, redox balance and inflammatory profile in maintenance hemodialysis patients: A randomized controlled trial. Sci. Rep. 2020, 10, 11708. [Google Scholar] [CrossRef]
- Viana, J.L.; Kosmadakis, G.C.; Watson, E.L.; Bevington, A.; Feehally, J.; Bishop, N.C.; Smith, A.C. Evidence for Anti-Inflammatory Effects of Exercise in CKD. J. Am. Soc. Nephrol. 2014, 25, 2121–2130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S.; Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Green, S., Eds.; Cochrane Book Series; John Wiley & Sons, Ltd.: Chichester, UK, 2008. [Google Scholar]
- Dungey, M.; Hull, K.L.; Smith, A.C.; Burton, J.O.; Bishop, N.C. Inflammatory factors and exercise in chronic kidney disease. Int. J. Endocrinol. 2013, 2013, 569831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. (Eds.) GRADE handbook for grading quality of evidence and strength of recommendations. The GRADE Working Group, 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 10 January 2022).
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G.; Cochrane Statistical Methods Group. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Chichester, UK, 2019; Volume 5. [Google Scholar]
- Pellizzaro, C.O.; Thomé, F.S.; Veronese, F.V. Effect of peripheral and respiratory muscle training on the functional capacity of hemodialysis patients. Ren. Fail. 2013, 35, 189–197. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Robinson-Cohen, C.; Ellis, C.; Headley, S.A.; Tuttle, K.; Wood, R.J.; Evans, E.E.; Milch, C.M.; Moody, K.A.; Germain, M.; et al. Metabolic Effects of Diet and Exercise in Patients with Moderate to Severe CKD: A Randomized Clinical Trial. J. Am. Soc. Nephrol. 2018, 29, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Dong, Z.J.; Zhang, H.L.; Yin, L.X. Effects of intradialytic resistance exercise on systemic inflammation in maintenance hemodialysis patients with sarcopenia: A randomized controlled trial. Int. Urol. Nephrol. 2019, 51, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Lopes, L.C.C.; Mota, J.F.; Prestes, J.; Schincaglia, R.M.; Silva, D.M.; Queiroz, N.P.; Freitas, A.T.V.D.S.; Lira, F.D.S.; Peixoto, M.D.R.G. Intradialytic Resistance Training Improves Functional Capacity and Lean Mass Gain in Individuals on Hemodialysis: A Randomized Pilot Trial. Arch Phys. Med. Rehabil. 2019, 100, 2151–2158. [Google Scholar] [CrossRef]
- Suhardjono Umami, V.; Tedjasukmana, D.; Setiati, S. The effect of intradialytic exercise twice a week on the physical capacity, inflammation, and nutritional status of dialysis patients: A randomized controlled trial. Hemodial. Int. 2019, 23, 486–493. [Google Scholar] [CrossRef]
- Headley, S.; Germain, M.; Milch, C.; Pescatello, L.; Coughlin, M.A.; Nindl, B.C.; Cornelius, A.; Sullivan, S.; Gregory, S.; Wood, R. Exercise Training Improves HR Responses and V˙O2peak in Predialysis Kidney Patients. Med. Sci. Sport Exerc. 2012, 44, 2392–2399. [Google Scholar] [CrossRef]
- Headley, S.; Germain, M.; Wood, R.; Joubert, J.; Milch, C.; Evans, E.; Poindexter, A.; Cornelius, A.; Brewer, B.; Pescatello, L.S.; et al. Short-term aerobic exercise and vascular function in CKD stage 3: A randomized controlled trial. Am. J. Kidney Dis. 2014, 64, 222–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, C.; Cardozo, L.; Stockler-Pinto, M.; Esgalhado, M.; Barboza, J.; Frauches, R.; Mafra, D. Does resistance exercise performed during dialysis modulate Nrf2 and NF-κB in patients with chronic kidney disease? Life Sci. 2017, 188, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Liao, M.-T.; Liu, W.-C.; Lin, F.-H.; Huang, C.-F.; Chen, S.-Y.; Liu, C.-C.; Lin, S.-H.; Lu, K.-C.; Wu, C.-C. Intradialytic aerobic cycling exercise alleviates inflammation and improves endothelial progenitor cell count and bone density in hemodialysis patients. Medicine 2016, 95, e4134. [Google Scholar] [CrossRef] [PubMed]
- Leehey, D.J.; Moinuddin, I.; Bast, J.P.; Qureshi, S.; Jelinek, C.S.; Cooper, C.; Edwards, L.C.; Smith, B.M.; Collins, E.G. Aerobic exercise in obese diabetic patients with chronic kidney disease: A randomized and controlled pilot study. Cardiovasc. Diabetol. 2009, 8, 62–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilund, K.R.; Tomayko, E.J.; Wu, P.-T.; Chung, H.R.; Vallurupalli, S.; Lakshminarayanan, B.; Fernhall, B. Intradialytic exercise training reduces oxidative stress and epicardial fat: A pilot study. Nephrol. Dial. Transplant. 2010, 25, 2695–2701. [Google Scholar] [CrossRef] [Green Version]
- Cheema, B.; Abas, H.; Smith, B.; O’Sullivan, A.; Chan, M.; Patwardhan, A.; Kelly, J.; Gillin, A.; Pang, G.; Lloyd, B.; et al. Progressive exercise for anabolism in kidney disease (PEAK): A randomized, controlled trial of resistance training during hemodialysis. J. Am. Soc. Nephrol. 2007, 18, 1594–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frih, B.; Jaafar, H.; Mkacher, W.; Salah ZBen Hammami, M.; Frih, A. The effect of interdialytic combined resistance and aerobic exercise training on health related outcomes in chronic hemodialysis patients: The Tunisian randomized controlled study. Front Physiol. 2017, 8, 288. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Zhao, X.J.; Zeng, W.; Xu, M.C.; Ma, Y.C.; Wang, M. Effect of Intradialytic Exercise on Physical Performance and Cardiovascular Risk Factors in Patients Receiving Maintenance Hemodialysis: A Pilot and Feasibility Study. Blood Purif. 2020, 49, 409–418. [Google Scholar] [CrossRef]
- Corrêa, H.L.; Neves, R.V.P.; Deus, L.A.; Souza, M.K.; Haro, A.S.; Costa, F.; Silva, V.L.; Santos, C.A.R.; Moraes, M.R.; Simões, H.G.; et al. Blood Flow Restriction Training Blunts Chronic Kidney Disease Progression in Humans. Med. Sci. Sport Exerc. 2021, 53, 249–257. [Google Scholar] [CrossRef]
- Afshar, R.; Shegarfy, L.; Shavandi, N.; Sanavi, S. Effects of aerobic exercise and resistance training on lipid profiles and inflammation status in patients on maintenance hemodialysis. Indian J. Nephrol. 2010, 20, 185–189. [Google Scholar]
- Zhao, C.; Ma, H.; Yang, L.; Xiao, Y. Long-term bicycle riding ameliorates the depression of the patients undergoing hemodialysis by affecting the levels of interleukin-6 and interleukin-18. Neuropsychiatr. Dis. Treat 2016, 13, 91–100. [Google Scholar] [CrossRef] [Green Version]
- March, D.S.; Lai, K.-B.; Neal, T.; Graham-Brown, M.P.M.; Highton, P.J.; Churchward, D.R.; Young, H.M.L.; Dungey, M.; Stensel, D.J.; Smith, A.C.; et al. Circulating endotoxin and inflammation: Associations with fitness, physical activity and the effect of a 6-month programme of cycling exercise during haemodialysis. Nephrol. Dial. Transplant. 2022, 37, 366–374. [Google Scholar] [CrossRef]
- Highton, P.J.; March, D.S.; Churchward, D.R.; Grantham, C.E.; Young, H.M.L.; Graham-Brown, M.P.M.; Estruel, S.; Martin, N.; Brunskill, N.J.; Smith, A.C.; et al. Intradialytic cycling does not exacerbate microparticles or circulating markers of systemic inflammation in haemodialysis patients. Eur. J. Appl. Physiol. 2021, 122, 599–609. [Google Scholar] [CrossRef]
- Kopple, J.D.; Wang, H.; Casaburi, R.; Fournier, M.; Lewis, M.I.; Taylor, W.; Storer, T.W. Exercise in maintenance hemodialysis patients induces transcriptional changes in genes favoring anabolic muscle. J. Am. Soc. Nephrol. 2007, 18, 2975–2986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshar, R.; Emany, A.; Saremi, A.; Shavandi, N.; Sanavi, S. Effects of intradialytic aerobic training on sleep quality in hemodialysis patients. Iran J. Kidney Dis. 2011, 5, 119–123. [Google Scholar] [PubMed]
- Castaneda, C.; Gordon, P.L.; Parker, R.C.; Uhlin, K.L.; Roubenoff, R.; Levey, A.S. Resistance Training to Reduce the Malnutrition-Inflammation Complex Syndrome of Chronic Kidney Disease. Am. J. Kidney Dis. 2004, 43, 607–616. [Google Scholar] [CrossRef]
- Oliveros, M.S.; Avendaño, M.; Bunout Barnett, D.; Hirsch Birn, S.; Maza Cave, M.P.D.L.; Pedreros, C.; Müller, H. A pilot study on physical training of patients in Hemodialysis Estudio piloto sobre entrenamiento físico durante hemodiálisis. Rev. Med. Chil. 2011, 139, 1046–1053. [Google Scholar] [CrossRef]
- Li, W.-J.; Chen, X.-M.; Nie, X.-Y.; Zhang, J.; Cheng, Y.-J.; Lin, X.-X.; Wu, S.-H. Cardiac troponin and C-reactive protein for predicting all-cause and cardiovascular mortality in patients with chronic kidney disease: A meta-analysis. Clinics 2015, 70, 301–311. [Google Scholar] [CrossRef]
- Grgic, J.; Mcllvenna, L.C.; Fyfe, J.J.; Sabol, F.; Bishop, D.J.; Schoenfeld, B.J.; Pedisic, Z. Does Aerobic Training Promote the Same Skeletal Muscle Hypertrophy as Resistance Training? A Systematic Review and Meta-Analysis. Sport Med. 2019, 49, 233–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [Green Version]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon RO 3rd Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; Rifai, N.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the centers for disease control and prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Mitra, N.; Kanetsky, P.A.; Devaney, J.; Wing, M.R.; Reilly, M.; Shah, V.O.; Balakrishnan, V.S.; Guzman, N.J.; Girndt, M.; et al. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin. J. Am. Soc. Nephrol. 2012, 7, 1938–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonelli, M.; Sacks, F.; Pfeffer, M.; Jhangri, G.S.; Curhan, G. Biomarkers of inflammation and progression of chronic kidney disease. Kidney Int. 2005, 68, 237–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Liu, Y.; Wu, L.; Yang, J.; Jiang, T.; Li, M. Effects of exercise on markers of inflammation and indicators of nutrition in patients with chronic kidney disease: A systematic review and meta-analysis. Int. Urol. Nephrol. 2021, 54, 815–826. [Google Scholar] [CrossRef]
- Schaper, F.; Rose-John, S. Interleukin-6: Biology, signaling and strategies of blockade. Cytokine Growth Factor Rev. 2015, 26, 475–487. [Google Scholar] [CrossRef]
- McKay, B.R.; De Lisio, M.; Johnston, A.P.; O’Reilly, C.E.; Phillips, S.M.; Tarnopolsky, M.A.; Parise, G. Association of interleukin-6 signalling with the muscle stem cell response following muscle-lengthening contractions in humans. PLoS ONE 2009, 4, e6027. [Google Scholar] [CrossRef] [Green Version]
- Roy, N.; Rosas, S.E. IL-6 Is Associated with Progression of Coronary Artery Calcification and Mortality in Incident Dialysis Patients. Am. J. Nephrol. 2021, 52, 745–752. [Google Scholar] [CrossRef]
- Petersen, A.M.W.; Pedersen, B.K. The role of IL-6 in mediating the anti-inflammatory effects of exercise. J. Physiol. Pharmacol. 2006, 57 (Suppl. 10), 43–51. [Google Scholar]
- Stenvinkel, P.; Ketteler, M.; Johnson, R.J.; Lindholm, B.; Pecoits-Filho, R.; Riella, M.; Heimbürger, O.; Cederholm, T.; Girndt, M. IL-10, IL-6, and TNF-α: Central factors in the altered cytokine network of uremia—The good, the bad, and the ugly. Kidney Int. 2005, 67, 1216–1233. [Google Scholar] [CrossRef] [Green Version]
- Dungey, M.; Bishop, N.C.; Young, H.M.L.; Burton, J.O.; Smith, A.C. The Impact of Exercising during Haemodialysis on Blood Pressure, Markers of Cardiac Injury and Systemic Inflammation–Preliminary Results of a Pilot Study. Kidney Blood Press Res. 2015, 40, 593–604. [Google Scholar] [CrossRef] [Green Version]
- Opal, S.M.; DePalo, V.A. Anti-inflammatory cytokines. Chest 2000, 117, 1162–1172. [Google Scholar] [CrossRef] [Green Version]
- Calle, M.C.; Fernandez, M.L. Effects of resistance training on the inflammatory response. Nutr. Res. Pract. 2010, 4, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todd, J.S.; Shurley, J.P.; Todd, T.C.; Thomas, L. DeLorme and the science of progressive resistance exercise. J. Strength Cond. Res. 2012, 26, 2913–2923. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, H.S.; Andrade, F.P.; Leal, D.V.; Oliveira, J.S.; Wilund, K.R.; Viana, J.L. How is exercise being prescribed for patients on hemodialysis? A scoping review. J. Nephrol. 2022. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise Intervention | Studies | Individuals | Std. Mean Difference (95% CI) | Heterogeneity (i2, %) |
|---|---|---|---|---|
| Pooled exercise interventions | ||||
| CRP | 21 | 932 | −0.26 (−0.45 to −0.08) | 44 |
| IL-6 | 16 | 715 | −0.29 (−0.50 to −0.07) | 44 |
| IL-10 | 11 | 629 | 0.52 (0.04 to 1.00) | 87 |
| TNF-α | 11 | 558 | −0.48 (−0.84 to −0.12) | 74 |
| Aerobic interventions | ||||
| CRP | 10 | 383 | −0.23 (−0.74 to 0.01) | 65 |
| IL-6 | 7 | 296 | −0.20 (−0.48 to 0.08) | 28 |
| IL-10 | 5 | 239 | 0.28 (−0.31 to 0.87) | 78 |
| TNF-α | 3 | 122 | −0.34 (−0.84 to 0.16) | 55 |
| Resistance interventions | ||||
| CRP | 7 | 269 | −0.39 (−0.69 to −0.09) | 27 |
| IL-6 | 6 | 361 | −0.39 (−0.78 to 0.01) | 66 |
| IL-10 | 6 | 390 | 0.69 (0.00 to 1.37) | 89 |
| TNF-α | 5 | 359 | −0.72 (−1.20 to −0.23) | 77 |
| Combined interventions | ||||
| CRP | 6 | 280 | −0.05 (−0.29 to 0.18) | 0 |
| IL-6 | 3 | 58 | −0.16 (−0.68 to 0.36) | 0 |
| IL-10 | 0 | 0 | - | - |
| TNF-α | 2 | 37 | 0.16 (−0.49 to 0.81) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baião, V.M.; Cunha, V.A.; Duarte, M.P.; Andrade, F.P.; Ferreira, A.P.; Nóbrega, O.T.; Viana, J.L.; Ribeiro, H.S. Effects of Exercise on Inflammatory Markers in Individuals with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Metabolites 2023, 13, 795. https://doi.org/10.3390/metabo13070795
Baião VM, Cunha VA, Duarte MP, Andrade FP, Ferreira AP, Nóbrega OT, Viana JL, Ribeiro HS. Effects of Exercise on Inflammatory Markers in Individuals with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Metabolites. 2023; 13(7):795. https://doi.org/10.3390/metabo13070795
Chicago/Turabian StyleBaião, Victor M., Vinícius A. Cunha, Marvery P. Duarte, Francini P. Andrade, Aparecido P. Ferreira, Otávio T. Nóbrega, João L. Viana, and Heitor S. Ribeiro. 2023. "Effects of Exercise on Inflammatory Markers in Individuals with Chronic Kidney Disease: A Systematic Review and Meta-Analysis" Metabolites 13, no. 7: 795. https://doi.org/10.3390/metabo13070795