
Lipidomic Analysis to Assess Oxidative Stress in Acute Coronary Syndrome and Acute Stroke Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
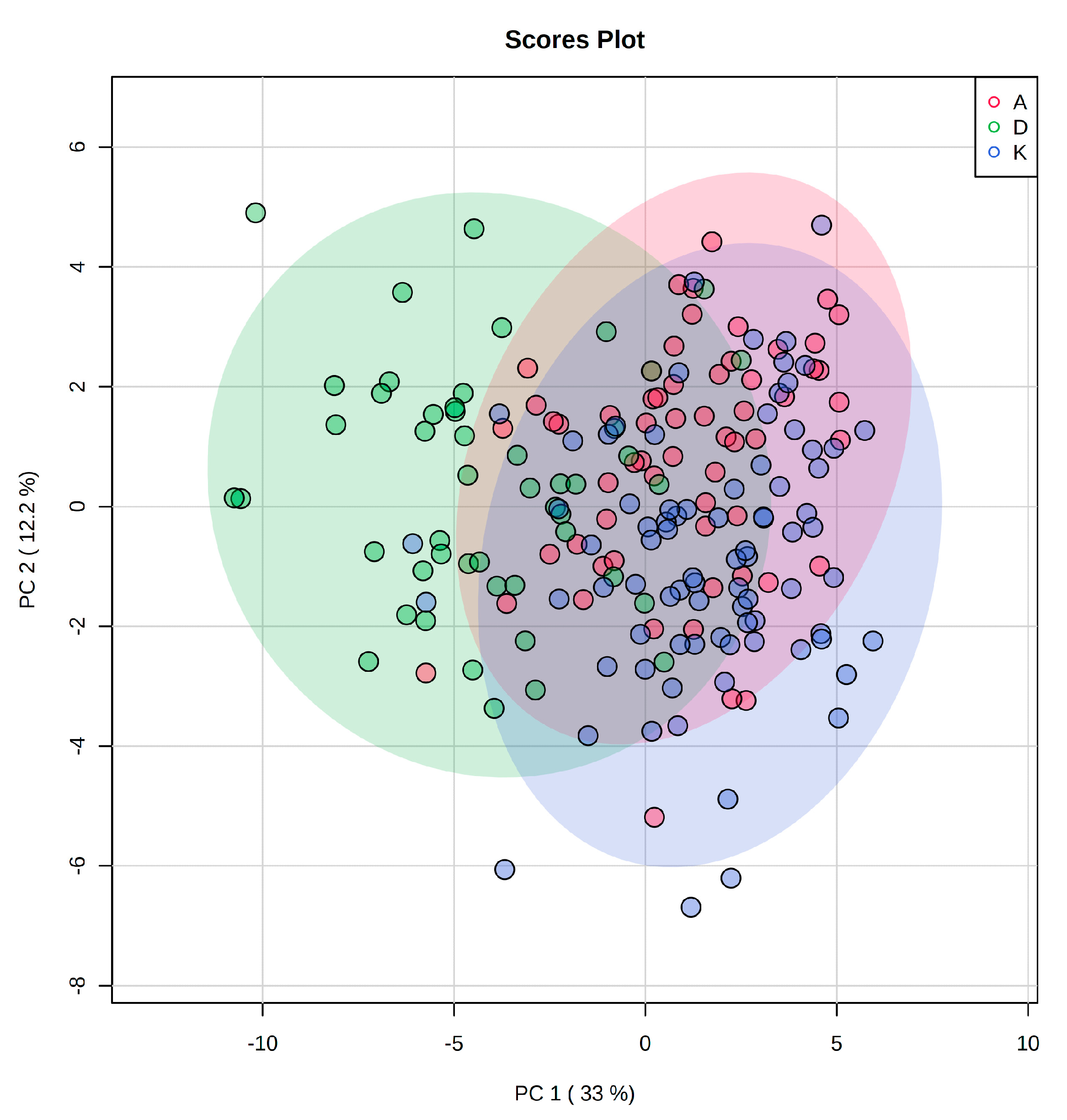
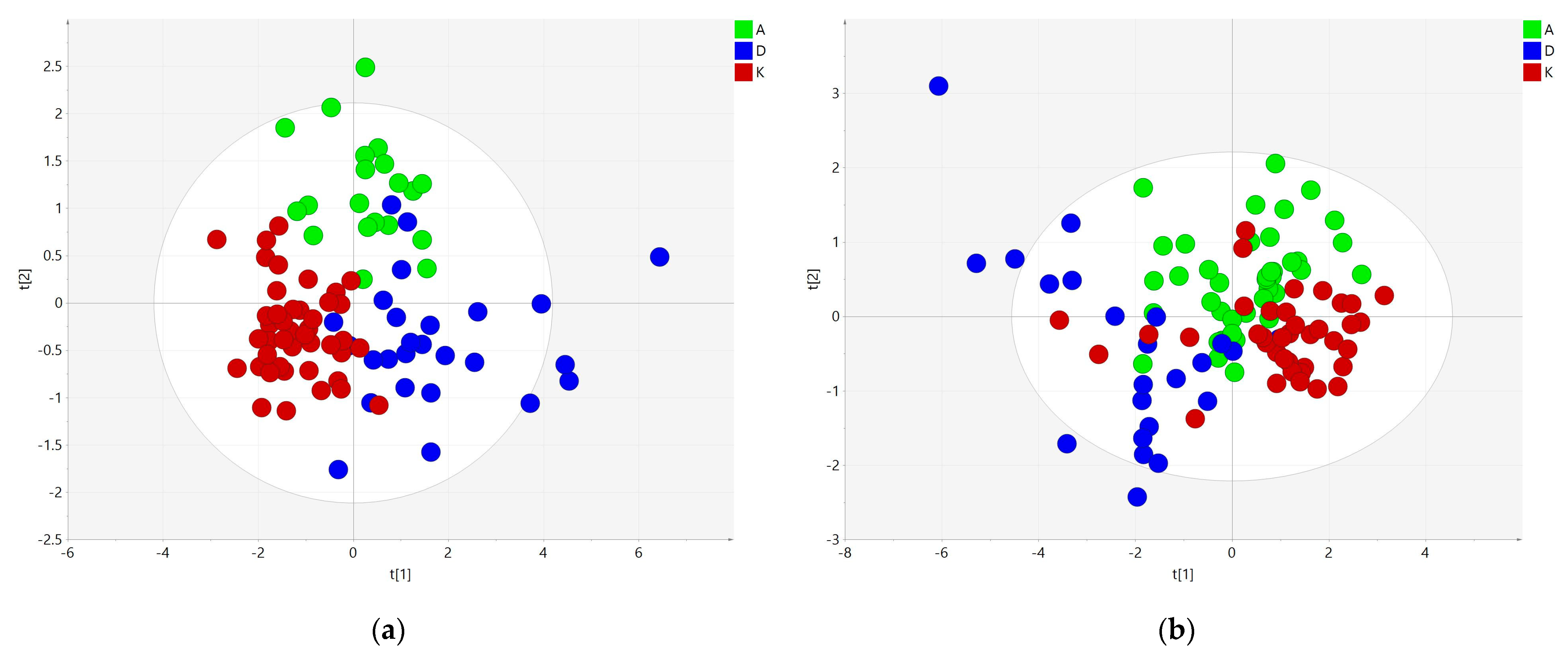
2.1. Multivariate Analysis for Data Overview
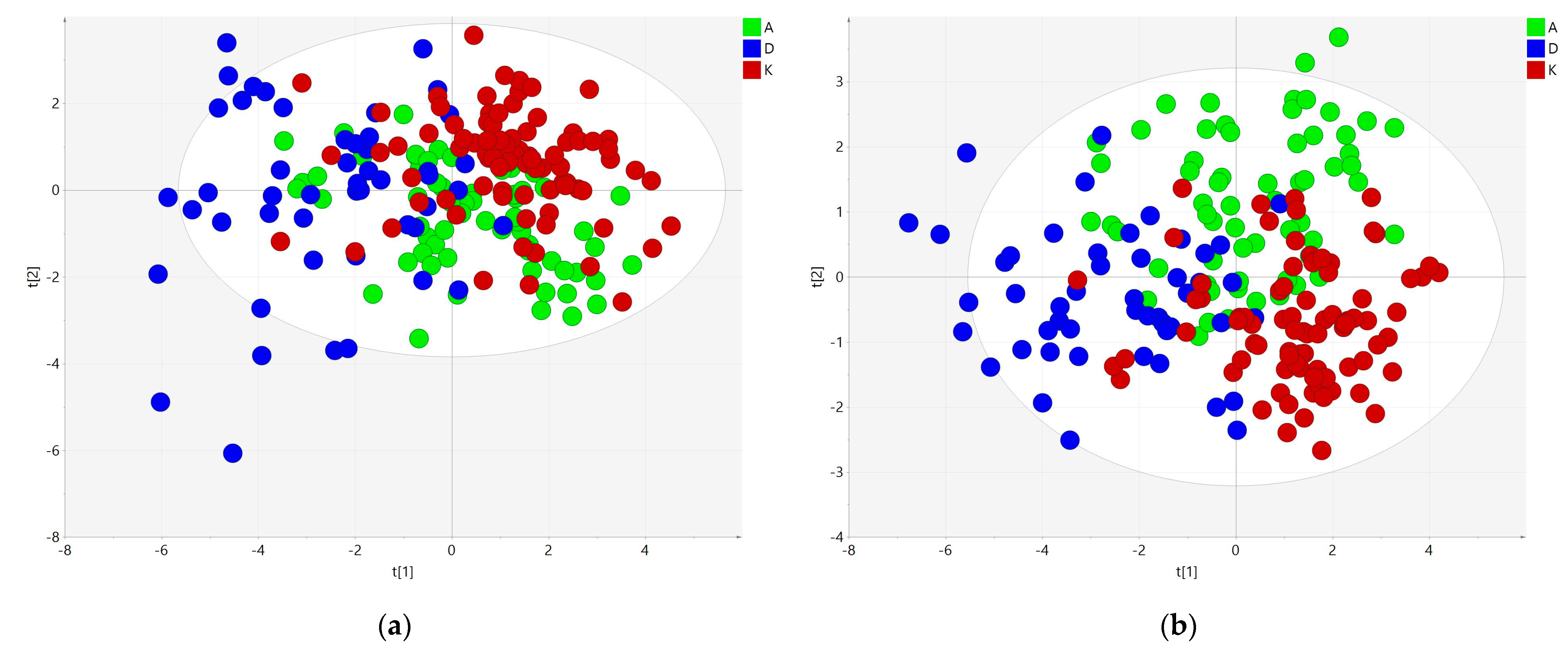
2.2. Supervised Statistical Analysis of All Lipidome Components
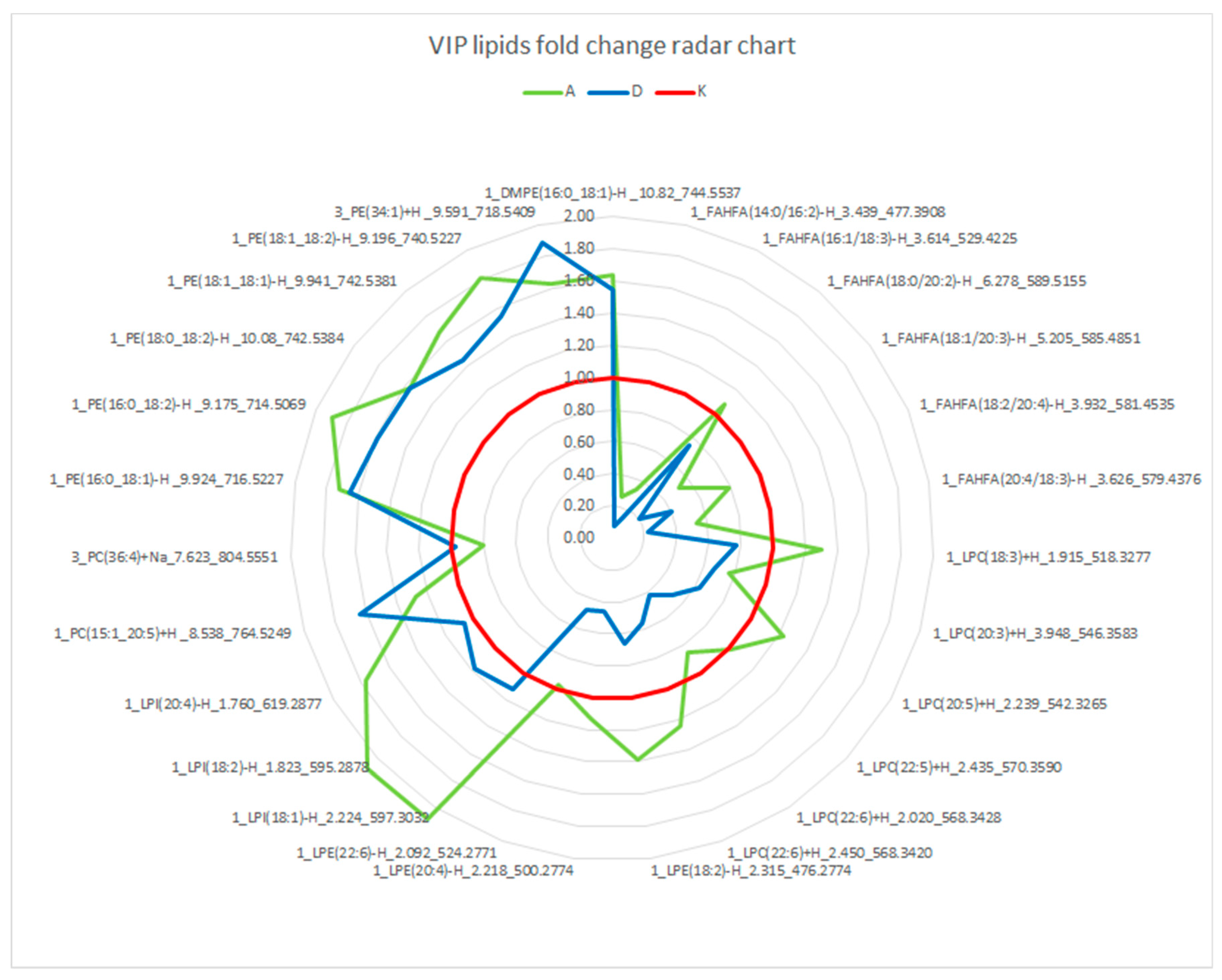
2.3. Analysis of Polar Lipids Subset
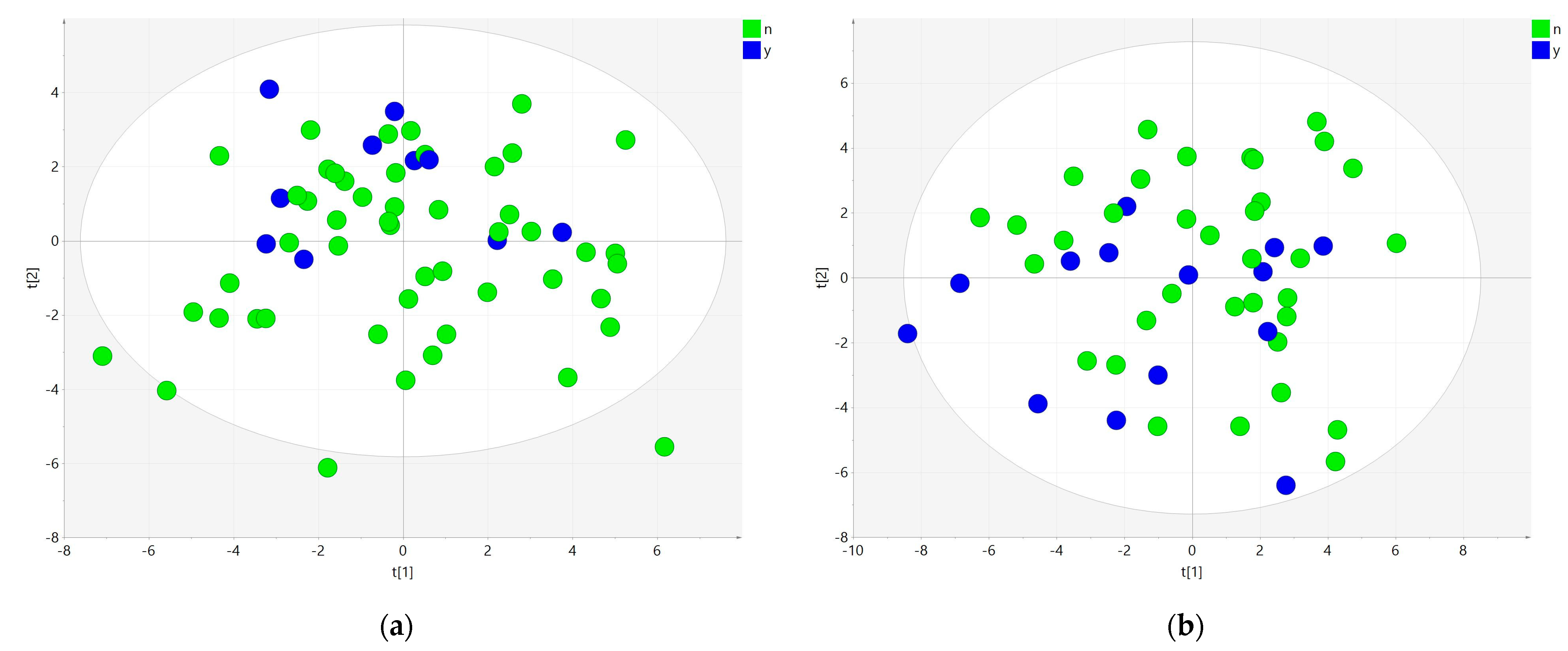
2.4. The Effect of Prior Statin Use
2.5. Effect of Sex
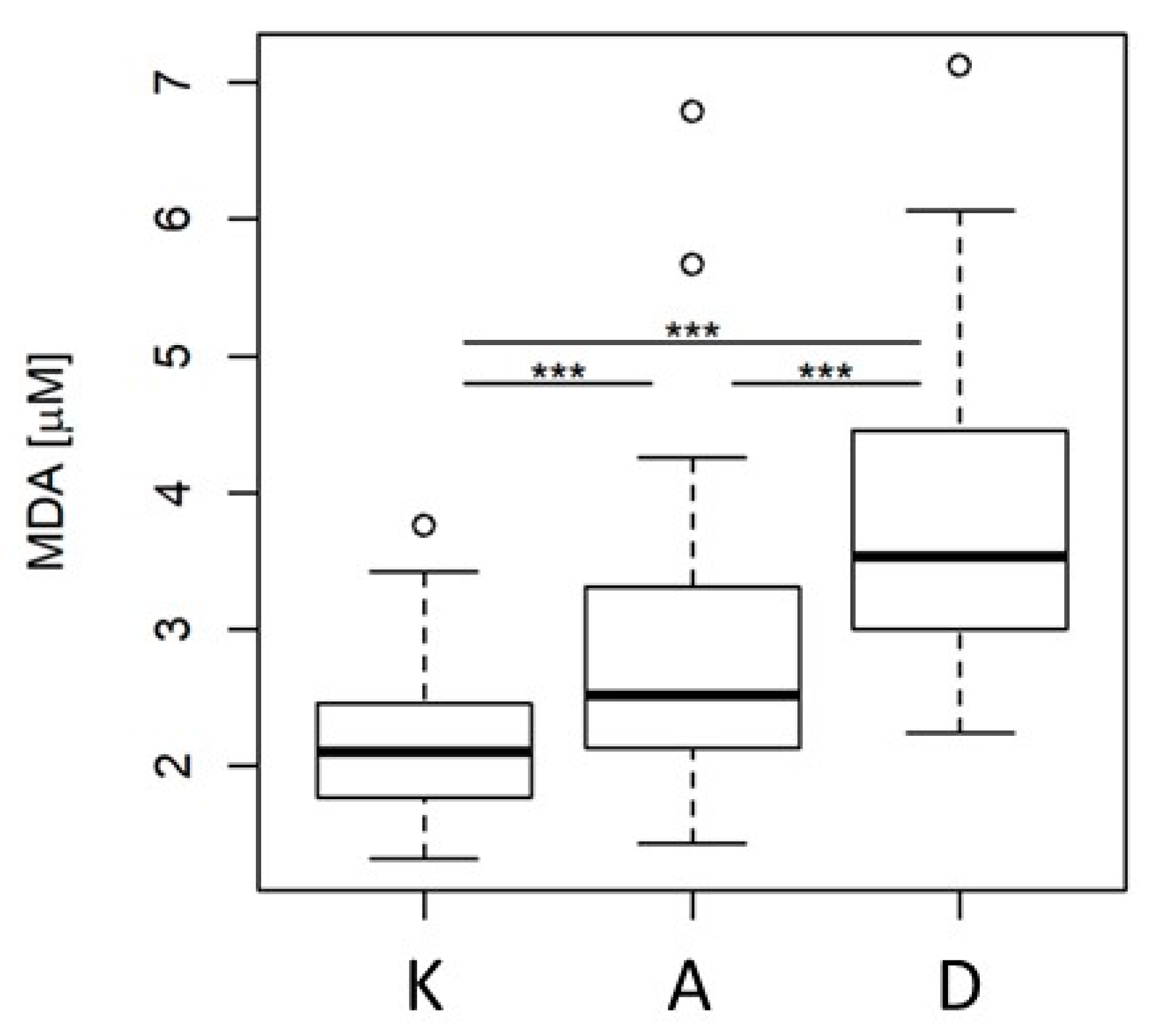
2.6. Malondialdehyde Concentration Analysis
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Chemicals and Materials
4.3. Sample Collection
4.4. Lipidomic Sample Preparation
4.5. Instrumental Conditions
4.6. Processing of Data Generated by Fingerprinting Experiments
4.7. Malondialdehyde Analysis
4.8. Limitations of the Study
5. Conclusions
- LC-HRMS/MS lipidomics enabled the detection and identification of approx. 500 lipid species in the studied plasma samples.
- Statistical evaluation of generated data must be carried out carefully, especially with regard to the type of administered heparin, because the extent of neutral lipid hydrolysis largely differs between LMWH and UFH. Lipids such as TG and CE substrates of LPL—together with products of their hydrolysis—had to be eliminated from the dataset to avoid biased results.
- Chemometric assessment of the reduced lipidomic dataset showed that LPIs are significantly different for ACS, diagnosing platelet activation. Higher levels of FAHFAs in controls might be connected to higher anti-inflammatory activity.
- The protective role of FAHFAs as potential biomarkers should be investigated based on larger patient sets.
- Multivariate analysis of lipidomic data is a promising new strategy for discovering the role of lipids in the development and progress of pathologies.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quehenberger, O.; Dennis, E.A. The human plasma lipidome. N. Engl. J. Med. 2011, 365, 1812–1823. [Google Scholar] [CrossRef]
- Kostner, G.M. Apolipoproteins and lipoproteins of human plasma: Significance in health and in disease. Adv. Lipid Res. 1983, 20, 1–43. [Google Scholar]
- Bucher, H.C.; Griffith, L.E.; Guyatt, G.H. Systematic review on the risk and benefit of different cholesterol-lowering interventions. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Thompson, G.R.; Packard, C.J.; Stone, N.J. Goals of statin therapy: Three viewpoints. Atheroscler. Supp. 2004, 5, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Tyroler, H.A. Review of lipid-lowering clinical trials in relation to observational epidemiologic studies. Circulation 1987, 76, 515–522. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Rexrode, K.M. A review of lipidomics of cardiovascular disease highlights the importance of isolating lipoproteins. Metabolites 2020, 10, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahy, E.; Subramaniam, S.; Brown, H.A.; Glass, C.K.; Merrill, A.H.; Murphy, R.C.; Raetz, C.R.H.; Russell, D.W.; Seyama, Y.; Shaw, W.; et al. A comprehensive classification system for lipids. J. Lipid Res. 2005, 46, 839–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, S.E.; Farag, M.A.; Holvoet, P.; Hanafi, R.S.; Gad, M.Z. a comparative metabolomics approach reveals early biomarkers for metabolic response to acute myocardial infarction. Sci. Rep. 2016, 6, 36359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Li, Z.; Chen, J.; Zhao, H.; Luo, L.; Chen, C.; Xu, X.; Zhang, W.; Gao, K.; Li, B.; et al. Metabolomic identification of diagnostic plasma biomarkers in humans with chronic heart Failure. Mol. BioSyst. 2013, 9, 2618–2626. [Google Scholar] [CrossRef]
- Laborde, C.M.; Mourino-Alvarez, L.; Posada-Ayala, M.; Alvarez-Llamas, G.; Serranillos-Reus, M.G.; Moreu, J.; Vivanco, F.; Padial, L.R.; Barderas, M.G. Plasma metabolomics reveals a potential panel of biomarkers for early diagnosis in acute coronary syndrome. Metabolomics 2014, 10, 414–424. [Google Scholar] [CrossRef] [Green Version]
- Teul, J.; Garcia, A.; Tuñón, J.; Martin-Ventura, J.L.; Tarín, N.; Bescós, L.L.; Egido, J.; Barbas, C.; Rupérez, F.J. Targeted and non-targeted metabolic time trajectory in plasma of patients after acute coronary syndrome. J. Pharmaceut. Biomed. 2011, 56, 343–351. [Google Scholar] [CrossRef]
- Vallejo, M.; García, A.; Tuñón, J.; García-Martínez, D.; Angulo, S.; Martin-Ventura, J.L.; Blanco-Colio, L.M.; Almeida, P.; Egido, J.; Barbas, C. Plasma fingerprinting with gc-ms in acute coronary syndrome. Anal. Bioanal. Chem. 2009, 394, 1517–1524. [Google Scholar] [CrossRef] [Green Version]
- Lam, S.M.; Wang, Y.; Li, B.; Du, J.; Shui, G. Metabolomics through the lens of precision cardiovascular medicine. J. Genet. Genom. 2017, 44, 127–138. [Google Scholar] [CrossRef]
- Yin, X.; de Carvalho, L.P.; Chan, M.Y.; Li, S.F.Y. Integrated metabolomics and metallomics analyses in acute coronary syndrome patients. Metallomics 2017, 9, 734–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taqueti, V.R. Sex Differences in the Coronary System. Adv. Exp. Med. Biol. 2018, 1065, 257–278. [Google Scholar] [PubMed]
- Hajsl, M.; Hlavackova, A.; Broulikova, K.; Sramek, M.; Maly, M.; Dyr, J.E.; Suttnar, J. tryptophan metabolism, inflammation, and oxidative stress in patients with neurovascular disease. Metabolites 2020, 10, 208. [Google Scholar] [CrossRef]
- Nasstrom, B.; Stegmayr, B.G.; Olivecrona, G.; Olivecrona, T. Lower plasma levels of lipoprotein lipase after infusion of low molecular weight heparin than after administration of conventional heparin indicate more rapid catabolism of the enzyme. J. Lab. Clin. Med. 2003, 142, 90–99. [Google Scholar] [CrossRef]
- Lee, J.; Moraes-Vieira, P.M.; Castoldi, A.; Aryal, P.; Yee, E.U.; Vickers, C.; Parnas, O.; Donaldson, C.J.; Saghatelian, A.; Kahn, B.B. Branched fatty acid esters of hydroxy fatty acids (FAHFAs) protect against colitis by regulating gut innate and adaptive immune responses. J. Biol. Chem. 2016, 291, 22207–22217. [Google Scholar] [CrossRef] [Green Version]
- Yore, M.M.; Syed, I.; Moraes-Vieira, P.M.; Zhang, T.; Herman, M.A.; Homan, E.A.; Patel, R.T.; Lee, J.; Chen, S.; Peroni, O.D.; et al. Discovery of a class of endogenous mammalian lipids with anti-diabetic and anti-inflammatory effects. Cell 2014, 159, 318–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, D.B.; Neufeld, E.J.; Majerus, P.W. Phosphoinositide interconversion in thrombin-stimulated human platelets. J. Biol. Chem. 1985, 260, 1046–1051. [Google Scholar] [CrossRef]
- Jackson, R.L.; Demel, R.A. Lipoprotein lipase-catalyzed hydrolysis of phospholipid monolayers: Effect of fatty acyl composition on enzyme activity. Biochem. Biophys. Res. Commun. 1985, 128, 670–675. [Google Scholar] [CrossRef]
- McCoy, M.G.; Sun, G.-S.; Marchadier, D.; Maugeais, C.; Glick, J.M.; Rader, D.J. Characterization of the lipolytic activity of endothelial lipase. J. Lipid Res. 2002, 43, 921–929. [Google Scholar] [CrossRef]
- Lee, J.H.; Yang, J.S.; Lee, S.-H.; Moon, M.H. Analysis of lipoprotein-specific lipids in patients with acute coronary syndrome by asymmetrical flow field-flow fractionation and nanoflow liquid chromatography-tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2018, 1099, 56–63. [Google Scholar] [CrossRef]
- Meikle, P.J.; Formosa, M.F.; Mellett, N.A.; Jayawardana, K.S.; Giles, C.; Bertovic, D.A.; Jennings, G.L.; Childs, W.; Reddy, M.; Carey, A.L.; et al. HDL phospholipids, but not cholesterol distinguish acute coronary syndrome from stable coronary artery disease. J. Am. Heart Assoc. 2019, 8, e011792. [Google Scholar] [CrossRef] [PubMed]
- Koelmel, J.P.; Kroeger, N.M.; Ulmer, C.Z.; Bowden, J.A.; Patterson, R.E.; Cochran, J.A.; Beecher, C.W.W.; Garrett, T.J.; Yost, R.A. LipidMatch: An automated workflow for rule-based lipid identification using untargeted high-resolution tandem mass spectrometry data. BMC Bioinform. 2017, 18, 331. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lipid Name | Adduct | Retention Time | m/z | Fold Change | |
|---|---|---|---|---|---|
| A-K | D-K | ||||
| FA (20:2) | [M − H]− | 5.408 | 307.2636 | 0.70 | 0.39 |
| FA (20:3) | [M − H]− | 4.316 | 305.2479 | 0.64 | 0.31 |
| FA (20:3) | [M − H]− | 4.669 | 305.2479 | 0.73 | 0.32 |
| FA (20:4). | [M − H]− | 3.632 | 303.2324 | 0.76 | 0.48 |
| FA (20:5) | [M − H]− | 2.861 | 301.2166 | 0.68 | 0.39 |
| FA (22:4) | [M − H]− | 4.741 | 331.2665 | 0.74 | 0.46 |
| FA (22:5) | [M − H]− | 3.794 | 329.2481 | 0.51 | 0.31 |
| FA (22:5) | [M − H]− | 4.118 | 329.2481 | 0.58 | 0.31 |
| FA (22:6) | [M − H]− | 3.235 | 327.2325 | 0.58 | 0.38 |
| FAHFA (14:0/16:2) | [M − H]− | 3.439 | 477.3908 | 0.27 | 0.08 |
| FAHFA (16:1/18:3) | [M − H]− | 3.614 | 529.4225 | 0.34 | 0.14 |
| FAHFA (18:1/20:3) | [M − H]− | 5.205 | 585.4851 | 0.52 | 0.21 |
| FAHFA (18:2/20:4) | [M − H]− | 3.932 | 581.4535 | 0.79 | 0.41 |
| FAHFA (20:4/18:3) | [M − H]− | 3.626 | 579.4376 | 0.53 | 0.23 |
| LPC (20:5) | [M + H]+ | 2.239 | 542.3265 | 1.23 | 0.63 |
| LPC (22:5) | [M + H]+ | 2.435 | 570.3590 | 1.97 | 0.48 |
| LPC (22:6) | [M + H]+ | 2.020 | 568.3428 | 0.85 | 0.42 |
| LPC (22:6) | [M + H]+ | 2.450 | 568.3420 | 1.24 | 0.56 |
| LPE (18:2) | [M − H]− | 2.315 | 476.2774 | 1.39 | 0.67 |
| LPE (20:4) | [M − H]− | 2.218 | 500.2774 | 1.13 | 0.46 |
| LPE (22:6) | [M − H]− | 2.092 | 524.2771 | 0.97 | 0.48 |
| LPI (18:1) | [M − H]− | 2.224 | 597.3032 | 2.09 | 1.13 |
| LPI (18:2) | [M − H]− | 1.823 | 595.2878 | 2.09 | 1.18 |
| TG (14.0_16.1_20.3) | [M + NH4]+ | 12.94 | 844.7394 | 0.79 | 1.78 |
| TG (16:0_16:1_18:0) | [M + Na]+ | 13.33 | 855.7420 | 0.80 | 3.46 |
| TG (16:0_18:2_18:3) | [M + NH4]+ | 13.00 | 870.7544 | 0.70 | 1.77 |
| TG (16:0_18:2_22:6) | [M + NH4]+ | 12.99 | 920.7687 | 0.71 | 1.49 |
| TG (17:1_17:2_19:0) | [M + NH4]+ | 13.85 | 888.8015 | 0.73 | 1.60 |
| FA (16:1) | [M − H]− | 3.617 | 253.2168 | 0.55 | 0.34 |
| FA (17:1) | [M − H]− | 4.325 | 267.2325 | 0.61 | 0.35 |
| Lipid Name | Adduct | Retention Time | m/z | PLS-DA VIP | FC A over K | FC D over K | MDA Correlation |
|---|---|---|---|---|---|---|---|
| FAHFA (14:0/16:2) | [M − H]− | 3.439 | 477.3908 | 2.10 | 0.27 | 0.08 | −0.437 *** |
| LPI (20:4) | [M − H]− | 1.760 | 619.2877 | 1.95 | 1.76 | 1.06 | 0.071 |
| FAHFA (16:1/18:3) | [M − H]− | 3.614 | 529.4225 | 1.94 | 0.34 | 0.14 | −0.411 *** |
| LPI (18:2) | [M − H]− | 1.823 | 595.2878 | 1.88 | 2.09 | 1.18 | 0.085 |
| LPI (18:1) | [M − H]− | 2.224 | 597.3032 | 1.81 | 2.09 | 1.13 | 0.029 |
| FAHFA (20:4/18:3) | [M − H]− | 3.626 | 579.4376 | 1.72 | 0.53 | 0.23 | −0.433 *** |
| FAHFA (18:1/20:3) | [M − H]− | 5.205 | 585.4851 | 1.65 | 0.52 | 0.21 | −0.359 *** |
| FAHFA (18:2/20:4) | [M − H]− | 3.932 | 581.4535 | 1.39 | 0.79 | 0.41 | −0.465 *** |
| PE (18:1_18:2) | [M − H]− | 9.196 | 740.5227 | 1.27 | 1.81 | 1.54 | 0.157 * |
| LPE (20:4) | [M − H]− | 2.218 | 500.2774 | 1.24 | 1.13 | 0.46 | −0.328 *** |
| PE (16:0_18:2) | [M − H]− | 9.175 | 714.5069 | 1.24 | 1.90 | 1.58 | 0.192 ** |
| LPE (22:6) | [M − H]− | 2.092 | 524.2771 | 1.24 | 0.97 | 0.48 | −0.340 *** |
| LPE (18:2) | [M − H]− | 2.315 | 476.2774 | 1.19 | 1.39 | 0.67 | −0.433 *** |
| LPC (20:3) | [M + H]+ | 3.948 | 546.3583 | 1.17 | 0.76 | 0.66 | −0.336 *** |
| PE (16:0_18:1) | [M − H]− | 9.924 | 716.5227 | 1.16 | 1.72 | 1.66 | 0.312 *** |
| FAHFA (18:0/20:2) | [M − H]− | 6.278 | 589.5155 | 1.16 | 1.09 | 0.75 | −0.215 ** |
| LPC (22:6) | [M + H]+ | 2.450 | 568.3420 | 1.16 | 1.24 | 0.56 | −0.348 *** |
| PC (36:4) | [M + Na]+ | 7.623 | 804.5551 | 1.14 | 0.80 | 0.98 | −0.114 |
| PE (18:0_18:2) | [M − H]− | 10.08 | 742.5384 | 1.14 | 1.57 | 1.57 | 0.192 ** |
| LPC (22:5) | [M + H]+ | 2.435 | 570.3590 | 1.13 | 1.00 | 0.51 | −0.384 *** |
| LPC (20:5) | [M + H]+ | 2.239 | 542.3265 | 1.13 | 1.23 | 0.63 | −0.330 *** |
| DMPE (16:0_18:1) | [M − H]− | 10.82 | 744.5537 | 1.12 | 1.64 | 1.55 | 0.256 *** |
| PE (18:1_18:1) | [M − H]− | 9.941 | 742.5381 | 1.10 | 1.67 | 1.44 | 0.222 ** |
| LPC (22:6) | [M + H]+ | 2.020 | 568.3428 | 1.07 | 0.85 | 0.42 | −0.382 *** |
| PC (15:1_20:5) | [M + H]+ | 8.538 | 764.5249 | 1.07 | 1.27 | 1.64 | 0.239 *** |
| PE (34:1) | [M + H]+ | 9.591 | 718.5409 | 1.05 | 1.63 | 1.89 | 0.362 *** |
| LPC (18:3) | [M + H]+ | 1.915 | 518.3277 | 1.02 | 1.30 | 0.77 | −0.230 ** |
| Lipid Name | Adduct | Retention Time | m/z | PLS-DA VIP | FC A-K | FC D-K |
|---|---|---|---|---|---|---|
| FAHFA (14:0/16:2) | [M − H]− | 3.439 | 477.3908 | 1.89 | 0.18 | 0.11 |
| FAHFA (16:1/18:3) | [M − H]− | 3.614 | 529.4225 | 1.63 | 0.29 | 0.22 |
| LPI (18:2) | [M − H]− | 1.823 | 595.2878 | 1.55 | 2.50 | 1.80 |
| FAHFA (20:4/18:3) | [M − H]− | 3.626 | 579.4376 | 1.45 | 0.46 | 0.33 |
| LPI (20:4) | [M − H]− | 1.760 | 619.2877 | 1.43 | 1.98 | 1.47 |
| FAHFA (18:1/20:3) | [M − H]− | 5.205 | 585.4851 | 1.39 | 0.45 | 0.27 |
| Plasmanyl PC (O-16:1/18:1) | [M + CH3COO]− | 10.14 | 802.5922 | 1.33 | 0.85 | 1.64 |
| Plasmenyl PC (P-16:1/20:3) | [M + H]+ | 9.725 | 766.5730 | 1.32 | 0.86 | 1.76 |
| Plasmanyl PC (O-16:0/18:2) | [M + H]+ | 9.729 | 744.5866 | 1.31 | 0.89 | 1.71 |
| PC (36:4) | [M + Na]+ | 7.623 | 804.5551 | 1.29 | 0.65 | 1.21 |
| LPI (18:1) | [M − H]− | 2.224 | 597.3032 | 1.20 | 1.87 | 1.78 |
| LPC (20:3) | [M + H]+ | 3.948 | 546.3583 | 1.14 | 0.64 | 0.92 |
| Plasmenyl PS (P-20:0/18:0) | [M − H]− | 3.922 | 802.5951 | 1.10 | 0.62 | 0.51 |
| LPC (20:1) | [M + H] | 4.024 | 550.3911 | 1.08 | 0.80 | 1.28 |
| FAHFA (18:2/20:4) | [M − H]− | 3.932 | 581.4535 | 1.07 | 0.79 | 0.57 |
| PE (34:1) | [M + H]+ | 9.591 | 718.5409 | 1.05 | 2.02 | 2.44 |
| Lipid Name | Adduct | Retention Time | m/z | PLS-DA VIP | FC A-K | FC D-K |
|---|---|---|---|---|---|---|
| FAHFA (14:0/16:2) | [M − H]− | 3.439 | 477.3908 | 2.81 | 0.34 | 0.05 |
| FAHFA (16:1/18:3) | [M − H]− | 3.614 | 529.4225 | 2.58 | 0.36 | 0.13 |
| FAHFA (20:4/18:3) | [M − H]− | 3.626 | 579.4376 | 2.28 | 0.47 | 0.20 |
| LPC (20:3) | [M + H]+ | 3.948 | 546.3583 | 2.25 | 0.75 | 0.78 |
| FAHFA (18:1/20:3) | [M − H]− | 5.205 | 585.4851 | 2.02 | 0.50 | 0.19 |
| LPE (18:2) | [M − H]− | 2.315 | 476.2774 | 1.87 | 1.17 | 0.83 |
| LPC (20:3) | [M + H]+ | 3.630 | 546.3580 | 1.78 | 0.80 | 0.91 |
| LPC (20:5) | [M + H]+ | 2.239 | 542.3265 | 1.75 | 1.15 | 0.65 |
| LPC (18:3) | [M + H]+ | 1.915 | 518.3277 | 1.74 | 1.41 | 0.70 |
| FAHFA (18:2/20:4) | [M − H]− | 3.932 | 581.4535 | 1.73 | 0.70 | 0.51 |
| LPC (20:1) | [M + H] | 4.024 | 550.3911 | 1.64 | 0.80 | 0.91 |
| LPE (20:4) | [M − H]− | 2.218 | 500.2774 | 1.59 | 0.94 | 0.60 |
| FAHFA (18:0/20:2) | [M − H]− | 6.278 | 589.5155 | 1.56 | 0.90 | 1.01 |
| LPC (18:2) | [M + H]+ | 2.240 | 520.3443 | 1.49 | 1.09 | 0.69 |
| LPC (22:6) | [M + H]+ | 2.450 | 568.3420 | 1.38 | 1.04 | 0.62 |
| LPC (22:5) | [M + H]+ | 2.435 | 570.3590 | 1.36 | 0.94 | 0.55 |
| FAHFA (18:1/18:2) | [M − H]− | 4.983 | 559.4692 | 1.36 | 0.86 | 0.94 |
| FAHFA (18:1/20:3) | [M − H]− | 5.205 | 585.4851 | 1.31 | 0.83 | 0.94 |
| LPC (22:6) | [M + H]+ | 2.020 | 568.3428 | 1.30 | 0.75 | 0.49 |
| LPC (22:5) | [M + H]+ | 2.214 | 570.3590 | 1.30 | 0.87 | 0.57 |
| FAHFA (16:0/18:2) | [M − H]− | 4.893 | 533.4541 | 1.30 | 0.82 | 0.90 |
| LPE (22:6) | [M − H]− | 2.092 | 524.2771 | 1.29 | 0.95 | 0.61 |
| LPE (18:1) | [M − H]− | 2.967 | 478.2928 | 1.25 | 1.22 | 1.00 |
| LPC (20:2) | [M + H]+ | 3.028 | 548.3753 | 1.06 | 1.02 | 0.76 |
| LPC (20:3) | [M + H]+ | 2.640 | 546.3598 | 1.06 | 1.02 | 0.71 |
| AIM (n = 61) Group A | AIS (n = 49) Group D | Control (n = 82) Group K | Kruskal–Wallis Test p-Value | |
|---|---|---|---|---|
| Age (y) | 64 | 71 | 64 | 0.001 |
| Sex (m/f) | 41/20 | 23/26 | 39/43 | − |
| Clinical characteristics | ||||
| Arterial hypertension | 35 (57%) | 38 (78%) | 53 (65%) | − |
| Diabetes mellitus | 13 (21%) | 13 (27%) | 11 (13%) | − |
| Current smoker | 36 (59%) | 10 (20%) | 19 (23%) | − |
| BMI | 28.5 | 28.6 | 28.1 | 0.874 |
| Medical history | ||||
| History of MI | 8 (13%) | 5 (10%) | 0 | − |
| History of PCI | 6 (10%) | 2 (4%) | 0 | − |
| History of CABG | 1 (2%) | 3 (6%) | 0 | − |
| History of stroke | 1 (2%) | 0 | 0 | − |
| Laboratory results | ||||
| Creatine (µmol/L) | 78 | 74 | 73 | 0.647 |
| Total cholesterol (mmol/L) | 4.63 | 4.4 | 4.47 | 0.405 |
| TAG (mmol/L) | 1.18 | 1.39 | 1.27 | 0.014 a |
| LDL cholesterol (mmol/L) | 2.88 | 2.59 | 2.52 | 0.008 b |
| HDL cholesterol (mmol/L) | 1.13 | 1.18 | 1.37 | <0.0012 b |
| Pre-procedure hypolidimic treatment | ||||
| Statin | 10 (16%) | 14 (29%) | 31 (38%) | – |
| Fibrate | 1 (2%) | 0 | 1 (1%) | – |
| Ezetimibe | 0 | 0 | 1 (1%) | – |
| Statin + ezetimibe | 0 | 0 | 1 (1%) | – |
| Fibrate + ezetimibe | 0 | 0 | 1 (1%) | – |
| Post-procedure hypolidimic treatment | ||||
| Statin | 60 (98%) | 43 (88%) | NA | – |
| No treatment—patient died | 1 (2%) | 6 (12%) | NA | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malý, M.; Hajšl, M.; Bechyňská, K.; Kučerka, O.; Šrámek, M.; Suttnar, J.; Hlaváčková, A.; Hajšlová, J.; Kosek, V. Lipidomic Analysis to Assess Oxidative Stress in Acute Coronary Syndrome and Acute Stroke Patients. Metabolites 2021, 11, 412. https://doi.org/10.3390/metabo11070412
Malý M, Hajšl M, Bechyňská K, Kučerka O, Šrámek M, Suttnar J, Hlaváčková A, Hajšlová J, Kosek V. Lipidomic Analysis to Assess Oxidative Stress in Acute Coronary Syndrome and Acute Stroke Patients. Metabolites. 2021; 11(7):412. https://doi.org/10.3390/metabo11070412
Chicago/Turabian StyleMalý, Martin, Martin Hajšl, Kamila Bechyňská, Ondřej Kučerka, Martin Šrámek, Jiří Suttnar, Alžběta Hlaváčková, Jana Hajšlová, and Vít Kosek. 2021. "Lipidomic Analysis to Assess Oxidative Stress in Acute Coronary Syndrome and Acute Stroke Patients" Metabolites 11, no. 7: 412. https://doi.org/10.3390/metabo11070412