
Comprehensive Literature Review of Hyperpolarized Carbon-13 MRI: The Road to Clinical Application


Abstract
:1. Introduction
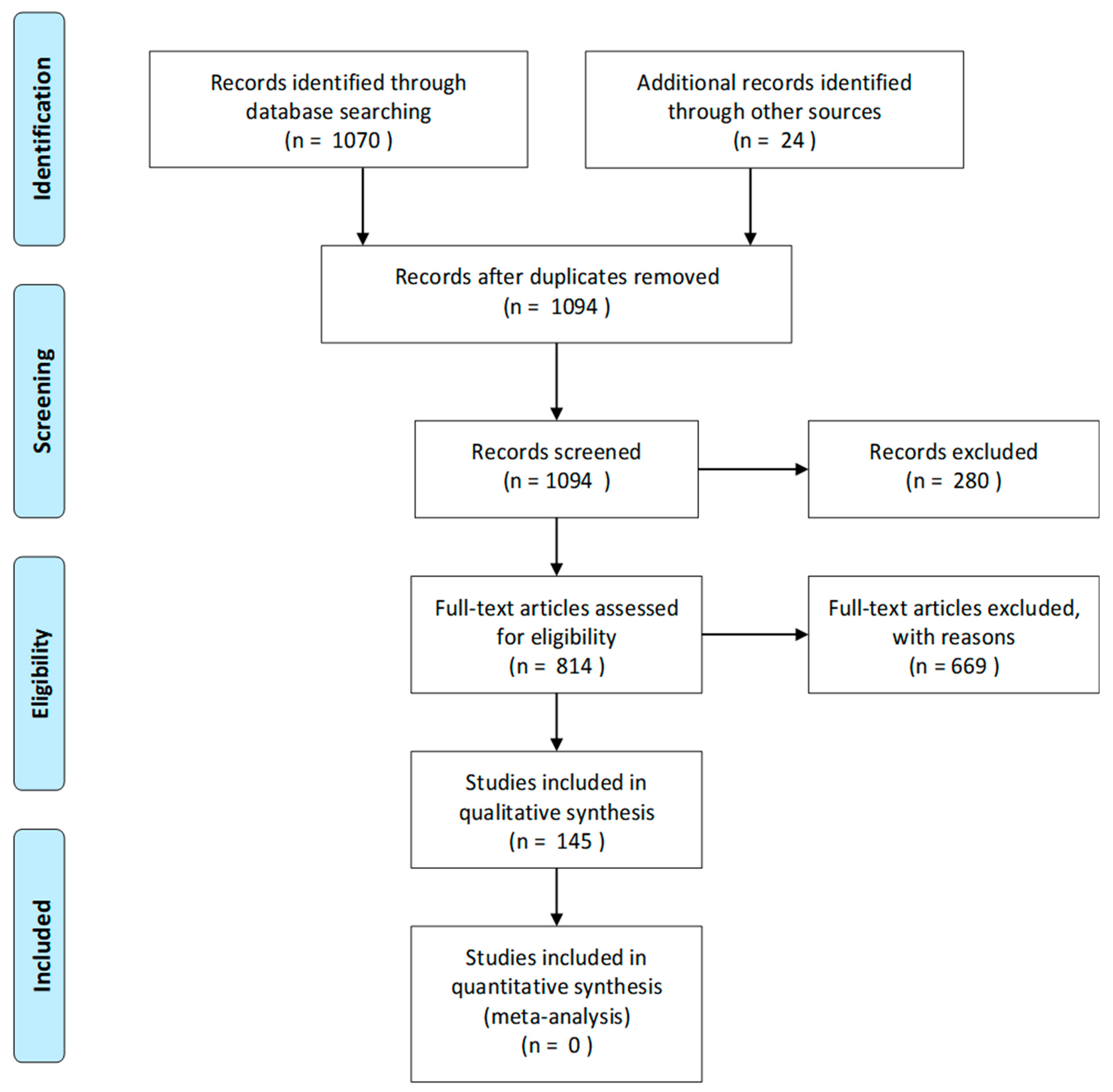
2. Literature Search and Review Strategy
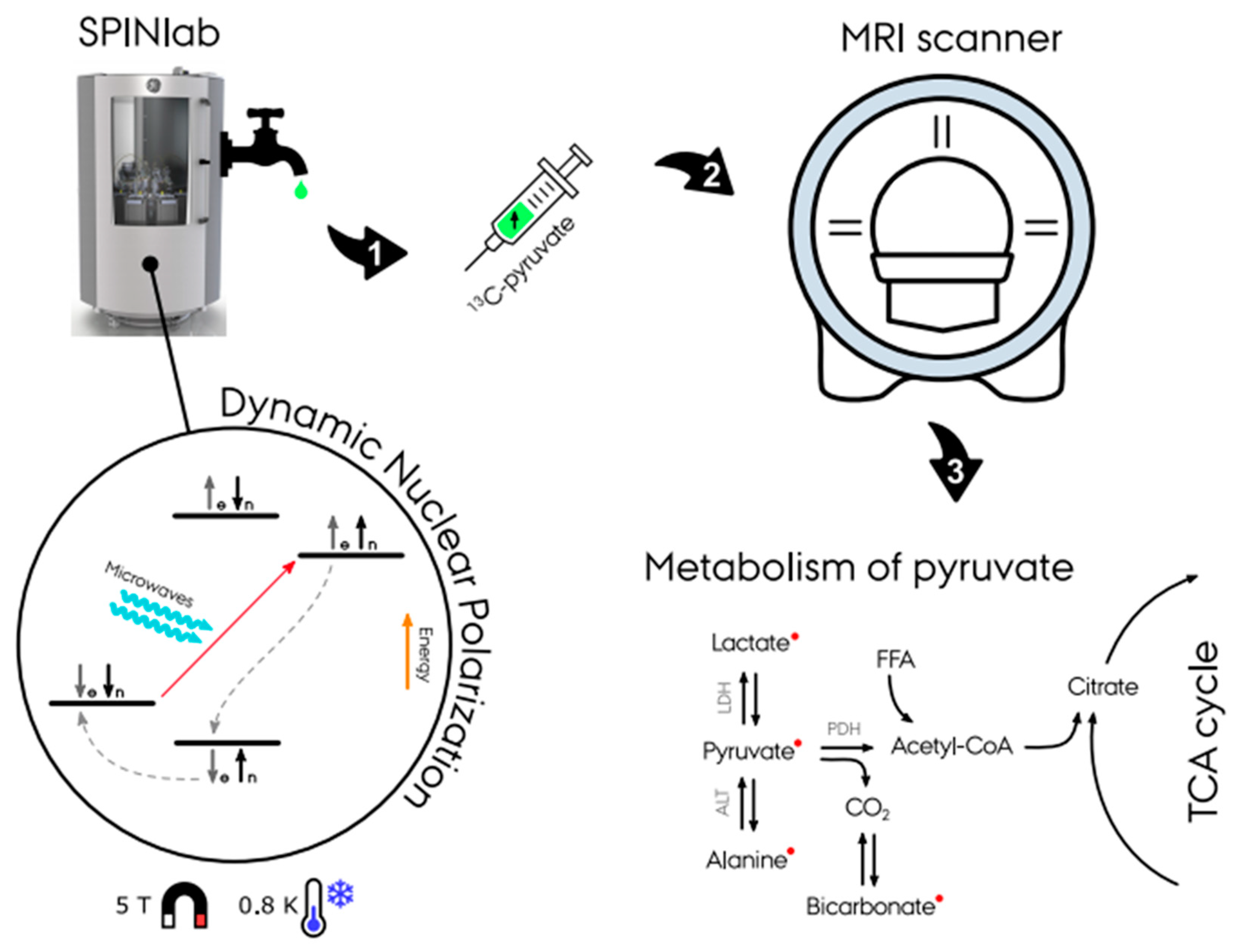
3. Hyperpolarized Carbon-13 MRI
4. Applications of Hyperpolarized Carbon-13 MRI
4.1. Hyperpolarized [1-13C]pyruvate: The Most Used Biomarker
4.2. Oncology
4.3. Brain
4.4. Cardiovascular Disease
4.5. Kidney Disease
4.6. Liver Disease
4.7. Technical Advances
4.7.1. Polarizer
4.7.2. Sequences
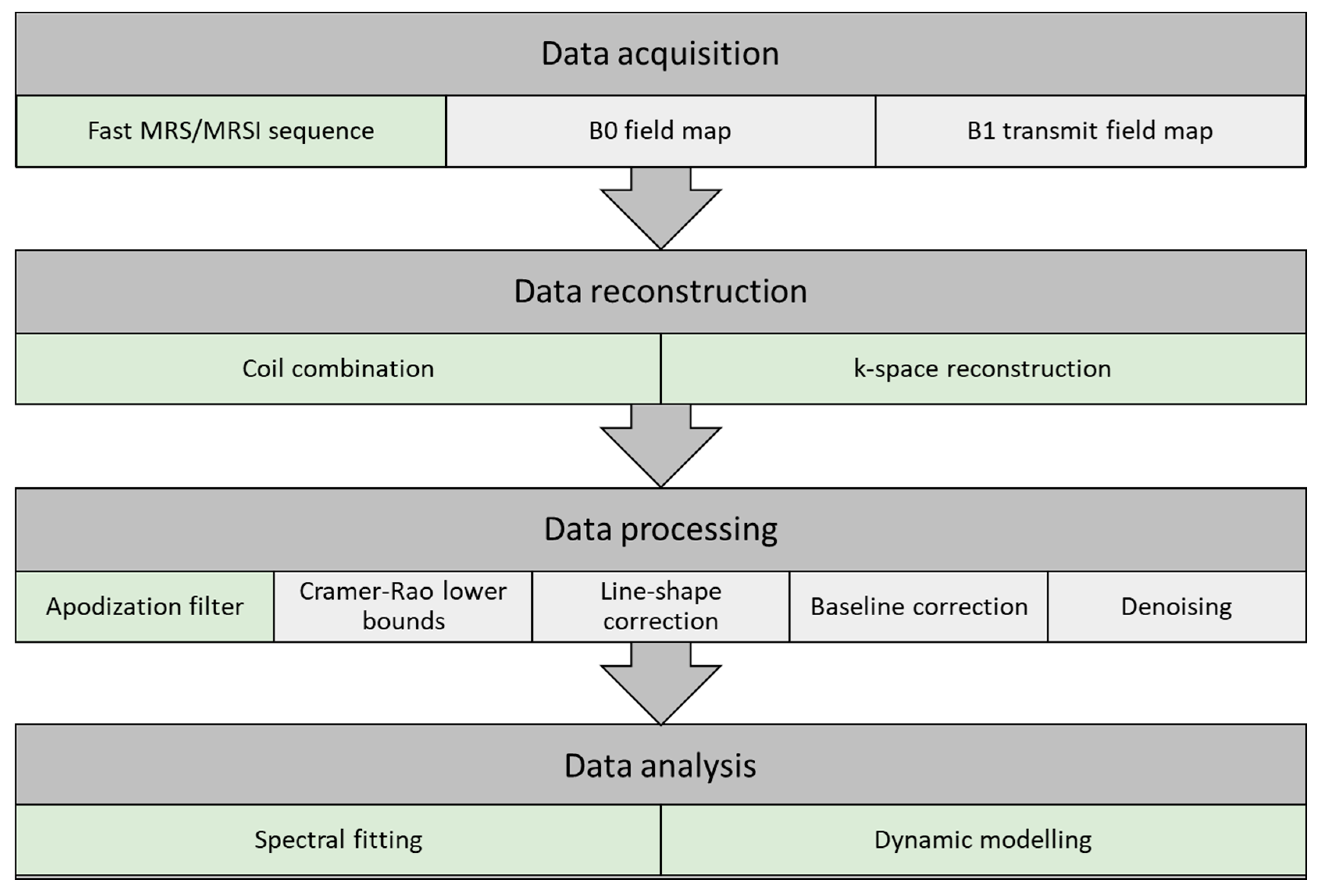
4.7.3. Data Acquisition, Reconstruction, Processing, and Analysis
Data Acquisition
Data Reconstruction
Data Processing
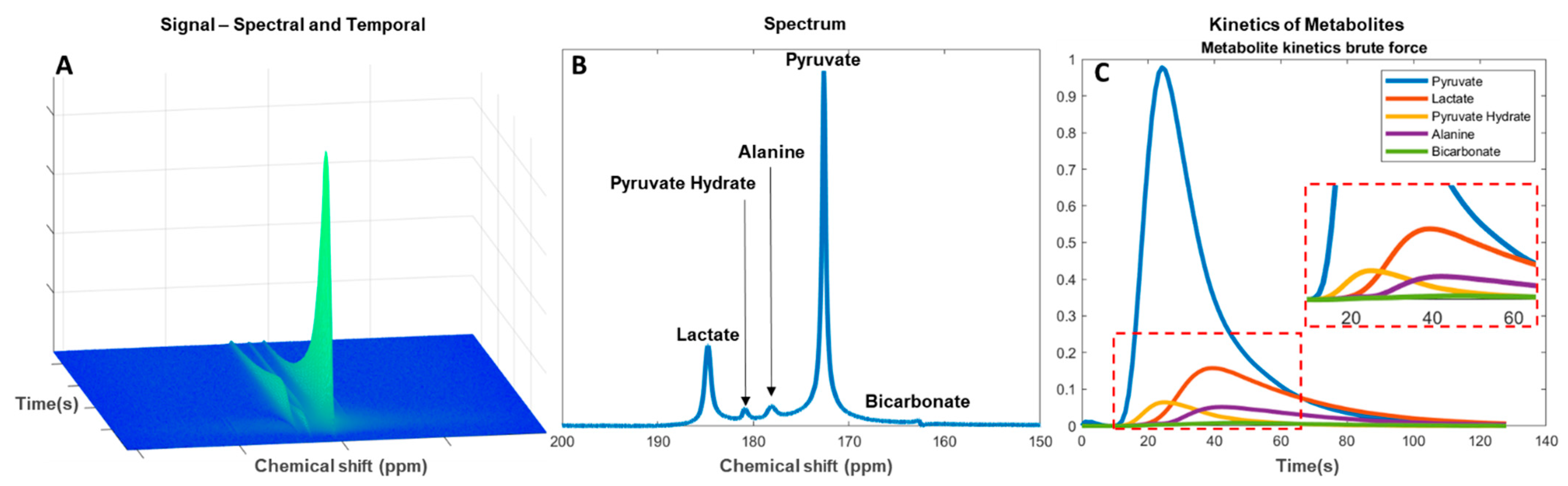
Data Analysis
4.8. Other
4.9. Clinical Transition
4.10. Challenges and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
Appendix A.1. Electronic Search Strategy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Search Item | No. of Results | Excluded (Why) | Included |
|---|---|---|---|---|
| 1 | Ardenkjaer-Larsen JH (Author) | 123 (8 review) | 9 (age < 2003) 1 (not English) 3 (not hyperpolarized) 1 (corrigendum) 1 (not carbon) | 108 |
| 2 | hyperpolarized AND MR AND carbon review | 26 | 3 (not carbon, not hyperpolarized) 2 (duplicates from 1) | 21 |
| 3 | hyperpolarized AND MR AND carbon NOT review | 178 | 19 (not carbon) 2 (not hyperpolarized) 1 (hyperpolarized diamonds) 11 (duplicates from 1) | 145 |
| 4 | hyperpolarized AND 13C | 743 (48 review) | 174 (duplicates from 1,2,3) 1 (duplicate in PubMed) 30 (not carbon) 9 (diamonds) 2 (not English) 11 (not hyperpolarized) | 516 |
| 5 | forward and backward citations from papers | 24 | 24 | |
| Total | 1094 | 280 | 814 |
Appendix A.2. Studies Reported to clinicaltrials.gov as “Active, Not Recruiting” or “Recruiting” on Hyperpolarized Carbon-13 MRI
| Title | Condition | Trial Number | |
|---|---|---|---|
| 1 | Pilot Study of Safety and Toxicity of Acquiring Hyperpolarized Carbon-13 Imaging in Children With Brain Tumors | Pediatric brain tumors | NCT02947373 |
| 2 | Hyperpolarized Carbon-13 Imaging of Metastatic Prostate Cancer | Prostate cancer | NCT02844647 |
| 3 | Imaging of Traumatic Brain Injury Metabolism Using Hyperpolarized Carbon-13 Pyruvate | Traumatic brain injury | NCT03502967 |
| 4 | Metabolic Characteristics of Brain Tumors Using Hyperpolarized Carbon-13 Magnetic Resonance Spectroscopic Imaging (MRSI) | Brain tumor adult | NCT03067467 |
| 5 | Hyperpolarized Carbon 13-Based Metabolic Imaging to Detect Radiation-Induced Cardiotoxicity | Thoracic cancer/left sided breast cancer | NCT04044872 |
| 6 | Hyperpolarized Carbon-13 (13C) Pyruvate Imaging in Patients With Glioblastoma | Glioblastoma multiforme (GBM) | NCT04019002 |
| 7 | Hyperpolarized 13C Pyruvate MRI for Treatment Response Assessment in Patients With Locally Advanced or Metastatic Pancreatic Cancer | Pancreatic ductal adenocarcinoma | NCT04565327 |
| 8 | Feasibility of Acquiring Hyperpolarized Imaging in Patients With Primary CNS Lymphoma | Primary CNS lymphoma | NCT04656431 |
| 9 | Effect of Cardiotoxic Anticancer Chemotherapy on the Metabolism of [1-13C]Pyruvate in Cardiac Mitochondria | Breast neoplasms | NCT03685175 |
| 10 | Hyperpolarized Carbon C 13 Pyruvate Magnetic Resonance Spectroscopic Imaging in Predicting Treatment Response in Patients With Prostate Cancer | Prostate cancer | NCT03581500 |
| 11 | Hyperpolarized 13C Pyruvate MRI Scan in Predicting Tumor Aggressiveness in Patients With Localized Renal Tumor | Benign kidney cancer | NCT04258462 |
| 12 | Hyperpolarized Pyruvate (13C) MR Imaging in Monitoring Patients With Prostate Cancer on Active Surveillance | Prostate adenocarcinoma | NCT03933670 |
| 13 | Hyperpolarized Carbon C 13 Pyruvate in Diagnosing Glioma in Patients With Brain Tumors | Primary brain neoplasm | NCT03830151 |
| 14 | Serial MR Imaging and MR Spectroscopic Imaging for the Characterization of Lower Grade Glioma | Glioma | NCT04540107 |
| 15 | Hyperpolarized 13C MR Imaging of Lactate in Patients With Locally Advanced Cervical Cancer (LACC) Cervical Cancer | Uterine cervical neoplasms | NCT03129776 |
| 16 | Role of Hyperpolarized 13C-Pyruvate MR Spectroscopy in Patients With Intracranial Metastasis Treated With (SRS) | Brain metastases | NCT03324360 |
| 17 | Hyperpolarized Imaging in Diagnosing Participants With Glioma | Glioma | NCT03739411 |
| 18 | Metabolic Imaging of the Heart Using Hyperpolarized (13C) Pyruvate Injection | Hypertension/hypertrophy | NCT02648009 |
| 19 | Magnetic Resonance Imaging (MRI) With Hyperpolarized Pyruvate (13C) as Diagnostic Tool in Advanced Prostate Cancer | Prostate cancer | NCT04346225 |
| 20 | Imaging Oxidative Metabolism and Neurotransmitter Synthesis in the Human Brain | Brain cancer | NCT03849963 |
| 21 | Study to Evaluate the Feasibility of 13-C Pyruvate Imaging in Breast Cancer Patients Receiving Neoadjuvant Chemotherapy | Breast cancer | NCT03121989 |
| 22 | Development and Evaluation of a Quantitative HP MRI for Clinical Prostate Cancer Exam | Prostate adenocarcinoma | NCT04286386 |
| 23 | A Pilot Study of (MR) Imaging With Pyruvate (13C) to Detect High Grade Prostate Cancer | Prostate cancer | NCT02526368 |
| 24 | An Investigational Scan (hpMRI) for Monitoring Treatment Response in Patients With Thyroid Cancer Undergoing Radiation Therapy and/or Systemic Therapy | Thyroid gland carcinoma | NCT04589624 |
| 25 | Effect of Fatty Liver on TCA Cycle Flux and the Pentose Phosphate Pathway | Fatty liver | NCT03480594 |
| 26 | Hyperpolarized C-13 Pyruvate as a Biomarker in Patients With Advanced Solid Tumor Malignancies | Prostate cancer | NCT02913131 |
| 27 | Characterization of Hyperpolarized Pyruvate MRI Reproducibility | Malignant solid tumors | NCT02421380 |
Appendix A.3. Studies Reported to EudraCT for Clinical Trials of Hyperpolarized Carbon-13 MRI
| Title | Condition | EudraCT Number | |
|---|---|---|---|
| 1 | Early detection of effects of chemotherapy in pancreatic cancer patients—a study using MR-hyperpolarization scanning based on hyperpolarized Pyruvate (13C) injection | Pancreatic cancer | 2016-004491-22 |
| 2 | MRI of neurometabolic impairment in ALS and TIA using hyperpolarized pyruvate | Amyotrophic lateral sclerosis | 2020-000352-36 |
| 3 | Clinical and pathophysiological aspects of visualization of metabolic flux in the failing human heart using hyperpolarized [1-13C]-pyruvate cardiac magnetic resonance | Chronic heart failure | 2018-003533-15 |
| 4 | MRI with hyperpolarised pyruvate in glioblastoma—a phase II study | Glioblastoma multiforme | 2020-000310-15 |
| 5 | Metabolic imaging of patients with mycosis fungoides using hyperpolarized 13C-Pyruvate magnetic resonance imaging—A feasibility study | Mycosis fungoides | 2018-001656-35 |
| 6 | A Dose-Ranging Pharmacodynamic Study to Evaluate the Effects of IMB-1018972 on Myocardial Energetics, Metabolism, and Function in Patients with Type 2 Diabetes | Diabetic cardiomyopathy | 2020-003280-26 |
References
- Kurhanewicz, J.; Vigneron, D.B.; Ardenkjaer-Larsen, J.H.; Bankson, J.A.; Brindle, K.; Cunningham, C.H.; Gallagher, F.A.; Keshari, K.R.; Kjaer, A.; Laustsen, C.; et al. Hyperpolarized 13C MRI: Path to Clinical Translation in Oncology. Neoplasia 2019, 21, 1–16. [Google Scholar] [CrossRef]
- Qin, H.; Zhang, V.; Bok, R.A.; Santos, R.D.; Cunha, J.A.; Hsu, I.-C.; Santos, B.J.D.; Lee, J.E.; Sukumar, S.; Larson, P.E.; et al. Simultaneous Metabolic and Perfusion Imaging Using Hyperpolarized 13C MRI Can Evaluate Early and Dose-Dependent Response to Radiation Therapy in a Prostate Cancer Mouse Model. Int. J. Radiat. Oncol. 2020, 107, 887–896. [Google Scholar] [CrossRef]
- Ardenkjaer-Larsen, J.H.; Fridlund, B.; Gram, A.; Hansson, L.; Lerche, M.H.; Servin, R.; Thaning, M.; Golman, K. Increase in signal-to-noise ratio of >10,000 times in liquid-state NMR. Proc. Natl. Acad. Sci. USA 2003, 100, 10158–10163. [Google Scholar] [CrossRef] [Green Version]
- Ardenkjaer-Larsen, J.H. Hyperpolarized MR—What’s up Doc? J. Magn. Reson. 2019, 306, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, C.H.; Lau, J.Y.; Chen, A.P.; Geraghty, B.J.; Perks, W.J.; Roifman, I.; Wright, G.A.; Connelly, K.A. Hyperpolarized 13C Metabolic MRI of the Human Heart. Circ. Res. 2016, 119, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Grist, J.T.; Mariager, C.Ø.; Qi, H.; Nielsen, P.M.; Laustsen, C. Detection of acute kidney injury with hyperpolarized [13C, 15N] Urea and multiexponential relaxation modeling. Magn. Reson. Med. 2019, 84, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.J.; Kurhanewicz, J.; Vigneron, D.B.; Larson, P.E.Z.; Harzstark, A.L.; Ferrone, M.; Van Criekinge, M.; Chang, J.W.; Bok, R.; Park, I.; et al. Metabolic Imaging of Patients with Prostate Cancer Using Hyperpolarized [1-13C]Pyruvate. Sci. Transl. Med. 2013, 5, 198ra108. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Soliman, H.; Geraghty, B.J.; Chen, A.P.; Connelly, K.A.; Endre, R.; Perks, W.J.; Heyn, C.; Black, S.E.; Cunningham, C.H. Lactate topography of the human brain using hyperpolarized 13C-MRI. NeuroImage 2020, 78, 3755–3760. [Google Scholar] [CrossRef] [PubMed]
- Miloushev, V.Z.; Granlund, K.L.; Boltyanskiy, R.; Lyashchenko, S.K.; DeAngelis, L.M.; Mellinghoff, I.K.; Brennan, C.W.; Tabar, V.; Yang, T.J.; Holodny, A.I.; et al. Metabolic Imaging of the Human Brain with Hyperpolarized 13C Pyruvate Demonstrates 13C Lactate Production in Brain Tumor Patients. Cancer Res. 2018, 256, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Granlund, K.L.; Tee, S.-S.; Vargas, H.A.; Lyashchenko, S.K.; Reznik, E.; Fine, S.; Laudone, V.; Eastham, J.A.; Touijer, K.A.; Reuter, V.E.; et al. Hyperpolarized MRI of Human Prostate Cancer Reveals Increased Lactate with Tumor Grade Driven by Monocarboxylate Transporter 1. Cell Metab. 2020, 31, 105–114. [Google Scholar] [CrossRef]
- Ardenkjaer-Larsen, J.H. On the present and future of dissolution-DNP. J. Magn. Reson. 2016, 264, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.J.; Ohliger, M.A.; Larson, P.E.Z.; Gordon, J.W.; Bok, R.A.; Slater, J.; Villanueva-Meyer, J.E.; Hess, C.P.; Kurhanewicz, J.; Vigneron, D.B. Hyperpolarized 13C MRI: State of the Art and Future Directions. Radiology 2019, 291, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Grist, J.T.; McLean, M.A.; Riemer, F.; Schulte, R.F.; Deen, S.S.; Zaccagna, F.; Woitek, R.; Daniels, C.J.; Kaggie, J.D.; Matys, T.; et al. Quantifying normal human brain metabolism using hyperpolarized [1–13C]pyruvate and magnetic resonance imaging. NeuroImage 2019, 189, 171–179. [Google Scholar] [CrossRef]
- Keshari, K.R.; Wilson, D.M. Chemistry and biochemistry of 13C hyperpolarized magnetic resonance using dynamic nuclear polarization. Chem. Soc. Rev. 2014, 43, 1627–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grist, J.T.; Miller, J.J.; Zaccagna, F.; McLean, M.A.; Riemer, F.; Matys, T.; Tyler, D.J.; Laustsen, C.; Coles, A.J.; Gallagher, F.A. Hyperpolarized 13C MRI: A novel approach for probing cerebral metabolism in health and neurological disease. Br. J. Pharmacol. 2020, 40, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Warburg, O. On the Origin of Cancer Cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Zaccagna, F.; Grist, J.T.; Deen, S.S.; Woitek, R.; Lechermann, L.M.; McLean, M.A.; Basu, B.; Gallagher, F.A. Hyperpolarized carbon-13 magnetic resonance spectroscopic imaging: A clinical tool for studying tumour metabolism. Br. J. Radiol. 2018, 91, 20170688. [Google Scholar] [CrossRef]
- Heiden, M.G.V.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef] [Green Version]
- Golman, K.; Lerche, M.; Pehrson, R.; Ardenkjaer-Larsen, J.H. Metabolic Imaging by Hyperpolarized 13C Magnetic Resonance Imaging for In vivo Tumor Diagnosis. Cancer Res. 2006, 66, 10855–10860. [Google Scholar] [CrossRef] [Green Version]
- Gordon, J.W.; Chen, H.-Y.; Autry, A.; Park, I.; Van Criekinge, M.; Mammoli, D.; Milshteyn, E.; Bok, R.; Xu, D.; Li, Y.; et al. Translation of Carbon-13 EPI for hyperpolarized MR molecular imaging of prostate and brain cancer patients. Magn. Reson. Med. 2019, 81, 2702–2709. [Google Scholar] [CrossRef]
- Kurhanewicz, J.; Bok, R.; Nelson, S.J.; Vigneron, D.B. Current and Potential Applications of Clinical 13C MR Spectroscopy. J. Nucl. Med. 2008, 49, 341–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-Y.; Aggarwal, R.; Bok, R.A.; Ohliger, M.A.; Zhu, Z.; Lee, P.; Gordon, J.W.; Van Criekinge, M.; Carvajal, L.; Slater, J.B.; et al. Hyperpolarized 13C-pyruvate MRI detects real-time metabolic flux in prostate cancer metastases to bone and liver: A clinical feasibility study. Prostate Cancer Prostatic Dis. 2020, 23, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, R.; Vigneron, D.B.; Kurhanewicz, J. Hyperpolarized 1-[13C]-Pyruvate Magnetic Resonance Imaging Detects an Early Metabolic Response to Androgen Ablation Therapy in Prostate Cancer. Eur. Urol. 2017, 72, 1028–1029. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.; Riemer, F.; McLean, M.A.; Kaggie, J.D.; Robb, F.; Warren, A.Y.; Graves, M.J.; Gallagher, F.A. Molecular imaging of the prostate: Comparing total sodium concentration quantification in prostate cancer and normal tissue using dedicated 13C and 23Na endorectal coils. J. Magn. Reson. Imaging 2020, 51, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Kurhanewicz, J.; Vigneron, D.B. Advances in MR Spectroscopy of the Prostate. Magn. Reson. Imaging Clin. North Am. 2008, 16, 697–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, D.M.; Kurhanewicz, J. Hyperpolarized 13C MR for Molecular Imaging of Prostate Cancer. J. Nucl. Med. 2014, 55, 1567–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stødkilde-Jørgensen, H.; Laustsen, C.; Hansen, E.S.S.; Schulte, R.; Ardenkjaer-Larsen, J.H.; Comment, A.; Frøkiær, J.; Ringgaard, S.; Bertelsen, L.B.; Ladekarl, M.; et al. Pilot Study Experiences With Hyperpolarized [1-13C]pyruvate MRI in Pancreatic Cancer Patients. J. Magn. Reson. Imaging 2020, 51, 961–963. [Google Scholar] [CrossRef]
- Gallagher, F.A.; Woitek, R.; McLean, M.A.; Gill, A.B.; Garcia, R.M.; Provenzano, E.; Riemer, F.; Kaggie, J.; Chhabra, A.; Ursprung, S.; et al. Imaging breast cancer using hyperpolarized carbon-13 MRI. Proc. Natl. Acad. Sci. USA 2020, 117, 2092–2098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woitek, R.; McLean, M.A.; Gill, A.B.; Grist, J.T.; Provenzano, E.; Patterson, A.J.; Ursprung, S.; Torheim, T.; Zaccagna, F.; Locke, M.; et al. Hyperpolarized 13C MRI of Tumor Metabolism Demonstrates Early Metabolic Response to Neoadjuvant Chemotherapy in Breast Cancer. Radiol. Imaging Cancer 2020, 2, e200017. [Google Scholar] [CrossRef]
- Jagannathan, N.R. Application of in vivo MR methods in the study of breast cancer metabolism. NMR Biomed. 2019, 32, e4032. [Google Scholar] [CrossRef]
- Zhu, X.; Gordon, J.W.; Bok, R.A.; Kurhanewicz, J.; Larson, P.E. Dynamic diffusion-weighted hyperpolarized 13C imaging based on a slice-selective double spin echo sequence for measurements of cellular transport. Magn. Reson. Med. 2019, 81, 2001–2010. [Google Scholar] [CrossRef] [PubMed]
- Autry, A.W.; Gordon, J.W.; Chen, H.-Y.; Lafontaine, M.; Bok, R.; Van Criekinge, M.; Slater, J.B.; Carvajal, L.; Villanueva-Meyer, J.E.; Chang, S.M.; et al. Characterization of serial hyperpolarized 13C metabolic imaging in patients with glioma. NeuroImage Clin. 2020, 27, 102323. [Google Scholar] [CrossRef]
- Tran, M.; Latifoltojar, A.; Neves, J.B.; Papoutsaki, M.-V.; Gong, F.; Comment, A.; Costa, A.S.H.; Glaser, M.; Tran-Dang, M.-A.; El Sheikh, S.; et al. First-in-human in vivo non-invasive assessment of intra-tumoral metabolic heterogeneity in renal cell carcinoma. BJR Case Rep. 2019, 5, 20190003. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, C.; Najac, C.; Didonna, A.; Van Der Linden, A.; Ronen, S.M.; Chaumeil, M.M. Hyperpolarized 13C MR metabolic imaging can detect neuroinflammation in vivo in a multiple sclerosis murine model. Proc. Natl. Acad. Sci. USA 2017, 114, E6982–E6991. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Ringgaard, S.; Mariager, C.Ø.; Bertelsen, L.B.; Schroeder, M.; Qi, H.; Laustsen, C.; Stødkilde-Jørgensen, H. Hyperpolarized 13C Magnetic Resonance Imaging Can Detect Metabolic Changes Characteristic of Penumbra in Ischemic Stroke. Tomography 2017, 3, 67–73. [Google Scholar] [CrossRef]
- Stovell, M.G.; Yan, J.-L.; Sleigh, A.; Mada, M.O.; Carpenter, T.A.; Hutchinson, P.J.A.; Carpenter, K.L.H. Assessing Metabolism and Injury in Acute Human Traumatic Brain Injury with Magnetic Resonance Spectroscopy: Current and Future Applications. Front. Neurol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- DeVience, S.J.; Lu, X.; Proctor, J.; Rangghran, P.; Melhem, E.R.; Gullapalli, R.; Fiskum, G.M.; Mayer, D. Metabolic imaging of energy metabolism in traumatic brain injury using hyperpolarized [1-13C]pyruvate. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, C.; Chou, A.; Krukowski, K.; Najac, C.; Feng, X.; Riparip, L.-K.; Rosi, S.; Chaumeil, M.M. In vivo metabolic imaging of Traumatic Brain Injury. Sci. Rep. 2017, 7, 17525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takado, Y.; Cheng, T.; Bastiaansen, J.A.M.; Yoshihara, H.A.I.; Lanz, B.; Mishkovsky, M.; Lengacher, S.; Comment, A. Hyperpolarized 13C Magnetic Resonance Spectroscopy Reveals the Rate-Limiting Role of the Blood–Brain Barrier in the Cerebral Uptake and Metabolism of l-Lactate in Vivo. ACS Chem. Neurosci. 2018, 9, 2554–2562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.J.; Grist, J.T.; Serres, S.; Larkin, J.R.; Lau, A.Z.; Ray, K.; Fisher, K.R.; Hansen, E.; Tougaard, R.S.; Nielsen, P.M.; et al. 13C Pyruvate Transport Across the Blood-Brain Barrier in Preclinical Hyperpolarised MRI. Sci. Rep. 2018, 8, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josan, S.; Hurd, R.E.; Billingsley, K.L.; Senadheera, L.; Park, J.M.; Yen, Y.-F.; Pfefferbaum, A.; Spielman, D.M.; Mayer, D. Effects of isoflurane anesthesia on hyperpolarized 13C metabolic measurements in rat brain. Magn. Reson. Med. 2013, 70, 1117–1124. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Ramirez, M.S.; Walker, C.M.; Chen, Y.; Yi, S.; Sandulache, V.C.; Lai, S.Y.; Bankson, J.A. High-throughput hyperpolarized 13 C metabolic investigations using a multi-channel acquisition system. J. Magn. Reson. 2015, 260, 20–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Autry, A.W.; Brender, J.R.; Kishimoto, S.; Krishna, M.C.; Vareth, M.; Bok, R.A.; Reed, G.D.; Carvajal, L.; Gordon, J.W.; et al. Tensor image enhancement and optimal multichannel receiver combination analyses for human hyperpolarized 13 C MRSI. Magn. Reson. Med. 2020, 84, 3351–3365. [Google Scholar] [CrossRef]
- Gordon, J.W.; Hansen, R.B.; Shin, P.J.; Feng, Y.; Vigneron, D.B.; Larson, P.E. 3D hyperpolarized C-13 EPI with calibrationless parallel imaging. J. Magn. Reson. 2018, 289, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.J.; Ozhinsky, E.; Li, Y.; Park, I.W.; Crane, J. Strategies for rapid in vivo 1H and hyperpolarized 13C MR spectroscopic imaging. J. Magn. Reson. 2013, 229, 187–197. [Google Scholar] [CrossRef] [Green Version]
- Chung, B.T.; Chen, H.-Y.; Gordon, J.; Mammoli, D.; Sriram, R.; Autry, A.W.; Le Page, L.M.; Chaumeil, M.M.; Shin, P.; Slater, J.; et al. First hyperpolarized [2-13C]pyruvate MR studies of human brain metabolism. J. Magn. Reson. 2019, 309, 106617. [Google Scholar] [CrossRef]
- Captur, G.; Manisty, C.; Moon, J.C. Cardiac MRI evaluation of myocardial disease. Heart 2016, 102, 1429–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neubauer, S. The Failing Heart—An Engine Out of Fuel. N. Engl. J. Med. 2007, 356, 1140–1151. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, M.A.; Clarke, K.; Neubauer, S.; Tyler, D.J. Hyperpolarized Magnetic Resonance: A Novel Technique for the In Vivo Assessment of Cardiovascular Disease. Circulation 2011, 124, 1580–1594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rider, O.J.; Tyler, D.J. Clinical Implications of Cardiac Hyperpolarized Magnetic Resonance Imaging. J. Cardiovasc. Magn. Reson. 2013, 15, 93. [Google Scholar] [CrossRef] [Green Version]
- Lauritzen, M.; Sogaard, L.; Madsen, P.; Ardenkjaer-Larsen, J. Hyperpolarized Metabolic MR in the Study of Cardiac Function and Disease. Curr. Pharm. Des. 2014, 20, 6162–6170. [Google Scholar] [CrossRef] [PubMed]
- Lau, A.Z.; Lau, J.Y.C.; Chen, A.P.; Cunningham, C.H. Simultaneous multislice acquisition without trajectory modification for hyperpolarized 13 C experiments. Magn. Reson. Med. 2018, 80, 1588–1594. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, W.; Geraghty, B.J.; Lau, J.Y.; Robb, F.J.; Chen, A.P.; Cunningham, C.H. Intensity correction for multichannel hyperpolarized 13 C imaging of the heart. Magn. Reson. Med. 2015, 75, 859–865. [Google Scholar] [CrossRef]
- Rider, O.J.; Apps, A.; Miller, J.J.; Lau, J.Y.; Lewis, A.J.; Peterzan, M.A.; Dodd, M.S.; Lau, A.Z.; Trumper, C.; Gallagher, F.A.; et al. Noninvasive In Vivo Assessment of Cardiac Metabolism in the Healthy and Diabetic Human Heart Using Hyperpolarized 13 C MRI. Circ. Res. 2020, 126, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Lewis, A.J.M.; Tyler, D.J.; Rider, O. Clinical Cardiovascular Applications of Hyperpolarized Magnetic Resonance. Cardiovasc. Drugs Ther. 2020, 34, 231–240. [Google Scholar] [CrossRef] [Green Version]
- Dekkers, I.A.; De Boer, A.; Sharma, K.; Cox, E.F.; Lamb, H.J.; Buckley, D.L.; Bane, O.; Morris, D.M.; Prasad, P.V.; Semple, S.I.K.; et al. Consensus-based technical recommendations for clinical translation of renal T1 and T2 mapping MRI. Magma Magn. Reson. Mater. Phys. Biol. Med. 2020, 33, 163–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendichovszky, I.; Pullens, P.; Dekkers, I.; Nery, F.; Bane, O.; Pohlmann, A.; De Boer, A.; Ljimani, A.; Odudu, A.; Buchanan, C.; et al. Technical recommendations for clinical translation of renal MRI: A consensus project of the Cooperation in Science and Technology Action PARENCHIMA. Magma Magn. Reson. Mater. Phys. Biol. Med. 2020, 33, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laustsen, C. Hyperpolarized Renal Magnetic Resonance Imaging: Potential and Pitfalls. Front. Physiol. 2016, 7, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, E.; Olsson, L.E.; Månsson, S.; Petersson, J.; Golman, K.; Ståhlberg, F.; Wirestam, R. Perfusion assessment with bolus differentiation: A technique applicable to hyperpolarized tracers. Magn. Reson. Med. 2004, 52, 1043–1051. [Google Scholar] [CrossRef]
- Golman, K.; Petersson, J.S. Metabolic Imaging and Other Applications of Hyperpolarized 13C1. Acad. Radiol. 2006, 13, 932–942. [Google Scholar] [CrossRef]
- Laustsen, C.; Østergaard, J.A.; Lauritzen, M.H.; Nørregaard, R.; Bowen, S.; Søgaard, L.V.; Flyvbjerg, A.; Pedersen, M.; Ardenkjaer-Larsen, J.H. Assessment of early diabetic renal changes with hyperpolarized [1-13C]pyruvate. Diabetes Metab. Res. Rev. 2013, 29, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Grobner, T. Gadolinium—A specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol. Dial. Transplant. 2006, 21, 1104–1108. [Google Scholar] [CrossRef] [Green Version]
- Keshari, K.R.; Wilson, D.M.; Sai, V.; Bok, R.; Jen, K.-Y.; Larson, P.; Van Criekinge, M.; Kurhanewicz, J.; Wang, Z.J. Noninvasive In Vivo Imaging of Diabetes-Induced Renal Oxidative Stress and Response to Therapy Using Hyperpolarized 13C Dehydroascorbate Magnetic Resonance. Diabetes 2015, 64, 344–352. [Google Scholar] [CrossRef] [Green Version]
- Laustsen, C.; Lycke, S.; Palm, F.; Østergaard, J.A.; Bibby, B.M.; Nørregaard, R.; Flyvbjerg, A.; Pedersen, M.; Ardenkjaer-Larsen, J.H.; Ardenkjær-Larsen, J.H. High altitude may alter oxygen availability and renal metabolism in diabetics as measured by hyperpolarized [1-13C]pyruvate magnetic resonance imaging. Kidney Int. 2014, 86, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baligand, C.; Qin, H.; True-Yasaki, A.; Gordon, J.W.; Von Morze, C.; Santos, J.D.; Wilson, D.M.; Raffai, R.; Cowley, P.M.; Baker, A.J.; et al. Hyperpolarized13C magnetic resonance evaluation of renal ischemia reperfusion injury in a murine model. NMR Biomed. 2017, 30, e3765. [Google Scholar] [CrossRef] [PubMed]
- Reed, G.D.; Von Morze, C.; Bok, R.; Koelsch, B.L.; Van Criekinge, M.; Smith, K.J.; Larson, P.E.Z.; Kurhanewicz, J.; Vigneron, D.B.; Shang, H. High resolution (13)C MRI with hyperpolarized urea: In vivo T(2) mapping and (15)N labeling effects. IEEE Trans. Med. Imaging 2013, 33, 362–371. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, M.; Ursprung, S.; Jensen, J.D.; Jespersen, B.; Gallagher, F.; Laustsen, C. Hyperpolarised 13C-MRI metabolic and functional imaging: An emerging renal MR diagnostic modality. Magma: Magn. Reson. Mater. Phys. Biol. Med. 2019, 33, 23–32. [Google Scholar] [CrossRef]
- Durst, M.; Chiavazza, E.; Haase, A.; Aime, S.; Schwaiger, M.; Schulte, R.F. α-trideuteromethyl[15N]glutamine: A long-lived hyperpolarized perfusion marker. Magn. Reson. Med. 2016, 76, 1900–1904. [Google Scholar] [CrossRef]
- Ohliger, M.A.; Von Morze, C.; Marco-Rius, I.; Gordon, J.; Larson, P.E.Z.; Bok, R.; Chen, H.-Y.; Kurhanewicz, J.; Vigneron, D. Combining hyperpolarized 13C MRI with a liver-specific gadolinium contrast agent for selective assessment of hepatocyte metabolism. Magn. Reson. Med. 2017, 77, 2356–2363. [Google Scholar] [CrossRef] [Green Version]
- Moreno, K.X.; Satapati, S.; DeBerardinis, R.J.; Burgess, S.C.; Malloy, C.R.; Merritt, M.E. Real-time Detection of Hepatic Gluconeogenic and Glycogenolytic States Using Hyperpolarized [2-13C]Dihydroxyacetone. J. Biol. Chem. 2014, 289, 35859–35867. [Google Scholar] [CrossRef] [Green Version]
- Moon, C.-M.; Shin, S.-S.; Lim, N.-Y.; Kim, S.-K.; Kang, Y.-J.; Kim, H.-O.; Lee, S.-J.; Beak, B.-H.; Kim, Y.-H.; Jeong, G.-W. Metabolic alterations in a rat model of hepatic ischaemia reperfusion injury: In vivo hyperpolarized 13 C MRS and metabolic imaging. Liver Int. 2018, 38, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Moon, C.-M.; Shin, S.-S.; Heo, S.-H.; Lim, H.-S.; Moon, M.-J.; Surendran, S.P.; Kim, G.-E.; Park, I.-W.; Jeong, Y.-Y. Metabolic Changes in Different Stages of Liver Fibrosis: In vivo Hyperpolarized 13C MR Spectroscopy and Metabolic Imaging. Mol. Imaging Biol. 2019, 21, 842–851. [Google Scholar] [CrossRef]
- Moon, C.-M.; Oh, C.-H.; Ahn, K.-Y.; Yang, J.-S.; Kim, J.-Y.; Shin, S.-S.; Lim, H.-S.; Heo, S.-H.; Seon, H.-J.; Kim, J.-W.; et al. Metabolic biomarkers for non-alcoholic fatty liver disease induced by high-fat diet: In vivo magnetic resonance spectroscopy of hyperpolarized [1-13C] pyruvate. Biochem. Biophys. Res. Commun. 2017, 482, 112–119. [Google Scholar] [CrossRef]
- Josan, S.; Billingsley, K.L.; Orduna, J.; Park, J.M.; Luong, R.; Yu, L.; Hurd, R.E.; Pfefferbaum, A.; Spielman, D.M.; Mayer, D. Assessing inflammatory liver injury in an acute CCl4model using dynamic 3D metabolic imaging of hyperpolarized [1-13C]pyruvate. NMR Biomed. 2015, 28, 1671–1677. [Google Scholar] [CrossRef] [Green Version]
- Spielman, D.M.; Mayer, D.; Yen, Y.-F.; Tropp, J.; Hurd, R.E.; Pfefferbaum, A. In vivo measurement of ethanol metabolism in the rat liver using magnetic resonance spectroscopy of hyperpolarized [1-13C]pyruvate. Magn. Reson. Med. 2009, 62, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Jin, E.S.; Moreno, K.X.; Wang, J.; Fidelino, L.; Merritt, M.E.; Sherry, A.D.; Malloy, C.R. Metabolism of hyperpolarized [1-13C]pyruvate through alternate pathways in rat liver. NMR Biomed. 2016, 29, 466–474. [Google Scholar] [CrossRef]
- Sharma, G.; Wu, C.-Y.; Wynn, R.M.; Gui, W.; Malloy, C.R.; Sherry, A.D.; Chuang, D.T.; Khemtong, C. Real-time hyperpolarized 13C magnetic resonance detects increased pyruvate oxidation in pyruvate dehydrogenase kinase 2/4–double knockout mouse livers. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Høyer, K.F.; Laustsen, C.; Ringgaard, S.; Qi, H.; Mariager, C.Ø.; Nielsen, T.S.; Sundekilde, U.K.; Treebak, J.T.; Jessen, N.; Stødkilde-Jørgensen, H. Assessment of mouse liver [1-13C]pyruvate metabolism by dynamic hyperpolarized MRS. J. Endocrinol. 2019, 242, 251–260. [Google Scholar] [CrossRef]
- Lee, P.; Leong, W.; Tan, T.; Lim, M.; Han, W.; Radda, G.K. In Vivohyperpolarized carbon-13 magnetic resonance spectroscopy reveals increased pyruvate carboxylase flux in an insulin-resistant mouse model. Hepatology 2013, 57, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Marco-Rius, I.; Wright, A.J.; Hu, D.-E.; Savic, D.; Miller, J.J.; Timm, K.N.; Tyler, D.; Brindle, K.M.; Comment, A. Probing hepatic metabolism of [2-13C]dihydroxyacetone in vivo with 1H-decoupled hyperpolarized 13C-MR. Magma Magn. Reson. Mater. Phys. Biol. Med. 2021, 34, 49–56. [Google Scholar] [CrossRef]
- Hövener, J.-B.; Chekmenev, E.Y.; Harris, K.C.; Perman, W.H.; Tran, T.T.; Ross, B.D.; Bhattacharya, P. Quality assurance of PASADENA hyperpolarization for 13C biomolecules. Magma Magn. Reson. Mater. Phys. Biol. Med. 2008, 22, 123–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehmkuhl, S.; Suefke, M.; Kentner, A.; Yen, Y.-F.; Blümich, B.; Rosen, M.S.; Appelt, S.; Theis, T. SABRE polarized low field rare-spin spectroscopy. J. Chem. Phys. 2020, 152, 184202. [Google Scholar] [CrossRef] [PubMed]
- Berner, S.; Schmidt, A.B.; Zimmermann, M.; Pravdivtsev, A.N.; Glöggler, S.; Hennig, J.; Von Elverfeldt, D.; Hövener, J. SAMBADENA Hyperpolarization of 13C-Succinate in an MRI: Singlet-Triplet Mixing Causes Polarization Loss. ChemistryOpen 2019, 8, 728–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, M.L.; Kalechofsky, N.; Belzer, A.; Rosay, M.; Kempf, J.G. Brute-Force Hyperpolarization for NMR and MRI. J. Am. Chem. Soc. 2015, 137, 8428–8434. [Google Scholar] [CrossRef]
- Duckett, S.B.; Mewis, R.E. Application of Parahydrogen Induced Polarization Techniques in NMR Spectroscopy and Imaging. Acc. Chem. Res. 2012, 45, 1247–1257. [Google Scholar] [CrossRef]
- Reineri, F.; Boi, T.; Aime, S. ParaHydrogen Induced Polarization of 13C carboxylate resonance in acetate and pyruvate. Nat. Commun. 2015, 6, 5858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardenkjaer-Larsen, J.H.; Leach, A.M.; Clarke, N.; Urbahn, J.; Anderson, D.; Skloss, T.W. Dynamic nuclear polarization polarizer for sterile use intent. NMR Biomed. 2011, 24, 927–932. [Google Scholar] [CrossRef]
- Ardenkjaer-Larsen, J.H.; Bowen, S.; Petersen, J.R.; Rybalko, O.; Vinding, M.S.; Ullisch, M.; Nielsen, N.C. Cryogen-free dissolution dynamic nuclear polarization polarizer operating at 3.35 T, 6.70 T, and 10.1 T. Magn. Reson. Med. 2019, 81, 2184–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, T.; Gaunt, A.P.; Marco-Rius, I.; Gehrung, M.; Chen, A.P.; Van Der Klink, J.J.; Comment, A. A multisample 7 T dynamic nuclear polarization polarizer for preclinical hyperpolarized MR. NMR Biomed. 2020, 33, e4264. [Google Scholar] [CrossRef]
- Pinon, A.C.; Capozzi, A.; Ardenkjær-Larsen, J.H. Hyperpolarization via dissolution dynamic nuclear polarization: New technological and methodological advances. Magma Magn. Reson. Mater. Phys. Biol. Med. 2021, 34, 5–23. [Google Scholar] [CrossRef]
- Hurd, R.E.; Yen, Y.-F.; Chen, A.; Ardenkjaer-Larsen, J.H. Hyperpolarized13C metabolic imaging using dissolution dynamic nuclear polarization. J. Magn. Reson. Imaging 2012, 36, 1314–1328. [Google Scholar] [CrossRef] [PubMed]
- Maudsley, A. Sensitivity in fourier imaging. J. Magn. Reson. 1986, 68, 363–366. [Google Scholar] [CrossRef]
- Golman, K.; Thaning, M. Real-time metabolic imaging. Proc. Natl. Acad. Sci. USA 2006, 103, 11270–11275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, Y.-F.; Kohler, S.; Chen, A.; Tropp, J.; Bok, R.; Wolber, J.; Albers, M.; Gram, K.; Zierhut, M.; Park, I.; et al. Imaging considerations for in vivo13C metabolic mapping using hyperpolarized13C-pyruvate. Magn. Reson. Med. 2009, 62, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Mayer, D.; Levin, Y.S.; Hurd, R.E.; Glover, G.H.; Spielman, D.M. Fast metabolic imaging of systems with sparse spectra: Application for hyperpolarized13C imaging. Magn. Reson. Med. 2006, 56, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, M.S.; Lee, J.; Walker, C.M.; Sandulache, V.C.; Hennel, F.; Lai, S.Y.; Bankson, J.A. Radial spectroscopic MRI of hyperpolarized [1-13C] pyruvate at 7 tesla. Magn. Reson. Med. 2014, 72, 986–995. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Lustig, M.; Larson, P.E.Z. Concentric rings K-space trajectory for hyperpolarized 13C MR spectroscopic imaging. Magn. Reson. Med. 2016, 75, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, J.W.; Chen, H.; Dwork, N.; Tang, S.; Larson, P.E.Z. Fast Imaging for Hyperpolarized MR Metabolic Imaging. J. Magn. Reson. Imaging 2021, 53, 686–702. [Google Scholar] [CrossRef] [PubMed]
- Schulte, R.F.; Sperl, J.I.; Weidl, E.; Menzel, M.I.; Janich, M.A.; Khegai, O.; Durst, M.; Ardenkjaer-Larsen, J.H.; Glaser, S.J.; Haase, A.; et al. Saturation-recovery metabolic-exchange rate imaging with hyperpolarized [1-13C] pyruvate using spectral-spatial excitation. Magn. Reson. Med. 2012, 69, 1209–1216. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, C.H.; Chen, A.P.; Lustig, M.; Hargreaves, B.A.; Lupo, J.; Xu, D.; Kurhanewicz, J.; Hurd, R.E.; Pauly, J.M.; Nelson, S.J.; et al. Pulse sequence for dynamic volumetric imaging of hyperpolarized metabolic products. J. Magn. Reson. 2008, 193, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arunachalam, A.; Whitt, D.; Fish, K.; Giaquinto, R.; Piel, J.; Watkins, R.; Hancu, I. Accelerated spectroscopic imaging of hyperpolarized C-13 pyruvate using SENSE parallel imaging. NMR Biomed. 2009, 22, 867–873. [Google Scholar] [CrossRef]
- Chen, H.-Y.; Larson, P.E.; Gordon, J.W.; Bok, R.A.; Ferrone, M.; Van Criekinge, M.; Carvajal, L.; Cao, P.; Pauly, J.M.; Kerr, A.B.; et al. Technique development of 3D dynamic CS-EPSI for hyperpolarized 13 C pyruvate MR molecular imaging of human prostate cancer. Magn. Reson. Med. 2018, 80, 2062–2072. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Lustig, M.; Chen, A.P.; Crane, J.; Kerr, A.; Kelley, D.A.; Hurd, R.; Kurhanewicz, J.; Nelson, S.J.; Pauly, J.M.; et al. Compressed sensing for resolution enhancement of hyperpolarized 13C flyback 3D-MRSI. J. Magn. Reson. 2008, 192, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, S.; Lustig, M.; Balakrishnan, A.; Larson, P.E.Z.; Bok, R.; Kurhanewicz, J.; Nelson, S.J.; Goga, A.; Pauly, J.M.; Vigneron, D.B. 3D compressed sensing for highly accelerated hyperpolarized 13 C MRSI with in vivo applications to transgenic mouse models of cancer. Magn. Reson. Med. 2010, 63, 312–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, P.E.Z.; Hu, S.; Lustig, M.; Kerr, A.B.; Nelson, S.J.; Kurhanewicz, J.; Pauly, J.M.; Vigneron, D.B. Fast dynamic 3D MR spectroscopic imaging with compressed sensing and multiband excitation pulses for hyperpolarized 13C studies. Magn. Reson. Med. 2011, 65, 610–619. [Google Scholar] [CrossRef] [Green Version]
- Sigfridsson, A.; Weiss, K.; Wissmann, L.; Busch, J.; Krajewski, M.; Batel, M.; Batsios, G.; Ernst, M.; Kozerke, S. Hybrid multiband excitation multiecho acquisition for hyperpolarized 13 C spectroscopic imaging. Magn. Reson. Med. 2014, 73, 1713–1717. [Google Scholar] [CrossRef]
- Hu, X.; Levin, D.N.; Lauterbur, P.C.; Spraggins, T. SLIM: Spectral localization by imaging. Magn. Reson. Med. 1988, 8, 314–322. [Google Scholar] [CrossRef]
- Von Kienlin, M.; Mejia, R. Spectral localization with optimal pointspread function. J. Magn. Reson. 1991, 94, 268–287. [Google Scholar] [CrossRef]
- Farkash, G.; Markovic, S.; Novakovic, M.; Frydman, L. Enhanced hyperpolarized chemical shift imaging based on a priori segmented information. Magn. Reson. Med. 2019, 81, 3080–3093. [Google Scholar] [CrossRef]
- Zhang, Y.; Gabr, R.E.; Schär, M.; Weiss, R.G.; Bottomley, P.A. Magnetic resonance Spectroscopy with Linear Algebraic Modeling (SLAM) for higher speed and sensitivity. J. Magn. Reson. 2012, 218, 66–76. [Google Scholar] [CrossRef] [Green Version]
- Haldar, J.P.; Liang, Z.-P. Spatiotemporal imaging with partially separable functions: A matrix recovery approach. In Proceedings of the 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Rotterdam, The Netherlands, 14–17 April 2010; pp. 716–719. [Google Scholar] [CrossRef]
- Lee, H.; Song, J.E.; Shin, J.; Joe, E.; Joo, C.G.; Choi, Y.-S.; Song, H.-T.; Kim, D.-H. High resolution hyperpolarized13C MRSI using SPICE at 9.4 T. Magn. Reson. Med. 2018, 80, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Song, J.E.; Shin, J.; Lee, H.; Choi, Y.; Song, H.; Kim, D. Dynamic hyperpolarized 13 C MR spectroscopic imaging using SPICE in mouse kidney at 9.4 T. NMR Biomed. 2020, 33, e4230. [Google Scholar] [CrossRef] [PubMed]
- Wiesinger, F.; Weidl, E.; Menzel, M.I.; Janich, M.A.; Khegai, O.; Glaser, S.J.; Haase, A.; Schwaiger, M.; Schulte, R.F. IDEAL spiral CSI for dynamic metabolic MR imaging of hyperpolarized [1-13C]pyruvate. Magn. Reson. Med. 2012, 68, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.W.; Larson, P.E. Pulse Sequences for Hyperpolarized MRS. Encycl. Magn. Reson. 2016, 5, 1229–1246. [Google Scholar] [CrossRef]
- Gordon, J.W.; Vigneron, D.B.; Larson, P.E.Z. Development of a symmetric echo planar imaging framework for clinical translation of rapid dynamic hyperpolarized 13 C imaging. Magn. Reson. Med. 2016, 77, 826–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purvis, L.A.B.; Clarke, W.T.; Biasiolli, L.; Valkovič, L.; Robson, M.D.; Rodgers, C.T. OXSA: An open-source magnetic resonance spectroscopy analysis toolbox in MATLAB. PLoS ONE 2017, 12, e0185356. [Google Scholar] [CrossRef]
- Naressi, A.; Couturier, C.; Devos, J.M.; Janssen, M.; Mangeat, C.; De Beer, R.; Graveron-Demilly, D. Java-based graphical user interface for the MRUI quantitation package. Magma Magn. Reson. Mater. Phys. Biol. Med. 2001, 12, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Henry, P.-G.; Öz, G.; Provencher, S.; Gruetter, R. Toward dynamic isotopomer analysis in the rat brainin vivo: Automatic quantitation of13C NMR spectra using LCModel. NMR Biomed. 2003, 16, 400–412. [Google Scholar] [CrossRef]
- Cavassila, S.; Deval, S.; Huegen, C.; Van Ormondt, D.; Graveron-Demilly, D. Cramér-Rao bounds: An evaluation tool for quantitation. NMR Biomed. 2001, 14, 278–283. [Google Scholar] [CrossRef]
- Young, K.; Khetselius, D.; Soher, B.J.; Maudsley, A.A. Confidence images for MR spectroscopic imaging. Magn. Reson. Med. 2000, 44, 537–545. [Google Scholar] [CrossRef]
- Nelson, S.J.; Brown, T.R. The accuracy of quantification from 1D NMR spectra using the PIQABLE algorithm. J. Magn. Reson. 1989, 84, 95–109. [Google Scholar] [CrossRef]
- Brender, J.R.; Kishimoto, S.; Merkle, H.; Reed, G.; Hurd, R.E.; Chen, A.P.; Ardenkjaer-Larsen, J.H.; Munasinghe, J.; Saito, K.; Seki, T.; et al. Dynamic Imaging of Glucose and Lactate Metabolism by 13C-MRS without Hyperpolarization. Sci. Rep. 2019, 9, 3410. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.; Yang, C.; Jindal, A.; DeBerardinis, R.J.; Hooshyar, M.A.; Merritt, M.E.; Sherry, A.D.; Malloy, C.R. Comparison of kinetic models for analysis of pyruvate-to-lactate exchange by hyperpolarized13C NMR. NMR Biomed. 2012, 25, 1286–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagès, G.; Kuchel, P.W. Mathematical Modeling and Data Analysis of Nmr Experiments Using Hyperpolarized 13C Metabolites. Magn. Reson. Insights 2013, 6, MRI.S11084-21. [Google Scholar] [CrossRef] [Green Version]
- Larson, P.E.Z.; Chen, H.; Gordon, J.W.; Korn, N.; Maidens, J.; Arcak, M.; Tang, S.; Criekinge, M.; Carvajal, L.; Mammoli, D.; et al. Investigation of analysis methods for hyperpolarized 13C-pyruvate metabolic MRI in prostate cancer patients. NMR Biomed. 2018, 31, e3997. [Google Scholar] [CrossRef]
- Hill, D.K.; Orton, M.R.; Mariotti, E.; Boult, J.K.R.; Panek, R.; Jafar, M.; Parkes, H.G.; Jamin, Y.; Miniotis, M.F.; Al-Saffar, N.M.S.; et al. Model Free Approach to Kinetic Analysis of Real-Time Hyperpolarized 13C Magnetic Resonance Spectroscopy Data. PLoS ONE 2013, 8, e71996. [Google Scholar] [CrossRef]
- Daniels, C.J.; McLean, M.A.; Schulte, R.F.; Robb, F.J.; Gill, A.B.; McGlashan, N.; Graves, M.J.; Schwaiger, M.; Lomas, D.J.; Brindle, K.M.; et al. A comparison of quantitative methods for clinical imaging with hyperpolarized 13 C-pyruvate. NMR Biomed. 2016, 29, 387–399. [Google Scholar] [CrossRef] [Green Version]
- Santarelli, M.F.; Positano, V.; Giovannetti, G.; Frijia, F.; Menichetti, L.; Ardenkjaer-Larsen, J.-H.; De Marchi, D.; Lionetti, V.; Aquaro, G.; Lombardi, M.; et al. How the signal-to-noise ratio influences hyperpolarized 13C dynamic MRS data fitting and parameter estimation. NMR Biomed. 2011, 25, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, F.A.; Kettunen, M.I.; Brindle, K.M. Imaging pH with hyperpolarized 13 C. NMR Biomed. 2011, 24, 1006–1015. [Google Scholar] [CrossRef]
- Gallagher, F.A.; Kettunen, M.I.; Day, S.E.; Hu, D.-E.; Ardenkjaer-Larsen, J.H.; Zandt, R.; Jensen, P.R.; Karlsson, M.; Golman, K.; Lerche, M.H.; et al. Magnetic resonance imaging of pH in vivo using hyperpolarized 13C-labelled bicarbonate. Nat. Cell Biol. 2008, 453, 940–943. [Google Scholar] [CrossRef]
- Pourfathi, M.; Kadlecek, S.J.; Chatterjee, S.; Rizi, R.R. Metabolic Imaging and Biological Assessment: Platforms to Evaluate Acute Lung Injury and Inflammation. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Ishii, M.; Emami, K.; Kadlecek, S.; Petersson, J.S.; Golman, K.; Vahdat, V.; Yu, J.; Cadman, R.V.; MacDuffie-Woodburn, J.; Stephen, M.; et al. Hyperpolarized13C MRI of the pulmonary vasculature and parenchyma. Magn. Reson. Med. 2007, 57, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Lipso, K.W.; Magnusson, P.; Ardenkjaer-Larsen, J.H. Hyperpolarized 13C MR Angiography. Curr. Pharm. Des. 2015, 22, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markovic, S.; Fages, A.; Roussel, T.; Hadas, R.; Brandis, A.; Neeman, M.; Frydman, L. Placental physiology monitored by hyperpolarized dynamic 13C magnetic resonance. Proc. Natl. Acad. Sci. USA 2018, 115, E2429–E2436. [Google Scholar] [CrossRef] [Green Version]
- Madsen, K.E.; Mariager, C.Ø.; Duvald, C.S.; Hansen, E.S.S.; Bertelsen, L.B.; Pedersen, M.; Pedersen, L.H.; Uldbjerg, N.; Laustsen, C. Ex Vivo Human Placenta Perfusion, Metabolic and Functional Imaging for Obstetric Research—A Feasibility Study. Tomography 2019, 5, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Josan, S.; Mayer, D.; Hurd, R.E.; Chung, Y.; Bendahan, D.; Spielman, D.M.; Jue, T. Hyperpolarized 13C NMR observation of lactate kinetics in skeletal muscle. J. Exp. Biol. 2015, 218, 3308–3318. [Google Scholar] [CrossRef] [Green Version]
- Leftin, A.; Degani, H.; Frydman, L. In vivo magnetic resonance of hyperpolarized [13C1]pyruvate: Metabolic dynamics in stimulated muscle. Am. J. Physiol. Metab. 2013, 305, E1165–E1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastiaansen, J.A.; Cheng, T.; Mishkovsky, M.; Duarte, J.M.; Comment, A.; Gruetter, R. In vivo enzymatic activity of acetylCoA synthetase in skeletal muscle revealed by 13C turnover from hyperpolarized [1-13C]acetate to [1-13C]acetylcarnitine. Biochim. Biophys. Acta Gen. Subj. 2013, 1830, 4171–4178. [Google Scholar] [CrossRef] [Green Version]
- Laustsen, C. Hyperpolarized 13C Magnetic Resonance Treatment Response Monitoring: A New Paradigm for Multiorgan Metabolic Assessment of Pharmacological Interventions? Diabetes 2016, 65, 3529–3531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, A.J.; Miller, J.J.; McCallum, C.; Rider, O.J.; Neubauer, S.; Heather, L.C.; Tyler, D.J. Assessment of Metformin-Induced Changes in Cardiac and Hepatic Redox State Using Hyperpolarized[1-13C]Pyruvate. Diabetes 2016, 65, 3544–3551. [Google Scholar] [CrossRef] [Green Version]
- Bertelsen, L.B.; Nielsen, P.M.; Qi, H.; Nørlinger, T.S.; Zhang, X.; Stødkilde-Jørgensen, H.; Laustsen, C. Diabetes induced renal urea transport alterations assessed with 3D hyperpolarized13C,15N-Urea. Magn. Reson. Med. 2017, 77, 1650–1655. [Google Scholar] [CrossRef]
- Larson, P.E.Z.; Gold, G.E. Science to practice: Can inflammatory arthritis be monitored by using MR imaging with injected hyperpolarized 13C-pyruvate? Radiology 2011, 259, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Neveu, M.-A.; Beziere, N.; Daniels, R.; Bouzin, C.; Comment, A.; Schwenck, J.; Fuchs, K.; Kneilling, M.; Pichler, B.J.; Schmid, A.M. Lactate Production Precedes Inflammatory Cell Recruitment in Arthritic Ankles: An Imaging Study. Mol. Imaging Biol. 2020, 22, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Le Page, L.M.; Guglielmetti, C.; Najac, C.F.; Tiret, B.; Chaumeil, M.M. Hyperpolarized 13C magnetic resonance spectroscopy detects toxin-induced neuroinflammation in mice. NMR Biomed. 2019, 32, e4164. [Google Scholar] [CrossRef] [Green Version]
- Thind, K.; Chen, A.; Friesen-Waldner, L.; Ouriadov, A.; Scholl, T.J.; Fox, M.; Wong, E.; VanDyk, J.; Hope, A.; Santyr, G. Detection of radiation-induced lung injury using hyperpolarized13C magnetic resonance spectroscopy and imaging. Magn. Reson. Med. 2012, 70, 601–609. [Google Scholar] [CrossRef]
- Thind, K.; Jensen, M.D.; Hegarty, E.; Chen, A.P.; Lim, H.; Martínez-Santiesteban, F.; Van Dyk, J.; Wong, E.; Scholl, T.J.; Santyr, G.E. Mapping metabolic changes associated with early Radiation Induced Lung Injury post conformal radiotherapy using hyperpolarized 13C-pyruvate Magnetic Resonance Spectroscopic Imaging. Radiother. Oncol. 2014, 110, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumata, L.L.; Yang, C.; Ragavan, M.; Carpenter, N.R.; DeBerardinis, R.J.; Merritt, M.E. Hyperpolarized 13C Magnetic Resonance and Its Use in Metabolic Assessment of Cultured Cells and Perfused Organs. In Methods in Enzymology; Academic Press Inc.: Cambridge, MA, USA, 2015; Volume 561, pp. 73–106. [Google Scholar]
- Brindle, K.M. Imaging Metabolism with Hyperpolarized13C-Labeled Cell Substrates. J. Am. Chem. Soc. 2015, 137, 6418–6427. [Google Scholar] [CrossRef]
- Katsikis, S.; Marin-Montesinos, I.; Ludwig, C.; Günther, U.L. Detecting acetylated aminoacids in blood serum using hyperpolarized 13C-1H-2D-NMR. J. Magn. Reson. 2019, 305, 175–179. [Google Scholar] [CrossRef]
- Shishmarev, D.; Kuchel, P.W.; Pagès, G.; Wright, A.J.; Hesketh, R.L.; Kreis, F.; Brindle, K.M. Glyoxalase activity in human erythrocytes and mouse lymphoma, liver and brain probed with hyperpolarized 13C-methylglyoxal. Commun. Biol. 2018, 1, 232. [Google Scholar] [CrossRef]
- Sriram, R.; Sun, J.; Villanueva-Meyer, J.; Mutch, C.; Santos, J.D.L.; Peters, J.; Korenchan, D.E.; Neumann, K.; Van Criekinge, M.; Kurhanewicz, J.; et al. Detection of Bacteria-Specific Metabolism Using Hyperpolarized [2-13C]Pyruvate. ACS Infect. Dis. 2018, 4, 797–805. [Google Scholar] [CrossRef]
- Autry, A.; Park, I.; Kline, C.; Chen, H.-Y.; Gordon, J.; Raber, S.; Hoffman, C.; Kim, Y.; Okamoto, K.; Vigneron, D.; et al. Pilot Study of Hyperpolarized 13C Metabolic Imaging in Pediatric Patients with Diffuse Intrinsic Pontine Glioma and Other CNS Cancers. Am. J. Neuroradiol. 2021, 42, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Capozzi, A.; Patel, M.S.S.; Gunnarsson, M.S.C.P.; Marco-Rius, I.; Comment, A.; Karlsson, M.; Lerche, M.H.; Ouari, O.; Ardenkjaer-Larsen, J.H. Efficient Hyperpolarization of U-13 C-Glucose Using Narrow-Line UV-Generated Labile Free Radicals. Angew. Chem. Int. Ed. 2019, 58, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Damián, P.A.G.; Sperl, J.I.; Janich, M.A.; Khegai, O.; Wiesinger, F.; Glaser, S.J.; Haase, A.; Schwaiger, M.; Schulte, R.F.; Menzel, M.I. Multisite Kinetic Modeling of13C Metabolic MR Using [1-13C]Pyruvate. Radiol. Res. Pr. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Crane, J.C.; Gordon, J.W.; Chen, H.-Y.; Autry, A.W.; Li, Y.; Olson, M.P.; Kurhanewicz, J.; Vigneron, D.B.; Larson, P.E.; Xu, D. Hyperpolarized 13C MRI data acquisition and analysis in prostate and brain at University of California, San Francisco. NMR Biomed. 2020, e4280. [Google Scholar] [CrossRef] [PubMed]
- Park, I.; Larson, P.E.; Gordon, J.W.; Carvajal, L.; Chen, H.-Y.; Bok, R.; Van Criekinge, M.; Ferrone, M.; Slater, J.B.; Xu, D.; et al. Development of methods and feasibility of using hyperpolarized carbon-13 imaging data for evaluating brain metabolism in patient studies. Magn. Reson. Med. 2018, 80, 864–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Area of Interest | Publications | Human Trials | Translation State |
|---|---|---|---|
| Oncology | 170 | prostate: [7,20,22,23,24] pancreas: [27], breast: [28,29], brain: [9,20,32,153], kidney: [33] | High |
| Brain | 37 | [8,13,46] | Low |
| Heart | 87 | [5,54] | Medium |
| Kidney | 31 | - | Low |
| Liver | 21 | - | Low |
| Technical advances 1 | 349 | - | - |
| Other 2 | 118 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaeggemose, M.; F. Schulte, R.; Laustsen, C. Comprehensive Literature Review of Hyperpolarized Carbon-13 MRI: The Road to Clinical Application. Metabolites 2021, 11, 219. https://doi.org/10.3390/metabo11040219
Vaeggemose M, F. Schulte R, Laustsen C. Comprehensive Literature Review of Hyperpolarized Carbon-13 MRI: The Road to Clinical Application. Metabolites. 2021; 11(4):219. https://doi.org/10.3390/metabo11040219
Chicago/Turabian StyleVaeggemose, Michael, Rolf F. Schulte, and Christoffer Laustsen. 2021. "Comprehensive Literature Review of Hyperpolarized Carbon-13 MRI: The Road to Clinical Application" Metabolites 11, no. 4: 219. https://doi.org/10.3390/metabo11040219