
Analysis of Walking Economy after Sleeve Gastrectomy in Patients with Severe Obesity
 , , , , , , , and
, , , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sleeve Gastrectomy
2.3. Anthropometric Measurements
2.4. Cardiopulmonary Exercise Testing
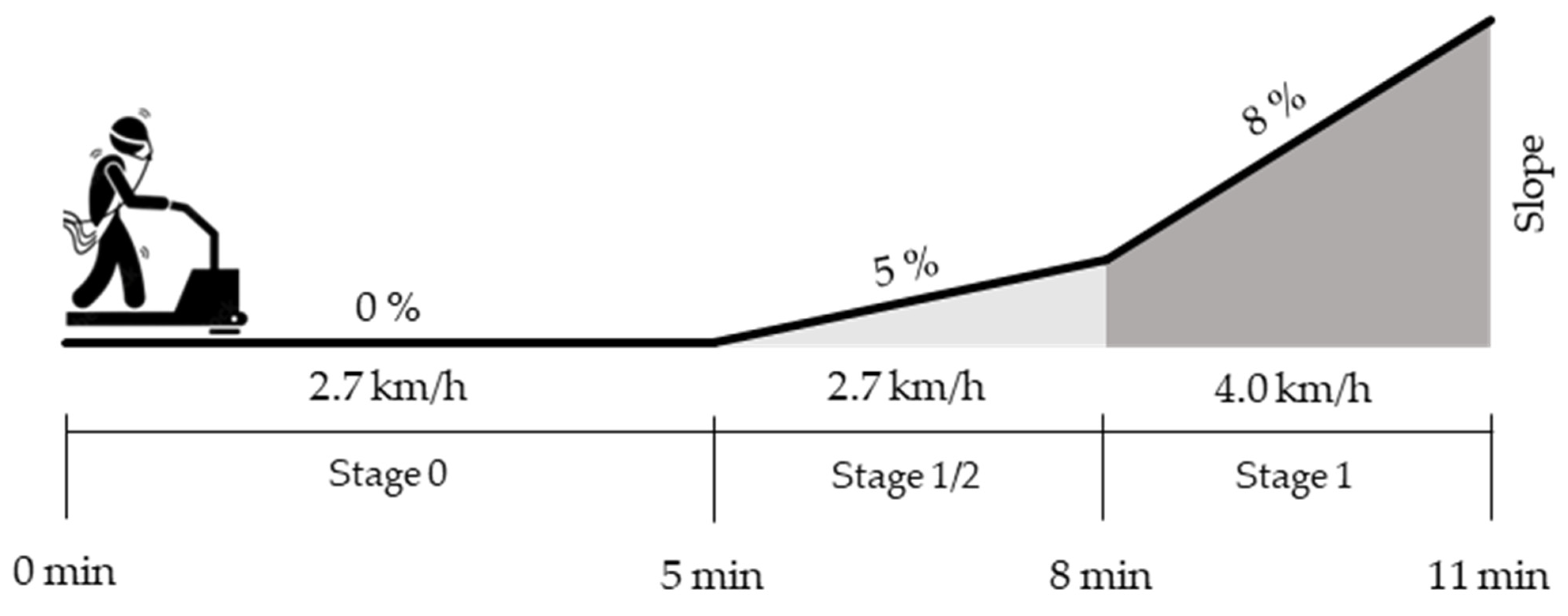
2.5. Protocol Stages and Energy Cost
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Regional Office for Europe. WHO European Regional Obesity Report 2022; WHO: Geneva, Switzerland, 2022; ISBN 9789289057738. [Google Scholar]
- Malnick, S.D.H.; Knobler, H. The Medical Complications of Obesity. QJM 2006, 99, 565–579. [Google Scholar] [CrossRef] [PubMed]
- González-Muniesa, P.; Mártinez-González, M.A.; Hu, F.B.; Després, J.P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Prim. 2017, 3, 17034. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.P.; Mesidor, M.; Winters, K.; Dubbert, P.M.; Wyatt, S.B. Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem. Curr. Obes. Rep. 2015, 4, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global Epidemiology and Pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global Burden of Obesity in 2005 and Projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef]
- Di Cesare, M.; Bentham, J.; Stevens, G.A.; Zhou, B.; Danaei, G.; Lu, Y.; Bixby, H.; Cowan, M.J.; Riley, L.M.; Hajifathalian, K.; et al. Trends in Adult Body-Mass Index in 200 Countries from 1975 to 2014: A Pooled Analysis of 1698 Population-Based Measurement Studies with 19.2 Million Participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- Aghili, S.M.M.; Ebrahimpur, M.; Arjmand, B.; Shadman, Z.; Pejman Sani, M.; Qorbani, M.; Larijani, B.; Payab, M. Obesity in COVID-19 Era, Implications for Mechanisms, Comorbidities, and Prognosis: A Review and Meta-Analysis. Int. J. Obes. 2021, 45, 998–1016. [Google Scholar] [CrossRef]
- Palermi, S.; Vecchiato, M.; Pennella, S.; Marasca, A.; Spinelli, A.; de Luca, M.; de Martino, L.; Fernando, F.; Sirico, F.; Biffi, A. The Impact of the COVID-19 Pandemic on Childhood Obesity and Lifestyle—A Report from Italy. Pediatr. Rep. 2022, 14, 410–418. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for Weight Loss in Adults. Cochrane Database Syst. Rev. 2014, 2014, 107–114. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; Christian, N.J.; Belle, S.H.; Berk, P.D.; Flum, D.R.; Garcia, L.; Horlick, M.; Kalarchian, M.A.; King, W.C.; Mitchell, J.E.; et al. Weight Change and Health Outcomes at 3 Years after Bariatric Surgery among Individuals with Severe Obesity. JAMA 2013, 310, 2416–2425. [Google Scholar] [CrossRef]
- Bellicha, A.; Ciangura, C.; Roda, C.; Torcivia, A.; Aron-Wisnewsky, J.; Poitou, C.; Oppert, J.M. Effect of Exercise Training after Bariatric Surgery: A 5-Year Follow-up Study of a Randomized Controlled Trial. PLoS ONE 2022, 17, e0271561. [Google Scholar] [CrossRef] [PubMed]
- Herman, K.M.; Carver, T.E.; Christou, N.V.; Andersen, R.E. Physical Activity and Sitting Time in Bariatric Surgery Patients 1-16 Years Post-Surgery. Clin. Obes. 2014, 4, 267–276. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate Physical Activity Intervention Strategies for Weight Loss and Prevention of Weight Regain for Adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Villablanca, P.A.; Alegria, J.R.; Mookadam, F.; Holmes, D.R.; Wright, R.S.; Levine, J.A. Nonexercise Activity Thermogenesis in Obesity Management. Mayo. Clin. Proc. 2015, 90, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.A.; vander Weg, M.W.; Hill, J.O.; Klesges, R.C. Non-Exercise Activity Thermogenesis: The Crouching Tiger Hidden Dragon of Societal Weight Gain. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.A.; Mecrady, S.K.; Lanningham-Foster, L.M.; Kane, P.H.; Foster, R.C.; Manohar, C.U. The Role of Free-Living Daily Walking in Human Weight Gain and Obesity. Diabetes 2008, 57, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.R.; Weinsier, R.L.; Zuckerman, P.A.; Darnell, B.E. Aerobic Fitness, Physiologic Difficulty and Physical Activity in Black and White Women. Int. J. Obes. 2004, 28, 1111–1117. [Google Scholar] [CrossRef]
- Murtagh, E.M.; Nichols, L.; Mohammed, M.A.; Holder, R.; Nevill, A.M.; Murphy, M.H. The Effect of Walking on Risk Factors for Cardiovascular Disease: An Updated Systematic Review and Meta-Analysis of Randomised Control Trials. Prev. Med. 2015, 72, 34–43. [Google Scholar] [CrossRef]
- Lafortuna, C.L.; Agosti, F.; Galli, R.; Busti, C.; Lazzer, S.; Sartorio, A. The Energetic and Cardiovascular Response to Treadmill Walking and Cycle Ergometer Exercise in Obese Women. Eur. J. Appl. Physiol. 2008, 103, 707–717. [Google Scholar] [CrossRef]
- Primavesi, J.; Menéndez, A.F.; Hans, D.; Favre, L.; Crettaz von Roten, F.; Malatesta, D. The Effect of Obesity Class on the Energetics and Mechanics of Walking. Nutrients 2021, 13, 4546. [Google Scholar] [CrossRef]
- Laroche, D.P.; Marques, N.R.; Shumila, H.N.; Logan, C.R.; Laurent, R.S.; Goncąlves, M. Excess Body Weight and Gait Influence Energy Cost of Walking in Older Adults. Med. Sci. Sports Exerc. 2015, 47, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, A.F.; Uva, B.; Favre, L.; Hans, D.; Borrani, F.; Malatesta, D. Mass-Normalized Internal Mechanical Work in Walking Is Not Impaired in Adults with Class III Obesity. J. Appl. Physiol. 2020, 129, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Browning, R.C.; Reynolds, M.M.; Board, W.J.; Walters, K.A.; Reiser, R.F. Obesity Does Not Impair Walking Economy across a Range of Speeds and Grades. J. Appl. Physiol. 2013, 114, 1125–1131. [Google Scholar] [CrossRef]
- Bode, V.G.; Croce, R.V.; Quinn, T.J.; Laroche, D.P. Influence of Excess Weight on Lower-Extremity Vertical Stiffness and Metabolic Cost of Walking. Eur. J. Sport Sci. 2020, 20, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.R.; Fisher, G.; Neumeier, W.H.; Carter, S.J.; Plaisance, E.P. Exercise Training and Energy Expenditure Following Weight Loss. Med. Sci. Sports Exerc. 2015, 47, 1950–1957. [Google Scholar] [CrossRef]
- Stephenson, J.; Smith, C.M.; Kearns, B.; Haywood, A.; Bissell, P. The Association between Obesity and Quality of Life: A Retrospective Analysis of a Large-Scale Population-Based Cohort Study. BMC Public Health 2021, 21, 1990. [Google Scholar] [CrossRef]
- Vecchiato, M.; Quinto, G.; Palermi, S.; Foccardi, G.; Mazzucato, B.; Battista, F.; Duregon, F.; Michieletto, F.; Neunhaeuserer, D.; Ermolao, A. Are Gyms a Feasible Setting for Exercise Training Interventions in Patients with Cardiovascular Risk Factors? An Italian 10-Years Cross-Sectional Survey Comparison. Int. J. Environ. Res. Public Health 2022, 19, 2407. [Google Scholar] [CrossRef]
- Borges, J.H.; Carter, S.J.; Singh, H.; Hunter, G.R. Inverse Relationship between Changes of Maximal Aerobic Capacity and Changes in Walking Economy after Weight Loss. Eur. J. Appl. Physiol. 2018, 118, 1573–1578. [Google Scholar] [CrossRef]
- D’alleva, M.; Gonnelli, F.; Vaccari, F.; Boirie, Y.; Montaurier, C.; Thivel, D.; Isacco, L.; Vermorel, M.; Lazzer, S. Energy Cost of Walking and Body Composition Changes during a 9-Month Multidisciplinary Weight Reduction Program and 4-Month Follow-up in Adolescents with Obesity. Appl. Physiol. Nutr. Metab. 2021, 47, 60–68. [Google Scholar] [CrossRef]
- Malatesta, D.; Favre, J.; Ulrich, B.; Hans, D.; Suter, M.; Favre, L.; Fernández Menéndez, A. Effect of Very Large Body Mass Loss on Energetics, Mechanics and Efficiency of Walking in Adults with Obesity: Mass-Driven versus Behavioural Adaptations. J. Physiol. 2022, 600, 979–996. [Google Scholar] [CrossRef]
- Serés, L.; Lopez-Ayerbe, J.; Coll, R.; Rodriguez, O.; Vila, J.; Formiguera, X.; Alastrue, A.; Rull, M.; Valle, V. Increased Exercise Capacity after Surgically Induced Weight Loss in Morbid Obesity. Obesity 2006, 14, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402. [Google Scholar] [CrossRef] [PubMed]
- Mognol, P.; Chosidow, D.; Marmuse, J.P. Laparoscopic Sleeve Gastrectomy as an Initial Bariatric Operation for High-Risk Patients: Initial Results in 10 Patients. Obes. Surg. 2005, 15, 1030–1033. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Jeukendrup, A.E. Validity and Reliability of Three Commercially Available Breath-by-Breath Respiratory Systems. Eur. J. Appl. Physiol. 2002, 86, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Radtke, T.; Crook, S.; Kaltsakas, G.; Louvaris, Z.; Berton, D.; Urquhart, D.S.; Kampouras, A.; Rabinovich, R.A.; Verges, S.; Kontopidis, D.; et al. ERS Statement on Standardisation of Cardiopulmonary Exercise Testing in Chronic Lung Diseases. Eur. Respir. Rev. 2019, 28, 1901441. [Google Scholar] [CrossRef]
- Wood, R.E.; Hills, A.P.; Hunter, G.R.; King, N.A.; Byrne, N.M. Vo2max in Overweight and Obese Adults: Do They Meet the Threshold Criteria? Med. Sci Sports Exerc. 2010, 42, 470–477. [Google Scholar] [CrossRef]
- Glass, S.; Dwyer, G.B. ACSM’s Metabolic Calculations Handbook; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; ISBN 9780781742382. [Google Scholar]
- Vecchiato, M.; Neunhaeuserer, D.; Quinto, G.; Bettini, S.; Gasperetti, A.; Battista, F.; Vianello, A.; Vettor, R.; Busetto, L.; Ermolao, A. Cardiopulmonary Exercise Testing in Patients with Moderate-Severe Obesity: A Clinical Evaluation Tool for OSA? Sleep Breath. 2021, 1, 1115–1123. [Google Scholar] [CrossRef]
- Garby, L.; Astrup, A. The Relationship between the Respiratory Quotient and the Energy Equivalent of Oxygen during Simultaneous Glucose and Lipid Oxidation and Lipogenesis. Acta Physiol. Scand. 1987, 129, 443–444. [Google Scholar] [CrossRef]
- Saibene, F.; Minetti, A.E. Biomechanical and Physiological Aspects of Legged Locomotion in Humans. Eur. J. Appl. Physiol. 2003, 88, 297–316. [Google Scholar] [CrossRef]
- Vecchiato, M.; Quinto, G.; Neunhaeuserer, D.; Battista, F.; Bettini, S.; Gasperetti, A.; Vettor, R.; Busetto, L.; Ermolao, A. The Incidence of Cardiac Arrhythmias during Exercise Stress Testing: A Focus on Patients with Severe Obesity Undergoing Sleeve Gastrectomy. Int. J. Obes. 2023, 47, 175–180. [Google Scholar] [CrossRef]
- Neunhaeuserer, D.; Gasperetti, A.; Savalla, F.; Gobbo, S.; Bullo, V.; Bergamin, M.; Foletto, M.; Vettor, R.; Zaccaria, M.; Ermolao, A. Functional Evaluation in Obese Patients Before and After Sleeve Gastrectomy. Obes. Surg. 2017, 27, 3230–3239. [Google Scholar] [CrossRef] [PubMed]
- Wilms, B.; Ernst, B.; Thurnheer, M.; Weisser, B.; Schultes, B. Differential Changes in Exercise Performance after Massive Weight Loss Induced by Bariatric Surgery. Obes. Surg. 2013, 23, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Ciangura, C.; Bouillot, J.L.; Lloret-Linares, C.; Poitou, C.; Veyrie, N.; Basdevant, A.; Oppert, J.M. Dynamics of Change in Total and Regional Body Composition after Gastric Bypass in Obese Patients. Obesity 2010, 18, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Zalesin, K.C.; Franklin, B.A.; Lillystone, M.A.; Shamoun, T.; Krause, K.R.; Chengelis, D.L.; Mucci, S.J.; Shaheen, K.W.; McCullough, P.A. Differential Loss of Fat and Lean Mass in the Morbidly Obese after Bariatric Surgery. Metab. Syndr. Relat. Disord. 2010, 8, 15–20. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Jubeau, M.; Munzinger, U.; Bizzini, M.; Agosti, F.; de Col, A.; Lafortuna, C.L.; Sartorio, A. Differences in Quadriceps Muscle Strength and Fatigue between Lean and Obese Subjects. Eur. J. Appl. Physiol. 2007, 101, 51–59. [Google Scholar] [CrossRef]
- Chen, Y.; Rennie, D.; Cormier, Y.F.; Dosman, J. Waist Circumference Is Associated with Pulmonary Function in Normal-Weight, Overweight, and Obese Subjects. Am. J. Clin. Nutr. 2007, 85, 35–39. [Google Scholar] [CrossRef]
- Browning, R.C.; Baker, E.A.; Herron, J.A.; Kram, R. Effects of Obesity and Sex on the Energetic Cost and Preferred Speed of Walking. J. Appl. Physiol. 2006, 100, 390–398. [Google Scholar] [CrossRef]
- Browning, R.C.; Kram, R. Energetic Cost and Preferred Speed of Walking in Obese vs. Normal Weight Women. Obes. Res. 2005, 13, 891–899. [Google Scholar] [CrossRef]
- Peyrot, N.; Thivel, D.; Isacco, L.; Morin, J.B.; Belli, A.; Duche, P. Why Does Walking Economy Improve after Weight Loss in Obese Adolescents? Med. Sci. Sports Exerc. 2012, 44, 659–665. [Google Scholar] [CrossRef]
- Vartiainen, P.; Bragge, T.; Lyytinen, T.; Hakkarainen, M.; Karjalainen, P.A.; Arokoski, J.P. Kinematic and Kinetic Changes in Obese Gait in Bariatric Surgery-Induced Weight Loss. J. Biomech. 2012, 45, 1769–1774. [Google Scholar] [CrossRef]
- Vecchiato, M.; Zanardo, E.; Battista, F.; Quinto, G.; Bergia, C.; Palermi, S.; Duregon, F.; Ermolao, A.; Neunhaeuserer, D. The Effect of Exercise Training on Irisin Secretion in Patients with Type 2 Diabetes: A Systematic Review. J. Clin. Med. 2022, 12, 62. [Google Scholar] [CrossRef] [PubMed]
- Santarpia, L.; Contaldo, F.; Pasanisi, F. Body Composition Changes after Weight-Loss Interventions for Overweight and Obesity. Clin. Nutr. 2013, 32, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Ortolan, S.; Neunhaeuserer, D.; Quinto, G.; Barra, B.; Centanini, A.; Battista, F.; Vecchiato, M.; de Marchi, V.; Celidoni, M.; Rebba, V.; et al. Potential Cost Savings for the Healthcare System by Physical Activity in Different Chronic Diseases: A Pilot Study in the Veneto Region of Italy. Int. J. Environ. Res. Public Health 2022, 19, 7375. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | Waist Circumference (cm) | ||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |||
| All | 44.1 ± 10.7 | 166.2 ± 9.5 | 117.9 ± 19.6 | 87.4 ± 15.8 * | 42.5 ± 4.7 | 31.6 ± 4.2 * | 127.8 ± 12.8 | 103.4 ± 13.4 * |
| All women | 44.1 ± 10.6 | 162.7 ± 6.3 | 112.0 ± 14.6 | 83.1 ± 12.1 * | 42.3 ± 4.4 | 31.4 ± 3.9 * | 124.2 ± 11.0 | 100.1 ± 9.7 * |
| All men | 44.0 ± 11.3 | 179.0 ± 8.1 | 139.3 ± 20.8 | 103.1 ± 17.6 * | 43.5 ± 5.8 | 32.3 ± 5.1 * | 138.8 ± 11.6 | 113.6 ± 17.7 * |
| Women BMI 35–40 | 45.8 ± 8.7 | 162.8 ± 5.3 | 100.2 ± 7.2 | 74.6 ± 7.9 * | 37.8 ± 1.53 | 28.2 ± 2.72 * | 115.4 ± 9.4 | 93.0 ± 7.5 * |
| Women BMI ≥ 40 | 43.3 ± 11.4 | 162.6 ± 6.8 | 117.8 ± 13.8 | 87.3 ± 11.7 * | 44.5 ± 3.5 | 33.0 ± 3.4 * | 128.1 ± 9.4 | 103.1 ± 9.0 * |
| Men BMI 35–40 | 42.0 ± 14.3 | 182 ± 7.1 | 124.3 ± 11.2 | 91.5 ± 14.4 * | 37.4 ± 1.7 | 27.6 ± 3.5 * | 127.5 ± 7.9 | 102.6 ± 15.0 * |
| Men BMI ≥ 40 | 45.0 ± 9.7 | 177.4 ± 8.3 | 146.8 ± 20.6 | 108.8 ± 16.4 * | 46.5 ± 4.5 | 34.7 ± 4.0 * | 144.8 ± 8.0 | 119.5 ± 16.4 * |
| HR Rest (bpm) | HR Max (% Predicted) | METs Max | RER Max | VO2 Rest (L/min) | VO2 Rest (mL/kg/min) | VO2 Peak (L/min) | VO2 Peak (mL/kg/min) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| All | 81.6 ± 12.8 | 64.5 ± 9.5 * | 91.1 ± 7.4 | 90.7 ± 7.4 | 1.13 ± 0.09 | 1.19 ± 0.10 * | 1.13 ± 0.09 | 1.19 ± 0.10 * | 0.42 ± 0.13 | 0.32 ± 0.11 * | 3.6 ± 0.9 | 3.7 ± 1.2 | 2.46 ± 0.58 | 2.15 ± 0.55 * | 20.8 ± 3.2 | 24.7 ± 5.2 * |
| All women | 81.8 ± 12.6 | 65.0 ± 9.1 * | 91.1 ± 7.5 | 90.5 ± 7.1 | 1.13 ± 0.10 | 1.17 ± 0.10 * | 1.13 ± 0.10 | 1.17 ± 0.10 * | 0.39 ± 0.11 | 0.30 ± 0.09 * | 3.5 ± 0.9 | 3.6 ± 1.1 | 2.24 ± 0.35 | 1.96 ± 0.36 * | 20.0 ± 2.5 | 23.8 ± 4.5 * |
| All men | 80.7 ± 13.6 | 62.3 ± 10.9 * | 90.7 ± 7.1 | 91.4 ± 8.5 | 1.14 ± 0.07 | 1.23 ± 0.10 * | 1.14 ± 0.07 | 1.23 ± 0.10 * | 0.54 ± 0.15 | 0.40 ± 0.13 * | 3.9 ± 1.1 | 3.9 ± 1.3 | 3.26 ± 0.55 | 2.84 ± 0.59 * | 23.6 ± 4.0 | 27.7 ± 6.2 * |
| Women BMI 35–40 | 80.6 ± 12.8 | 65.5 ± 9.0 * | 90.9 ± 8.9 | 90.8 ± 8.8 | 1.14 ± 0.10 | 1.17 ± 0.11 | 1.14 ± 0.10 | 1.17 ± 0.11 | 0.34 ± 0.09 | 0.29 ± 0.08 * | 3.4 ± 0.8 | 3.9 ± 1.1 | 2.08 ± 0.28 | 1.79 ± 0.30 * | 20.8 ± 2.5 | 24.2 ± 4.8 * |
| Women BMI ≥ 40 | 82.4 ± 12.5 | 64.8 ± 9.2 * | 91.3 ± 6.8 | 90.4 ± 6.2 | 1.12 ± 0.09 | 1.18 ± 0.10 * | 1.12 ± 0.09 | 1.18 ± 0.10* | 0.41 ± 0.11 | 0.30 ± 0.09 * | 3.5 ± 0.9 | 3.5 ± 1.1 | 2.31 ± 0.36 | 2.05 ± 0.36 * | 19.6 ± 2.4 | 23.7 ± 4.4 * |
| Men BMI 35–40 | 76.9 ± 18.5 | 59.0 ± 12.4 * | 89.9 ± 6.4 | 87.5 ± 9.3 | 1.13 ± 0.08 | 1.21 ± 0.13 | 1.13 ± 0.08 | 1.21 ± 0.13 | 0.56 ± 0.11 | 0.36 ± 0.14 * | 4.5 ± 1.2 | 3.9 ± 1.6 | 3.30 ± 0.64 | 2.85 ± 0.75 * | 26.6 ± 5.1 | 30.7 ± 8.6 |
| Men BMI ≥ 40 | 82.6 ± 10.4 | 64.0 ± 10.0 * | 91.1 ± 7.5 | 93.4 ± 7.5 * | 1.14 ± 0.06 | 1.25 ± 0.09 * | 1.14 ± 0.06 | 1.25 ± 0.09 * | 0.53 ± 0.15 | 0.42 ± 0.12 * | 3.6 ± 0.8 | 3.9 ± 1.1 | 3.24 ± 0.51 | 2.84 ± 0.51 * | 22.1 ± 2.2 | 26.2 ± 3.9 * |
| CPET Parameters | Net Energy Cost of Walking | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR (bpm) | RER | VO2 (L/min) | VO2 (mL/kg/min) | Absolute (J/m) | Relative (J/kg/m) | |||||||
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Stage 0 | ||||||||||||
| All | 113.3 ± 14.0 | 89.8 ± 12.2 * | 0.81 ± 0.06 | 0.80 ± 0.07 * | 1.25 ± 0.29 | 0.81 ± 0.19 * | 10.6 ± 1.8 | 9.3 ± 1.6 * | 370.21 ± 114.19 | 218.82 ± 81.78 * | 3.15 ± 0.86 | 2.50 ± 0.81 * |
| Women BMI 35–40 | 111.4 ± 13.6 | 90.5 ± 12.2 * | 0.82 ± 0.06 | 0.79 ± 0.07 | 1.04 ± 0.19 | 0.70 ± 0.15 * | 10.4 ± 2.1 | 9.5 ± 2.1 * | 312.49 ± 84.71 | 183.73 ± 75.73 * | 3.15 ± 0.94 | 2.48 ± 1.05 * |
| Women BMI ≥ 40 | 115.9 ± 13.7 | 91.2 ± 12.0 * | 0.81 ± 0.05 | 0.79 ± 0.07 * | 1.24 ± 0.24 | 0.80 ± 0.18 * | 10.5 ± 1.7 | 9.2 ± 1.4 * | 369.49 ± 109.69 | 222.04 ± 82.10 * | 3.13 ± 0.86 | 2.51 ± 0.73 * |
| Men BMI 35–40 | 105.9 ± 20.1 | 82.9 ± 12.6 * | 0.83 ± 0.13 | 0.83 ± 0.09 | 1.44 ± 0.25 | 0.92 ± 0.13 * | 11.6 ± 1.7 | 10.1 ± 1.0 * | 392.30 ± 137.75 | 252.79 ± 66.94 * | 3.16 ± 1.07 | 2.77 ± 0.66 * |
| Men BMI ≥ 40 | 111.0 ± 10.3 | 86.7 ± 11.5 * | 0.81 ± 0.05 | 0.80 ± 0.06 | 1.57 ± 0.28 | 0.99 ± 0.16 * | 10.8 ± 1.6 | 9.1 ± 1.0 * | 465.65 ± 77.74 | 253.24 ± 78.21 * | 3.19 ± 0.67 | 2.33 ± 0.62 * |
| Stage 1/2 | ||||||||||||
| All | 119.2 ± 13.7 | 95.6 ± 12.6 * | 0.85 ± 0.06 | 0.85 ± 0.07 | 1.40 ± 0.31 | 0.92 ± 0.21 * | 11.9 ± 1.8 | 10.6 ± 1.5 * | 437.32 ± 127.16 | 271.12 ± 90.18 * | 3.73 ± 0.92 | 3.09 ± 0.82 * |
| Women BMI 35–40 | 118.1 ± 13.9 | 95.6 ± 12.3 * | 0.86 ± 0.06 | 0.85 ± 0.07 | 1.18 ± 0.20 | 0.79 ± 0.13 * | 11.8 ± 2.1 | 10.6 ± 1.9 * | 377.91 ± 90.65 | 225.07 ± 73.03 * | 3.80 ± 1.01 | 3.04 ± 1.01 * |
| Women BMI ≥ 40 | 121.3 ± 13.1 | 97.1 ± 12.6 * | 0.85 ± 0.05 | 0.85 ± 0.06 | 1.36 ± 0.22 | 0.92 ± 0.20 * | 11.7 ± 1.5 | 10.5 ± 1.5 * | 424.33 ± 114.04 | 276.33 ± 90.14 * | 3.63 ± 0.90 | 3.13 ± 0.77 * |
| Men BMI 35–40 | 111.5 ± 19.6 | 88.7 ± 11.8 * | 0.87 ± 0.12 | 0.87 ± 0.09 | 1.61 ± 0.27 | 1.02 ± 0.15 * | 13.0 ± 1.7 | 11.2 ± 0.9 * | 475.39 ± 146.73 | 302.81 ± 86.61 * | 3.83 ± 1.09 | 3.31 ± 0.81 * |
| Men BMI ≥ 40 | 117.5 ± 10.9 | 93.4 ± 13.2 * | 0.86 ± 0.05 | 0.85 ± 0.06 | 1.80 ± 0.31 | 1.13 ± 0.19 * | 12.3 ± 1.6 | 10.4 ± 0.9 * | 571.96 ± 124.43 | 319.10 ± 88.45 * | 3.92 ± 0.77 | 2.92 ± 0.60 * |
| Stage 1 | ||||||||||||
| All | 128.3 ± 13.8 | 104.8 ± 13.4 * | 0.88 ± 0.06 | 0.88 ± 0.06 | 1.68 ± 0.45 | 1.12 ± 0.25 * | 14.1 ± 1.9 | 12.7 ± 1.6 * | 384.83 ± 126.92 | 241.07 ± 80.18 * | 3.26 ± 0.77 | 2.75 ± 0.58 * |
| Women BMI 35–40 | 127.0 ± 13.6 | 104.7 ± 13.3 * | 0.90 ± 0.08 | 0.87 ± 0.07 | 1.39 ± 0.22 | 0.94 ± 0.14 * | 13.9 ± 2.3 | 12.7 ± 1.9 * | 323.62 ± 68.01 | 201.27 ± 49.69 * | 3.24 ± 0.74 | 2.71 ± 0.66 * |
| Women BMI ≥ 40 | 130.5 ± 13.1 | 106.5 ± 13.4 * | 0.88 ± 0.06 | 0.87 ± 0.06 | 1.62 ± 0.26 | 1.1 ± 0.23 * | 13.8 ± 1.7 | 12.6 ± 1.8 * | 370.13 ± 79.70 | 244.04 ± 77.16 * | 3.16 ± 0.60 | 2.77 ± 0.59 * |
| Men BMI 35–40 | 116.9 ± 21.1 | 95.6 ± 12.4 * | 0.85 ± 0.06 | 0.89 ± 0.08 | 1.89 ± 0.34 | 1.19 ± 0.19 * | 15.0 ± 1.8 | 13.0 ± 0.7 * | 401.23 ± 122.01 | 256.50 ± 60.40 * | 3.19 ± 0.80 | 2.79 ± 0.42 * |
| Men BMI ≥ 40 | 127.7 ± 10.4 | 103.4 ± 13.3 * | 0.89 ± 0.05 | 0.88 ± 0.07 | 2.28 ± 0.68 | 1.38 ± 0.21 * | 14.7 ± 1.6 | 12.7 ± 0.9 * | 536.77 ± 208.60 | 294.15 ± 68.14 * | 3.64 ± 1.21 | 2.70 ± 0.44 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vecchiato, M.; Faggian, S.; Quinto, G.; Battista, F.; Foletto, M.; Di Vincenzo, A.; Bettini, S.; Gasperetti, A.; Busetto, L.; Ermolao, A.; et al. Analysis of Walking Economy after Sleeve Gastrectomy in Patients with Severe Obesity. Biology 2023, 12, 746. https://doi.org/10.3390/biology12050746
Vecchiato M, Faggian S, Quinto G, Battista F, Foletto M, Di Vincenzo A, Bettini S, Gasperetti A, Busetto L, Ermolao A, et al. Analysis of Walking Economy after Sleeve Gastrectomy in Patients with Severe Obesity. Biology. 2023; 12(5):746. https://doi.org/10.3390/biology12050746
Chicago/Turabian StyleVecchiato, Marco, Sara Faggian, Giulia Quinto, Francesca Battista, Mirto Foletto, Angelo Di Vincenzo, Silvia Bettini, Andrea Gasperetti, Luca Busetto, Andrea Ermolao, and et al. 2023. "Analysis of Walking Economy after Sleeve Gastrectomy in Patients with Severe Obesity" Biology 12, no. 5: 746. https://doi.org/10.3390/biology12050746