


Effects of Inspiratory Muscle Warm-Up on Physical Exercise: A Systematic Review

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Data Sources and Search Strategy
2.3. Quality Assessment
2.4. Risk of Bias Assessment
2.5. Data Extraction and Management
3. Results
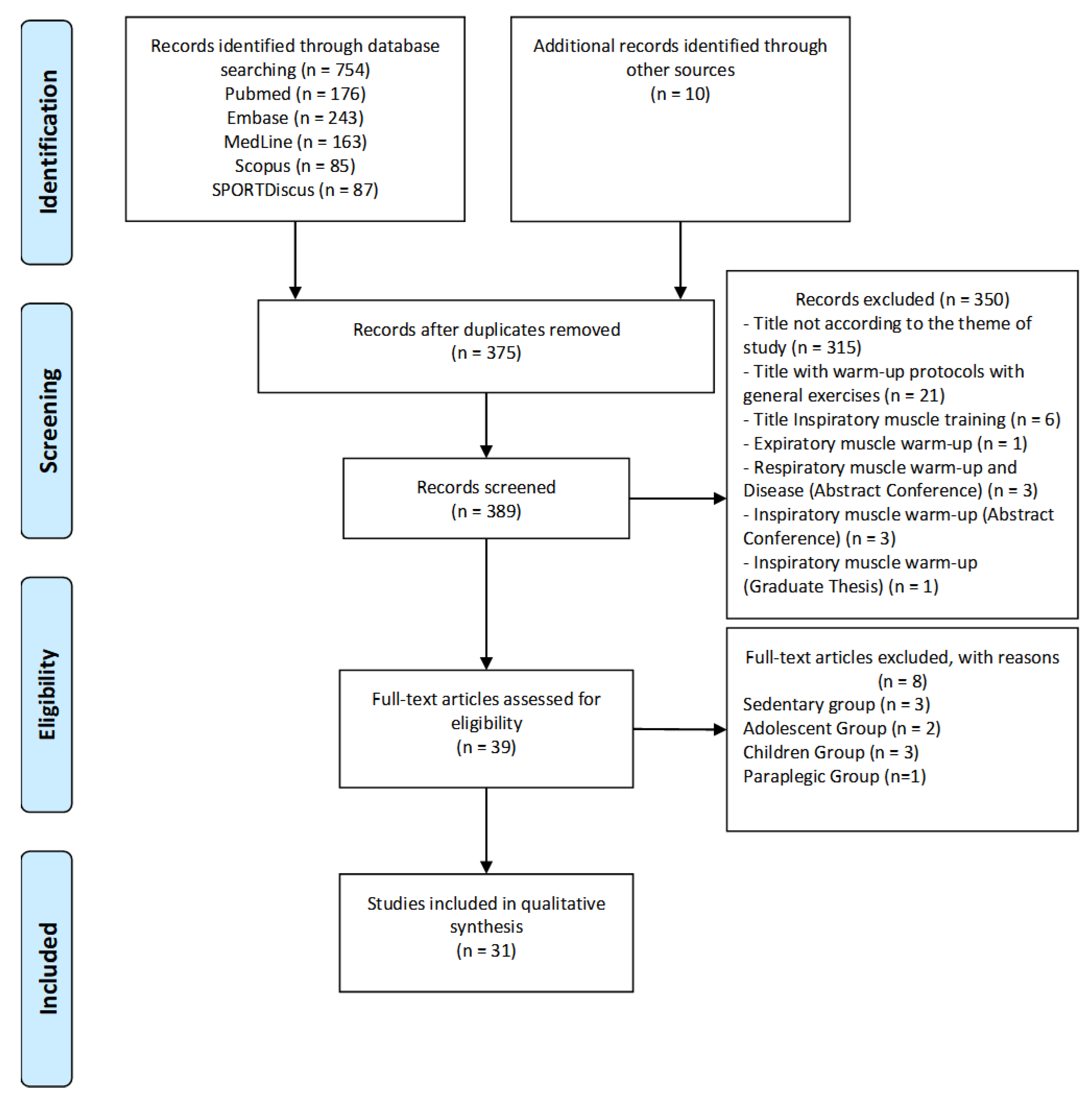
3.1. Study Selection
3.2. Quality Assessment
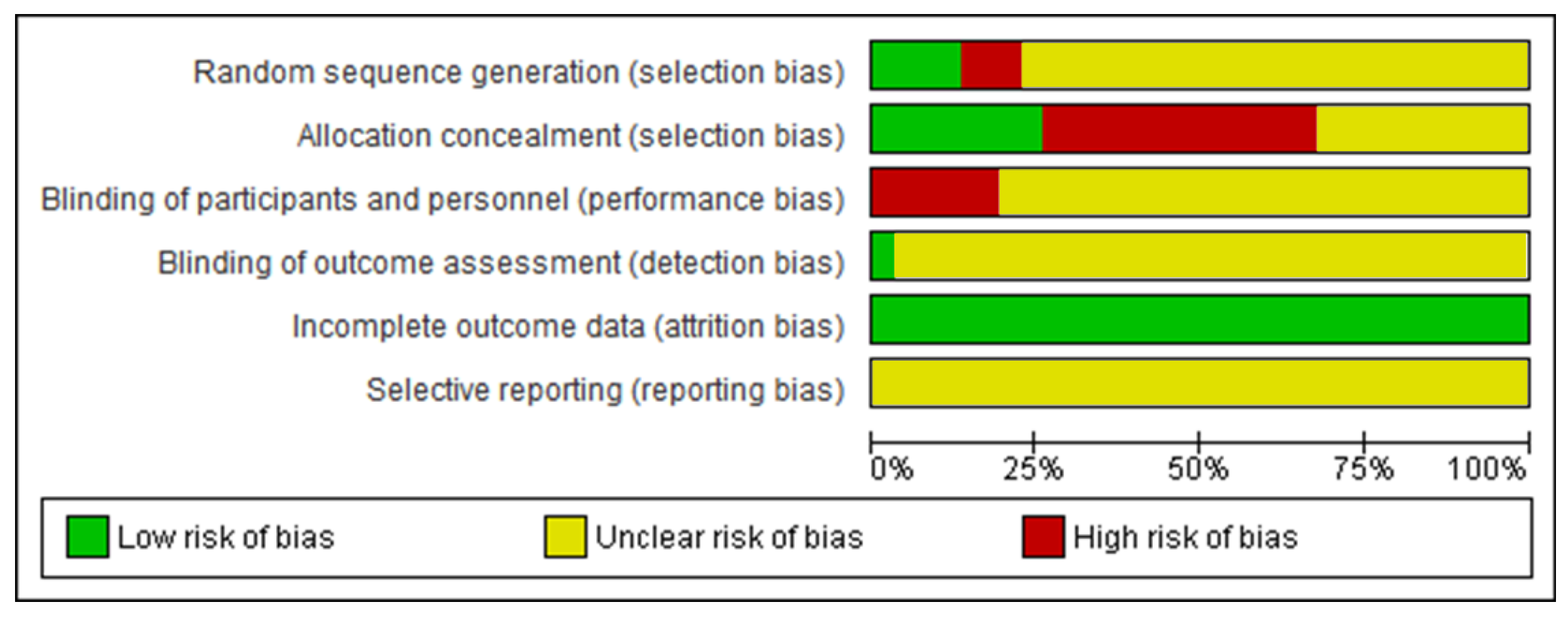
3.3. Risk-of-Bias Assessment
3.4. Study Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forster, H.V.; Haouzi, P.; Dempsey, J.A. Control of Breathing During Exercise. Compr. Physiol. 2012, 2, 743–777. [Google Scholar] [CrossRef]
- Welch, J.F.; Kipp, S.; Sheel, A.W. Respiratory muscles during exercise: Mechanics, energetics, and fatigue. Curr. Opin. Physiol. 2019, 10, 102–109. [Google Scholar] [CrossRef]
- Aaron, E.A.; Seow, K.C.; Johnson, B.D.; Dempsey, J.A. Oxygen cost of exercise hyperpnea: Implications for performance. J. Appl. Physiol. 1992, 72, 1818–1825. [Google Scholar] [CrossRef]
- Harms, C.A.; Wetter, T.J.; McClaran, S.R.; Pegelow, D.F.; Nickele, G.A.; Nelson, W.B.; Hanson, P.; Dempsey, J.A. Effects of respiratory muscle work on cardiac output and its distribution during maximal exercise. J. Appl. Physiol. 1998, 85, 609–618. [Google Scholar] [CrossRef]
- Ratnovsky, A.; Elad, D.; Halpern, P. Mechanics of respiratory muscles. Respir. Physiol. Neurobiol. 2008, 163, 82–89. [Google Scholar] [CrossRef]
- Hudson, A.L.; Butler, J.E.; Gandevia, S.C.; De Troyer, A. Interplay Between the Inspiratory and Postural Functions of the Human Parasternal Intercostal Muscles. J. Neurophysiol. 2010, 103, 1622–1629. [Google Scholar] [CrossRef] [Green Version]
- Saillant, N.N. Chest Wall Anatomy. In Rib Fracture Management; Moya, M., Mayberry, J., Eds.; Springer: Cham, Switzerland, 2018; pp. 25–33. [Google Scholar]
- Lorca-Santiago, J.; Jiménez, S.L.; Pareja-Galeano, H.; Lorenzo, A. Inspiratory Muscle Training in Intermittent Sports Modalities: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4448. [Google Scholar] [CrossRef]
- Silva, C.D.; Abreu, R.M.; Rehder-Santos, P.; De Noronha, M.; Catai, A.M. Can respiratory muscle training change the blood pressure levels in hypertension? A systematic review with meta-analysis. Scand. J. Med. Sci. Sports 2021, 31, 1384–1394. [Google Scholar] [CrossRef]
- Newall, C.; Stockley, R.A.; Hill, S.L. Exercise training and inspiratory muscle training in patients with bronchiectasis. Thorax 2005, 60, 943–948. [Google Scholar] [CrossRef] [Green Version]
- Dall’Ago, P.; Chiappa, G.R.S.; Guths, H.; Stein, R.; Ribeiro, J.P. Inspiratory Muscle Training in Patients With Heart Failure and Inspiratory Muscle Weakness: A Randomized Trial. J. Am. Coll. Cardiol. 2006, 47, 757–763. [Google Scholar] [CrossRef] [Green Version]
- Palermo, A.E.; Cahalin, L.P.; Nash, M.S. A case for inspiratory muscle training in SCI: Potential role as a preventative tool in infectious respiratory diseases like COVID-19. Spinal Cord Ser. Cases 2020, 6, 87. [Google Scholar] [CrossRef]
- Witt, J.D.; Guenette, J.A.; Rupert, J.L.; McKenzie, D.C.; Sheel, A.W. Inspiratory muscle training attenuates the human respiratory muscle metaboreflex. J. Physiol. 2007, 584, 1019–1028. [Google Scholar] [CrossRef]
- Klusiewicz, A.; Borkowski, L.; Zdanowicz, R.; Boros, P.; Wesołowski, S. The inspiratory muscle training in elite rowers. J. Sports Med. Phys. Fit. 2008, 48, 279–284. [Google Scholar]
- Tong, T.K.; Fu, F.H.; Chung, P.K.; Eston, R.; Lu, K.; Quach, B.; Nie, J.; So, R. The effect of inspiratory muscle training on high-intensity, intermittent running performance to exhaustion. Appl. Physiol. Nutr. Metab. 2008, 33, 671–681. [Google Scholar] [CrossRef]
- Karsten, M.; Ribeiro, G.S.; Esquivel, M.S.; Matte, D.L. The effects of inspiratory muscle training with linear workload devices on the sports performance and cardiopulmonary function of athletes: A systematic review and meta-analysis. Phys. Ther. Sport 2018, 34, 92–104. [Google Scholar] [CrossRef]
- Caruso, F.R.; Archiza, B.; Andaku, D.K.; Trimer, R.; Bonjorno-Junior, J.C.; de Oliveira, C.R.; Libardi, C.A.; Phillips, S.A.; Arena, R.; Mendes, R.G.; et al. Effects of acute inspiratory loading during treadmill running on cerebral, locomotor and respiratory muscle oxygenation in women soccer players. Respir. Physiol. Neurobiol. 2020, 281, 103488. [Google Scholar] [CrossRef]
- Tanriverdi, A.; Kahraman, B.O.; Ozsoy, I.; Ozpelit, E.; Savci, S. Acute effects of inspiratory muscle training at different intensities in healthy young people. Ir. J. Med. Sci. 2020, 190, 577–585. [Google Scholar] [CrossRef]
- Cheng, C.-F.; Hsu, W.-C.; Kuo, Y.-H.; Chen, T.-W. Acute effect of inspiratory resistive loading on sprint interval exercise performance in team-sport athletes. Respir. Physiol. Neurobiol. 2020, 282, 103531. [Google Scholar] [CrossRef]
- Lin, H.; Tong, T.K.; Huang, C.; Nie, J.; Lu, K.; Quach, B. Specific inspiratory muscle warm-up enhances badminton footwork performance. Appl. Physiol. Nutr. Metab. 2007, 32, 1082–1088. [Google Scholar] [CrossRef]
- Cheng, C.-F.; Tong, T.K.; Kuo, Y.-C.; Chen, P.-H.; Huang, H.-W.; Lee, C.-L. Inspiratory muscle warm-up attenuates muscle deoxygenation during cycling exercise in women athletes. Respir. Physiol. Neurobiol. 2013, 186, 296–302. [Google Scholar] [CrossRef]
- Wilson, E.; McKeever, T.; Lobb, C.; Sherriff, T.; Gupta, L.; Hearson, G.; Martin, N.; Lindley, M.; Shaw, D. Respiratory muscle specific warm-up and elite swimming performance. Br. J. Sports Med. 2014, 48, 789–791. [Google Scholar] [CrossRef]
- Özdal, M.; Bostanci, Ö.; Dağlioğlu, Ö.; Ağaoğlu, S.A.; Kabadayi, M. Effect of respiratory warm-up on anaerobic power. J. Phys. Ther. Sci. 2016, 28, 2097–2098. [Google Scholar] [CrossRef] [Green Version]
- Barnes, K.R.; Ludge, A.R. Inspiratory Muscle Warm-up Improves 3200-m Running Performance in Distance Runners. J. Strength Cond. Res. 2021, 35, 1739–1747. [Google Scholar] [CrossRef]
- Bishop, D. Warm up II: Performance Changes Following Active Warm Up and How to Structure the Warm Up. Sports Med. 2003, 33, 483–498. [Google Scholar] [CrossRef]
- Hamada, T.; Sale, D.G.; MacDougall, J.D.; Tarnopolsky, M.A. Postactivation potentiation, fiber type, and twitch contraction time in human knee extensor muscles. J. Appl. Physiol. 2000, 88, 2131–2137. [Google Scholar] [CrossRef]
- Dallas, G.; Mavvidis, A.; Kosmathaki, I.; Tsoumani, I. The post activation potentiation effect of two different conditioning stimuli on drop jump parameters on young female artistic gymnasts. Sci. Gymnastics J. 2019, 11, 103–113. [Google Scholar] [CrossRef]
- Volianitis, S.; McConnell, A.K.; Koutedakis, Y.; Jones, D.A. The Influence of Prior Activity Upon Inspiratory Muscle Strength in Rowers and Non-Rowers. Int. J. Sports Med. 1999, 20, 542–547. [Google Scholar] [CrossRef]
- Volianitis, S.; McConnell, A.; Koutedakis, Y.; Jones, D.A. Specific respiratory warm-up improves rowing performance and exertional dyspnea. Med. Sci. Sports Exerc. 2001, 33, 1189–1193. [Google Scholar] [CrossRef] [Green Version]
- Lomax, M.; McConnell, A. Influence of Prior Activity (Warm-Up) and Inspiratory Muscle Training upon Between- and Within-Day Reliability of Maximal Inspiratory Pressure Measurement. Respiration 2009, 78, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Lomax, M.; Grant, I.; Corbett, J. Inspiratory muscle warm-up and inspiratory muscle training: Separate and combined effects on intermittent running to exhaustion. J. Sports Sci. 2011, 29, 563–569. [Google Scholar] [CrossRef]
- Ohya, T.; Hagiwara, M.; Suzuki, Y. Inspiratory muscle warm-up has no impact on performance or locomotor muscle oxygenation during high-intensity intermittent sprint cycling exercise. Springerplus 2015, 4, 556. [Google Scholar] [CrossRef] [Green Version]
- Arend, M.; Kivastik, J.; Mäestu, J. Maximal inspiratory pressure is influenced by intensity of the warm-up protocol. Respir. Physiol. Neurobiol. 2016, 230, 11–15. [Google Scholar] [CrossRef]
- Johnson, M.A.; Gregson, I.R.; Mills, D.E.; Gonzalez, J.T.; Sharpe, G.R. Inspiratory muscle warm-up does not improve cycling time-trial performance. Eur. J. Appl. Physiol. 2014, 114, 1821–1830. [Google Scholar] [CrossRef] [Green Version]
- Arend, M.; Mäestu, J.; Kivastik, J.; Rämson, R.; Jürimäe, J. Effect of Inspiratory Muscle Warm-up on Submaximal Rowing Performance. J. Strength Cond. Res. 2015, 29, 213–218. [Google Scholar] [CrossRef]
- Cirino, C.; Gobatto, C.A.; Pinto, A.S.; Torres, R.S.; Hartz, C.S.; Azevedo, P.H.S.M.; Moreno, M.A.; Manchado-Gobatto, F.B. Complex network model indicates a positive effect of inspiratory muscles pre-activation on performance parameters in a judo match. Sci. Rep. 2021, 11, 11148. [Google Scholar] [CrossRef]
- Manchado-Gobatto, F.B.; Torres, R.S.; Marostegan, A.B.; Rasteiro, F.M.; Hartz, C.S.; Moreno, M.A.; Pinto, A.S.; Gobatto, C.A. Complex Network Model Reveals the Impact of Inspiratory Muscle Pre-Activation on Interactions among Physiological Responses and Muscle Oxygenation during Running and Passive Recovery. Biology 2022, 11, 963. [Google Scholar] [CrossRef]
- Marostegan, A.B.; Gobatto, C.A.; Rasteiro, F.M.; Hartz, C.S.; Moreno, M.A.; Manchado-Gobatto, F.B. Effects of different inspiratory muscle warm-up loads on mechanical, physiological and muscle oxygenation responses during high-intensity running and recovery. Sci. Rep. 2022, 12, 11223. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Chichester, UK, 2018. [Google Scholar]
- Volianitis, S.; McConnell, A.K.; Jones, D.A. Assessment of Maximum Inspiratory Pressure. Respiration 2001, 68, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Tong, T.K.; Fu, F.H. Effect of specific inspiratory muscle warm-up on intense intermittent run to exhaustion. Eur. J. Appl. Physiol. 2006, 97, 673–680. [Google Scholar] [CrossRef]
- Hawkes, E.Z.; Nowicky, A.; McConnell, A. Diaphragm and intercostal surface EMG and muscle performance after acute inspiratory muscle loading. Respir. Physiol. Neurobiol. 2007, 155, 213–219. [Google Scholar] [CrossRef]
- Thurston, T.S.; Coburn, J.W.; Brown, L.E.; Bartolini, A.; Beaudette, T.L.; Karg, P.; McLeland, K.A.; Arevalo, J.A.; Judelson, D.A.; Galpin, A.J. Effects of Respiratory Muscle Warm-up on High-Intensity Exercise Performance. Sports 2015, 3, 312–324. [Google Scholar] [CrossRef] [Green Version]
- Özdal, M. Acute effects of inspiratory muscle warm-up on pulmonary function in healthy subjects. Respir. Physiol. Neurobiol. 2016, 227, 23–26. [Google Scholar] [CrossRef]
- Faghy, M.A.; Brown, P.I. Whole-body active warm-up and inspiratory muscle warm-up do not improve running performance when carrying thoracic loads. Appl. Physiol. Nutr. Metab. 2017, 42, 810–815. [Google Scholar] [CrossRef] [Green Version]
- Hartz, C.S.; Ferreira, C.R.; Moreno, M.A. Effects of the Application of an Inspiratory Muscular Warm-Up Protocol in the Physical Performance of Handball Athletes. J. Exerc. Physiol. 2017, 20, 12–22. [Google Scholar]
- Özdal, M.; Bostanci, Ö. Influence of inspiratory muscle warm-up on aerobic performance during incremental exercise. Isokinet. Exerc. Sci. 2018, 26, 167–173. [Google Scholar] [CrossRef]
- Richard, P.; Billaut, F. Combining Chronic Ischemic Preconditioning and Inspiratory Muscle Warm-Up to Enhance On-Ice Time-Trial Performance in Elite Speed Skaters. Front. Physiol. 2018, 9, 1036. [Google Scholar] [CrossRef] [Green Version]
- Merola, P.K.; Zaccani, W.A.; Faria, C.C.; Berton, D.C.; Verges, S.; Franchini, E. High load inspiratory muscle warm-up has no impact on Special Judo Fitness Test performance. Ido Mov. Cult. 2019, 19, 66–74. [Google Scholar] [CrossRef]
- Richard, P.; Billaut, F. Effects of inspiratory muscle warm-up on locomotor muscle oxygenation in elite speed skaters during 3000 m time trials. Eur. J. Appl. Physiol. 2018, 119, 191–200. [Google Scholar] [CrossRef]
- Tong, T.K.; Baker, J.S.; Zhang, H.; Kong, Z.; Nie, J. Effects of Specific Core Re-Warm-Ups on Core Function, Leg Perfusion and Second-Half Team Sport-Specific Sprint Performance: A Randomized Crossover Study. J. Sports Sci. Med. 2019, 18, 479–489. [Google Scholar]
- Avci, N.; Özdal, M.; Vural, M. Influence of inspiratory muscle warm-up exercise on field hockey drag-flick and shooting performance. Eur. J. Phys. Educ. Sport Sci. 2021, 6, 92–104. [Google Scholar] [CrossRef]
- Arend, M.; Kivastik, J.; Talts, J.; Mäestu, J. The Effect of Inspiratory Muscle Warm-Up on VO2 Kinetics during Submaximal Rowing. Sports 2021, 9, 42. [Google Scholar] [CrossRef]
- Silapabanleng, S.; Boonkobkaew, N.; Singthongyam, T.; Phangjaem, M.; Puengtanom, V.; Nakpanom, W.; Suwondit, P. Effect of Inspiratory Muscle Warm-Up on Short-Distance Cycling Performance. Sci. Technol. Asia 2021, 26, 221–228. [Google Scholar]
- Bardou, P.; Mariette, J.; Escudié, F.; Djemiel, C.; Klopp, C. jvenn: An interactive Venn diagram viewer. BMC Bioinf. 2014, 15, 293. [Google Scholar] [CrossRef] [Green Version]
- McCool, F.D.; Conomos, P.; Benditt, J.O.; Cohn, D.; Sherman, C.B.; Hoppin, F.G. Maximal inspiratory pressures and dimensions of the diaphragm. Am. J. Respir. Crit. Care Med. 1997, 155, 1329–1334. [Google Scholar] [CrossRef]
- Silva, P.E.; Chiappa, G.R.; Vieira, P.J.C.; Roncada, C. Avaliação da função muscular ventilatória. In PROFISIO Programa de Atualização em Fisioterapia Cardiovascular e Respiratória: Ciclo 2; Martins, J.A., Karsten, M., Dal Corso, S., Associação Brasileira de Fisioterapia Cardiorrespiratória e Fisioterapia em Terapia Intensiva, Eds.; Artmed Panamericana: Porto Alegre, BR, 2016; pp. 9–46. (In Portuguese) [Google Scholar]
- Caruso, P.; Albuquerque, A.L.P.; Santana, P.V.; Cardenas, L.Z.; Ferreira, J.G.; Prina, E.; Trevizan, P.F.; Pereira, M.C.; Iamonti, V.; Pletsch, R.; et al. Métodos diagnósticos para avaliação da força muscular inspiratória e expiratória. J. Bras. Pneumol. 2015, 41, 110–123. [Google Scholar] [CrossRef]
- De Troyer, A.; Estenne, M. Limitations of measurement of transdiaphragmatic pressure in detecting diaphragmatic weakness. Thorax 1981, 36, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Areias, G.D.S.; Santiago, L.R.; Teixeira, D.S.; Reis, M.S. Concurrent Validity of the Static and Dynamic Measures of Inspiratory Muscle Strength: Comparison between Maximal Inspiratory Pressure and S-Index. Rev. Bras. Cir. Cardiovasc. 2020, 35, 459–464. [Google Scholar] [CrossRef]
- Neder, J.; Andreoni, S.; Lerario, M.; Nery, L. Reference values for lung function tests: II. Maximal respiratory pressures and voluntary ventilation. Braz. J. Med. Biol. Res. 1999, 32, 719–727. [Google Scholar] [CrossRef]
- Minahan, C.; Sheehan, B.; Doutreband, R.; Kirkwood, T.; Reeves, D.; Cross, T. Repeated-sprint cycling does not induce respiratory muscle fatigue in active adults: Measurements from the powerbreathe® inspiratory muscle trainer. J. Sports Sci. Med. 2015, 14, 233–238. [Google Scholar]
- Silva, P.E.; De Carvalho, K.L.; Frazão, M.; Maldaner, V.; Daniel, C.R.; Gomes-Neto, M. Assessment of Maximum Dynamic Inspiratory Pressure. Respir. Care 2018, 63, 1231–1238. [Google Scholar] [CrossRef]
- Roussos, C.S.; Macklem, P.T. Diaphragmatic fatigue in man. J. Appl. Physiol. 1977, 43, 189–197. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Babault, N. Post-activation potentiation (PAP) versus post-activation performance enhancement (PAPE) in humans: Historical perspective, underlying mechanisms, and current issues. Front. Physiol. 2019, 10, 1359. [Google Scholar] [CrossRef] [Green Version]
- McConnell, A.K.; Romer, L.M. Respiratory Muscle Training in Healthy Humans: Resolving the Controversy. Int. J. Sports Med. 2004, 25, 284–293. [Google Scholar] [CrossRef] [Green Version]
- McDonald, T.; Stiller, K. Inspiratory muscle training is feasible and safe for patients with acute spinal cord injury. J. Spinal Cord Med. 2018, 42, 220–227. [Google Scholar] [CrossRef]
- Hodges, P.W.; Heijnen, I.; Gandevia, S.C. Postural activity of the diaphragm is reduced in humans when respiratory demand increases. J. Physiol. 2001, 537, 999–1008. [Google Scholar] [CrossRef]
- Kolar, P.; Sulc, J.; Kyncl, M.; Sanda, J.; Neuwirth, J.; Bokarius, A.V.; Kriz, J.; Kobesova, A. Stabilizing function of the diaphragm: Dynamic MRI and synchronized spirometric assessment. J. Appl. Physiol. 2010, 109, 1064–1071. [Google Scholar] [CrossRef] [Green Version]
- Fogarty, M.J.; Mantilla, C.B.; Sieck, G.C. Breathing: Motor Control of Diaphragm Muscle. Physiology 2018, 33, 113–126. [Google Scholar] [CrossRef]
- Mantilla, C.B.; Seven, Y.B.; Sieck, G.C. Convergence of Pattern Generator Outputs on a Common Mechanism of Diaphragm Motor Unit Recruitment. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2014; pp. 309–329. [Google Scholar] [CrossRef] [Green Version]
- Croix, C.M.S.; Morgan, B.J.; Wetter, T.J.; Dempsey, J.A. Fatiguing inspiratory muscle work causes reflex sympathetic activation in humans. J. Physiol. 2000, 529, 493–504. [Google Scholar] [CrossRef]
- Hill, J.M. Discharge of group IV phrenic afferent fibers increases during diaphragmatic fatigue. Brain Res. 2000, 856, 240–244. [Google Scholar] [CrossRef]
- Dempsey, J.A.; Romer, L.; Rodman, J.; Miller, J.; Smith, C. Consequences of exercise-induced respiratory muscle work. Respir. Physiol. Neurobiol. 2006, 151, 242–250. [Google Scholar] [CrossRef]
- Luce, J.M.; Culver, B.H. Respiratory Muscle Function in Health and Disease. Chest 1982, 81, 82–90. [Google Scholar] [CrossRef] [Green Version]
- Green, M.; Moxham, J. The respiratory muscles. Clin. Sci. 1985, 68, 1–10. [Google Scholar] [CrossRef]
- Sieck, G.C.; Gransee, H.M. Respiratory Muscles: Structure, Function, and Regulation. In Colloquium Series on Integrated Systems Physiology: From Molecule to Function to Disease; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2012; pp. 1–96. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Intervention | Comparison | Outcome | Study Design |
|---|---|---|---|---|
| Athletes and healthy and active adults | Inspiratory-muscle warm-up | Experimental condition X Control and/or placebo | Parameters associated with the physical exercise * | Randomized studies |
| Authors (Year) | Items | Total | Quality | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Volianitis et al. (1999) [28] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | G |
| Volianitis et al. (2001) [42] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Volianitis et al. (2001) [29] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | G |
| Tong and Fu (2006) [43] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Hawkes et al. (2007) [44] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | G |
| Lin et al. (2007) [20] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Lomax and McConnell (2009) [30] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Lomax et al. (2011) [31] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Cheng et al. (2013) [21] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Johnson et al. (2014) [34] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Wilson et al. (2014) [22] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Arend et al. (2015) [35] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Ohya et al. (2015) [32] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Thurston et al. (2015) [45] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Arend et al. (2016) [33] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Ozdal (2016) [46] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Ozdal et al. (2016) [23] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Faghy and Brown (2017) [47] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Hartz et al. (2017) [48] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Ozdal and Bostanci (2018) [49] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Richard and Billaut (2018) [50] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Merola et al. (2019) [51] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Richard and Billaut (2019) [52] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Tong et al. (2019) [53] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Avci et al. (2021) [54] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Arend et al. (2021) [55] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Barnes and Ludge (2021) [24] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Cirino et al. (2021) [36] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | E |
| Silapabanleng et al. (2021) [56] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Manchado-Gobatto et al. (2022) [37] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Marostegan et al. (2022) [38] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | G |
| Authors (Year) | Subjects | IMW Protocol | Physical Exercise | Results | |
|---|---|---|---|---|---|
| Population | Age (Years) | ||||
| a Volianitis et al. (1999) [28] | 23 subjects 12 non-rowers 11 rowers | 20 ± 1 20 ± 2 | Control: without IMW IMW: 2 × 30 (40% MIP) | MIP assessment | ↑ MIP |
| a Volianitis et al. (2001) [42] | 14 healthy subjects | 26 ± 3 | Control: without IMW IMW: 2 × 30 (40% MIP) (2 min before physical exercise) | Repeated measurement of MIP(after each series) | ↓ “Learning effect” between repeated measurements of MIP |
| a Volianitis et al. (2001) [29] | 14 competitive club rowers 7 Male 7 Female | 19.9 ± 0.7 20.1 ± 0.9 | Control: without IMW IMW: 2 × 30 (40% MIP) | MIP assessment 6-min all-out rowing | <MIP decrease (%) in the post-test ↑ Power (W) ↑ Distance (m) ↓ Dyspnea |
| a Tong and Fu (2006) [43] | 10 healthy male subjects | 21.3 ± 1.2 | Control: without IMW Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) IMW performed between specific warm-up activities Physical exercise performed immediately after specific warm-up activities and IMW | Dynamic inspiratory-muscle-function Ttest Yo-Yo intermittent-recovery test | ↑ MIP at zero flow ↑ Maximal inspiratory-muscle power ↑ Optimal pressure ↑ Maximal inspiratory flow↑ Maximal rate of pressure development ↓ Dyspnea No changes in performance parameters |
| a Hawkes et al. (2007) [44] | 12 healthy subjects (6 male) | 25 ± 9 | Control: without IMW IMW: 2 × 30 (40% MIP) | MIP assessment | ↑ MIP ↑ EMG activity of the diaphragm and intercostal muscles on the MIP assessment |
| a Lin et al. (2007) [20] | 10 male badminton players | 23 ± 2 | Control: without IMW Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) | Dynamic inspiratory-muscle-function test Maximum incremental badminton-footwork test | ↑ MIP at zero flow ↑ Maximal rate of pressure development ↑ Distance (m) ↓ Dyspnea ↓ [Lac] (ISO trial) |
| a Lomax and McConnell (2009) [30] | 8 healthy and active subjects (7 females and 1 male) | 29.1± 6.3 | Control: without IMW IMW: 2 × 30 (40% MIP) (60 s pause) | MIP assessment | ↑ MIP |
| b Lomax et al. (2011) [31] | 12 healthy and semi-professional male football players | 24.6 ± 1.3 | Control: without IMW IMW: 2 × 30 (40% MIP) (60 s pause) (3 min before physical exercise) | MIP assessment Yo-Yo intermittent-recovery test | ↑ MIP ↑ Distance (m) No changes in respiratory parameters |
| a Cheng et al. (2013) [21] | 10 female soccer players | 19.9 ± 1.4 | Control: without IMW Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) | 2 sets of 6-min cycling exercises 6 × 10 s sprints | No changes in performance, metabolic or respiratory parameters, except ↓ ∆ TSI |
| a Johnson et al. (2014) [34] | 10 trained competitive road cyclists | 32 ± 9 | 1: Without any preliminary activity 2: Control without IMW 3: IMW-2 × 30 (40% MIP) (30s pause) | 10-kilometer-cycling time-trial tests | No changes in performance, metabolic or respiratory parameters |
| a Wilson et al. (2014) [22] | 15 elite swimmers (9 male) | 21.2 ± 1.6 | 1: Control without IMW 2: Only IMW-2 × 30 (40% MIP) 3: IMW-2 × 30 (15% MIP) 4: IMW-2 × 30 (40% MIP) | 100-m freestyle-sprint time trial | ↓ Time No changes in metabolic or respiratory parameters |
| a Arend et al. (2015) [35] | 10 competitive male rowers | 23.1 ± 3.8 | Control: Without IMW IMW: 2 × 30 (40% MIP) (2 min pause) | Submaximal-intensity rowing test (90% VO2 max) | No changes in performance, metabolic or respiratory parameters, except ↓ breathing frequency |
| a Ohya et al. (2015) [32] | 10 healthy and active male subjects | 25.1 ± 4.8 | Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) (60 s pause) | 5 × 5-s cycling sprints (25-s active recovery) | ↑ MIP post-IMW No changes in performance, metabolic or respiratory parameters |
| c Thurston et al. (2015) [45] | 11 recreationally active male subjects | 24.9 ± 4.2 | Airflow restriction Control: Without IMW Low: 2 × 30 (13-millimeter opening) Medium: 2 × 30 (8-millimeter opening) High: 2 × 30 (3-millimeter opening) (60 s pause) | Cycling test to exhaustion (85% VO2max) Pulmonary-function testing (spirometry) | No changes in performance, metabolic or respiratory parameters |
| a Arend et al. (2016) [33] | 10 healthy male subjects | 26.4 ± 4.1 | Control: Without IMW 1: IMW—2 × 30 (15% MIP) 2: IMW–2 × 30 (40% MIP) 3: IMW—2 × 12 (60% MIP) 4: IMW—2 × 6 (80% MIP) (5 min before physical exercise) | MIP assessment | ↑ MIP (IMW at 40 and 60% MIP) |
| a Ozdal (2016) [46] | 26 healthy male subjects | 26.31 ± 4.39 | Control: Without IMW Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) | MIP assessment Pulmonary-function testing (spirometry) | ↑ MIP ↑ Pulmonary function |
| a Ozdal et al. (2016) [23] | 30 field hockey players | 20.5 ± 2.0 | Control: Without IMW IMW: 2 × 30 (40% MIP) (2 min pause) | Wingate test | ↑ Performance parameters |
| a Faghy and Brown (2017) [47] | 9 healthy and active male subjects | 26.4 ± 9.1 | 1: Control without IMW 2: Only IMW 2 × 30 (40% MIP) 3: Only placebo (5-min breathing using a sham device) 4: IMW 2 × 30 (40% MIP) 5: Placebo (5-min breathing using a sham device) | 2.4-kilometer-running timetrials (25-kilogram thoracic load) MIP Assessment | ↓ MIP post physical exercise (no difference among protocols)No changes in performance, metabolic or respiratory parameters |
| a Hartz et al. (2017) [48] | 14 female handball athletes | 19 ± 1 | Control: Without IMW Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) | Yo-Yo endurance test | No changes in performance, metabolic or respiratory parameters |
| a Ozdal & Bostanci (2018) [49] | 30 male elite field hockey players | 20.50 ± 1.98 | Baseline: MIP/MEP values Control: Without IMW IMW: 2 × 30 (40% MIP) (2-min pause) | MIP/MEP assessment Incremental test with cycle ergometer (VO2 peak) | ↑ MIP/MEP (comparison with baseline) ↑ Respiratory parameters |
| a Richard and Billaut (2018) [50] | 7 elite male long-track speed skaters | 23.4 ± 3.3 | Protocols combined with chronic ischemic preconditioning Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) (60-s pause) | 600-m ice-skating time-trials | No changes in performance or respiratory parameters |
| a Merola et al. (2019) [51] | 11 judo athletes | 22.3 ± 2.3 | Control: Without IMW Placebo: 2 × 15 (15% MIP) IMW: 2 × 15 (60% MIP) (with one breath immediately after each movement during specific warm-up activities) | Special judo fitness test MIP and MEP assessment | No changes in inspiratory, performance or respiratory parameters |
| a Richard and Billaut (2019) [52] | 8 elite speed skaters (5 Male) | 21.4 ± 3.5 | Placebo: 2 × 30 (15% MIP) IMW: 2 × 30 (40% MIP) (60 s pause) | 3000-m ice-skating time-trials | No changes in performance or respiratory parameters |
| a Tong et al. (2019) [53] | 9 male college athletes (soccer and handball) | 20.6 ± 0.9 | Control: Without any preliminary activity IMW: 40% MIP (IMW was performed simultaneously with four exercises for the trunk musculature) Interventions were performed between exercises on the treadmill | 2 × intermittent efforts on a non-motorized treadmill at progressive speeds up to all-out speed (15-min pause) MIP assessment Sport-specific-endurance plank test (trunk-muscles strength) | Accelerated recovery of MIP and trunk-muscle strength ↑ Performance parameters (sprints) No changes in metabolic or respiratory parameters in the recovery period |
| d Avci et al. (2021) [54] | 30 male hockey players | 21.50 ± 2.98 | Control: Without IMW Placebo: 2 × 30 (5% MIP) IMW: 2 × 30 (40% MIP) (60-s pause) | Hockey Tests: Hockey drag-flick and shot-performance test Goal and scoring Drag-flick-performance test Hit-performance test | ↑ Drag-flick and shooting performance |
| a Arend et al. (2021) [55] | 10 high-level male rowers | 23.1 ± 3.8 | Control: Without IMW IMW: 2 × 30 (40% MIP) (2-min pause) | Submaximal-intensity rowing test (90% VO2max) | No changes in performance or respiratory parameters (VO2 kinetics) |
| a Barnes and Ludge (2021) [24] | 17 middle-distance runners: 10 Male 7 Female | 20.3 ± 1.5 20.2 ± 1.3 | Control: 1 × 30 (30 slow protracted breaths against 3 cm of H20 resistance) IMW: 1 × 30 (50% S-index) | Inspiratory-muscle-function test (S-index) 3200-m-run-performance trial | ↑ Performance parameters ↑ S-index No changes in respiratory parameters, except ↓ Dyspnea |
| a Cirino et al. (2021) [36] | 10 male judo athletes | 22 ± 1 | Control: Without IMW Placebo: 2 × 15 (15% MIP) IMW: 2 × 15 (40% MIP) (60-s pause) (2 min before physical exercise) | Judo match—4 min Recovery post-combat | ↑ Technical-tactical parameters No changes in metabolic or respiratory parameters in the recovery period |
| a Silapabanleng et al. (2021) [56] | 26 healthy males subjects | 19–23 | Control: Without IMW IMW: 2 × 30 (40% S-index) Physical exercise performed immediately after IMW | 3-min all-out test in cycle ergometer | ↓ Heart rate at the third minute of the test No changes in performance parameters or rate of perceived exertion (RPE) |
| a Manchado-Gobatto et al. (2022) [37] | 15 physically active young men | 23 ± 1 | Control: Without IMW IMW: 2 × 15 (40% MIP) (60-s pause) (2 min before the physical exercise) | 30-s all-out tethered running on a non-motorized treadmill Recovery post-test | ↑ Absolute (W) and relative power (W.kg−1) No changes in metabolic or respiratory parameters at rest or in the recovery period |
| a Marostegan et al. (2022) [38] | 16 physically active young men | 23 ± 1 | Control: Without IMW 1: IMW-2 × 15 (15% MIP) 2: IMW-2 × 15 (40% MIP) 3: IMW-2 × 15 (60% MIP) (60-s pause)(2 min before physical exercise) | 30-s all-out tethered running on a non-motorized treadmill Recovery post-test | ↑ Relative power (W.kg−1) and force (N.kg−1) in IMW at 15, 40 and 60% MIP ↑ Velocity (m.s−1) in IMW at 60% MIP) No changes in metabolic or respiratory parameters in the recovery period |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirino, C.; Marostegan, A.B.; Hartz, C.S.; Moreno, M.A.; Gobatto, C.A.; Manchado-Gobatto, F.B. Effects of Inspiratory Muscle Warm-Up on Physical Exercise: A Systematic Review. Biology 2023, 12, 333. https://doi.org/10.3390/biology12020333
Cirino C, Marostegan AB, Hartz CS, Moreno MA, Gobatto CA, Manchado-Gobatto FB. Effects of Inspiratory Muscle Warm-Up on Physical Exercise: A Systematic Review. Biology. 2023; 12(2):333. https://doi.org/10.3390/biology12020333
Chicago/Turabian StyleCirino, Carolina, Anita B. Marostegan, Charlini S. Hartz, Marlene A. Moreno, Claudio A. Gobatto, and Fúlvia B. Manchado-Gobatto. 2023. "Effects of Inspiratory Muscle Warm-Up on Physical Exercise: A Systematic Review" Biology 12, no. 2: 333. https://doi.org/10.3390/biology12020333