
The Ratio of von Willebrand Factor Antigen to ADAMTS13 Activity: Usefulness as a Prognostic Biomarker in Acute-on-Chronic Liver Failure
 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
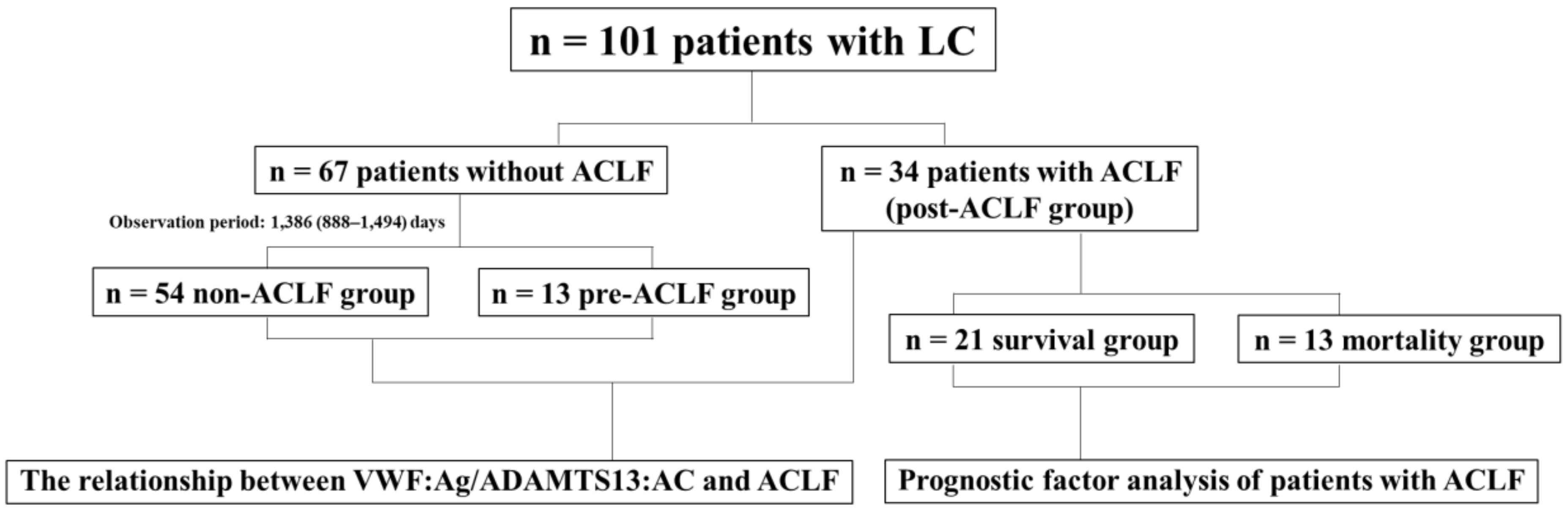
2.1. Patients and Study Design
2.2. Determination of ADAMTS13 Activity and VWF Antigen
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients
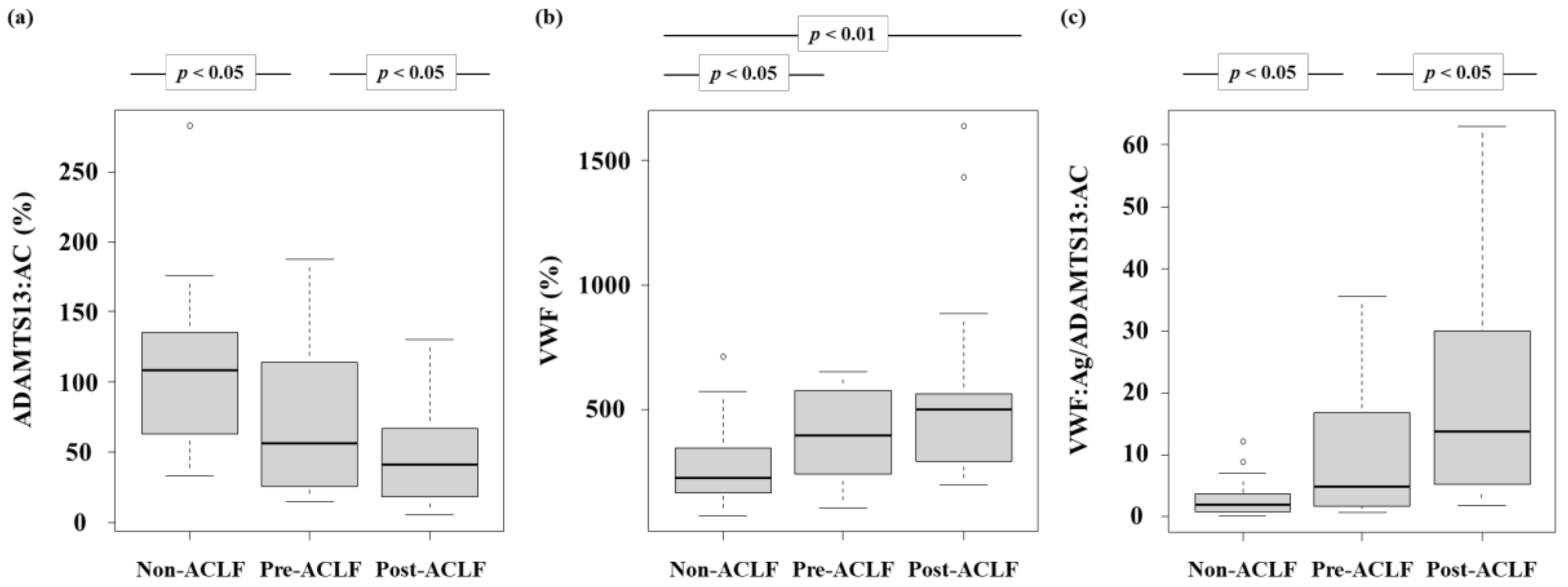
3.2. ADAMTS13:AC and VWF:Ag Levels
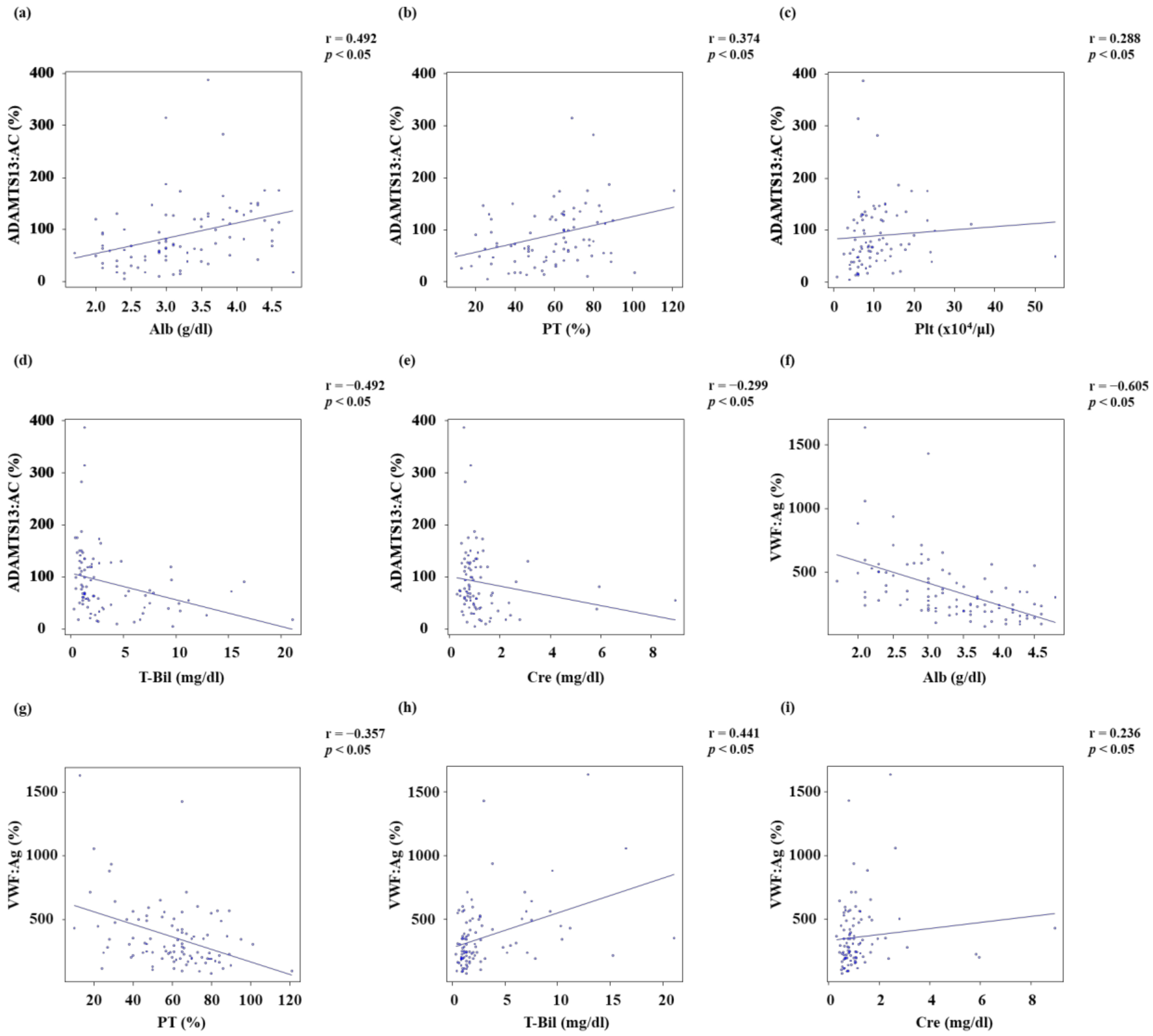
3.3. Relationship between ADAMTS13:AC or VWF:Ag and Other Parameters
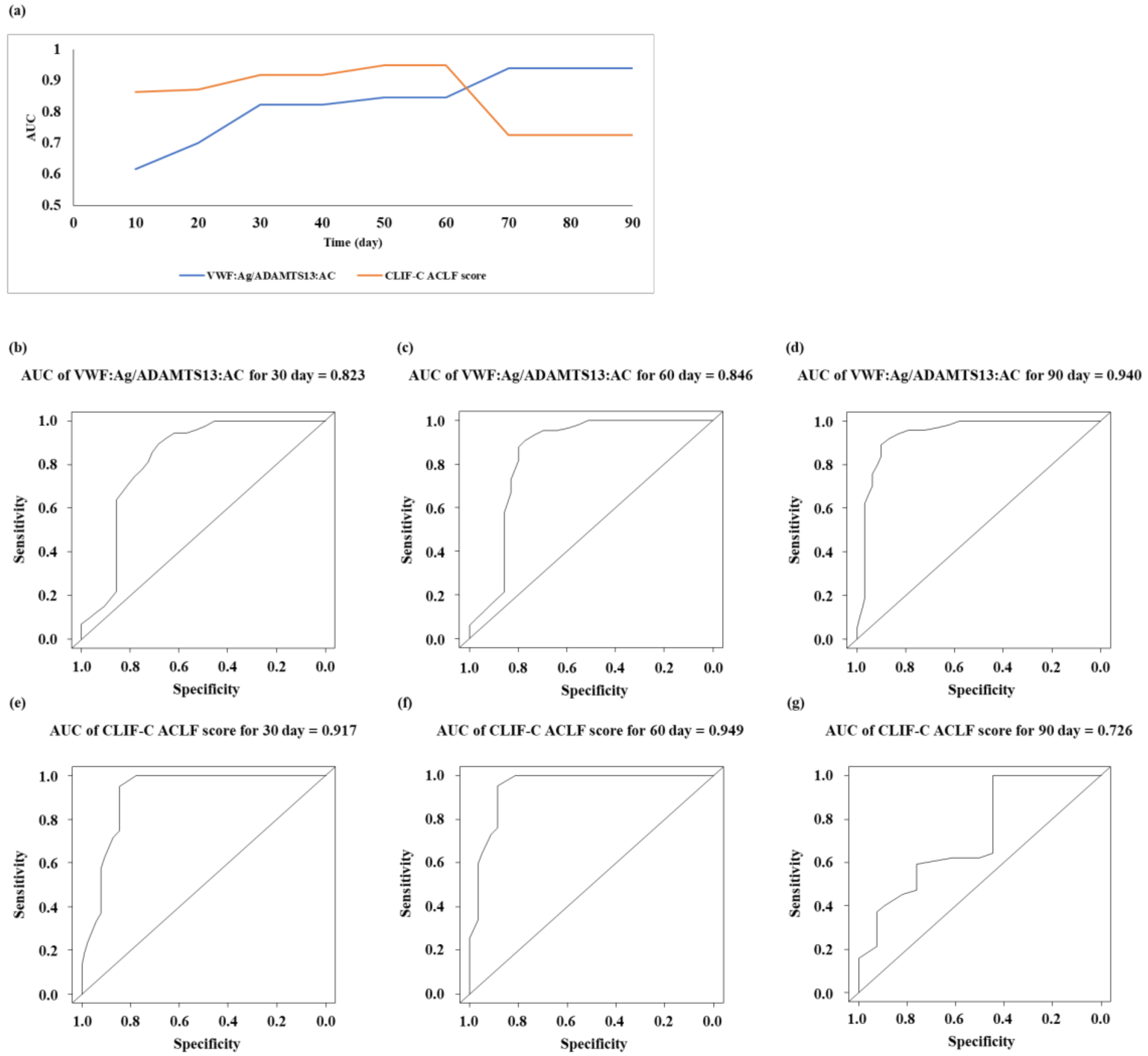
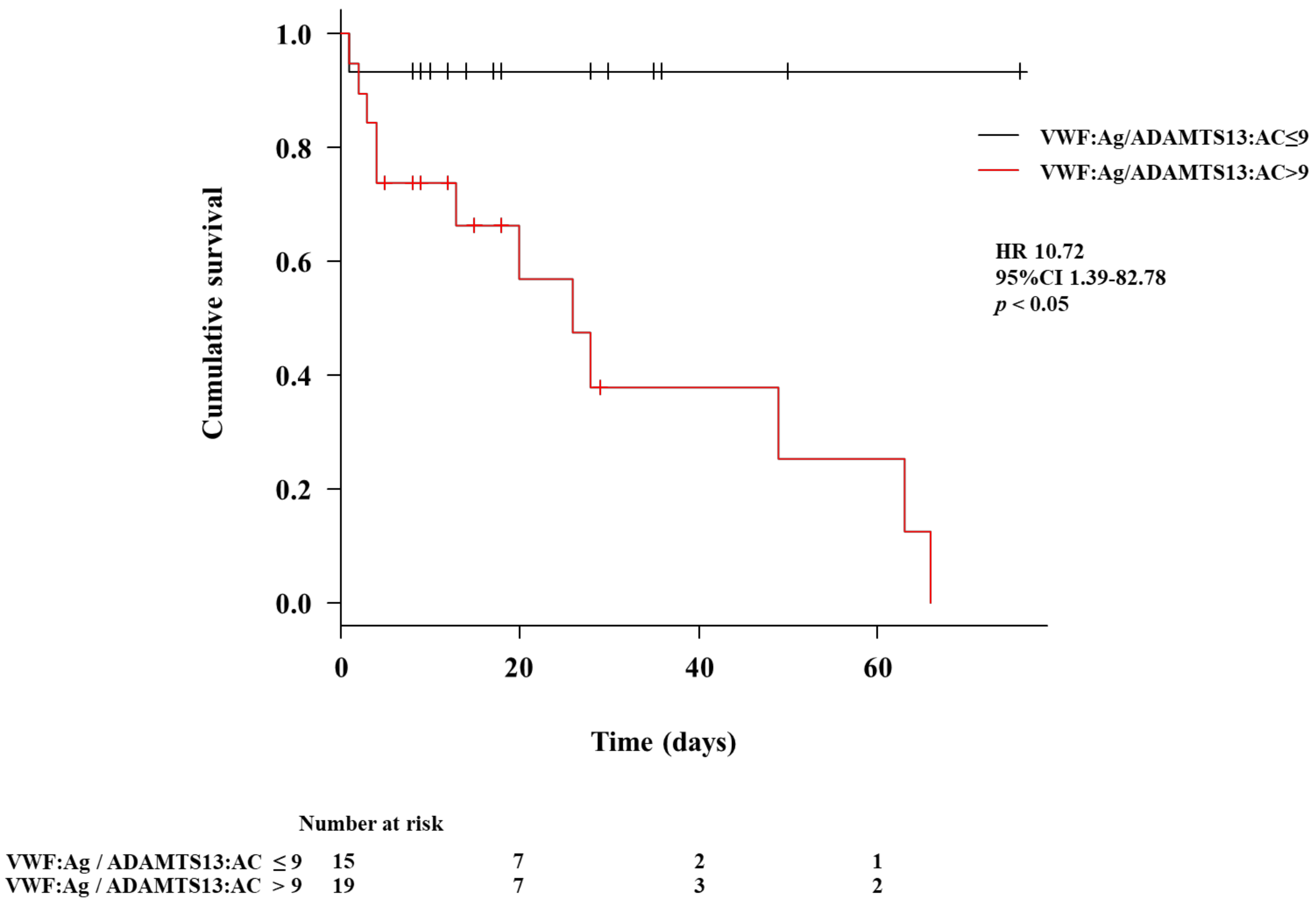
3.4. Prognostic Factor for Patients with Liver Cirrhosis in the Post-ACLF Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADAMTS13 | a disintegrin-like and metalloproteinase with thrombospondin type-1 motifs 13 |
| VWF | von Willebrand factor |
| ECs | endothelial cells Please ensure that all individuals included in this section have consented to the acknowledgement. |
| ADAMTS13:AC | ADAMTS13 activity |
| VWF:Ag | VWF antigen |
| LC | liver cirrhosis |
| ALF | acute liver failure |
| HRS | hepatorenal syndrome |
| ACLF | acute-on-chronic liver failure |
| PHT | portal hypertension |
| VWF:Ag/ADAMTS13:AC | the ratio of VWF:Ag to ADAMTS13:AC |
| VTE | venous thromboembolism |
| PT | prothrombin time |
| T-Bil | total bilirubin |
| ELISA | enzyme-linked immunosorbent assay |
| HR | hazard ratio |
| Alb | albumin |
| Cre | creatinine |
| AST | aspartate aminotransferase |
| ALT | alanine aminotransferase |
| MELD | model for end-stage liver disease |
| CLIF-C | the chronic liver failure consortium |
| AUC | area under curve |
| DIC | disseminated intravascular coagulation |
References
- Takaya, H.; Kawaratani, H.; Kubo, T.; Seki, K.; Sawada, Y.; Kaji, K.; Okura, Y.; Takeda, K.; Kitade, M.; Moriya, K.; et al. Platelet hyperaggregability is associated with decreased ADAMTS13 activity and enhanced endotoxemia in patients with acute cholangitis. Hepatol. Res. 2018, 48, E52–E60. [Google Scholar] [CrossRef] [Green Version]
- Takaya, H.; Uemura, M.; Fujimura, Y.; Matsumoto, M.; Matsuyama, T.; Kato, S.; Morioka, C.; Ishizashi, H.; Hori, Y.; Fujimoto, M.; et al. ADAMTS13 activity may predict the cumulative survival of patients with liver cirrhosis in comparison with the Child-Turcotte-Pugh score and the Model for End-Stage Liver Disease score. Hepatol. Res. 2012, 42, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Takaya, H.; Yoshiji, H.; Kawaratani, H.; Sakai, K.; Matsumoto, M.; Fujimura, Y.; Fukui, H. Decreased activity of plasma ADAMTS13 are related to enhanced cytokinemia and endotoxemia in patients with acute liver failure. Biomed. Rep. 2017, 7, 277–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takaya, H.; Kawaratani, H.; Tsuji, Y.; Nakanishi, K.; Saikawa, S.; Sato, S.; Sawada, Y.; Kaji, K.; Okura, Y.; Shimozato, N.; et al. von Willebrand factor is a useful biomarker for liver fibrosis and prediction of hepatocellular carcinoma development in patients with hepatitis B and C. United Eur. Gastroenterol. J. 2018, 6, 1401–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uemura, M.; Tatsumi, K.; Matsumoto, M.; Fujimoto, M.; Matsuyama, T.; Ishikawa, M.; Iwamoto, T.A.; Mori, T.; Wanaka, A.; Fukui, H.; et al. Localization of ADAMTS13 to the stellate cells of human liver. Blood 2005, 106, 922–924. [Google Scholar] [CrossRef] [Green Version]
- Moake, J.L.; Turner, N.A.; Stathopoulos, N.A.; Nolasco, L.H.; Hellums, J.D. Involvement of large plasma von Willebrand factor (vWF) multimers and unusually large vWF forms derived from endothelial cells in shear stress-induced platelet aggregation. J. Clin. Investig. 1986, 78, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- Furlan, M.; Robles, R.; Galbusera, M.; Remuzzi, G.; Kyrle, P.A.; Brenner, B.; Krause, M.; Scharrer, I.; Aumann, V.; Mittler, U.; et al. Von Willebrand Factor–Cleaving Protease in Thrombotic Thrombocytopenic Purpura and the Hemolytic–Uremic Syndrome. N. Engl. J. Med. 1998, 339, 1578–1584. [Google Scholar] [CrossRef]
- Uemura, M.; Fujimura, Y.; Ko, S.; Matsumoto, M.; Nakajima, Y.; Fukui, H. Determination of ADAMTS13 and Its Clinical Significance for ADAMTS13 Supplementation Therapy to Improve the Survival of Patients with Decompensated Liver Cirrhosis. Int. J. Hepatol. 2011, 2011, 759047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uemura, M.; Fujimura, Y.; Matsumoto, M.; Ishizashi, H.; Kato, S.; Matsuyama, T.; Isonishi, A.; Ishikawa, M.; Yagita, M.; Morioka, C.; et al. Comprehensive analysis of ADAMTS13 in patients with liver cirrhosis. Thromb. Haemost 2008, 99, 1019–1029. [Google Scholar] [CrossRef]
- Matsuyama, T.; Uemura, M.; Ishikawa, M.; Matsumoto, M.; Ishizashi, H.; Kato, S.; Morioka, C.; Fujimoto, M.; Kojima, H.; Yoshiji, H.; et al. Increased von Willebrand factor over decreased ADAMTS13 activity may contribute to the development of liver disturbance and multiorgan failure in patients with alcoholic hepatitis. Alcohol. Clin. Exp. Res. 2007, 31, S27–S35. [Google Scholar] [CrossRef]
- Ishikawa, M.; Uemura, M.; Matsuyama, T.; Matsumoto, M.; Ishizashi, H.; Kato, S.; Morioka, C.; Fujimoto, M.; Kojima, H.; Yoshiji, H.; et al. Potential Role of Enhanced Cytokinemia and Plasma Inhibitor on the Decreased Activity of Plasma ADAMTS13 in Patients with Alcoholic Hepatitis: Relationship to Endotoxemia. Alcohol. Clin. Exp. Res. 2010, 34, S25–S33. [Google Scholar] [CrossRef] [PubMed]
- Takaya, H.; Namisaki, T.; Asada, S.; Iwai, S.; Kubo, T.; Suzuki, J.; Enomoto, M.; Tsuji, Y.; Fujinaga, Y.; Nishimura, N.; et al. ADAMTS13, VWF, and Endotoxin Are Interrelated and Associated with the Severity of Liver Cirrhosis via Hypercoagulability. J. Clin. Med. 2022, 11, 1835. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, M.; Takaya, H.; Namisaki, T.; Fujinaga, Y.; Nishimura, N.; Sawada, Y.; Kaji, K.; Kawaratani, H.; Moriya, K.; Akahane, T.; et al. Ratio of von Willebrand factor antigen to ADAMTS13 activity is a useful biomarker for acute-on-chronic liver failure development and prognosis in patients with liver cirrhosis. Hepatol. Res. 2021, 52, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Kalambokis, G.N.; Oikonomou, A.; Christou, L.; Kolaitis, N.I.; Tsianos, E.V.; Christodoulou, D.; Baltayiannis, G. Von Willebrand factor and procoagulant imbalance predict outcome in patients with cirrhosis and thrombocytopenia. J. Hepatol. 2016, 65, 921–928. [Google Scholar] [CrossRef]
- Hugenholtz, G.C.G.; Adelmeijer, J.; Meijers, J.C.M.; Porte, R.J.; Stravitz, R.T.; Lisman, T. An unbalance between von Willebrand factor and ADAMTS13 in acute liver failure: Implications for hemostasis and clinical outcome. Hepatology 2013, 58, 752–761. [Google Scholar] [CrossRef]
- Sarin, S.K.; Choudhury, A. Acute-on-chronic liver failure: Terminology, mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 131–149. [Google Scholar] [CrossRef]
- Zhang, T.; Sun, K.; Wang, Y.; Huang, L.; Lang, R.; Jiang, W. Disruption of the gut-liver axis in the pathogenesis of acute-on-chronic liver failure. Eur. J. Gastroenterol. Hepatol. 2018, 30, 130–135. [Google Scholar] [CrossRef]
- Mochida, S.; Nakayama, N.; Terai, S.; Yoshiji, H.; Shimizu, M.; Ido, A.; Inoue, K.; Genda, T.; Takikawa, Y.; Takami, T.; et al. Diagnostic criteria for acute-on-chronic liver failure and related disease conditions in Japan. Hepatol. Res. 2022, 52, 417–421. [Google Scholar] [CrossRef]
- Goulis, J.; Patch, D.; Burroughs, A.K. Bacterial infection in the pathogenesis of variceal bleeding. Lancet 1999, 353, 139–142. [Google Scholar] [CrossRef]
- Carrion, A.F.; Martin, P. Keeping Patients with End-Stage Liver Disease Alive While Awaiting Transplant: Management of Complications of Portal Hypertension. Clin. Liver Dis. 2021, 25, 103–120. [Google Scholar] [CrossRef]
- Carnevale, R.; Raparelli, V.; Nocella, C.; Bartimoccia, S.; Novo, M.; Severino, A.; De Falco, E.; Cammisotto, V.; Pasquale, C.; Crescioli, C.; et al. Gut-derived endotoxin stimulates factor VIII secretion from endothelial cells. Implications for hypercoagulability in cirrhosis. J. Hepatol. 2017, 67, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Ferlitsch, M.; Reiberger, T.; Hoke, M.; Salzl, P.; Schwengerer, B.; Ulbrich, G.; Payer, B.A.; Trauner, M.; Peck-Radosavljevic, M.; Ferlitsch, A. Von Willebrand factor as new noninvasive predictor of portal hypertension, decompensation and mortality in patients with liver cirrhosis. Hepatology 2012, 56, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Reiberger, T.; Mandorfer, M.; Kivaranovic, D.; Hametner, S.; Hametner, S.; Paternostro, R.; Scheiner, B.; Schneeweiss-Friedl, J.; Trauner, M.; et al. The von Willebrand Factor antigen to platelet ratio (VITRO) score predicts hepatic decompensation and mortality in cirrhosis. J. Gastroenterol. 2019, 55, 533–542. [Google Scholar] [CrossRef]
- Hametner, S.; Ferlitsch, A.; Ferlitsch, M.; Etschmaier, A.; Schöfl, R.; Ziachehabi, A.; Maieron, A. The VITRO Score (Von Willebrand Factor Antigen/Thrombocyte Ratio) as a New Marker for Clinically Significant Portal Hypertension in Comparison to Other Non-Invasive Parameters of Fibrosis Including ELF Test. PLoS ONE 2016, 11, e0149230. [Google Scholar] [CrossRef] [Green Version]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for Liver Cirrhosis 2020. J. Gastroenterol. 2021, 56, 593–619. [Google Scholar] [CrossRef] [PubMed]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2020. Hepatol. Res. 2021, 51, 725–749. [Google Scholar] [CrossRef]
- Kato, S.; Matsumoto, M.; Matsuyama, T.; Isonishi, A.; Hiura, H.; Fujimura, Y. Novel monoclonal antibody-based enzyme immunoassay for determining plasma levels of ADAMTS13 activity. Transfusion 2006, 46, 1444–1452. [Google Scholar] [CrossRef]
- Matsumoto, M.; Kawaguchi, S.; Ishizashi, H.; Yagi, H.; Iida, J.; Sakaki, T.; Fujimura, Y. Platelets Treated with Ticlopidine Are Less Reactive to Unusually Large von Willebrand Factor Multimers than Are Those Treated with Aspirin under High Shear Stress. Pathophysiol. Haemost. Thromb. 2005, 34, 35–40. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Mandorfer, M.; Schwabl, P.; Paternostro, R.; Pomej, K.; Bauer, D.; Thaler, J.; Ay, C.; Quehenberger, P.; Fritzer-Szekeres, M.; Peck-Radosavljevic, M.; et al. Von Willebrand factor indicates bacterial translocation, inflammation, and procoagulant imbalance and predicts complications independently of portal hypertension severity. Aliment. Pharmacol. Ther. 2018, 47, 980–988. [Google Scholar] [CrossRef]
- Wu, H.; Yan, S.; Wang, G.; Cui, S.; Zhang, C.; Zhu, Q. von Willebrand factor as a novel noninvasive predictor of portal hypertension and esophageal varices in hepatitis B patients with cirrhosis. Scand. J. Gastroenterol. 2015, 50, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Prasanna, K.S.; Goel, A.; Amirtharaj, G.J.; Ramachandran, A.; Balasubramanian, K.A.; Mackie, I.; Zachariah, U.; Sajith, K.G.; Elias, E.; Eapen, C.E. Plasma von Willebrand factor levels predict in-hospital survival in patients with acute-on-chronic liver failure. Indian J. Gastroenterol. 2016, 35, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.Q.; Han, M.F.; Ma, K.; Chen, G.; Wan, X.Y.; Kilonzo, S.B.; Wu, W.Y.; Wang, Y.L.; You, J.; Ning, Q. Acute kidney injury in acute-on-chronic liver failure is different from in decompensated cirrhosis. World J. Gastroenterol. 2018, 24, 2300–2310. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Park, J.W.; Kim, H.S.; Jang, M.K.; Suk, K.T.; Kim, D.J. The Role of Gut Dysbiosis in Acute-on-Chronic Liver Failure. Int. J. Mol. Sci. 2021, 22, 11680. [Google Scholar] [CrossRef]
- Takaya, H.; Namisaki, T.; Sato, S.; Kaji, K.; Tsuji, Y.; Kaya, D.; Fujinaga, Y.; Sawada, Y.; Shimozato, N.; Kawaratani, H.; et al. Increased Endotoxin Activity Is Associated with the Risk of Developing Acute-on-Chronic Liver Failure. J. Clin. Med. 2020, 9, 1467. [Google Scholar] [CrossRef]
- Okura, Y.; Namisaki, T.; Sato, S.; Moriya, K.; Akahane, T.; Kitade, M.; Kawaratani, H.; Kaji, K.; Takaya, H.; Sawada, Y.; et al. Proton pump inhibitor therapy does not increase serum endotoxin activity in patients with cirrhosis. Hepatol. Res. 2019, 49, 232–238. [Google Scholar] [CrossRef]
- Reiter, R.A.; Varadi, K.; Turecek, P.L.; Jilma, B.; Knöbl, P. Changes in ADAMTS13 (von-Willebrand-factor-cleaving protease) activity after induced release of von Willebrand factor during acute systemic inflammation. Thromb. Haemost. 2005, 93, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, H.; Nishio, K.; Asai, H.; Watanabe, T.; Seki, T.; Matsui, H.; Sugimoto, M.; Matsumoto, M.; Fujimura, Y.; Okuchi, K. Ratio of von Willebrand factor propeptide to ADAMTS13 is associated with severity of sepsis. Shock 2013, 39, 409–414. [Google Scholar] [CrossRef] [Green Version]
- Pépin, M.; Kleinjan, A.; Hajage, D.; Büller, H.R.; Di Nisio, M.; Kamphuisen, P.W.; Salomon, L.; Veyradier, A.; Stepanian, A.; Mahé, I. ADAMTS-13 and von Willebrand factor predict venous thromboembolism in patients with cancer. J. Thromb. Haemost. 2016, 14, 306–315. [Google Scholar] [CrossRef]
- Samuelson Bannow, B.T.; Konkle, B.A. Laboratory biomarkers for venous thromboembolism risk in patients with hematologic malignancies: A review. Thromb. Res. 2018, 163, 138–145. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 101) | Non-ACLF Group (n = 54) | Pre-ACLF Group (n = 13) | Post-ACLF Group (n = 34) |
|---|---|---|---|---|
| Age (years) | 71 (62–75) | 69 (63–75) | 73 (71–81) | 71 (62–77) |
| Sex (male/female) | 64/37 | 32/22 | 8/5 | 24/10 |
| Etiology (HBV/HCV/alcohol/NASH/AIH/PBC/others) | 5/23/40/14/7/5/7 | 2/14/18/11/3/4/2 | 1/5/5/1/0/1/0 | 2/4/17/2/4/0/5 |
| Albumin (g/dL) | 3.2 (2.8–3.9) | 3.8 (3.4–4.2) | 3.0 (2.9–3.2) * | 2.5 (2.1–3.0) *, ** |
| Aspartate aminotransferase (U/L) | 43 (32–76) | 36 (28–50) | 42 (39–69) | 80 (42–232) *, ** |
| Alanine aminotransferase (U/L) | 28 (19–58) | 24 (17–41) | 27 (23–39) | 65 (30–113) *, ** |
| Blood urea nitrogen (mg/dL) | 16 (13–25) | 15 (12–21) | 16 (14–20) | 22 (12–37) * |
| Creatinine (mg/dL) | 0.9 (0.7–1.2) | 0.8 (0.5–1.0) | 1.0 (0.9–1.1) * | 1.1 (0.7–1.7) * |
| Total bilirubin (mg/dL) | 1.6 (1.0–4.1) | 1.1 (0.9–1.6) | 1.8 (1.1–2.2) * | 7.1 (5.0–10.2) *, ** |
| Prothrombin time (%) | 61 (40–73) | 65 (55–73) | 67 (62–79) | 33 (28–40) *, ** |
| Platelet count (×104/mm3) | 9.2 (6.3–12.8) | 9.6 (7.5–12.8) | 6.8 (5.5–13.0) | 7.7 (6.0–11.8) * |
| C-reactive protein (mg/dL) | 0.3 (0.0–1.0) | 0.1 (0.0–0.3) | 0.2 (0.1–0.6) | 1.5 (0.9–4.3) *, ** |
| MELD score | 10 (9–17) | 9 (8–11) | 9 (7–12) | 20 (14–28) *, ** |
| Variable | Total (n = 34) | Survival Group (n = 21) | Mortality Group (n = 13) | p-Value * |
|---|---|---|---|---|
| Age (years) | 71 (62–77) | 63 (47–73) | 77 (65–81) | 0.022 |
| Sex (male/female) | 24/10 | 14/7 | 10/3 | 0.704 |
| Etiology (HBV/HCV/alcohol/NASH/AIH/others) | 2/4/17/2/4/5 | 0/1/13/1/3/3 | 2/3/4/1/1/2 | 0.155 |
| Events (infection/bleeding/alcohol/underlying liver disease/circulatory insufficiency/others) | 11/5/8/7/1/2 | 6/3/6/5/0/1 | 5/2/2/2/1/1 | 0.794 |
| Severity grade of ACLF (0/1/2/3) | 20/2/4/8 | 18/2/1/0 | 2/0/3/8 | 0.000 |
| CLIF-C ACLF score | 44 (38–52) | 40 (37–45) | 52 (45–58) | 0.002 |
| Albumin (g/dL) | 2.5 (2.1–3.0) | 2.5 (2.3–3.0) | 2.5 (2.1–2.9) | 0.301 |
| Aspartate aminotransferase (U/L) | 80 (42–232) | 74 (47–226) | 71 (43–240) | 0.808 |
| Alanine aminotransferase(U/L) | 62 (30–113) | 57 (29–90) | 61 (22–133) | 0.955 |
| Blood urea nitrogen (mg/dL) | 22 (12–37) | 26 (12–34) | 22 (21–41) | 0.600 |
| Creatinine (mg/dL) | 1.1 (0.7–1.7) | 1.2 (0.7–1.5) | 1.2 (1.0–1.9) | 0.203 |
| Total bilirubin (mg/dL) | 7.1 (5.0–10.2) | 6.0 (5.0–7.5) | 9.7 (6.1–10.7) | 0.062 |
| Prothrombin time (%) | 33 (28–40) | 38 (30–40) | 28 (22–30) | 0.016 |
| Platelet count (×104/mm3) | 7.7 (6.0–11.8) | 8.0 (6.4–13.1) | 8.2 (5.9–10.9) | 0.779 |
| C-reactive protein (mg/dL) | 1.5 (0.9–4.3) | 1.2 (0.7–3.9) | 2.0 (1.0–4.5) | 0.339 |
| MELD score | 20 (14–28) | 18 (13–25) | 25 (22–30) | 0.018 |
| ADAMTS13:AC (%) | 41 (18–67) | 63 (29–71) | 35 (14–44) | 0.038 |
| VWF:Ag (%) | 502 (298–763) | 314 (242–561) | 819 (444–1560) | 0.007 |
| VWF:Ag/ADAMTS13:AC | 13.7 (6.1–29.5) | 7.4 (3.7–14.1) | 19.6 (9.8–31.2) | 0.009 |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | p-Value | HR | 95%CI | p-Value | |
| ADAMTS13:AC | 0.99 | 0.950–1.023 | 0.4409 | |||
| VWF:Ag | 1.00 | 1.000–1.002 | 0.2601 | |||
| VWF:Ag/ADAMTS13:AC | 1.01 | 0.999–1.012 | 0.0789 | 1.01 | 1.001–1.009 | 0.0261 |
| CLIF-C ACLF score | 1.17 | 1.078–1.273 | 0.0002 | 1.19 | 1.039–1.404 | 0.0138 |
| Creatinine | 1.63 | 1.152–2.296 | 0.0057 | 1.20 | 0.610–2.401 | 0.5844 |
| C-reactive protein | 1.04 | 0.925–1.176 | 0.4956 | |||
| MELD score | 1.10 | 1.039–1.172 | 0.0013 | 0.96 | 0.803–1.156 | 0.6885 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takaya, H.; Namisaki, T.; Enomoto, M.; Kubo, T.; Tsuji, Y.; Fujinaga, Y.; Nishimura, N.; Kaji, K.; Kawaratani, H.; Moriya, K.; et al. The Ratio of von Willebrand Factor Antigen to ADAMTS13 Activity: Usefulness as a Prognostic Biomarker in Acute-on-Chronic Liver Failure. Biology 2023, 12, 164. https://doi.org/10.3390/biology12020164
Takaya H, Namisaki T, Enomoto M, Kubo T, Tsuji Y, Fujinaga Y, Nishimura N, Kaji K, Kawaratani H, Moriya K, et al. The Ratio of von Willebrand Factor Antigen to ADAMTS13 Activity: Usefulness as a Prognostic Biomarker in Acute-on-Chronic Liver Failure. Biology. 2023; 12(2):164. https://doi.org/10.3390/biology12020164
Chicago/Turabian StyleTakaya, Hiroaki, Tadashi Namisaki, Masahide Enomoto, Takahiro Kubo, Yuki Tsuji, Yukihisa Fujinaga, Norihisa Nishimura, Kosuke Kaji, Hideto Kawaratani, Kei Moriya, and et al. 2023. "The Ratio of von Willebrand Factor Antigen to ADAMTS13 Activity: Usefulness as a Prognostic Biomarker in Acute-on-Chronic Liver Failure" Biology 12, no. 2: 164. https://doi.org/10.3390/biology12020164