

The Gut Microbiota in Kidney Transplantation: A Target for Personalized Therapy?
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
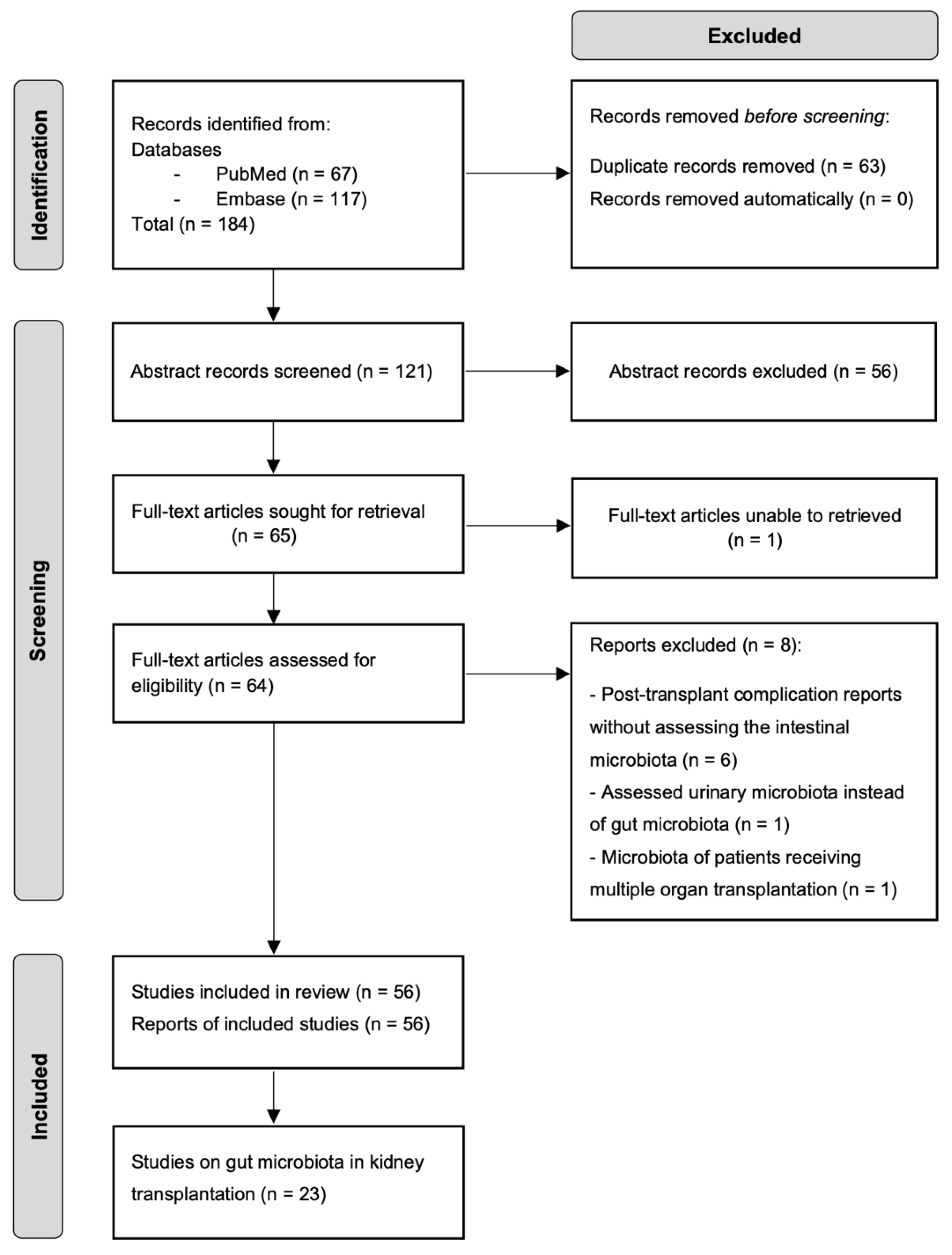
2. Review Strategy
2.1. Literature Search
2.2. Eligible Criteria
2.3. Data Extraction
3. Gut Microbial Dysbiosis in Kidney Transplant Recipients
4. The Impact of Gut Microbiota on Kidney Transplantation
4.1. Uremic Retention Solutes
4.2. Allograft Function
4.3. Allograft Rejection
4.4. Immunosuppressants Metabolism
4.5. Post-Transplant Infection
4.6. Post-Transplant Diarrhea
4.7. New Onset Diabetes (NODAT)
5. Gut-Microbiota-Based Therapies in Kidney Transplantation
6. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nobakht, E.; Jagadeesan, M.; Paul, R.; Bromberg, J.; Dadgar, S. Precision Medicine in Kidney Transplantation: Just Hype or a Realistic Hope? Transplant. Direct 2021, 7, e650. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.R.; Muthukumar, T.; Dadhania, D.; Taur, Y.; Jenq, R.R.; Toussaint, N.C.; Ling, L.; Pamer, E.; Suthanthiran, M. Gut Microbiota and Tacrolimus Dosing in Kidney Transplantation. PLoS ONE 2015, 10, e0122399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Transplant Recipient–KDIGO. Available online: https://kdigo.org/guidelines/transplant-recipient/ (accessed on 5 October 2022).
- Guirong, Y.E.; Minjie, Z.; Lixin, Y.U.; Junsheng, Y.E.; Lin, Y.; Lisha, S. Gut Microbiota in Renal Transplant Recipients, Patients with Chronic Kidney Disease and Healthy Subjects. Nan Fang Yi Ke Da Xue Xue Bao 2018, 38, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Swarte, J.C.; Douwes, R.M.; Hu, S.; Vich Vila, A.; Eisenga, M.F.; van Londen, M.; Gomes-Neto, A.W.; Weersma, R.K.; Harmsen, H.J.M.; Bakker, S.J.L. Characteristics and Dysbiosis of the Gut Microbiome in Renal Transplant Recipients. J. Clin. Med. 2020, 9, 386. [Google Scholar] [CrossRef] [Green Version]
- Souai, N.; Zidi, O.; Mosbah, A.; Kosai, I.; Manaa, J.E.; Mokhtar, N.B.; Asimakis, E.; Stathopoulou, P.; Cherif, A.; Tsiamis, G.; et al. Impact of the Post-Transplant Period and Lifestyle Diseases on Human Gut Microbiota in Kidney Graft Recipients. Microorganisms 2020, 8, 1724. [Google Scholar] [CrossRef]
- Lee, J.R.; Muthukumar, T.; Dadhania, D.; Toussaint, N.C.; Ling, L.; Pamer, E.; Suthanthiran, M. Gut Microbial Community Structure and Complications Following Kidney Transplantation: A Pilot Study. Transplantation 2014, 98, 697. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.H.; Ying, N.; Lian, Z.H.; Fa, Y.Q. The Alteration Human of Gut Microbiota and Metabolites before and after Renal Transplantation. Microb. Pathog. 2021, 160, 105191. [Google Scholar] [CrossRef]
- Chan, S.; Morrison, M.; Hawley, C.M.; Campbell, S.B.; Francis, R.S.; Isbel, N.M.; Pascoe, E.M.; Johnson, D.W. Characteristics of the Gastrointestinal Microbiota in Paired Live Kidney Donors and Recipients. Nephrology 2021, 26, 471–478. [Google Scholar] [CrossRef]
- Wang, J.; Li, X.; Wu, X.; Wang, Z.; Zhang, C.; Cao, G.; Liu, S.; Yan, T. Gut Microbiota Alterations Associated with Antibody-Mediated Rejection after Kidney Transplantation. Appl. Microbiol. Biotechnol. 2021, 105, 2473–2484. [Google Scholar] [CrossRef]
- Guo, Y.; Crnkovic, C.; Won, K.J.; Lee, J.R.; Orjala, J.; Lee, H.; Jeong, H. Commensal Gut Bacteria Convert the Immunosuppressant Tacrolimus to Less Potent Metabolites. Drug Metab. Dispos. 2019, 47, 194–202. [Google Scholar] [CrossRef]
- Guo, Y.; Lee, H.; Edusei, E.; Albakry, S.; Jeong, H.; Lee, J.R. Blood Profiles of Gut Bacterial Tacrolimus Metabolite in Kidney Transplant Recipients. Transplant. Direct 2020, 6, 601. [Google Scholar] [CrossRef] [PubMed]
- Fricke, W.F.; Maddox, C.; Song, Y.; Bromberg, J.S. Human Microbiota Characterization in the Course of Renal Transplantation. Am. J. Transplant. 2014, 14, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Magruder, M.; Sholi, A.N.; Gong, C.; Zhang, L.; Edusei, E.; Huang, J.; Albakry, S.; Satlin, M.J.; Westblade, L.F.; Crawford, C.; et al. Gut Uropathogen Abundance Is a Risk Factor for Development of Bacteriuria and Urinary Tract Infection. Nat. Commun. 2019, 10, 5521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magruder, M.; Edusei, E.; Zhang, L.; Albakry, S.; Satlin, M.J.; Westblade, L.F.; Malha, L.; Sze, C.; Lubetzky, M.; Dadhania, D.M.; et al. Gut Commensal Microbiota and Decreased Risk for Enterobacteriaceae Bacteriuria and Urinary Tract Infection. Gut Microbes 2020, 12, 1805281. [Google Scholar] [CrossRef]
- Lee, J.R.; Huang, J.; Magruder, M.; Zhang, L.T.; Gong, C.; Sholi, A.N.; Albakry, S.; Edusei, E.; Muthukumar, T.; Lubetzky, M.; et al. Butyrate-Producing Gut Bacteria and Viral Infections in Kidney Transplant Recipients: A Pilot Study. Transpl. Infect. Dis. 2019, 21, e13180. [Google Scholar] [CrossRef]
- Lee, J.R.; Magruder, M.; Zhang, L.; Westblade, L.F.; Satlin, M.J.; Robertson, A.; Edusei, E.; Crawford, C.; Ling, L.; Taur, Y.; et al. Gut Microbiota Dysbiosis and Diarrhea in Kidney Transplant Recipients. Am. J. Transplant. 2019, 19, 488–500. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.T.; Westblade, L.F.; Iqbal, F.; Taylor, M.R.; Chung, A.; Satlin, M.J.; Magruder, M.; Edusei, E.; Albakry, S.; Botticelli, B.; et al. Gut Microbiota Profiles and Fecal Beta-Glucuronidase Activity in Kidney Transplant Recipients with and without Post-Transplant Diarrhea. Clin. Transplant. 2021, 35, e14260. [Google Scholar] [CrossRef]
- Lecronier, M.; Tashk, P.; Tamzali, Y.; Tenaillon, O.; Denamur, E.; Barrou, B.; Aron-Wisnewsky, J.; Tourret, J. Gut Microbiota Composition Alterations Are Associated with the Onset of Diabetes in Kidney Transplant Recipients. PLoS ONE 2020, 15, e0227373. [Google Scholar] [CrossRef] [Green Version]
- Ardalan, M.; Vahed, S.Z. Gut Microbiota and Renal Transplant Outcome. Biomed. Pharmacother. 2017, 90, 229–236. [Google Scholar] [CrossRef]
- Taylor, M.R.; Flannigan, K.L.; Rahim, H.; Mohamud, A.; Lewis, I.A.; Hirota, S.A.; Greenway, S.C. Vancomycin Relieves Mycophenolate Mofetil-Induced Gastrointestinal Toxicity by Eliminating Gut Bacterial β-Glucuronidase Activity. Sci. Adv. 2019, 5, eaax2358. [Google Scholar] [CrossRef]
- Stripling, J.; Kumar, R.; Baddley, J.W.; Nellore, A.; Dixon, P.; Howard, D.; Ptacek, T.; Lefkowitz, E.J.; Tallaj, J.A.; Benjamin, W.H.; et al. Loss of Vancomycin-Resistant Enterococcus Fecal Dominance in an Organ Transplant Patient With Clostridium Difficile Colitis After Fecal Microbiota Transplant. Open Forum Infect. Dis. 2015, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biehl, L.M.; Cruz Aguilar, R.; Farowski, F.; Hahn, W.; Nowag, A.; Wisplinghoff, H.; Vehreschild, M.J.G.T. Fecal Microbiota Transplantation in a Kidney Transplant Recipient with Recurrent Urinary Tract Infection. Infection 2018, 46, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Grosen, A.K.; Povlsen, J.V.; Lemming, L.E.; Jørgensen, S.M.D.; Dahlerup, J.F.; Hvas, C.L. Faecal Microbiota Transplantation Eradicated Extended-Spectrum Beta-Lactamase-Producing Klebsiella Pneumoniae from a Renal Transplant Recipient with Recurrent Urinary Tract Infections. Case Rep. Nephrol. Dial. 2019, 9, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, X.; Wu, X.; Wang, Z.; Wu, X.; Wang, S.; Jing, G.; Yan, T. Fecal Microbiota Transplantation as an Effective Treatment for Carbapenem-Resistant Klebsiella Pneumoniae Infection in a Renal Transplant Patient. Infect. Drug Resist. 2021, 14, 1805–1811. [Google Scholar] [CrossRef]
- Gabarre, P.; Loens, C.; Tamzali, Y.; Barrou, B.; Jaisser, F.; Tourret, J. Immunosuppressive Therapy after Solid Organ Transplantation and the Gut Microbiota: Bidirectional Interactions with Clinical Consequences. Am. J. Transplant. 2022, 22, 1014–1030. [Google Scholar] [CrossRef]
- Cohen-Poradosu, R.; McLoughlin, R.M.; Lee, J.C.; Kasper, D.L. Bacteroides Fragilis–Stimulated Interleukin-10 Contains Expanding Disease. J. Infect. Dis. 2011, 204, 363–371. [Google Scholar] [CrossRef]
- Round, J.L.; Mazmanian, S.K. Inducible Foxp3+ Regulatory T-Cell Development by a Commensal Bacterium of the Intestinal Microbiota. Proc. Natl. Acad. Sci. USA 2010, 107, 12204–12209. [Google Scholar] [CrossRef] [Green Version]
- Wood, K.J.; Bushell, A.; Hester, J. Regulatory Immune Cells in Transplantation. Nat. Rev. Immunol. 2012, 12, 417–430. [Google Scholar] [CrossRef]
- Sampaio-Maia, B.; Simões-Silva, L.; Pestana, M.; Araujo, R.; Soares-Silva, I.J. The Role of the Gut Microbiome on Chronic Kidney Disease. Adv. Appl. Microbiol. 2016, 96, 65–94. [Google Scholar] [CrossRef]
- Vaziri, N.D. Gut Microbial Translocation in the Pathogenesis of Systemic Inflammation in Patients with End-Stage Renal Disease. Dig. Dis. Sci. 2014, 59, 2020–2022. [Google Scholar] [CrossRef]
- Wang, X.; Yang, S.; Li, S.; Zhao, L.; Hao, Y.; Qin, J.; Zhang, L.; Zhang, C.; Bian, W.; Zuo, L.; et al. Aberrant Gut Microbiota Alters Host Metabolome and Impacts Renal Failure in Humans and Rodents. Gut 2020, 69, 2131–2142. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, W.M.; Valujskikh, A.; Fairchild, R.L. Mechanisms of Antibody-Mediated Acute and Chronic Rejection of Kidney Allografts. Curr. Opin. Organ Transplant. 2016, 21, 7. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Hansrivijit, P.; Leeaphorn, N.; Acharya, P.; Torres-Ortiz, A.; Kaewput, W.; Kovvuru, K.; Kanduri, S.R.; Bathini, T.; Cheungpasitporn, W. Recent Advances and Clinical Outcomes of Kidney Transplantation. J. Clin. Med. 2020, 9, 1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glorieux, G.; Gryp, T.; Perna, A. Gut-Derived Metabolites and Their Role in Immune Dysfunction in Chronic Kidney Disease. Toxins 2020, 12, 245. [Google Scholar] [CrossRef] [Green Version]
- Gryp, T.; Huys, G.R.B.; Joossens, M.; van Biesen, W.; Glorieux, G.; Vaneechoutte, M. Isolation and Quantification of Uremic Toxin Precursor-Generating Gut Bacteria in Chronic Kidney Disease Patients. Int. J. Mol. Sci. 2020, 21, 1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores-Guerrero, J.L.; Osté, M.C.J.; Baraldi, P.B.; Connelly, M.A.; Garcia, E.; Navis, G.; Bakker, S.J.L.; Dullaart, R.P.F. Association of Circulating Trimethylamine N-Oxide and Its Dietary Determinants with the Risk of Kidney Graft Failure: Results of the TransplantLines Cohort Study. Nutrients 2021, 13, 262. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.T.; Shu, K.H.; Cheng, C.H.; Wu, M.J.; Yu, T.M.; Chuang, Y.W.; Chen, C.H. Serum Total P-Cresol and Indoxyl Sulfate Correlated With Stage of Chronic Kidney Disease in Renal Transplant Recipients. Transplant. Proc. 2012, 44, 621–624. [Google Scholar] [CrossRef]
- Guida, B.; Cataldi, M.; Memoli, A.; Trio, R.; di Maro, M.; Grumetto, L.; Capuano, I.; Federico, S.; Pisani, A.; Sabbatini, M. Effect of a Short-Course Treatment with Synbiotics on Plasma p-Cresol Concentration in Kidney Transplant Recipients. J. Am. Coll. Nutr. 2017, 36, 586–591. [Google Scholar] [CrossRef] [Green Version]
- Liabeuf, S.; Desjardins, L.; Massy, Z.A.; Brazier, F.; Westeel, P.F.; Mazouz, H.; Titeca-Beauport, D.; Diouf, M.; Glorieux, G.; Vanholder, R.; et al. Levels of Indoxyl Sulfate in Kidney Transplant Patients, and the Relationship With Hard Outcomes. Circ. J. 2016, 80, 722–730. [Google Scholar] [CrossRef] [Green Version]
- Liabeuf, S.; Laville, S.M.; Glorieux, G.; Cheddani, L.; Brazier, F.; Beauport, D.T.; Valholder, R.; Choukroun, G.; Massy, Z.A. Difference in Profiles of the Gut-Derived Tryptophan Metabolite Indole Acetic Acid between Transplanted and Non-Transplanted Patients with Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 2031. [Google Scholar] [CrossRef]
- Campbell, P.M.; Humphreys, G.J.; Summers, A.M.; Konkel, J.E.; Knight, C.G.; Augustine, T.; McBain, A.J. Does the Microbiome Affect the Outcome of Renal Transplantation? Front. Cell. Infect. Microbiol. 2020, 10, 794. [Google Scholar] [CrossRef]
- Kim, J.E.; Kim, H.E.; Cho, H.; Park, J.I.; Kwak, M.J.; Kim, B.Y.; Yang, S.H.; Lee, J.P.; Kim, D.K.; Joo, K.W.; et al. Effect of the Similarity of Gut Microbiota Composition between Donor and Recipient on Graft Function after Living Donor Kidney Transplantation. Sci. Rep. 2020, 10, 18881. [Google Scholar] [CrossRef] [PubMed]
- Tabibian, J.H.; Kenderian, S.S. The Microbiome and Immune Regulation after Transplantation. Transplantation 2017, 101, 56. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, M.; Pirozzolo, I.; Alegre, M.L. Impact of the Microbiota on Solid Organ Transplant Rejection. Curr. Opin. Organ Transplant. 2019, 24, 679. [Google Scholar] [CrossRef] [PubMed]
- Mendes, V.; Galvão, I.; Vieira, A.T. Mechanisms by Which the Gut Microbiota Influences Cytokine Production and Modulates Host Inflammatory Responses. J. Interferon Cytokine Res. 2019, 39, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Schirmer, M.; Smeekens, S.P.; Vlamakis, H.; Jaeger, M.; Oosting, M.; Franzosa, E.A.; Jansen, T.; Jacobs, L.; Bonder, M.J.; Kurilshikov, A.; et al. Linking the Human Gut Microbiome to Inflammatory Cytokine Production Capacity. Cell 2016, 167, 1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, S.; Cao, C.; Pascoe, E.M.; Johnson, D.W.; Shah, A.; Holtmann, G.A.; Campbell, S.B.; Francis, R.S.; Isbel, N.M.; Hawley, C.M. Patient-Reported Gastrointestinal Symptoms and the Association With Quality of Life Following Kidney Transplantation. Kidney Int. Rep. 2021, 6, 138–145. [Google Scholar] [CrossRef]
- Bunnapradist, S.; Lentine, K.L.; Burroughs, T.E.; Pinsky, B.W.; Hardinger, K.L.; Brennan, D.C.; Schnitzler, M.A. Mycophenolate Mofetil Dose Reductions and Discontinuations after Gastrointestinal Complications Are Associated with Renal Transplant Graft Failure. Transplantation 2006, 82, 102–107. [Google Scholar] [CrossRef]
- Hollyer, I.; Ison, M.G. The Challenge of Urinary Tract Infections in Renal Transplant Recipients. Transpl. Infect. Dis. 2018, 20, e12828. [Google Scholar] [CrossRef]
- Haak, B.W.; Littmann, E.R.; Chaubard, J.L.; Pickard, A.J.; Fontana, E.; Adhi, F.; Gyaltshen, Y.; Ling, L.; Morjaria, S.M.; Peled, J.U.; et al. Impact of Gut Colonization with Butyrate-Producing Microbiota on Respiratory Viral Infection Following Allo-HCT. Blood 2018, 131, 2978. [Google Scholar] [CrossRef] [PubMed]
- Bunnapradist, S.; Neri, L.; Wong, W.; Lentine, K.L.; Burroughs, T.E.; Pinsky, B.W.; Takemoto, S.K.; Schnitzler, M.A. Incidence and Risk Factors for Diarrhea Following Kidney Transplantation and Association With Graft Loss and Mortality. Am. J. Kidney Dis. 2008, 51, 478–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baghai Arassi, M.; Zeller, G.; Karcher, N.; Zimmermann, M.; Toenshoff, B. The Gut Microbiome in Solid Organ Transplantation. Pediatr. Transplant. 2020, 24, e13866. [Google Scholar] [CrossRef] [PubMed]
- Dudzicz, S.; Kujawa-Szewieczek, A.; Kwiecień, K.; Więcek, A.; Adamczak, M. Lactobacillus Plantarum 299v Reduces the Incidence of Clostridium Difficile Infection in Nephrology and Transplantation Ward-Results of One Year Extended Study. Nutrients 2018, 10, 1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, H.K.; Lee, C.G.; So, J.S.; Chae, C.S.; Hwang, J.S.; Sahoo, A.; Nam, J.H.; Rhee, J.H.; Hwang, K.C.; Im, S.H. Generation of Regulatory Dendritic Cells and CD4+Foxp3+ T Cells by Probiotics Administration Suppresses Immune Disorders. Proc. Natl. Acad. Sci. USA 2010, 107, 2159. [Google Scholar] [CrossRef] [Green Version]
- Defilipp, Z.; Bloom, P.P.; Soto, M.T.; Mansour, M.K.; Sater, M.R.A.; Huntley, M.H.; Turbett, S.; Chung, R.T.; Chen, Y.-B.; Hohmann, E.L. Drug-Resistant E. Coli Bacteremia Transmitted by Fecal Microbiota Transplant. New Engl. J. Med. 2019, 381, 2043–2050. [Google Scholar] [CrossRef]


{kind=link}
| Study Population | Sample | Method of Detection | Gut Microbiota Abundance after KT | Reference | |
|---|---|---|---|---|---|
| KTRs (N = 16) HD (N = 84) HC (N = 53) | Feces | V3 16SrRNA sequencing; Ion Personal Genome Machine | Family: ↑ Enterobacteriaceae Genus: ↑ Bacteroides | ↓ Ruminococcaceae ↓ Lachnospira ↓ Faecalibacterium | [4] |
| KTRs (N = 139) HC (N = 105) | Feces | V4-V5 16SrRNA sequencing; Illumina MiSeq | Phylum: ↑ Proteobacteria Species: ↑ Escherichia coli ↑ Streptococcus thermophilus ↑ Streptococcus mitis ↑ Streptococcus parasanguinis ↑ Blautia faecis ↑ Blautia glucerasea | ↓ Actinobacteria ↓ Bifidobacterium spp. ↓ Ruminococcus bromii ↓ Faecalibacterium prausnitzii ↓ Coprococcus eutactus ↓ Eubacterium siraeum ↓ Eubacterium rectale ↓ Dorea longicatena ↓ Coprococcus catus ↓ Coprococcus comes ↓ Roseburia sp. | [5] |
| KTRs (N = 40) HC (N = 18) | Feces | V3-V4 16SrRNA sequencing; Illumina MiSeq | Phylum: ↑ Proteobacteria Genus: ↑ Bacteroides ↑ Faecalibacterium ↑ Escherichia/Shigella ↑ Roseburia ↑ Succinivibrio | ↓ Actinobacteria ↓ Verrucomicrobia ↓ Ruminococcaceae UCG.002 ↓ Clostridium sensu strico 1 ↓ Subdoligranulum ↓ Dialister ↓ Parabacteroides ↓ Alistipes ↓ Prevotella 9 | [6] |
| KTRs (N = 26) | Feces | V4-V5 16SrRNA sequencing; Illumina MiSeq | Phylum: ↑ Proteobacteria Order: ↑ Erysipelotrichales ↑ Enterobacteriales | ↓ Bacteroidetes | [7] |
| KTRs (N = 10) | Feces | V4-V5 16SrRNA sequencing; Illumina MiSeq | Class: ↑ Bacilli Order: Family: ↑ Enterococcaceae Genus: ↑ Enterococcus ↑Anaerostipes | ↓ Clostridiales ↓ Ruminococcaceae ↓ Veillonellaceae ↓ Faecalibacterium | [8] |
| KTRs (N = 15) Donors (N = 15) | Feces | Metagenomic sequencing; Illumina NovaSeq 6000 | Family: Genus: ↑ Roseburia ↑ Streptococcus ↑ Oscillibacter ↑ Romboutsia ↑ Pauljensenia Species: ↑ Roseburia intestinalis ↑ Faecalibacterium prausnitzii | ↓ Acutalibacteracae ↓ Rikenellacea | [9] |
| Post-Transplant Setting | Study Population | Graft Time | Gut Bacteria Involved | Outcome | Reference | |
|---|---|---|---|---|---|---|
| TAC Dosing | KTRs (N = 19) | 1 month | ↑ Faecalibacterium prausnitzii | Increased abundance positively correlated with increased TAC dose requirements. | [3] | |
| Infection | KTRs (N = 26) - Infection (N = 3) | 3 months | ↑ Enterococcus | Increased abundance associated with the development of Enterococcus UTI. | [7] | |
| Diarrhea | - Diarrhea (N = 6) - No Diarrhea (N = 9) | ↓ Bacteroides ↓ Ruminococcus ↓ Coprococcus ↓ Dorea | Decreased abundance associated with the development of post-transplant diarrhea. | |||
| Rejection | Rejection (N = 3) | ↑ Lactobacillales ↑ Enterococcus ↑ Anaerofilum ↑ Clostridium tertium | ↓ Clostridiales ↓ Bacteroidales ↓ Lachnospiraceae ↓ Blautia ↓ Eubacterium dolichum ↓ Ruminococcus | Changes in the relative abundance associated with the development of acute rejection. | ||
| Rejection | KTRs (N = 53) - KTRs ABMR (N = 24) - KTRs No ABMR (N = 29) | ↑ Coprobacillus ↑ Serratia ↑ Thermus ↑ Atopobium ↑ Enterococcus ↑ Rothia ↑ Granulicatella ↑ Enterobacter ↑ Eubacterium ↑ Epulopiscium | ↓ Clostridiales ↓ Barnesiellaceae ↓ Paraprevotellaceae ↓ Pasteurellaceae ↓ Roseburia ↓ Haemophilus ↓ Faecalibacterium ↓ Paraprevotella | Gut microbiota alterations associated with ABMR. | [10] | |
| TAC Metabolism | In vitro (microbial culture) | - Faecalibacterium prausnitzii (Clostridiales) - Erysipelotrichales - Bacteroidales | Taxa able to metabolize TAC into a less effective immunosuppressant metabolite (M1). | [11] | ||
| TAC Metabolism | KTRs (N = 10) | Gut bacteria | Active metabolism of TAC by the gut bacteria. The gut microbiota could impact TAC trough variability. | [12] | ||
| Infection | KTRs (N = 60) - Infection (N = 4) - No infection (N = 14) | 6 months | ↓ Clostridiales ↓ Mogibacterium ↓ Peptoniphilus ↓ Coriobacterineae | Changes in the relative abundance associated with the development of infections after six months post transplantation. | [13] | |
| Rejection | - Rejection (N = 4) - No rejection (N = 14) | ↓ Anaerotruncus ↓ Coprobacillus ↓ Coprococcus ↓ Peptostreptococcaceae sp. | Decreased relative abundance correlated with future development of rejection events. | |||
| Infection | KTRs (N = 168)* | 3 months | ↑ Escherichia ↑ Enterococcus | Increased abundance associated with the development of Escherichia and Enterococcus bacteriuria. | [14] | |
| Infection | KTRs (N = 168)* | 3 months | ↑ Faecalibacterium ↑ Romboutsia | Increased abundance associated with lower risk of Enterobacteriaceae bacteriuria and UTI. | [15] | |
| ↑ Lactobacillus | Increased abundance associated with higher risk of Enterobacteriaceae bacteriuria and UTI. | |||||
| Infection | KTRs (N = 168)* | 3 months | Butyrate-producing bacteria | A relative abundance higher than 1% associated with lower risk of respiratory viral infection and CMV viremia. | [16] | |
| Diarrhea | KTRs (N = 64) - Diarrhea (N = 18) - No Diarrhea (N = 46) | 3 months | ↑ Enterococcus ↑ Escherichia ↑ Lachnoclostridium | ↓ Eubacterium ↓ Anaerostipes ↓ Coprococcus ↓ Romboutsia ↓ Ruminococcus ↓ Dorea ↓ Faecalibacterium ↓ Fusicatenibacter ↓ Oscillibacter ↓ Ruminiclostridium ↓ Blautia ↓ Bifidobacterium ↓ Bacteroides | Changes in the relative abundance associated with the development of diarrhea. | [17] |
| Diarrhea | KTRs (N = 79) - Diarrhea (N = 22) - No Diarrhea (N = 57) | 3 months | ↓ Eubacterium ↓ Anaerostipes ↓ Ruminococcus ↓ Dorea ↓ Fusicatenibacter V Ruminiclostridium ↓ Bifidobacterium | Decreased relative abundance associated with the development of non-infectious diarrhea. | [18] | |
| - Subdoligranulum - Coprococcus - Tyzzerella - Erysipelotrichaceae sp. | Relative abundance associated with β-glucuronidase activity, which in turn is associated with prolonged diarrhea. | |||||
| NODAT | KTRs (N = 50) - NODAT (N = 15) - Initial Diabetes (N = 16) - No Diabetes (N = 19) | 9 months | ↑ Lactobacillus sp. | ↓Akkermansia muciniphila | Changes in the relative abundance associated with the development of NODAT. | [19] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Martínez, Y.; Borriello, M.; Capolongo, G.; Ingrosso, D.; Perna, A.F. The Gut Microbiota in Kidney Transplantation: A Target for Personalized Therapy? Biology 2023, 12, 163. https://doi.org/10.3390/biology12020163
García-Martínez Y, Borriello M, Capolongo G, Ingrosso D, Perna AF. The Gut Microbiota in Kidney Transplantation: A Target for Personalized Therapy? Biology. 2023; 12(2):163. https://doi.org/10.3390/biology12020163
Chicago/Turabian StyleGarcía-Martínez, Yuselys, Margherita Borriello, Giovanna Capolongo, Diego Ingrosso, and Alessandra F. Perna. 2023. "The Gut Microbiota in Kidney Transplantation: A Target for Personalized Therapy?" Biology 12, no. 2: 163. https://doi.org/10.3390/biology12020163