
The Effects of Silicone Enclosure Colour on the Function of Optical Sensors



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Phantom Preparation
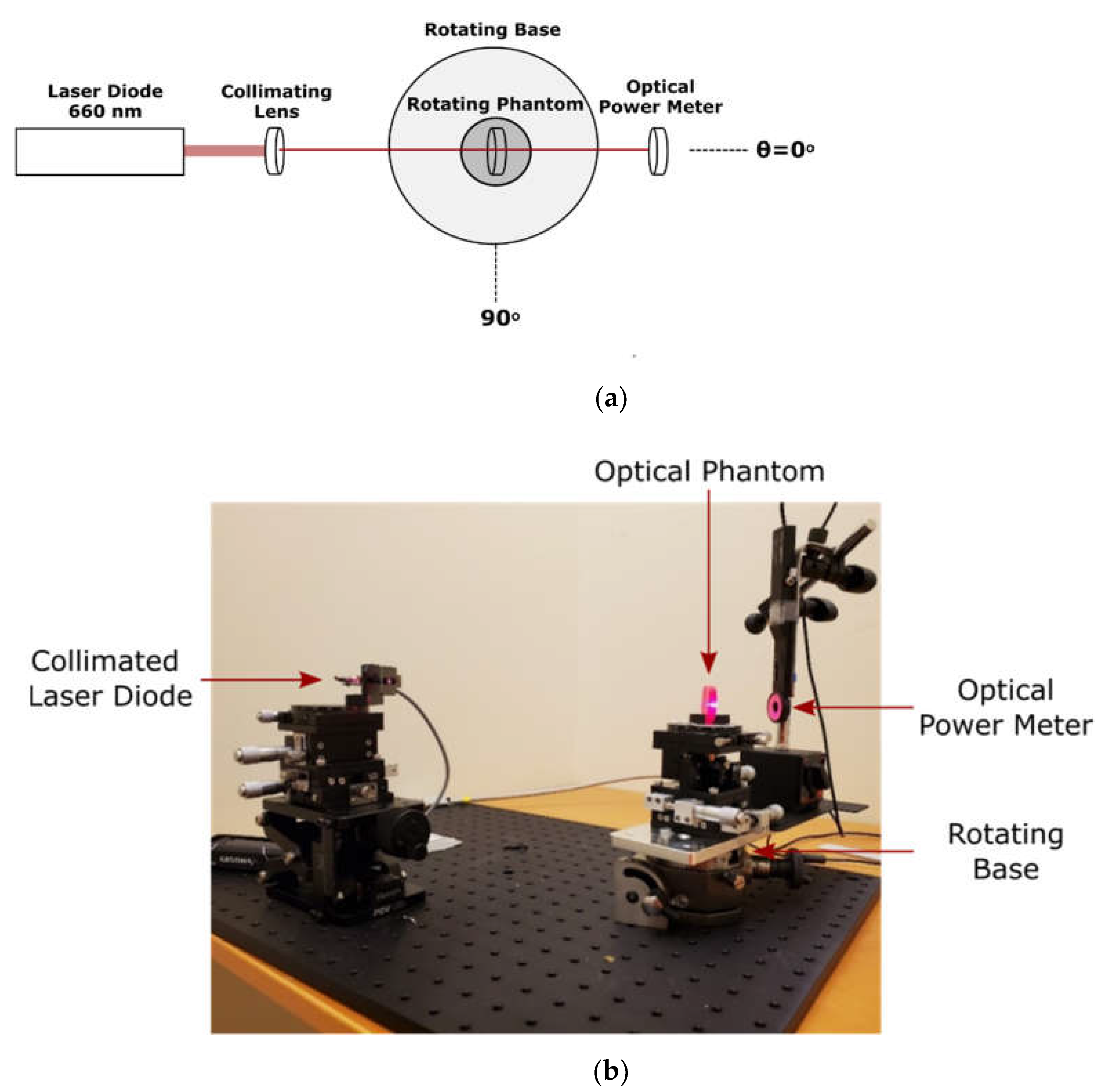
2.2. Direct Optical Measurement of Silicone Phantoms
2.3. Benchtop Tissue Oxygenation Measurements
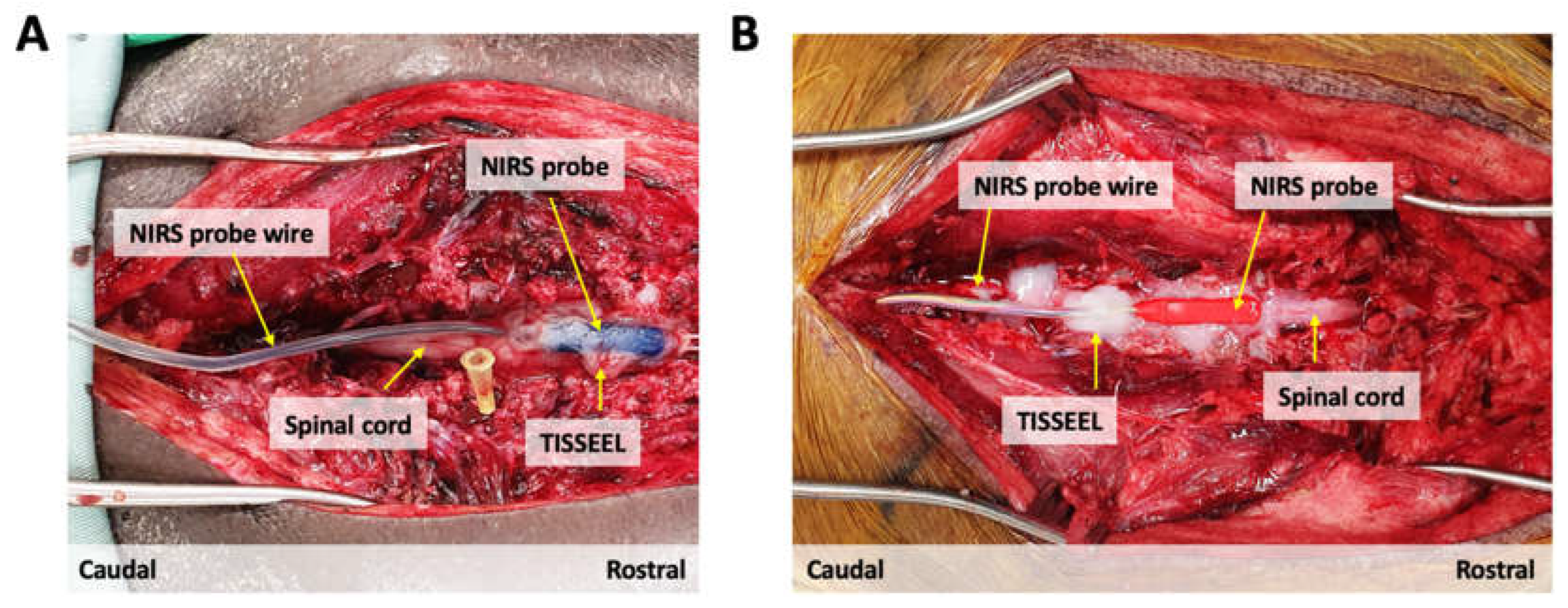
2.4. Animal Experiments
3. Results
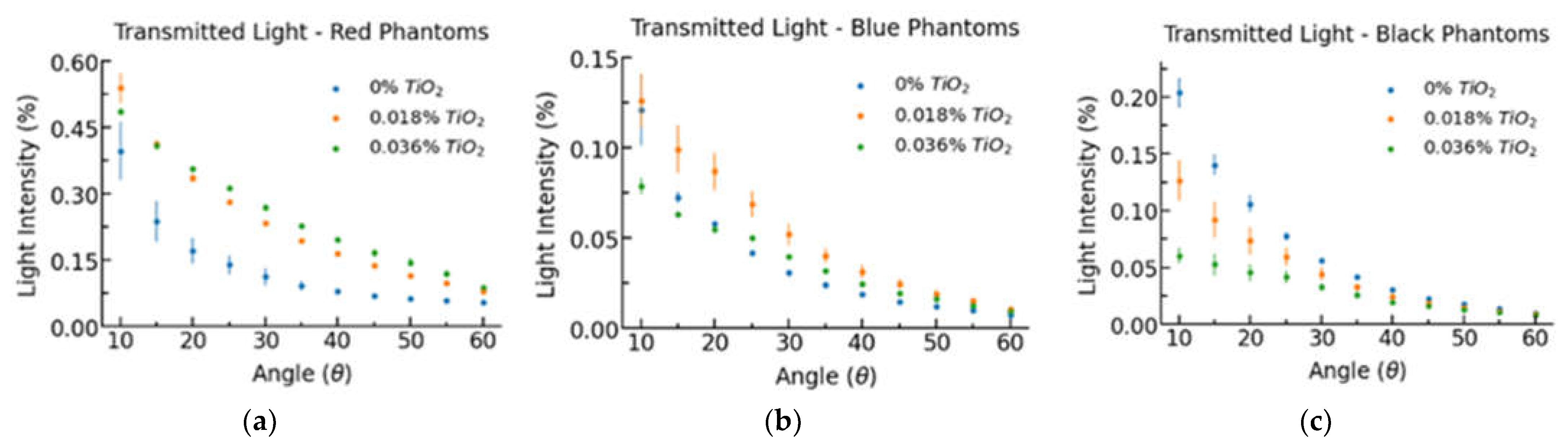
3.1. Direct Measurement
3.2. Benchtop Tissue Oxygenation Measurement
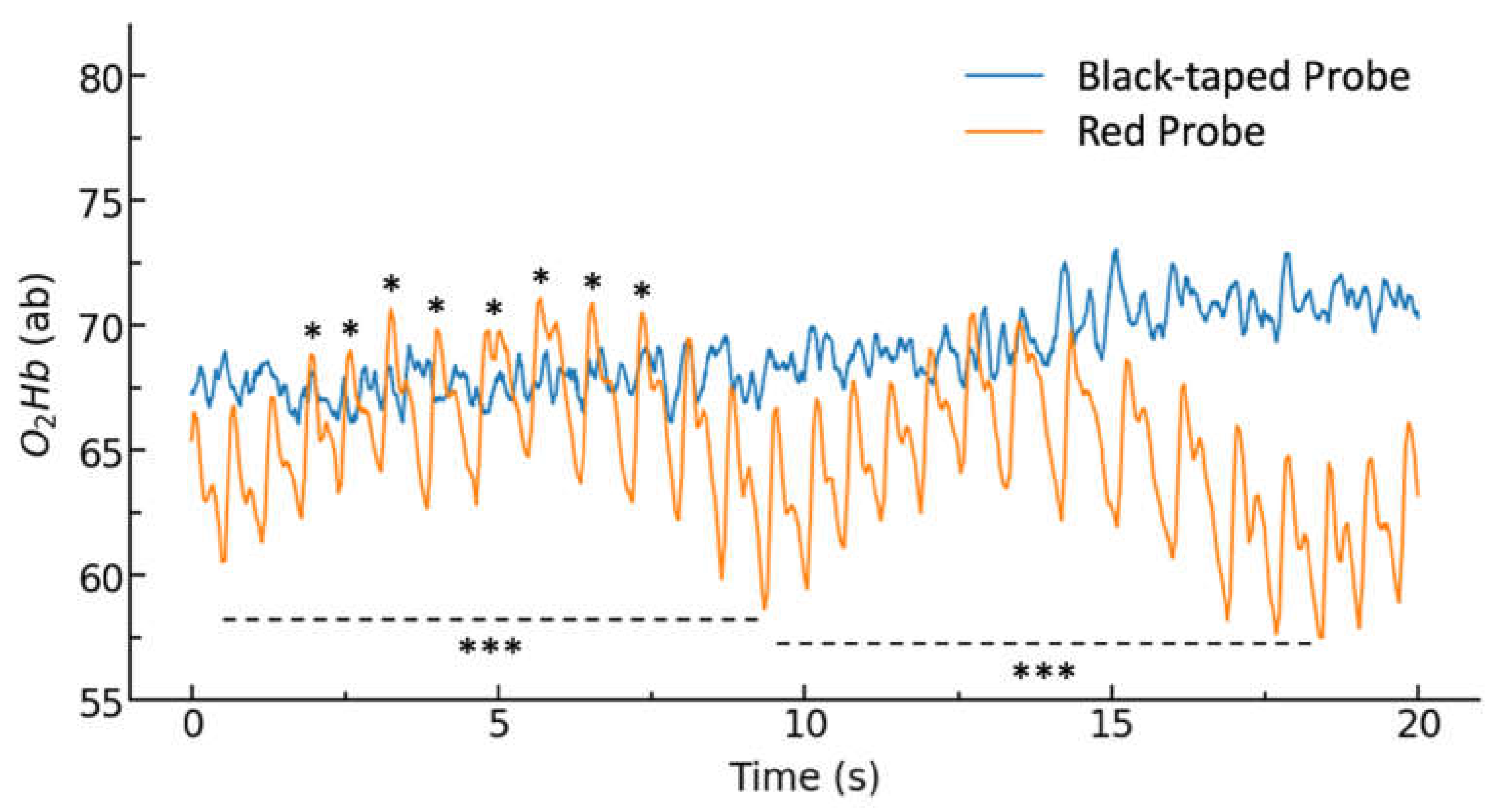
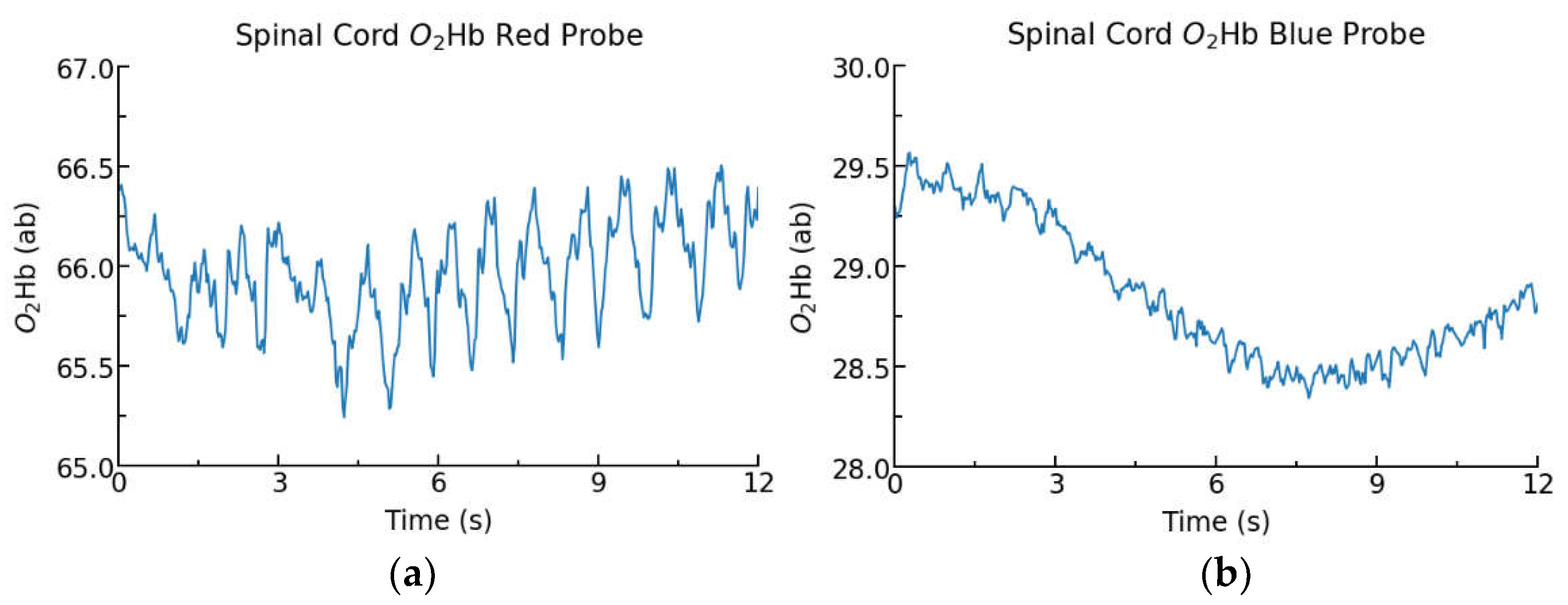
3.3. Animal Experiments
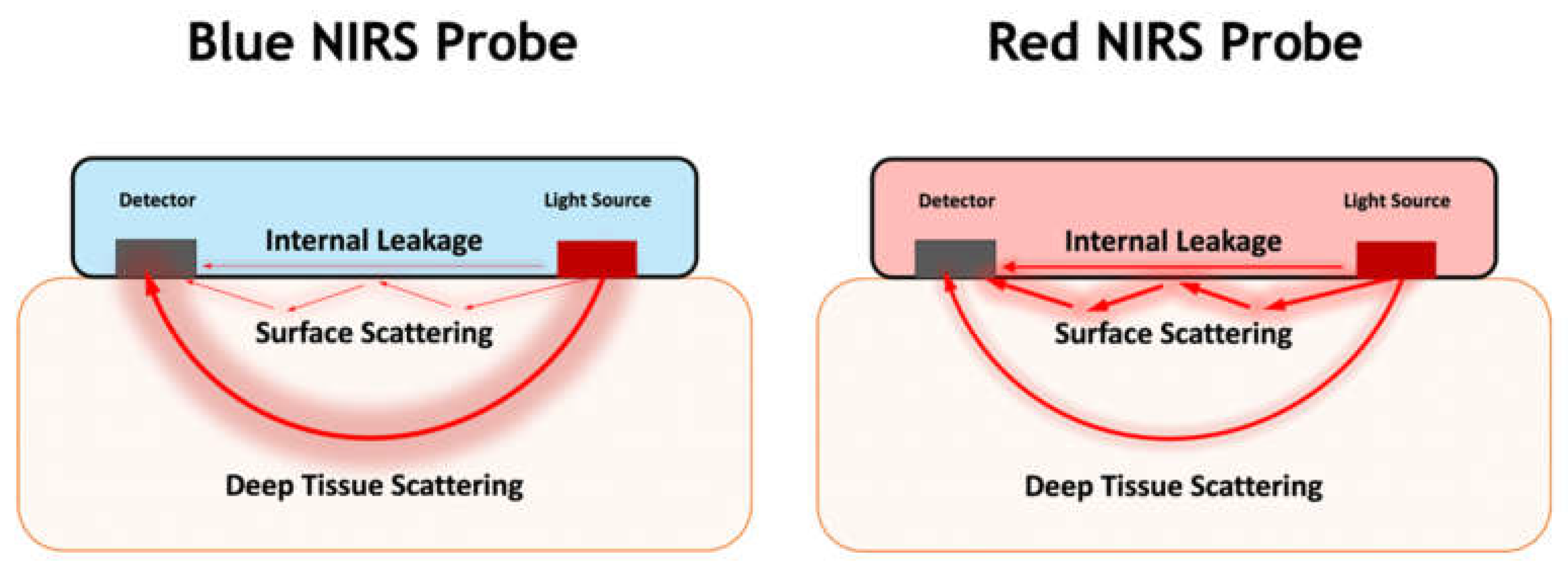
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Damborský, P.; Švitel, J.; Katrlík, J. Optical Biosensors. Essays Biochem. 2016, 60, 91–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Wang, J. Optical Biosensors: An Exhaustive and Comprehensive Review. Analyst 2020, 145, 1605–1628. [Google Scholar] [CrossRef] [PubMed]
- Windmiller, J.R.; Wang, J. Wearable Electrochemical Sensors and Biosensors: A Review. Electroanalysis 2013, 25, 29–46. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R.; Rab, S. Biosensors Applications in Medical Field: A Brief Review. Sens. Int. 2021, 2, 100100. [Google Scholar] [CrossRef]
- Kim, J.; Campbell, A.S.; de Ávila, B.E.-F.; Wang, J. Wearable Biosensors for Healthcare Monitoring. Nat. Biotechnol. 2019, 37, 389–406. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.; Barbosa, A.I.; Rebelo, R.; Kwon, I.K.; Reis, R.L.; Correlo, V.M. Skin-Integrated Wearable Systems and Implantable Biosensors: A Comprehensive Review. Biosensors 2020, 10, 79. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.; Meehan, J.; Ward, C.; Langdon, S.P.; Kunkler, I.H.; Murray, A.; Argyle, D. Implantable Biosensors and Their Contribution to the Future of Precision Medicine. Vet. J. 2018, 239, 21–29. [Google Scholar] [CrossRef]
- Córcoles, E.P.; Boutelle, M.G. Implantable Biosensors. In Biosensors and Invasive Monitoring in Clinical Applications; Córcoles, E.P., Boutelle, M.G., Eds.; Springer Briefs in Applied Sciences and Technology; Springer International Publishing: Berlin/Heidelberg, Germany, 2013; pp. 21–41. ISBN 978-3-319-00360-3. [Google Scholar]
- Bhunia, S.K.; Cinbis, C. Implanted Near-Infrared Spectroscopy for Cardiac Monitoring. In Proceedings of the Optical Tomography and Spectroscopy of Tissue IX, San Francisco, CA, USA, 17 February 2011; Volume 7896, pp. 561–568. [Google Scholar]
- Hui, P.-C.; Shtyrkova, K.; Zhou, C.; Chen, X.; Chodosh, J.; Dohlman, C.H.; Paschalis, E.I. Implantable Self-Aligning Fiber-Optic Optomechanical Devices for in Vivo Intraocular Pressure-Sensing in Artificial Cornea. J. Biophotonics 2020, 13, e202000031. [Google Scholar] [CrossRef]
- Delpy, D.T.; Cope, M.; van der Zee, P.; Arridge, S.; Wray, S.; Wyatt, J. Estimation of Optical Pathlength through Tissue from Direct Time of Flight Measurement. Phys. Med. Biol. 1988, 33, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Themelis, G.; D’Arceuil, H.; Diamond, S.G.; Thaker, S.; Huppert, T.J.; Boas, D.A.; Franceschini, M.A. Near-Infrared Spectroscopy Measurement of the Pulsatile Component of Cerebral Blood Flow and Volume from Arterial Oscillations. J. Biomed. Opt. 2007, 12, 014033. [Google Scholar] [CrossRef]
- Li, P.; Lee, G.-H.; Kim, S.Y.; Kwon, S.Y.; Kim, H.-R.; Park, S. From Diagnosis to Treatment: Recent Advances in Patient-Friendly Biosensors and Implantable Devices. ACS Nano 2021, 15, 1960–2004. [Google Scholar] [CrossRef] [PubMed]
- Ben Amar, A.; Kouki, A.B.; Cao, H. Power Approaches for Implantable Medical Devices. Sensors 2015, 15, 28889–28914. [Google Scholar] [CrossRef] [PubMed]
- Fiala, J.; Gehrke, R.; Weber, N.; Bingger, P.; Zappe, H.; Seifert, A. Implantable Optical Sensor for Continuous Monitoring of Various Hemoglobin Derivatives and Tissue Perfusion. In Proceedings of the 2009 IEEE SENSORS, Christchurch, New Zealand, 25–28 October 2009; pp. 1971–1974. [Google Scholar]
- Bashkatov, A.N.; Genina, E.A.; Tuchin, V.V. Optical Properties of Skin, Subcutaneous, and Muscle Tissues: A Review. J. Innov. Opt. Health Sci. 2011, 4, 9–38. [Google Scholar] [CrossRef]
- Clancy, N.T.; Jones, G.; Maier-Hein, L.; Elson, D.S.; Stoyanov, D. Surgical Spectral Imaging. Med. Image Anal. 2020, 63, 101699. [Google Scholar] [CrossRef] [PubMed]
- Pogue, B.W.; Patterson, M.S. Review of Tissue Simulating Phantoms for Optical Spectroscopy, Imaging and Dosimetry. J. Biomed. Opt. 2006, 11, 041102. [Google Scholar] [CrossRef]
- Akarçay, H.G.; Preisser, S.; Frenz, M.; Rička, J. Determining the Optical Properties of a Gelatin-TiO2 Phantom at 780 Nm. Biomed. Opt. Express 2012, 3, 418–434. [Google Scholar] [CrossRef] [Green Version]
- Cheung, A.; Askari, S.; Sahragard, F.; Raschdorf, K.; Webster, M.; Warner, A.; Ethridge, J.; So, K.; Frank, G.; Hill, J.; et al. A Method for the Fixation of an Implantable Spinal Cord NIRS Sensor. In Proceedings of the Biophotonics in Exercise Science, Sports Medicine, Health Monitoring Technologies, and Wearables III, Online, 2 March 2022; Volume 11956, pp. 36–43. [Google Scholar]
- Streijger, F.; So, K.; Manouchehri, N.; Tigchelaar, S.; Lee, J.H.T.; Okon, E.B.; Shortt, K.; Kim, S.-E.; McInnes, K.; Cripton, P.; et al. Changes in Pressure, Hemodynamics, and Metabolism within the Spinal Cord during the First 7 Days after Injury Using a Porcine Model. J. Neurotrauma 2017, 34, 3336–3350. [Google Scholar] [CrossRef]
- Kim, K.-T.; Streijger, F.; So, K.; Manouchehri, N.; Shortt, K.; Okon, E.B.; Tigchelaar, S.; Fong, A.; Morrison, C.; Keung, M.; et al. Differences in Morphometric Measures of the Uninjured Porcine Spinal Cord and Dural Sac Predict Histological and Behavioral Outcomes after Traumatic Spinal Cord Injury. J. Neurotrauma 2019, 36, 3005–3017. [Google Scholar] [CrossRef]
- Ayers, F.; Grant, A.; Kuo, D.; Cuccia, D.; Durkin, A. Fabrication and Characterization of Silicone-Based Tissue Phantoms with Tunable Optical Properties in the Visible and near Infrared Domain. Proc SPIE 2008, 6870, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Patterson, M.S.; Wilson, B.C.; Wyman, D.R. The Propagation of Optical Radiation in Tissue. II: Optical Properties of Tissues and Resulting Fluence Distributions. Lasers Med. Sci. 1991, 6, 379–390. [Google Scholar] [CrossRef]
- Diep, P.; Pannem, S.; Sweer, J.; Lo, J.; Snyder, M.; Stueber, G.; Zhao, Y.; Tabassum, S.; Istfan, R.; Wu, J.; et al. Three-Dimensional Printed Optical Phantoms with Customized Absorption and Scattering Properties. Biomed. Opt. Express 2015, 6, 4212–4220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duadi, H.; Fixler, D. Influence of Multiple Scattering and Absorption on the Full Scattering Profile and the Isobaric Point in Tissue. J. Biomed. Opt. 2015, 20, 056010. [Google Scholar] [CrossRef] [PubMed]
- Terán, E.; Méndez, E.R.; Quispe-Siccha, R.; Peréz-Pacheco, A.; Cuppo, F.L.S. Application of Single Integrating Sphere System to Obtain the Optical Properties of Turbid Media. OSA Contin. 2019, 2, 1791–1806. [Google Scholar] [CrossRef]
- Beć, K.B.; Grabska, J.; Huck, C.W. Principles and Applications of Miniaturized Near-Infrared (NIR) Spectrometers. Chem. Eur. J. 2021, 27, 1514–1532. [Google Scholar] [CrossRef]
- Feng, Z.; Tang, T.; Wu, T.; Yu, X.; Zhang, Y.; Wang, M.; Zheng, J.; Ying, Y.; Chen, S.; Zhou, J.; et al. Perfecting and Extending the Near-Infrared Imaging Window. Light Sci. Appl. 2021, 10, 197. [Google Scholar] [CrossRef]
- Maeda, Y.; Sekine, M.; Tamura, T. The Advantages of Wearable Green Reflected Photoplethysmography. J. Med. Syst. 2011, 35, 829–834. [Google Scholar] [CrossRef]
- Nguyen, H.-D.; Yoo, S.-H.; Bhutta, M.R.; Hong, K.-S. Adaptive Filtering of Physiological Noises in FNIRS Data. Biomed. Eng. OnLine 2018, 17, 180. [Google Scholar] [CrossRef] [Green Version]
- Simone, G.; Tordera, D.; Delvitto, E.; Peeters, B.; van Breemen, A.J.J.M.; Meskers, S.C.J.; Janssen, R.A.J.; Gelinck, G.H. High-Accuracy Photoplethysmography Array Using Near-Infrared Organic Photodiodes with Ultralow Dark Current. Adv. Opt. Mater. 2020, 8, 1901989. [Google Scholar] [CrossRef] [Green Version]
- Malakasioti, G.; Marks, S.D.; Watson, T.; Williams, F.; Taylor-Allkins, M.; Mamode, N.; Morgan, J.; Hayes, W.N. Continuous Monitoring of Kidney Transplant Perfusion with Near-Infrared Spectroscopy. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2018, 33, 1863–1869. [Google Scholar] [CrossRef]
- Lau, H.; Lopez, A.J.; Eguchi, N.; Shimomura, A.; Ferrey, A.; Tantisattamo, E.; Reddy, U.; Dafoe, D.; Ichii, H. Intraoperative Near-Infrared Spectroscopy Monitoring of Renal Allograft Reperfusion in Kidney Transplant Recipients: A Feasibility and Proof-of-Concept Study. J. Clin. Med. 2021, 10, 4292. [Google Scholar] [CrossRef]
- Stolik, S.; Delgado, J.A.; Pérez, A.; Anasagasti, L. Measurement of the Penetration Depths of Red and near Infrared Light in Human “Ex Vivo” Tissues. J. Photochem. Photobiol. B 2000, 57, 90–93. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dye Concentration | TiO2 Concentration | ||
|---|---|---|---|
| None | Low | High | |
| 0.27% Red (PMS 186C) | 0% | 0.018% | 0.036% |
| 0.27% Blue (PMS 2757C) | 0% | 0.018% | 0.036% |
| 0.27% Black (PMS Black) | 0% | 0.018% | 0.036% |
| Colour | Attenuation Coefficient (mm−1) | ||
|---|---|---|---|
| 0% TiO2 | 0.018% TiO2 | 0.036% TiO2 | |
| Red | 0.102 ± 0.017 | 0.260 ± 0.011 | 0.444 ± 0.020 |
| Blue | 0.366 ± 0.009 | 0.542 ± 0.039 | 0.805 ± 0.016 |
| Black | 0.591 ± 0.011 | 0.737 ± 0.013 | 0.978 ± 0.040 |
| Probe | Raw Photodetector Values (mV) | ||||
|---|---|---|---|---|---|
| 950 nm | 730 nm | 810 nm | 850 nm | 650 nm | |
| Red | 3800 | 3800 | 3800 | 3800 | 3800 |
| Black-taped | 600 | 550 | 500 | 500 | 450 |
| Participant | Condition | Cardiac Pulsation Amplitude (ab) | Cardiac Pulsation Width (s) | ||||
|---|---|---|---|---|---|---|---|
| Trial 1 | Trial 2 | Trial 3 | Trial 1 | Trial 2 | Trial 3 | ||
| P1 | Red Probe | 6.43 ± 0.55 | 13.29 ± 1.23 | 10.16 ± 1.15 | 0.74 ± 0.10 | 0.77 ± 0.13 | 0.68 ± 0.09 |
| Black-Taped | 2.29 ± 0.64 | 8.42 ± 1.17 | 1.94 ± 0.51 | 0.71 ± 0.18 | 0.81 ± 0.08 | 0.60 ± 0.18 | |
| P2 | Red Probe | 6.64 ± 0.38 | 5.17 ± 0.45 | 3.50 ± 0.56 | 0.82 ± 0.04 | 0.75 ± 0.04 | 0.79 ± 0.05 |
| Black-Taped | 2.64 ± 0.48 | 3.27 ± 0.91 | 2.26 ± 0.27 | 0.74 ± 0.14 | 0.70 ± 0.06 | 0.71 ± 0.17 | |
| Probe | LED Current (mA) | |||||
|---|---|---|---|---|---|---|
| 730 nm | 680 nm | 760 nm | 850 nm | 910 nm | Total | |
| Red | 9.4 | 20.4 | 9.4 | 9.4 | 17.3 | 65.9 |
| Blue | 51.0 | 60.0 | 31.0 | 8.0 | 8.0 | 158 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frank, G.; Askari, S.; Raschdorf, K.; Khosravi, S.; Kwon, B.K.; Shadgan, B. The Effects of Silicone Enclosure Colour on the Function of Optical Sensors. Biology 2022, 11, 932. https://doi.org/10.3390/biology11060932
Frank G, Askari S, Raschdorf K, Khosravi S, Kwon BK, Shadgan B. The Effects of Silicone Enclosure Colour on the Function of Optical Sensors. Biology. 2022; 11(6):932. https://doi.org/10.3390/biology11060932
Chicago/Turabian StyleFrank, Garrett, Shahbaz Askari, Katharina Raschdorf, Sadra Khosravi, Brian K. Kwon, and Babak Shadgan. 2022. "The Effects of Silicone Enclosure Colour on the Function of Optical Sensors" Biology 11, no. 6: 932. https://doi.org/10.3390/biology11060932