
Antimicrobial Stewardship Program for Patients in the Hematological Department Receiving Carbapenem Therapy: A Single-Center and Interrupted Time Series Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
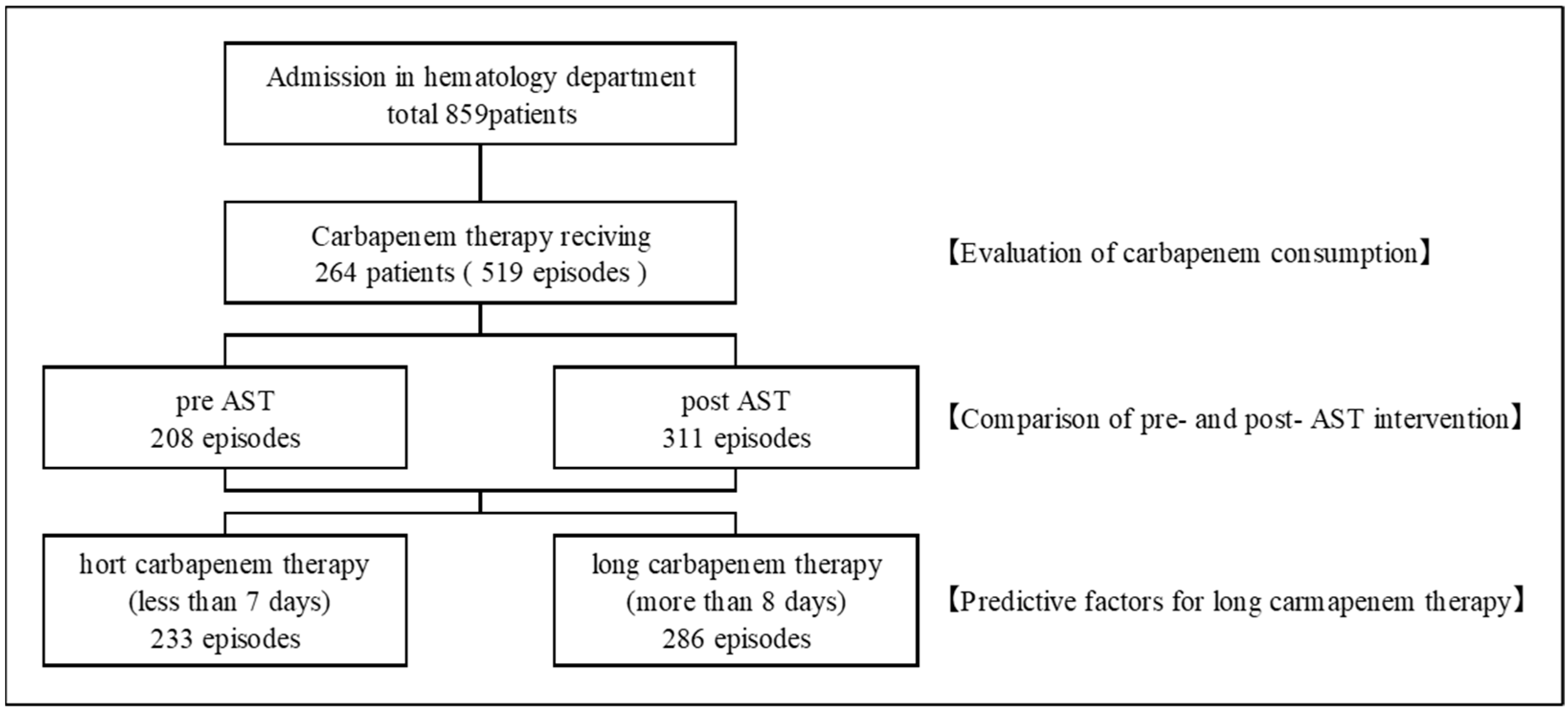
2.1. Characteristics of the Participants
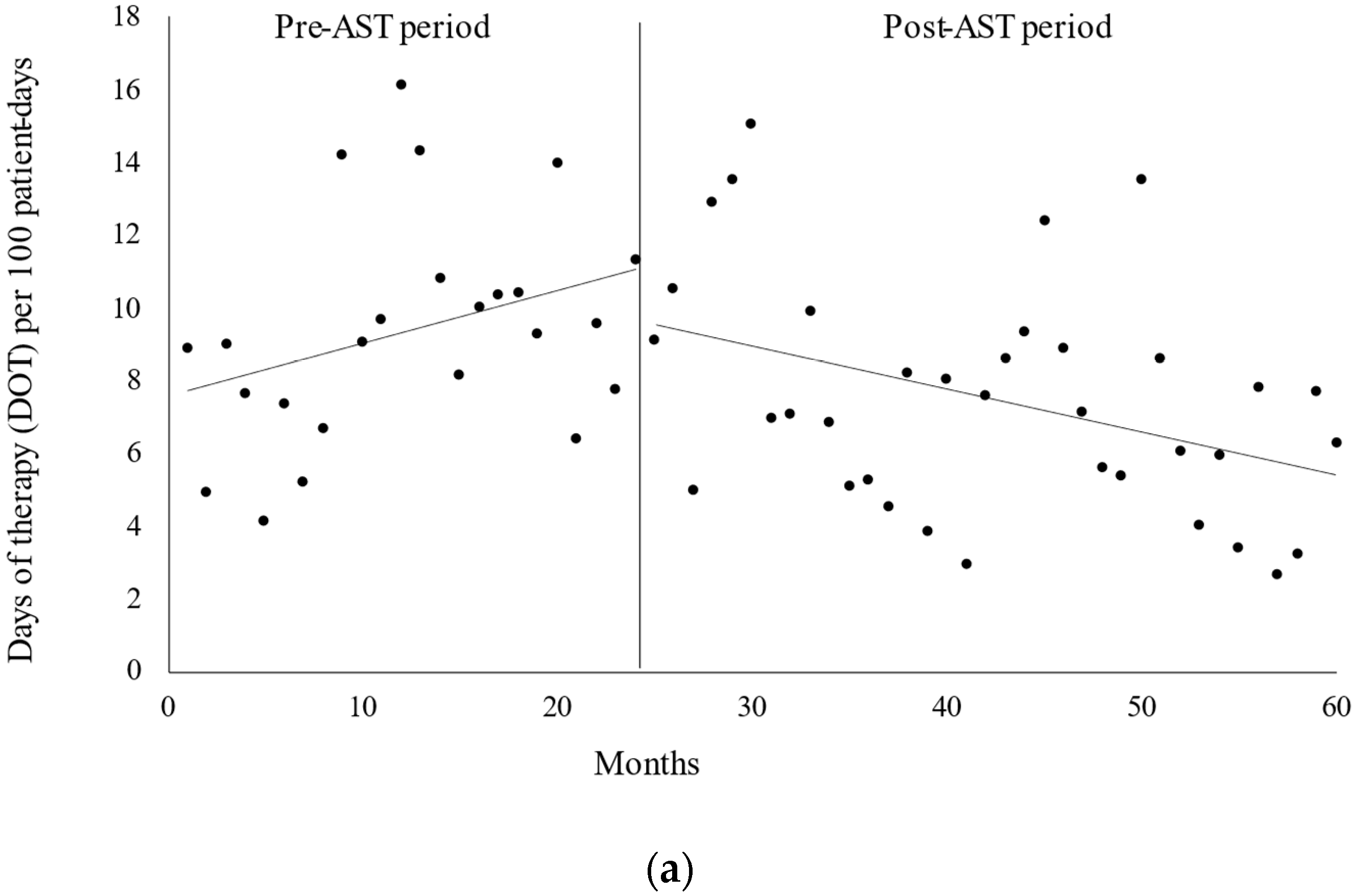
2.2. Carbapenem Consumption
2.3. Comparison between Pre-AST and Post-AST Groups
2.4. Predictive Factors for Long-Term Carbapenem Therapy
3. Discussion
4. Materials and Methods
4.1. Population and Data Collection
4.2. AST Implementations
4.3. AST Policy against the Hematology Department
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freifeld, A.G.; Bow, E.J.; Sepkowitz, K.A.; Boeckh, M.J.; Ito, J.I.; Mullen, C.A.; Raad, I.I.; Rolston, K.V.; Young, J.H.; Wingard, J.R. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clin. Infect. Dis. 2011, 52, e56–e93. [Google Scholar] [CrossRef] [PubMed]
- Kuderer, N.M.; Dale, D.C.; Crawford, J.; Cosler, L.E.; Lyman, G.H. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer 2006, 106, 2258–2266. [Google Scholar] [CrossRef] [PubMed]
- Averbuch, D.; Orasch, C.; Cordonnier, C.; Livermore, D.M.; Mikulska, M.; Viscoli, C.; Gyssens, I.C.; Kern, W.V.; Klyasova, G.; Marchetti, O.; et al. ECIL4, a joint venture of EBMT, EORTC, ICHS, ESGICH/ESCMID and ELN. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: Summary of the 2011. Haematol. 4th Eur Conf. Infect. Leuk. 2013, 98, 1826–1835. [Google Scholar] [CrossRef]
- Link, H.; Böhme, A.; Cornely, O.A.; Höffken, K.; Kellner, O.; Kern, W.V.; Mahlberg, R.; Maschmeyer, G.; Nowrousian, M.R.; Ostermann, H.; et al. Antimicrobial therapy of unexplained fever in neutropenic patients—Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO), Study Group Interventional Therapy of Unexplained Fever, Arbeitsgemeinschaft Supportivmassnahmen in der Onkologie (ASO) of the Deutsche Krebsgesellschaft (DKG-German Cancer Society). Ann. Hematol. 2003, 82 (Suppl. 2), S105–S117. [Google Scholar] [CrossRef]
- Villafuerte-Gutierrez, P.; Villalon, L.; Losa, J.E.; Henriquez-Camacho, C. Treatment of febrile neutropenia and prophylaxis in hematologic malignancies: A critical review and update. Adv. Hematol. 2014, 2014, 986938. [Google Scholar] [CrossRef]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Wilson, A.P.R. Sparing carbapenem usage. J. Antimicrob. Chemother. 2017, 72, 2410–2417. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.K.; Won, S.Y. Carbapenem-sparing therapy for extended-Spectrum β-lactamase-producing E coli and Klebsiella pneumoniae bloodstream infection: The search continues. JAMA 2018, 320, 979–981. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.K.; Lo, K.; Abbo, L.M. Current state of antimicrobial stewardship at Solid Organ and Hematopoietic Cell Transplant Centers in The United States. Infect. Control Hosp. Epidemiol. 2016, 37, 1195–1200. [Google Scholar] [CrossRef]
- Webb, B.J.; Majers, J.; Healy, R.; Jones, P.B.; Butler, A.M.; Snow, G.; Forsyth, S.; Lopansri, B.K.; Ford, C.D.; Hoda, D. Antimicrobial stewardship in a hematological malignancy unit: Carbapenem reduction and decreased vancomycin-resistant enterococcus infection. Clin. Infect. Dis. 2020, 71, 960–967. [Google Scholar] [CrossRef]
- la Martire, G.L.; Robin, C.; Oubaya, N.; Lepeule, R.; Beckerich, F.; Leclerc, M.; Barhoumi, W.; Toma, A.; Pautas, C.; Maury, S.; et al. De-escalation and discontinuation strategies in high-risk neutropenic patients: An interrupted time series analyses of antimicrobial consumption and impact on outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1931–1940. [Google Scholar] [CrossRef] [PubMed]
- Gedik, H. Antibiotic resistance status and its costs in hematological patients: A two-year analysis. Casp. J. Intern. Med. 2017, 8, 276–281. [Google Scholar] [CrossRef]
- O’Horo, J.C.; Marcelin, J.R.; Abu Saleh, O.M.A.; Barwise, A.K.; Odean, P.M.; Rivera, C.G.; Tande, A.J.; Wilson, J.W.; Osmon, D.R.; Tosh, P.K. Standardizing febrile neutropenia management: Antimicrobial stewardship in the hematologic malignancy population. J. Oncol. Pr. 2019, 15, e843–e848. [Google Scholar] [CrossRef]
- Nørgaard, M.; Larsson, H.; Pedersen, G.; Schønheyder, H.C.; Sørensen, H.T. Risk of bacteraemia and mortality in patients with haematological malignancies. Clin. Microbiol. Infect. 2006, 12, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Guisado-Gil, A.B.; Aguilar-Guisado, M.; Peñalva, G.; Lepe, J.A.; Espigado, I.; Rodríguez-Arbolí, E.; González-Campos, J.; Rodríguez-Torres, N.; Montero-Cuadrado, M.I.; Falantes-González, J.F.; et al. Long-term impact of an educational antimicrobial stewardship program on management of patients with hematological diseases. Antibiotics 2021, 10, 136. [Google Scholar] [CrossRef]
- Madran, B.; Keske, Ş.; Tokça, G.; Dönmez, E.; Ferhanoğlu, B.; Çetiner, M.; Mandel, N.M.; Ergönül, Ö. Implementation of an antimicrobial stewardship program for patients with febrile neutropenia. Am. J. Infect. Control 2018, 46, 420–424. [Google Scholar] [CrossRef]
- Mardani, M.; Abolghasemi, S.; Shabani, S. Impact of an antimicrobial stewardship program in the antimicrobial-resistant and prevalence of Clostridioides difficile infection and amount of antimicrobial consumed in cancer patients. BMC Res. Notes 2020, 13, 246. [Google Scholar] [CrossRef]
- Puerta-Alcalde, P.; Cardozo, C.; Suárez-Lledó, M.; Rodríguez-Núñez, O.; Morata, L.; Fehér, C.; Marco, F.; Del Río, A.D.; Martínez, J.A.; Mensa, J.; et al. Current time-to-positivity of blood cultures in febrile neutropenia: A tool to be used in stewardship de-escalation strategies. Clin. Microbiol. Infect. 2019, 25, 447–453. [Google Scholar] [CrossRef]
- Le Clech, L.; Talarmin, J.P.; Couturier, M.A.; Ianotto, J.C.; Nicol, C.; Le Calloch, R.; Dos Santos, S.; Hutin, P.; Tandé, D.; Cogulet, V.; et al. Early discontinuation of empirical antibacterial therapy in febrile neutropenia: The ANTIBIOSTOP study. Infect. Dis. 2018, 50, 539–549. [Google Scholar] [CrossRef]
- Haynes, R.B.; Devereaux, P.J.; Guyatt, G.H. Physicians’ and patients’ choices in evidence based practice. BMJ 2002, 324, 1350. [Google Scholar] [CrossRef]
- Djulbegovic, B.; Guyatt, G.H. Progress in evidence-based medicine: A quarter century on. Lancet 2017, 390, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Peng, Y.; Wang, X.; Chen, Y.; Jin, L.; Yang, T.; Qian, M.; Ni, W.; Tong, X.; Lan, J. Incidence, survival, and risk factors for adults with acute myeloid leukemia not otherwise specified and acute myeloid leukemia with recurrent genetic abnormalities: Analysis of the surveillance, epidemiology, and end results (SEER) Database, 2001–2013. Acta Haematol. 2018, 139, 115–127. [Google Scholar] [CrossRef] [PubMed]
- De Lima, M.C.; Da Silva, D.B.; Freund, A.P.F.; Dacoregio, J.S.; Costa, T.J.; Costa, I.; Faraco, D.; Silva, M.L. Acute myeloid leukemia: Analysis of epidemiological profile and survival rate. J. Pediatr. 2016, 92, 283–289. [Google Scholar] [CrossRef]
- Kumar, S.K.; Dispenzieri, A.; Lacy, M.Q.; Gertz, M.A.; Buadi, F.K.; Pandey, S.; Kapoor, P.; Dingli, D.; Hayman, S.R.; Leung, N.; et al. Continued improvement in survival in multiple myeloma: Changes in early mortality and outcomes in older patients. Leukemia 2014, 28, 1122–1128. [Google Scholar] [CrossRef]
- Landgren, O.; Iskander, K. Modern multiple myeloma therapy: Deep, sustained treatment response and good clinical outcomes. J. Intern. Med. 2017, 281, 365–382. [Google Scholar] [CrossRef] [PubMed]
- Niessen, F.A.; van Mourik, M.S.M.; Bruns, A.H.W.; Raijmakers, R.A.P.; de Groot, M.C.H.; van der Bruggen, T. Early discontinuation of empirical antibiotic treatment in neutropenic patients with acute myeloid leukaemia and high-risk myelodysplastic syndrome. Antimicrob. Resist. Infect. Control 2020, 9, 74. [Google Scholar] [CrossRef]
- Klastersky, J.; Paesmans, M.; Rubenstein, E.B.; Boyer, M.; Elting, L.; Feld, R.; Gallagher, J.; Herrstedt, J.; Rapoport, B.; Rolston, K.; et al. The Multinational Association for Supportive Care in Cancer Risk Index: A Multinational Scoring System for Identifying Low-Risk Febrile Neutropenic Cancer Patients. J. Clin. Oncol. 2000, 18, 3038–3051. [Google Scholar] [CrossRef]
- Alberta Provincial Tumour Teams. Management of febrile neutropenia in adult cancer patients. Albertha. Health Serv. 2014, 3, 2–19. [Google Scholar]
- Sethi, S.; Murphy, T.F. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N. Engl. J. Med. 2008, 359, 2355–2365. [Google Scholar] [CrossRef]
- Havey, T.C.; Fowler, R.A.; Daneman, N. Duration of antibiotic therapy for bacteremia: A systematic review and meta-analysis. Crit. Care 2011, 15, R267. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance. Clin. Infect. Dis. 2022, 25, 187–212. [Google Scholar] [CrossRef]
- Komagamine, J.; Yabuki, T.; Hiraiwa, T. A trend in prevalence of antimicrobial use and appropriateness of antimicrobial therapy in an acute care hospital from 2018 to 2019: Repeated prevalence surveys in Japan. BMC Res. Notes 2019, 12, 811. [Google Scholar] [CrossRef] [PubMed]
- ATC/DDD Index 2022. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 11 November 2022).
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Comparative Study Revised Equations for Estimated GFR from Serum Creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, S1–S276. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Maeda, M.; Yokoe, T.; Hashiguchi, M.; Togashi, M.; Ishino, K. Impact of the multidisciplinary antimicrobial stewardship team intervention focusing on carbapenem de-escalation: A single-centre and interrupted time series analysis. Int. J. Clin. Pract. 2021, 75, e13693. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total n = 264 (Patients) | Pre-AST n = 208 (Episodes) | Post-AST n = 311 (Episodes) | p-Value |
|---|---|---|---|---|
| Age (years) | 72.5 (24.0–94.0) | 71.0 (24.0–94.0) | 71.0 (30.0–90.0) | 0.616 |
| Sex (male) | 157 (59.5) | 128 (61.5) | 167 (53.7) | 0.077 |
| BMI (kg/m2) | 20.7 (12.9–42.1) | 19.8 (12.9–40.0) | 20.9 (13.9–42.1) | <0.001 * |
| CKD † | 89 (33.7) | 96 (46.2) | 135 (43.4) | 0.537 |
| Diabetes mellitus | 31 (11.7) | 35 (16.8) | 23 (7.4) | 0.001 * |
| COPD | 7 (2.7) | 11 (5.3) | 4 (1.3) | 0.013 * |
| Hematologic disease | ||||
| Acute myeloid leukemia | 77 (29.2) | 69 (33.2) | 101 (32.5) | 0.868 |
| Myelodysplastic syndrome | 30 (11.4) | 23 (11.1) | 42 (13.5) | 0.409 |
| Acute lymphocytic leukemia | 10 (3.8) | 3 (1.4) | 20 (6.4) | 0.008 * |
| Malignant lymphoma | 84 (31.8) | 64 (30.8) | 91 (29.3) | 0.713 |
| Multiple myeloma | 21 (8.0) | 16 (7.7) | 26 (8.4) | 0.785 |
| Aplastic anemia | 8 (3.0) | 13 (6.3) | 12 (3.9) | 0.212 |
| Others | 34 (12.9) | 20 (9.6) | 19 (6.1) | 0.138 |
| Category | Consumption | Pre-AST | Post-AST | U-Value | p-Value |
|---|---|---|---|---|---|
| Carbapenem | DOT | 9.2 (4.2–16.1) | 7.1 (2.7–15.0) | 270.0 | 0.015 * |
| AUD | 8.4 (2.7–15.1) | 6.6 (2.2–15.2) | 281.0 | 0.023 * | |
| Tazobactam/piperacillin | DOT | 44.5 (4.6–73.8) | 47.4 (14.6–145.0) | 509.0 | 0.245 |
| AUD | 37.7 (3.7–75.6) | 40.8 (10.6–127.1) | 480.0 | 0.469 | |
| Fourth-generation cephalosporins | DOT | 95.2 (40.8–139.3) | 67.1 (0.0–151.2) | 271.0 | 0.015 * |
| AUD | 79.3 (37.6–121.8) | 27.7 (0.0–102.0) | 65.0 | <0.001 * | |
| Third-generation cephalosporins | DOT | 15.7 (0.0–67.8) | 56.5 (0.0–155.8) | 716.0 | <0.001 * |
| AUD | 10.0 (0.0–48.6) | 39.2 (0.0–94.2) | 715.0 | <0.001 * |
| Characteristic | Pre-AST n = 208 (Episodes) | Post-AST n = 311 (Episodes) | p-Value |
|---|---|---|---|
| Blood culture (2 sets) before starting antibiotics | 96 (46.2) | 268 (86.2) | <0.001 * |
| Blood culture positivity | 36 (17.3) | 89 (28.6) | 0.003 * |
| Nursing record about antibiotics | 7 (3.4) | 33 (10.6) | 0.002 * |
| Length of carbapenem therapy | 8 (1.0–39.0) | 8 (1.0–31.0) | 0.542 |
| Number of days not receiving carbapenem with <500 granulocytes | 0 (0.0–180) | 3 (0.0–431) | <0.001 * |
| 30-day mortality | 44 (21.2) | 59 (19.0) | 0.541 |
| In-hospital mortality | 58 (27.9) | 82 (26.4) | 0.703 |
| Length of hospital stay | 20.5 (1.0–228.0) | 20.0 (1.0–383.0) | 0.269 |
| Gram-positive cocci | 15 (7.2) | 54 (17.4) | 0.001 * |
| Variable | Short-Term Carbapenem Therapy (<7 Days) n = 233 (Episodes) | Long-Term Carbapenem Therapy (>8 Days) n = 286 (Episodes) | p-Value |
|---|---|---|---|
| AST intervention | 137 (58.8) | 174 (60.8) | 0.637 |
| Age | 72.0 (24.0–94.0) | 70 (24.0–92.0) | 0.049 * |
| eGFR (mL/min/1.73 m2) | 61.1 (5.4–318.0) | 68.3 (3.7–268.6) | 0.206 |
| Granulocytes (/µL) | 456.0 (0.0–10,510) | 162.0 (0.0–50,300.0) | 0.005 * |
| Hypotension | 23 (9.9) | 19 (6.6) | 0.180 |
| Outpatient onset | 33 (14.2) | 60 (21.0) | 0.044 * |
| Diabetes mellitus | 19 (8.2) | 39 (13.6) | 0.049 * |
| COPD | 1 (0.4) | 14 (4.9) | 0.002 * |
| Medical device | |||
| Central venous catheter | 107 (45.9) | 122 (42.7) | 0.456 |
| Ventilator | 5 (2.1) | 5 (1.7) | 0.743 |
| Indwelling urinary catheter | 72 (30.9) | 58 (20.3) | 0.005 * |
| FUO | 130 (55.8) | 129 (45.1) | 0.015 * |
| MDI | 45 (19.3) | 61 (21.3) | 0.571 |
| CDI | 58 (24.9) | 96 (33.6) | 0.031 * |
| Hematologic disease | |||
| Acute myeloid leukemia | 55 (23.6) | 118 (41.3) | <0.001 * |
| Myelodysplastic syndrome | 27 (11.6) | 35 (12.2) | 0.820 |
| Acute lymphocytic leukemia | 11 (4.7) | 12 (4.2) | 0.772 |
| Malignant lymphoma | 82 (35.2) | 73 (25.5) | 0.017 * |
| Multiple myeloma | 28 (12.0) | 14 (4.9) | 0.003 * |
| Aplastic anemia | 9 (3.9) | 16 (5.6) | 0.359 |
| Chemotherapy within 3 weeks | 151 (64.8) | 190 (66.4) | 0.698 |
| AHSCT | 19 (8.2) | 17 (5.9) | 0.324 |
| Blood culture (two sets) before starting antibiotics | 155 (66.5) | 209 (73.1) | 0.105 |
| Blood culture positivity | 54 (23.2) | 71 (24.8) | 0.662 |
| ESBL and AmpC | 16 (6.9) | 37 (68.9) | 0.023 * |
| Variable | β | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|
| Age | −0.014 | 0.986 | 0.973–1.001 | 0.059 |
| Granulocytes | 0.000 | 1.000 | 1.000–1.000 | 0.127 |
| Outpatient onset | 0.533 | 1.704 | 1.030–2.818 | 0.038 * |
| Diabetes mellitus | 0.423 | 1.527 | 0.804–2.897 | 0.196 |
| COPD | 2.132 | 8.436 | 1.067–66.667 | 0.043 * |
| Indwelling urinary catheter | −0.406 | 0.666 | 0.421–1.056 | 0.084 |
| FUO | −0.257 | 0.773 | 0.461–1.296 | 0.329 |
| CDI | 0.281 | 1.325 | 0.750–2.341 | 0.333 |
| Acute myeloid leukemia | 0.539 | 1.715 | 1.057–2.782 | 0.029 * |
| Malignant lymphoma | −0.342 | 0.710 | 0.438–1.151 | 0.165 |
| Multiple myeloma | −1.010 | 0.364 | 0.168–0.792 | 0.011 * |
| ESBL and AmpC | 1.036 | 2.819 | 1.382–5.750 | 0.004 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, A.; Yamaguchi, F.; Maeda, M.; Hashiguchi, M.; Kabasawa, N.; Sasaki, J.; Sato, T.; Fuyama, M.; Yamazaki, Y.; Endo, K.; et al. Antimicrobial Stewardship Program for Patients in the Hematological Department Receiving Carbapenem Therapy: A Single-Center and Interrupted Time Series Analysis. Antibiotics 2023, 12, 302. https://doi.org/10.3390/antibiotics12020302
Suzuki A, Yamaguchi F, Maeda M, Hashiguchi M, Kabasawa N, Sasaki J, Sato T, Fuyama M, Yamazaki Y, Endo K, et al. Antimicrobial Stewardship Program for Patients in the Hematological Department Receiving Carbapenem Therapy: A Single-Center and Interrupted Time Series Analysis. Antibiotics. 2023; 12(2):302. https://doi.org/10.3390/antibiotics12020302
Chicago/Turabian StyleSuzuki, Ayako, Fumihiro Yamaguchi, Masayuki Maeda, Miyuki Hashiguchi, Nobuyuki Kabasawa, Jun Sasaki, Tokutada Sato, Masaki Fuyama, Yohei Yamazaki, Kei Endo, and et al. 2023. "Antimicrobial Stewardship Program for Patients in the Hematological Department Receiving Carbapenem Therapy: A Single-Center and Interrupted Time Series Analysis" Antibiotics 12, no. 2: 302. https://doi.org/10.3390/antibiotics12020302